
Diabetic Ketoacidosis Fluid Therapy Algorithm in the Golden Hours: Iatrogenic Hyperchloremic Acidosis Instead of Unmeasured Anion Acidosis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Definition of DKA
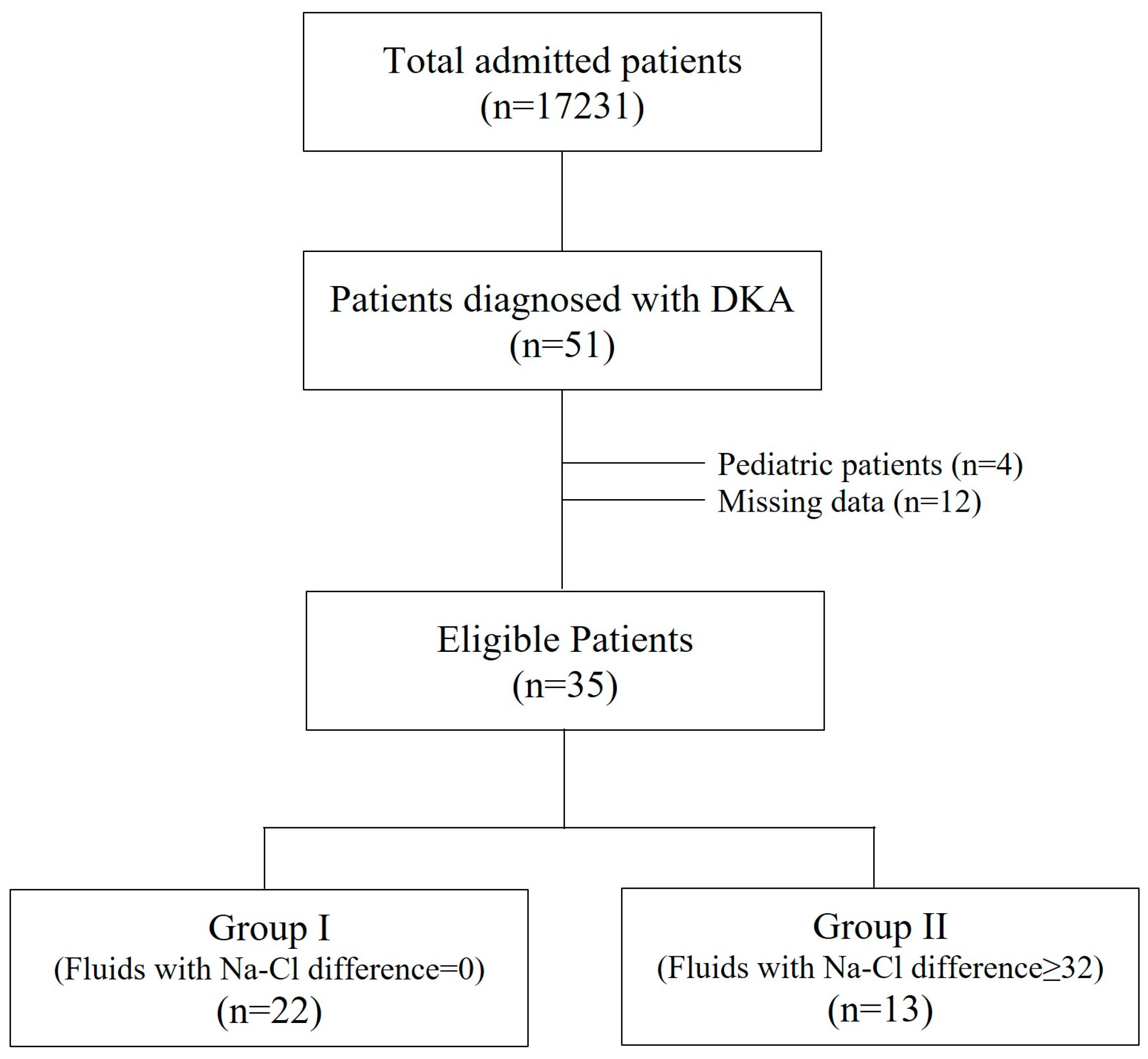
2.3. Patients
2.4. Collected Data
2.5. Statistical Analysis
3. Results
3.1. At the ICU Admission
3.2. Administered Fluids in the First 6 h (‘Golden Hours’)
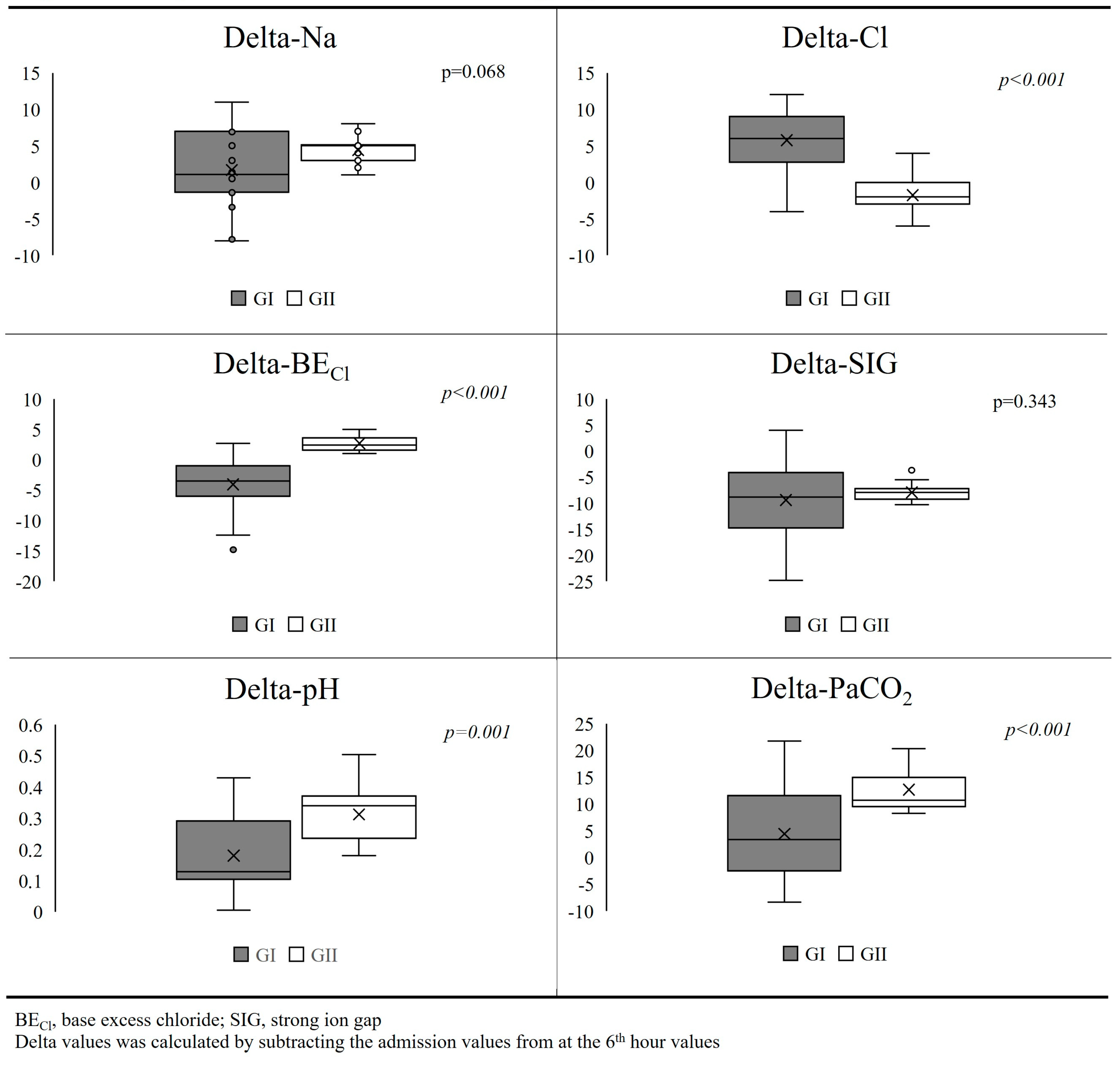
3.3. At the End of the Golden Hours
4. Discussion
4.1. Restoration of Circulatory Volume
4.2. Elimination of Ketones
4.3. Correction of Electrolyte Imbalances
4.4. What Is the Appropriate Type of Fluid?
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sieben, N.; Ramanan, M. Research Priorities for Diabetic Ketoacidosis: An Evidence and Gap Mapping Review. Med. Sci. 2025, 13, 53. [Google Scholar] [CrossRef] [PubMed]
- Ramanan, M.; Rajbhandari, D.; Koch, C.; Abdelhamid, Y.A.; Attokaran, A.; Billot, L.; Bompoint, S.; Cohen, J.; Delaney, A.; Devaux, A.; et al. Buffered salt solution versus 0.9% sodium chloride as fluid therapy for patients presenting with moderate to severe diabetic ketoacidosis: Study protocol for a Phase-3 cluster-crossover, blinded, randomised, controlled trial. Crit. Care Resusc. 2025, 27, 100104. [Google Scholar] [CrossRef] [PubMed]
- Dhatariya, K.K. Joint British Diabetes Societies for Inpatient Care. The Management of Diabetic Ketoacidosis in Adults-An Updated Guideline from the Joint British Diabetes Society for Inpatient Care. Diabet. Med. 2022, 39, e14788. [Google Scholar] [CrossRef] [PubMed]
- Al-Jaghbeer, M.; Kellum, J.A. Acid–Base Disturbances in Intensive Care Patients: Etiology, Pathophysiology and Treatment. Nephrol. Dial. Transpl. 2014, 30, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Kamel, K.S.; Halperin, M.L. Acid-Base Problems in Diabetic Ketoacidosis. N. Engl. J. Med. 2015, 372, 1969–1970. [Google Scholar] [CrossRef] [PubMed]
- Gucyetmez, B.; Tuzuner, F.; Atalan, H.K.; Sezerman, U.; Gucyetmez, K.; Telci, L. Base-Excess Chloride; the Best Approach to Evaluate the Effect of Chloride on the Acid-Base Status: A Retrospective Study. PLoS ONE 2021, 16, e0250274. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Elbers, P.W.G. Stewart’s Textbook of Acid-Base; Lulu.com: Morrisville, NC, USA, 2009; ISBN 9781409254706. [Google Scholar]
- Kellum, J.A.; Kramer, D.J.; Pinsky, M.R. Strong Ion Gap: A Methodology for Exploring Unexplained Anions. J. Crit. Care 1995, 10, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Davis, G.M.; ElSayed, N.A.; Fadini, G.P.; Galindo, R.J.; Hirsch, I.B.; Klonoff, D.C.; McCoy, R.G.; Misra, S.; Gabbay, R.A.; et al. Hyperglycemic Crises in Adults with Diabetes: A Consensus Report. Diabetes Care 2024, 47, 1257–1275. [Google Scholar] [CrossRef] [PubMed]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic Crises in Adult Patients with Diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Parajuli, B.; Angurana, S.K.; Baalaaji, M.; Williams, V. Acute Kidney Injury in Children with Diabetic Ketoacidosis: A Real Concern. Pediatr. Crit. Care Med. 2019, 20, 590–591. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.E.; Parsons, S.J.; Wade, A.W. The Effect of Dehydration, Hyperchloremia and Volume of Fluid Resuscitation on Acute Kidney Injury in Children Admitted to Hospital with Diabetic Ketoacidosis. Pediatr. Nephrol. 2024, 39, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Yunos, N.M.; Bellomo, R.; Hegarty, C.; Story, D.; Ho, L.; Bailey, M. Association between a Chloride-Liberal vs Chloride-Restrictive Intravenous Fluid Administration Strategy and Kidney Injury in Critically Ill Adults. JAMA 2012, 308, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Yunos, N.M.; Kim, I.B.; Bellomo, R.; Bailey, M.; Ho, L.; Story, D.; Gutteridge, G.A.; Hart, G.K. The Biochemical Effects of Restricting Chloride-Rich Fluids in Intensive Care. Crit. Care Med. 2011, 39, 2419–2424. [Google Scholar] [CrossRef] [PubMed]
- Todd, S.R.; Malinoski, D.; Muller, P.J.; Schreiber, M.A. Lactated Ringer’s Is Superior to Normal Saline in the Resuscitation of Uncontrolled Hemorrhagic Shock. J. Trauma 2007, 62, 636–639. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.W.; Slim, A.; Van Aarsen, K.; Choi, Y.-H.; Byrne, C.; Poonai, N.; Collins, H.; Clemens, K.K. Balanced Crystalloids (RInger’s Lactate) versus Normal Saline in Adults with Diabetic Ketoacidosis in the Emergency Department (BRISK-ED): A Pilot Randomised Controlled Trial. Emerg. Med. J. 2023, 41, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Evans, C.S.; Jenkins, C.A.; Brown, R.M.; Casey, J.D.; Collins, S.P.; Coston, T.D.; Felbinger, M.; Flemmons, L.N.; Hellervik, S.M.; et al. Clinical Effects of Balanced Crystalloids vs Saline in Adults with Diabetic Ketoacidosis: A Subgroup Analysis of Cluster Randomized Clinical Trials. JAMA Netw. Open 2020, 3, e2024596. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, A.R.; Elwood, K.; Werth, C.; Mitchell, J.; Sarangarm, P. Balanced Crystalloid Versus Normal Saline as Resuscitative Fluid in Diabetic Ketoacidosis. Ann. Pharmacother. 2022, 56, 998–1006. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| GI (Fluids with Na-Cl Difference = 0) (n = 22) | GII (Fluids with Na-Cl Difference > 32 mmol) (n = 13) | p | |
|---|---|---|---|
| Patient characteristics | |||
| Age (year) | 52 ± 23 | 50 ± 18 | 0.567 |
| Male (%) | 10 (47.6) | 4 (30.8) | 0.477 |
| BMI (kg/m2) | 24.2 ± 3.2 | 26.6 ± 6.6 | 0.184 |
| CCI | 3 (1–7) | 2 (2–6) | 0.972 |
| APACHE II | 14 (11–24) | 16 (12–25) | 0.311 |
| SOFA score | 2 (1–6) | 3 (1–9) | 0.362 |
| Blood gas and laboratory parameters at admission | |||
| pH | 7.10 ± 0.10 | 7.08 ± 0.10 | 0.562 |
| PaCO2 (mmHg) | 16.4 (8.1–31.7) | 14.3 (6.5–22.6) | 0.353 |
| HCO3 (mmol/L) | 7.2 ± 3.1 | 7.9 ± 3.5 | 0.577 |
| SBE (mmol/L) | −24.7 (−28.9; −12.5) | −23.5 (−27.9; −7.8) | 0.853 |
| Na (mmol/L) | 135 (120–146) | 136 (124–138) | 0.448 |
| Cl (mmol/L) | 106 ± 7 | 105 ± 6 | 0.876 |
| BECl (mmol/L) | −2 ± 6 | −4 ± 3 | 0.337 |
| K (mmol/L) | 4.4 (2.8–5.6) | 4.0 (1.9–7.6) | 0.319 |
| Lactate (mmol/L) | 2.1 (0.7–9.1) | 2.0 (1.3–8.6) | 0.933 |
| Hct (%) | 40.9 ± 2.9 | 39.0 ± 3.0 | 0.067 |
| Glucose (mg/dL) | 426 (255–850) | 537 (305–661) | 0.801 |
| SIG (mmol/L) | 19.3 (11.1–33.4) | 19.0 (7.0–24.7) | 0.827 |
| Urine ketones | 3 (2–4) | 2 (2–4) | 0.649 |
| Urea (mg/dL) | 56 (13–132) | 64 (49–115) | 0.243 |
| Creatinine (mg/dL) | 1.5 (0.6–4.7) | 1.9 (1.5–3.5) | 0.086 |
| Na (mmol/L) | Cl (mmol/L) | Na-Cl Difference | GI (Fluids with Na-Cl Difference = 0) (n = 22) | GII (Fluids with Na-Cl Difference > 32 mmol) (n = 13) | |
|---|---|---|---|---|---|
| %0.9 NaCl, n (%) (mL) | 154 | 154 | 0 | 21 (95.2) 2302 ± 1188 | - |
| %5 Dextrose %0.9 NaCl, n (%) (mL) | 154 | 154 | 0 | 1 (4.6) 0 (0–600) | - |
| %0.45 NaCl, n (%) (mL) | 77 | 77 | 0 | 1 (4.6) 0 (0–1500) | - |
| %5 Dextrose %0.45 NaCl, n (%) (mL) | 77 | 77 | 0 | 4 (18.2) 0 (0–2000) | - |
| %5 Dextrose, n (%) (mL) | - | - | 0 | 5 (22.7) 0 (0–1500) | - |
| Human Albumin 20%, n (%) (mL) | 125 | 100 | 0 | 1 (4.6) 0 (0–60) | - |
| HES 6%, n (%) (mL) | 154 | 154 | 0 | 1 (4.6) 0 (0–1000) | - |
| %0.45 NaCl (65 mEq NaHCO3/935 mL), n (%) (mL) | 143 | 83 | 50 | - | 5 (38.5) 0 (0–4450) |
| Isolyte, n (%) (mL) | 140 | 103 | 37 | - | 4 (30.8) 0 (0–3300) |
| Isolyte-S, n (%) (mL) | 141 | 98 | 43 | - | 4 (30.8) 0 (0–3250) |
| GI (Fluids with Na-Cl Difference = 0) (n = 22) | GII (Fluids with Na-Cl Difference > 32 mmol) (n = 13) | p | |
|---|---|---|---|
| Total fluid input in the first 6 h | |||
| Administered fluid (mL/kg/h) | 6.2 (4.4–15.5) | 6.9 (5.3–10.9) | 0.699 |
| NaHCO3 (mmol) | 60 (0–350) | 100 (0–150) | 0.389 |
| KCl (mmol) | 0 (0–75) | 0 (0–30) | 0.511 |
| Insulin (U/kg/h) | 0.08 (0.02–0.56) | 0.08 (0.04–0.11) | 0.933 |
| Administered Na (mmol) (only from fluids) | 343 (116–770) | 420 (310–636) | 0.091 |
| Administered Cl (mmol) (only from fluids) | 343 (116–770) | 273 (216–374) | 0.016 |
| Na-Cl difference (mmol) (only for fluids) | 0 (0–0) | 144 (95–263) | <0.001 |
| Urine output (mL kg−1 h−1) | 3.6 (0.5–7.8) | 2.7 (0.2–11.2) | 0.448 |
| Blood gas parameters at the 6th hour | |||
| pH | 7.28 (7.11–7.40) | 7.38 (7.35–7.49) | <0.001 |
| PaCO2 (mmHg) | 23.0 ± 5.7 | 27.8 ± 3.5 | 0.010 |
| HCO3 (mmol/L) | 12.9 (4.3–21.9) | 16.5 (16.1–23.1) | <0.001 |
| SBE (mmol/L) | −14.6 (−23.2; 0.0) | −9.8 (−12.2; −2.8) | 0.002 |
| Na (mmol/L) | 138 ± 6 | 139 ± 5 | 0.622 |
| Cl, (mmol/L) | 112 ± 7 | 104 ± 5 | <0.001 |
| BECl (mmol/L) | −6 ± 5 | 3 ± 1 | <0.001 |
| K (mmol/L) | 3.5 ± 0.6 | 3.2 ± 0.7 | 0.115 |
| Lactate (mmol/L) | 1.5 (0.8–6.4) | 1.7 (0.9–7.4) | 0.229 |
| Hct (%) | 35.9 ± 2.5 | 34.4 ± 2.1 | 0.091 |
| Glucose (mg/dL) | 256 (100–411) | 268 (113–431) | 0.972 |
| SIG (mmol/L) | 9.8 (−1.1; 22.8) | 11.1 (−1.0; 15.7) | 0.408 |
| Laboratory parameters at the 24th hour | |||
| Urine ketones (at the 24th hour) | 2 (0–3) | 1 (0–3) | 0.302 |
| Urea, (mg/dL) (at the 24th hour) | 30 (16–100) | 46 (34–92) | 0.112 |
| Creatinine (mg/dL), (at the 24th hour) | 1.1 (0.4–3.9) | 1.4 (0.9–2.6) | 0.089 |
| Outcomes | |||
| LOS-ICU (days) | 3 (2–4) | 2 (1–3) | 0.023 |
| OR (95% CI) | p | |
|---|---|---|
| Age | 0.19 (−0.001; 0.039) | 0.060 |
| BMI | −0.37 (−0.097; 0.023) | 0.214 |
| APACHE II | −0.031 (−0.100; 0.039) | 0.371 |
| SOFA Score | 0.068 (−0.087; 0.223) | 0.373 |
| Delta-pH (x100) | 0.036 (−0.021; 0.092) | 0.209 |
| Delta-CO2 | 0.070 (−0.106; 0.156) | 0.104 |
| Delta-HCO3 | −0.051 (−0.149; 0.047) | 0.295 |
| Delta-Na | −0.043 (−0.208; 0.123) | 0.597 |
| Delta-Cl | 0.203 (0.021; 0.386) | 0.031 |
| delta-lactate | 0.033 (0.020; 0.639) | 0.038 |
| Delta-SIG | 0.069 (−0.097; 0.235) | 0.396 |
| Delta-glucose | 0.001 (−0.002; 0.004) | 0.602 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarikaya, Z.T.; Gucyetmez, B.; Ozdemir, D.; Dogruel, B.; Ayyildiz, A.; Kesecioglu, J.; Telci, L. Diabetic Ketoacidosis Fluid Therapy Algorithm in the Golden Hours: Iatrogenic Hyperchloremic Acidosis Instead of Unmeasured Anion Acidosis. J. Clin. Med. 2025, 14, 4125. https://doi.org/10.3390/jcm14124125
Sarikaya ZT, Gucyetmez B, Ozdemir D, Dogruel B, Ayyildiz A, Kesecioglu J, Telci L. Diabetic Ketoacidosis Fluid Therapy Algorithm in the Golden Hours: Iatrogenic Hyperchloremic Acidosis Instead of Unmeasured Anion Acidosis. Journal of Clinical Medicine. 2025; 14(12):4125. https://doi.org/10.3390/jcm14124125
Chicago/Turabian StyleSarikaya, Zeynep Tugce, Bulent Gucyetmez, Duran Ozdemir, Behiye Dogruel, Aykut Ayyildiz, Jozef Kesecioglu, and Lutfi Telci. 2025. "Diabetic Ketoacidosis Fluid Therapy Algorithm in the Golden Hours: Iatrogenic Hyperchloremic Acidosis Instead of Unmeasured Anion Acidosis" Journal of Clinical Medicine 14, no. 12: 4125. https://doi.org/10.3390/jcm14124125
APA StyleSarikaya, Z. T., Gucyetmez, B., Ozdemir, D., Dogruel, B., Ayyildiz, A., Kesecioglu, J., & Telci, L. (2025). Diabetic Ketoacidosis Fluid Therapy Algorithm in the Golden Hours: Iatrogenic Hyperchloremic Acidosis Instead of Unmeasured Anion Acidosis. Journal of Clinical Medicine, 14(12), 4125. https://doi.org/10.3390/jcm14124125