
Non-Traumatic Lower-Limb Amputations: Outcome, Sex-Differences, Comorbidity Patterns and Temporal Trends from 2006 to 2022

 , , , ,
, , , , 
 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Population and Outcome
2.2. Statistics
3. Results
3.1. Baseline Characteristics and Comorbidities
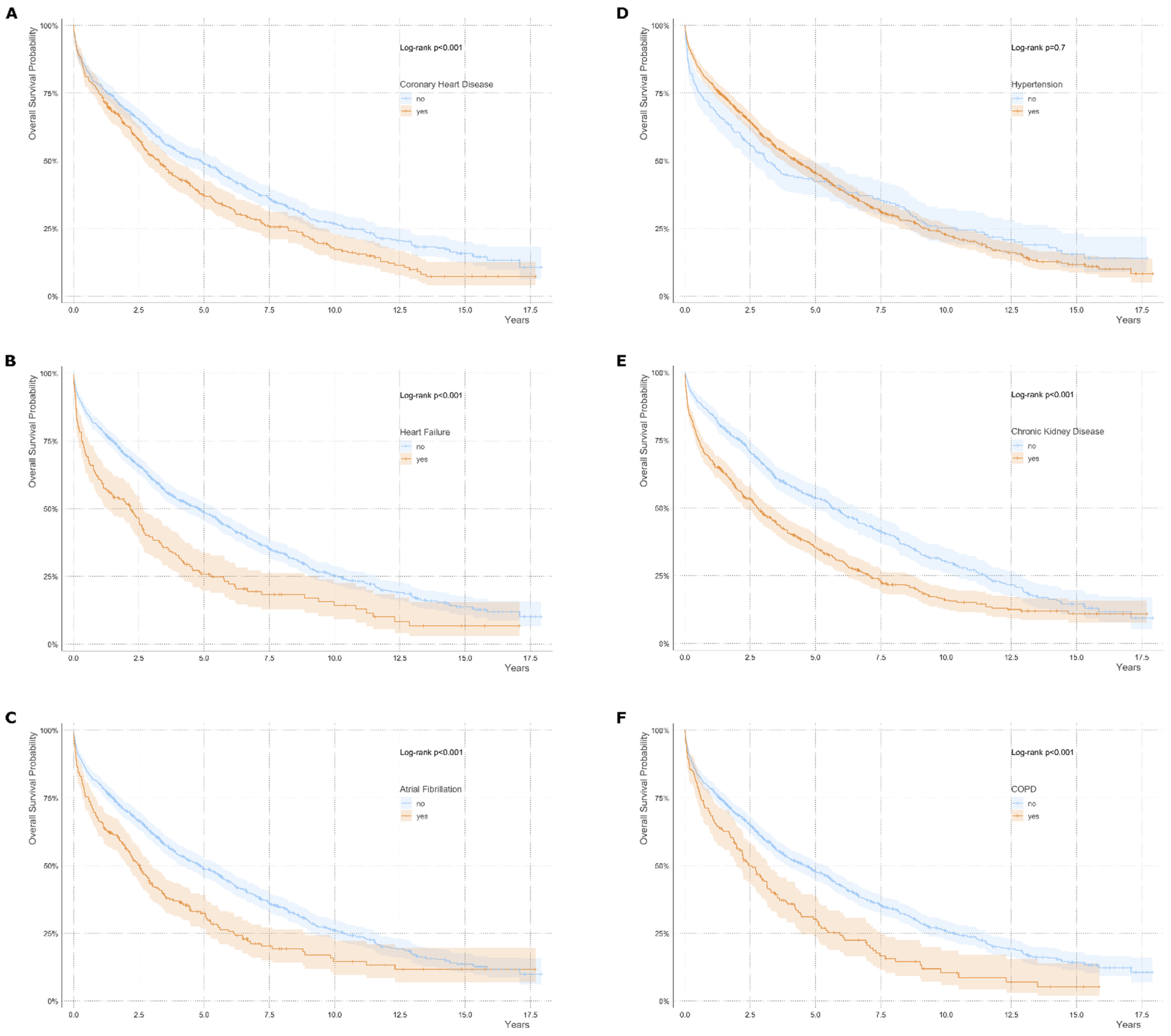
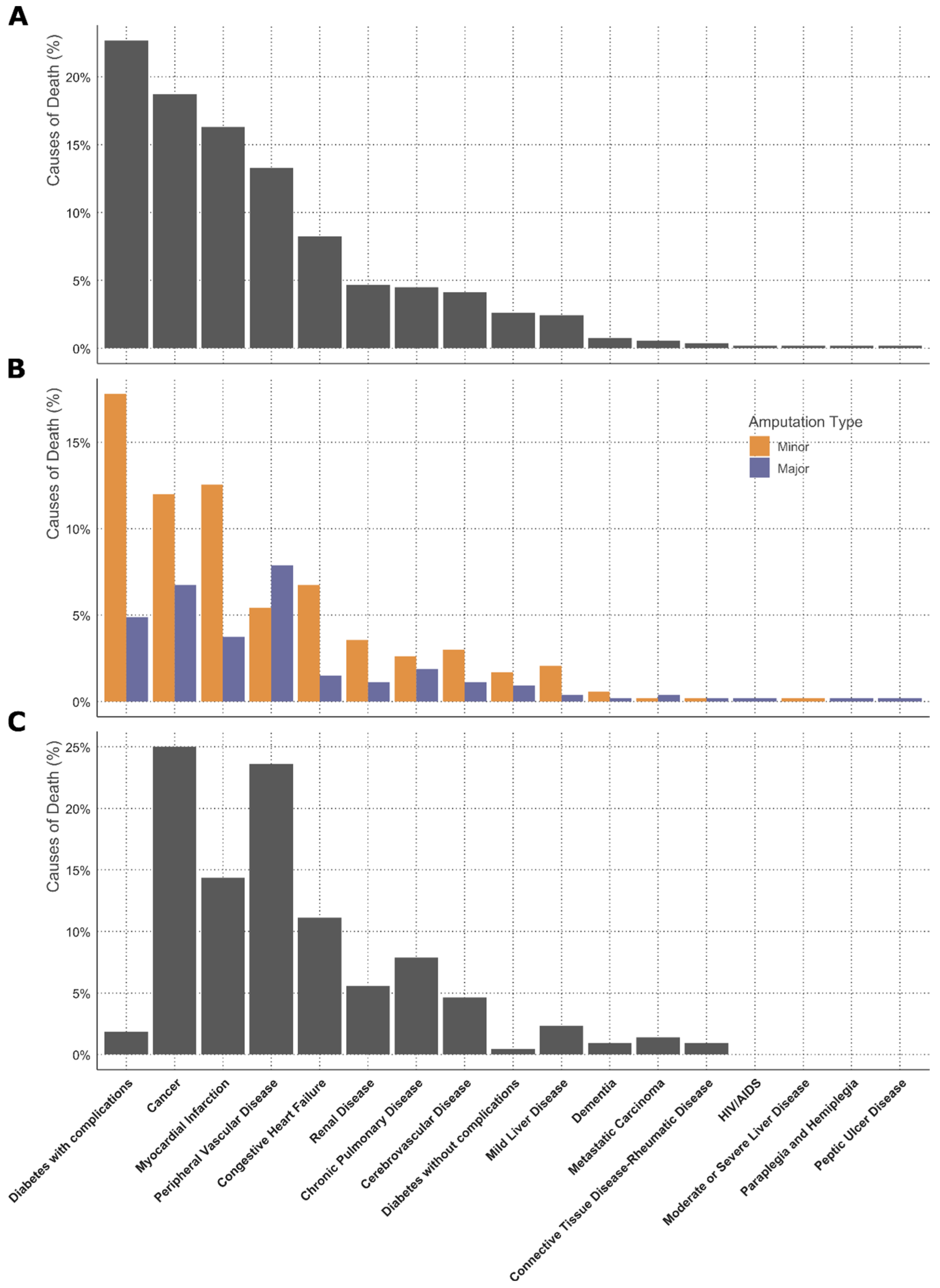
3.2. Survival Analysis and Causes of Death
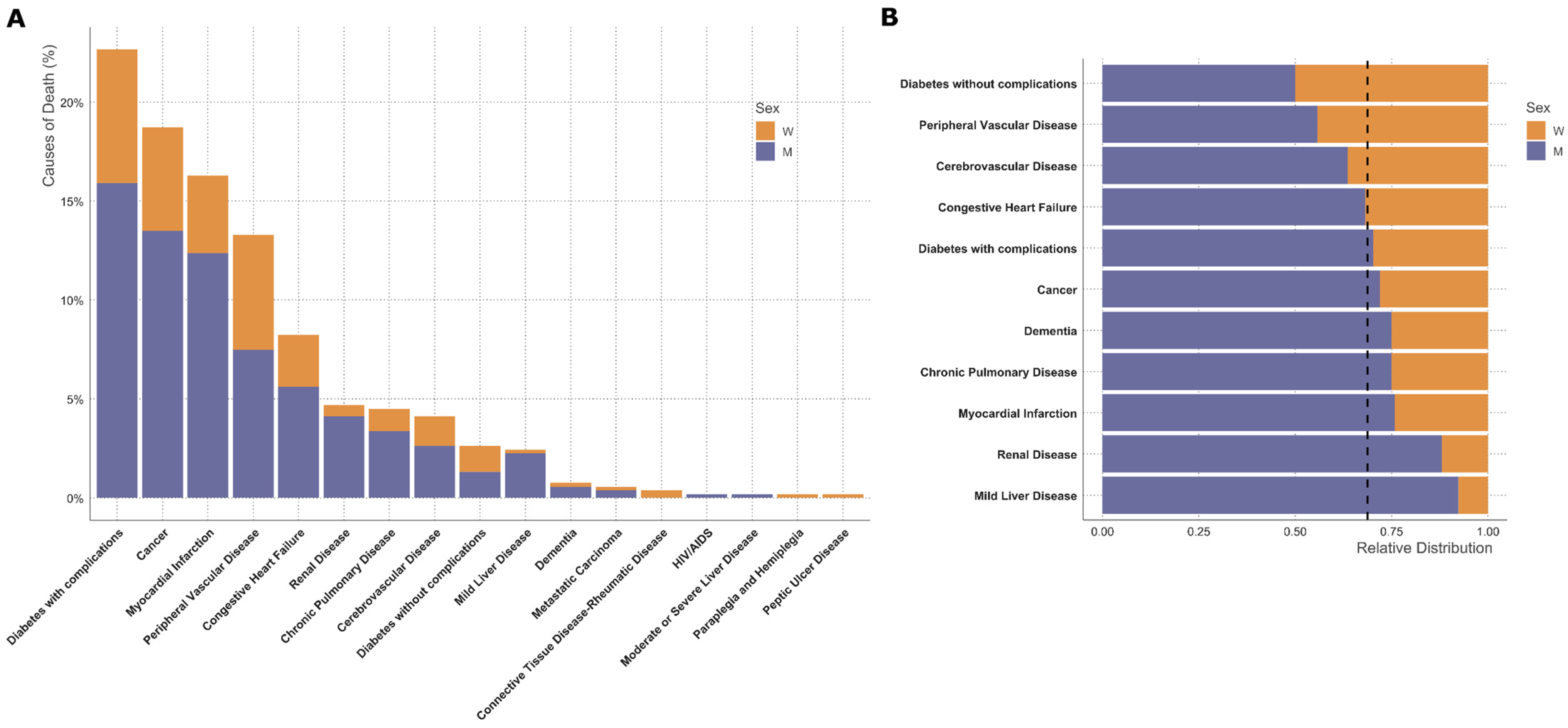
3.3. Sex-Specific Analysis
4. Discussion
5. Conclusions
Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Creager, M.A.; Matsushita, K.; Arya, S.; Beckman, J.A.; Duval, S.; Goodney, P.P.; Gutierrez, J.A.T.; Kaufman, J.A.; Maddox, K.E.J.; Pollak, A.W.; et al. Reducing Nontraumatic Lower-Extremity Amputations by 20% by 2030: Time to Get to Our Feet: A Policy Statement from the American Heart Association. Circulation 2021, 143, e875–e891. [Google Scholar] [CrossRef]
- Heikkila, K.; Loftus, I.M.; Mitchell, D.C.; Johal, A.S.; Waton, S.; Cromwell, D.A. Population-based study of mortality and major amputation following lower limb revascularization. Br. J. Surg. 2018, 105, 1145–1154. [Google Scholar] [CrossRef]
- Li, Q.; Birmpili, P.; Atkins, E.; Johal, A.S.; Waton, S.; Williams, R.; Boyle, J.R.; Harkin, D.W.; Pherwani, A.D.; Cromwell, D.A. Illness Trajectories After Revascularization in Patients with Peripheral Artery Disease: A Unified Approach to Understanding the Risk of Major Amputation and Death. Circulation 2024, 150, 261–271. [Google Scholar] [CrossRef]
- Qaarie, M.Y. Life Expectancy and Mortality After Lower Extremity Amputation: Overview and Analysis of Literature. Cureus 2023, 15, e38944. [Google Scholar] [CrossRef]
- Gyldenkerne, C.; Olesen, K.K.W.; Thrane, P.G.; Hansen, M.K.; Stodkilde-Jorgensen, N.; Sorensen, H.T.; Thomsen, R.W.; Maeng, M. Trends in Peripheral Artery Disease, Lower Extremity Revascularization, and Lower Extremity Amputation in Incident Type 2 Diabetes: A Danish Population-Based Cohort Study. Diabetes Care 2025, 48, 76–83. [Google Scholar] [CrossRef]
- Lopez-de-Andres, A.; Jimenez-Garcia, R.; Hernandez-Barrera, V.; de Miguel-Diez, J.; de Miguel-Yanes, J.M.; Omana-Palanco, R.; Carabantes-Alarcon, D. Trends of Non-Traumatic Lower-Extremity Amputation and Type 2 Diabetes: Spain, 2001–2019. J. Clin. Med. 2022, 11, 1246. [Google Scholar] [CrossRef]
- Aziz, F.; Reichardt, B.; Sourij, C.; Dimai, H.P.; Reichart, D.; Kohler, G.; Brodmann, M.; Sourij, H. Epidemiology of major lower extremity amputations in individuals with diabetes in Austria, 2014–2017: A retrospective analysis of health insurance database. Diabetes Res. Clin. Pract. 2020, 170, 108477. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Leutner, M.; Harreiter, J. Sex differences in type 2 diabetes. Diabetologia 2023, 66, 986–1002. [Google Scholar] [CrossRef]
- Emerging Risk Factors, C.; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef]
- Huxley, R.; Barzi, F.; Woodward, M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: Meta-analysis of 37 prospective cohort studies. BMJ 2006, 332, 73–78. [Google Scholar] [CrossRef]
- Norhammar, A. Diabetes and cardiovascular mortality: The impact of sex. Lancet Diabetes Endocrinol. 2018, 6, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Prospective Studies, C.; Asia Pacific Cohort Studies, C. Sex-specific relevance of diabetes to occlusive vascular and other mortality: A collaborative meta-analysis of individual data from 980 793 adults from 68 prospective studies. Lancet Diabetes Endocrinol. 2018, 6, 538–546. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Pabon, M.; Cheng, S.; Altin, S.E.; Sethi, S.S.; Nelson, M.D.; Moreau, K.L.; Hamburg, N.; Hess, C.N. Sex Differences in Peripheral Artery Disease. Circ. Res. 2022, 130, 496–511. [Google Scholar] [CrossRef]
- Sigvant, B.; Lundin, F.; Nilsson, B.; Bergqvist, D.; Wahlberg, E. Differences in presentation of symptoms between women and men with intermittent claudication. BMC Cardiovasc. Disord. 2011, 11, 39. [Google Scholar] [CrossRef]
- Hiramoto, J.S.; Katz, R.; Weisman, S.; Conte, M. Gender-specific risk factors for peripheral artery disease in a voluntary screening population. J. Am. Heart Assoc. 2014, 3, e000651. [Google Scholar] [CrossRef]
- Tunstall-Pedoe, H.; Peters, S.A.E.; Woodward, M.; Struthers, A.D.; Belch, J.J.F. Twenty-Year Predictors of Peripheral Arterial Disease Compared with Coronary Heart Disease in the Scottish Heart Health Extended Cohort (SHHEC). J. Am. Heart Assoc. 2017, 6, e005967. [Google Scholar] [CrossRef]
- Chase-Vilchez, A.Z.; Chan, I.H.Y.; Peters, S.A.E.; Woodward, M. Diabetes as a risk factor for incident peripheral arterial disease in women compared to men: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2020, 19, 151. [Google Scholar] [CrossRef]
- Anand, S.S.; Islam, S.; Rosengren, A.; Franzosi, M.G.; Steyn, K.; Yusufali, A.H.; Keltai, M.; Diaz, R.; Rangarajan, S.; Yusuf, S.; et al. Risk factors for myocardial infarction in women and men: Insights from the INTERHEART study. Eur. Heart J. 2008, 29, 932–940. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Ohman, E.M.; Hirsch, A.T.; Ikeda, Y.; Mas, J.L.; Goto, S.; Liau, C.S.; Richard, A.J.; Rother, J.; et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 2006, 295, 180–189. [Google Scholar] [CrossRef]
- Bavry, A.A.; Anderson, R.D.; Gong, Y.; Denardo, S.J.; Cooper-Dehoff, R.M.; Handberg, E.M.; Pepine, C.J. Outcomes Among hypertensive patients with concomitant peripheral and coronary artery disease: Findings from the INternational VErapamil-SR/Trandolapril STudy. Hypertension 2010, 55, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.J.; Shaw, P.A.; Townsend, R.R.; Anderson, A.H.; Xie, D.; Wang, X.; Nessel, L.C.; Mohler, E.R.; Sozio, S.M.; Jaar, B.G.; et al. Sex Differences in the Incidence of Peripheral Artery Disease in the Chronic Renal Insufficiency Cohort. Circ. Cardiovasc. Qual. Outcomes 2016, 9 (Suppl. S1), S86–S93. [Google Scholar] [CrossRef] [PubMed]
- Eraso, L.H.; Fukaya, E.; Mohler, E.R., 3rd; Xie, D.; Sha, D.; Berger, J.S. Peripheral arterial disease, prevalence and cumulative risk factor profile analysis. Eur. J. Prev. Cardiol. 2014, 21, 704–711. [Google Scholar] [CrossRef]
- Haine, A.; Kavanagh, S.; Berger, J.S.; Hess, C.N.; Norgren, L.; Fowkes, F.G.R.; Katona, B.G.; Mahaffey, K.W.; Blomster, J.I.; Patel, M.R.; et al. Sex-Specific Risks of Major Cardiovascular and Limb Events in Patients with Symptomatic Peripheral Artery Disease. J. Am. Coll. Cardiol. 2020, 75, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.H.; Arya, S.; Bryce, Y.; Gornik, H.L.; Long, C.A.; McDermott, M.M.; West Pollak, A.; Rowe, V.L.; Sullivan, A.E.; Whipple, M.O.; et al. Sex Differences in Peripheral Vascular Disease: A Scientific Statement from the American Heart Association. Circulation 2025, 151, e877–e904. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024. [Google Scholar]
- R Core Team. RStudio: Integrated Development Environment for R; RStudio, PBC: Boston, MA, USA, 2020. [Google Scholar]
- Subirana, I.; Sanz, H.; Vila, J. Building Bivariate Tables: The compareGroups Package for R. J. Stat. Softw. 2014, 57, 16. [Google Scholar] [CrossRef]
- TM, T. A Package for Survival Analysis in R. 2024. Available online: https://cran.r-project.org/web/packages/survival/vignettes/survival.pdf (accessed on 2 June 2025).
- Wasey, J.O.L.M.; R Core Team. icd: Comorbidity Calculations and Tools for ICD-9 and ICD-10 Codes; R Core Team: Vienna, Austria, 2024. [Google Scholar]
- Sarroca, N.; Valero, J.; Deus, J.; Casanova, J.; Luesma, M.J.; Lahoz, M. Quality of life, body image and self-esteem in patients with unilateral transtibial amputations. Sci. Rep. 2021, 11, 12559. [Google Scholar] [CrossRef]
- Collaborators, G.B.D.P.A.D. Global burden of peripheral artery disease and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Glob. Health 2023, 11, e1553–e1565. [Google Scholar] [CrossRef]
- IDF. IDF Diabetes Atlas, 10th ed.; IDF: Brussels, Belgium, 2021.
- Cherla, A.; Kyriopoulos, I.; Pearcy, P.; Tsangalidou, Z.; Hajrulahovic, H.; Theodorakis, P.; Andersson, C.E.; Mehra, M.R.; Mossialos, E. Trends in avoidable mortality from cardiovascular diseases in the European Union, 1995–2020: A retrospective secondary data analysis. Lancet Reg. Health Eur. 2024, 47, 101079. [Google Scholar] [CrossRef]
- Chesnaye, N.C.; Carrero, J.J.; Hecking, M.; Jager, K.J. Differences in the epidemiology, management and outcomes of kidney disease in men and women. Nat. Rev. Nephrol. 2024, 20, 7–20. [Google Scholar] [CrossRef]
- Inker, L.A.; Levey, A.S.; Tighiouart, H.; Shafi, T.; Eckfeldt, J.H.; Johnson, C.; Okparavero, A.; Post, W.S.; Coresh, J.; Shlipak, M.G. Performance of glomerular filtration rate estimating equations in a community-based sample of Blacks and Whites: The multiethnic study of atherosclerosis. Nephrol. Dial. Transplant. 2018, 33, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Bull, C.; Robinson, J.; Deanfield, J.E. Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J. Am. Coll. Cardiol. 1994, 24, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Moreau, K.L.; Hildreth, K.L.; Meditz, A.L.; Deane, K.D.; Kohrt, W.M. Endothelial function is impaired across the stages of the menopause transition in healthy women. J. Clin. Endocrinol. Metab. 2012, 97, 4692–4700. [Google Scholar] [CrossRef]
- Taddei, S.; Virdis, A.; Ghiadoni, L.; Mattei, P.; Sudano, I.; Bernini, G.; Pinto, S.; Salvetti, A. Menopause is associated with endothelial dysfunction in women. Hypertension 1996, 28, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Kavurma, M.M.; Boccanfuso, L.; Cutmore, C.; Passam, F.; Patel, S.; Hennessy, A.; Loa, J.; Figtree, G.A.; Golledge, J.; Robinson, D.A.; et al. A hidden problem: Peripheral artery disease in women. Eur. Heart J. Qual. Care Clin. Outcomes 2023, 9, 342–350. [Google Scholar] [CrossRef]
- Kozak, M.; Poredos, P.; Blinc, A.; Kaja Jezovnik, M.; Poredos, P. Peripheral arterial disease in women. Vasa 2024, 53, 366–370. [Google Scholar] [CrossRef]
- Altin, S.E.; Castro-Dominguez, Y.S.; Kennedy, K.F.; Orion, K.C.; Lanksy, A.J.; Abbott, J.D.; Aronow, H.D. Predictors of Underutilization of Medical Therapy in Patients Undergoing Endovascular Revascularization for Peripheral Artery Disease. JACC Cardiovasc. Interv. 2020, 13, 2911–2918. [Google Scholar] [CrossRef]
- Sourij, H.; Azhar, K.; Aziz, F.; Kojzar, H.; Sourij, C.; Fasching, P.; Clodi, M.; Ludvik, B.; Mader, J.K.; Resl, M.; et al. Metabolic risk factor targets in relation to clinical characteristics and comorbidities among individuals with type 2 diabetes treated in primary care—The countrywide cross-sectional AUSTRO-PROFIT study. Diabetes Obes. Metab. 2025, 27, 111–122. [Google Scholar] [CrossRef]
- Ramirez-Morros, A.; Franch-Nadal, J.; Real, J.; Miro-Catalina, Q.; Bundo, M.; Vlacho, B.; Mauricio, D. Clinical characteristics and degree of cardiovascular risk factor control in patients with newly-diagnosed type 2 diabetes in Catalonia. Front. Endocrinol. 2024, 15, 1339879. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Nault, P.; Giugliano, R.P.; Keech, A.C.; Pineda, A.L.; Kanevsky, E.; Kuder, J.; Murphy, S.A.; Jukema, J.W.; Lewis, B.S.; et al. Low-Density Lipoprotein Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial (Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk). Circulation 2018, 137, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Schafer, Z.; Mathisen, A.; Thomsen, T.R.; Rossing, P.; Kirketerp-Moller, K. Glucagon-like peptide-1 treatment reduces the risk of diabetes-type 2 related amputations: A cohort study in Denmark. Diabetes Res. Clin. Pract. 2023, 202, 110799. [Google Scholar] [CrossRef] [PubMed]
- Wisman, P.P.; Tangelder, M.J.; van Hattum, E.S.; de Borst, G.J.; Moll, F.L. Young women with PAD are at high risk of cardiovascular complications. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 441–445. [Google Scholar] [CrossRef]
- Pawlik, A.; Januszek, R.; Ruzsa, Z.; Orias, V.; Kleczynski, P.; Wojtasik-Bakalarz, J.; Arif, S.; Nyerges, A.; Chyrchel, M.; Stanek, A.; et al. Gender differences and long-term clinical outcomes in patients with chronic total occlusions of infrainguinal lower limb arteries treated from retrograde access with peripheral vascular interventions. Adv. Med. Sci. 2020, 65, 197–201. [Google Scholar] [CrossRef]
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2007, 25, 1105–1187. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| [ALL] | 2006–2010 | 2011–2015 | 2016–2019 | 2020–2022 | p.overall | p.trend | |
|---|---|---|---|---|---|---|---|
| N = 1107 | N = 361 | N = 290 | N = 250 | N = 206 | |||
| Age (years) | 73.6 [64.7; 81.5] | 72.0 [62.7; 80.5] | 73.9 [66.0; 82.0] | 73.4 [64.1; 81.4] | 75.3 [66.4; 82.1] | 0.071 | 0.033 |
| <Median | 553 (50.0%) | 192 (53.2%) | 140 (48.3%) | 127 (50.8%) | 94 (45.6%) | 0.328 | 0.194 |
| >Median | 554 (50.0%) | 169 (46.8%) | 150 (51.7%) | 123 (49.2%) | 112 (54.4%) | ||
| Female Sex | 345 (31.2%) | 135 (37.4%) | 92 (31.7%) | 59 (23.6%) | 59 (28.6%) | 0.006 | 0.007 |
| BMI (kg/m2) | 24.8 [22.0; 28.5] | 25.0 [21.8; 28.0] | 24.4 [21.6; 27.9] | 26.4 [22.9; 29.6] | 24.4 [22.0; 28.2] | 0.004 | 0.471 |
| Risk factors | |||||||
| Smoking | 279 (28.0%) | 83 (31.7%) | 83 (29.5%) | 58 (23.2%) | 55 (27.0%) | <0.001 | 0.011 |
| Diabetes | 608 (55.0%) | 224 (62.2%) | 134 (46.2%) | 142 (56.8%) | 108 (52.4%) | 0.001 | 0.124 |
| LDL-C (mg/dL) | 79.0 [59.0; 102] | 87.5 [68.0; 117] | 77.0 [57.0; 98.0] | 78.0 [59.0; 99.0] | 74.0 [52.0; 98.5] | 0.001 | 0.003 |
| Hypertension | 856 (77.5%) | 259 (72.1%) | 210 (72.4%) | 208 (83.2%) | 179 (86.9%) | <0.001 | <0.001 |
| Statin usage | 563 (50.9%) | 124 (34.3%) | 158 (54.5%) | 159 (63.6%) | 122 (59.2%) | <0.001 | <0.001 |
| Comorbidities | |||||||
| CHD | 401 (36.3%) | 123 (34.2%) | 81 (27.9%) | 102 (40.8%) | 95 (46.1%) | 0.001 | 0.003 |
| Heart failure | 182 (16.5%) | 59 (16.5%) | 35 (12.1%) | 53 (21.2%) | 35 (17.0%) | 0.071 | 0.330 |
| CKD | 478 (43.9%) | 157 (44.4%) | 134 (46.5%) | 114 (46.0%) | 73 (36.5%) | 0.143 | 0.197 |
| Creatinine (mg/dL) | 1.07 [0.81; 1.62] | 1.06 [0.80; 1.66] | 1.09 [0.82; 1.72] | 1.14 [0.86; 1.53] | 1.00 [0.77; 1.41] | 0.141 | 0.272 |
| eGFR (mL/min/1.73 m2) | 0.118 | 0.068 | |||||
| <30 | 174 (16.0%) | 66 (18.6%) | 50 (17.4%) | 33 (13.3%) | 25 (12.5%) | ||
| 30–60 | 304 (27.9%) | 91 (25.7%) | 84 (29.2%) | 81 (32.7%) | 48 (24.0%) | ||
| >60 | 612 (56.1%) | 197 (55.6%) | 154 (53.5%) | 134 (54.0%) | 127 (63.5%) | ||
| Atrial Fibrillation | 267 (24.2%) | 65 (18.1%) | 62 (21.4%) | 80 (32.1%) | 60 (29.1%) | 0.001 | <0.001 |
| COPD | 177 (16.0%) | 45 (12.5%) | 45 (15.5%) | 46 (18.5%) | 41 (20.0%) | 0.107 | 0.020 |
| Amputation Type | 0.263 | 0.230 | |||||
| Minor | 752 (67.9%) | 240 (66.5%) | 188 (64.8%) | 181 (72.4%) | 143 (69.4%) | ||
| Major | 355 (32.1%) | 121 (33.5%) | 102 (35.2%) | 69 (27.6%) | 63 (30.6%) |
| All N = 1107 | Females N = 345 | Males N = 762 | p-Value | |
|---|---|---|---|---|
| Age (years) | 73.6 [64.7; 81.5] | 78.9 [70.3; 86.8] | 71.4 [63.0; 79.3] | <0.001 |
| <Median | 553 (50.0%) | 115 (33.3%) | 438 (57.5%) | <0.001 |
| >Median | 554 (50.0%) | 230 (66.7%) | 324 (42.5%) | |
| BMI (kg/m2) | 24.8 [22.0; 28.5] | 23.9 [20.2; 28.6] | 25.1 [22.6; 28.5] | 0.002 |
| Risk factors | ||||
| Smoking | 279 (28.0%) | 65 (21.2%) | 214 (31.0%) | 0.002 |
| Diabetes | 608 (55.0%) | 167 (48.4%) | 441 (58.0%) | 0.005 |
| LDL-C (mg/dL) | 79.0 [59.0; 102] | 88.0 [63.0; 115] | 77.0 [57.0; 98.0] | 0.002 |
| Hypertension | 856 (77.5%) | 266 (77.1%) | 590 (77.6%) | 0.906 |
| Statin usage | 563 (50.9%) | 142 (41.2%) | 421 (55.2%) | <0.001 |
| Comorbidities | ||||
| CHD | 401 (36.3%) | 94 (27.2%) | 307 (40.3%) | <0.001 |
| Heart failure | 182 (16.5%) | 51 (14.8%) | 131 (17.3%) | 0.399 |
| CKD | 478 (43.9%) | 176 (51.6%) | 302 (40.3%) | 0.001 |
| Creatinine (mg/dL) | 1.07 [0.81; 1.62] | 0.98 [0.73; 1.50] | 1.12 [0.85; 1.65] | <0.001 |
| eGFR (mL/min/1.73 m2) | 0.003 | |||
| <30 | 174 (16.0%) | 64 (18.8%) | 110 (14.7%) | |
| 30–60 | 304 (27.9%) | 112 (32.8%) | 192 (25.6%) | |
| >60 | 612 (56.1%) | 165 (48.4%) | 447 (59.7%) | |
| Atrial Fibrillation | 267 (24.2%) | 77 (22.3%) | 190 (25.0%) | 0.399 |
| COPD | 177 (16.0%) | 36 (10.4%) | 141 (18.6%) | 0.002 |
| Amputation Type | <0.001 | |||
| Minor | 752 (67.9%) | 187 (54.2%) | 565 (74.1%) | |
| Major | 355 (32.1%) | 158 (45.8%) | 197 (25.9%) |
| [ALL] | 2006–2010 | 2011–2015 | 2016–2019 | 2020–2022 | p.overall | p.trend | |
|---|---|---|---|---|---|---|---|
| N = 345 | N = 135 | N = 92 | N = 59 | N = 59 | |||
| Age (years) | 78.9 [70.3; 86.8] | 79.3 [69.0; 85.5] | 80.8 [72.9; 89.3] | 77.1 [70.1; 86.5] | 78.3 [68.3; 86.9] | 0.678 | 0.893 |
| <Median | 115 (33.3%) | 46 (34.1%) | 27 (29.3%) | 22 (37.3%) | 20 (33.9%) | 0.774 | 0.893 |
| >Median | 230 (66.7%) | 89 (65.9%) | 65 (70.7%) | 37 (62.7%) | 39 (66.1%) | ||
| BMI (kg/m2) | 23.9 [20.2; 28.6] | 23.4 [19.8; 26.9] | 24.4 [19.3; 28.7] | 26.0 [21.2; 30.0] | 23.2 [21.7; 26.6] | 0.459 | 0.423 |
| Risk factors | |||||||
| Smoking | 65 (21.2%) | 24 (24.0%) | 19 (21.3%) | 8 (13.6%) | 14 (24.1%) | 0.090 | 0.423 |
| Diabetes | 167 (48.4%) | 70 (51.9%) | 41 (44.6%) | 30 (50.8%) | 26 (44.1%) | 0.710 | 0.671 |
| LDL-C (mg/dL) | 88.0 [63.0; 115] | 88.5 [61.8; 124] | 77.0 [63.0; 100] | 94.0 [70.0; 110] | 92.0 [57.0; 116] | 0.658 | 0.893 |
| Hypertension | 266 (77.1%) | 99 (73.3%) | 63 (68.5%) | 53 (89.8%) | 51 (86.4%) | 0.032 | 0.052 |
| Statin usage | 142 (41.2%) | 37 (27.4%) | 42 (45.7%) | 36 (61.0%) | 27 (45.8%) | 0.001 | 0.007 |
| Comorbidities | |||||||
| CHD | 94 (27.2%) | 42 (31.1%) | 18 (19.6%) | 15 (25.4%) | 19 (32.2%) | 0.468 | 0.962 |
| Heart Failure | 51 (14.8%) | 21 (15.6%) | 12 (13.2%) | 11 (18.6%) | 7 (11.9%) | 0.767 | 0.893 |
| CKD | 176 (51.6%) | 71 (53.4%) | 47 (51.6%) | 33 (55.9%) | 25 (43.1%) | 0.678 | 0.613 |
| Creatinine (mg/dL) | 0.98 [0.73; 1.50] | 1.01 [0.74; 1.63] | 0.98 [0.71; 1.41] | 1.01 [0.78; 1.21] | 0.84 [0.69; 1.41] | 0.678 | 0.423 |
|
eGFR (mL/min/1.73 m2) | 0.459 | 0.423 | |||||
| <30 | 64 (18.8%) | 30 (22.6%) | 17 (18.7%) | 6 (10.2%) | 11 (19.0%) | ||
| 30–60 | 112 (32.8%) | 41 (30.8%) | 30 (33.0%) | 27 (45.8%) | 14 (24.1%) | ||
| >60 | 165 (48.4%) | 62 (46.6%) | 44 (48.4%) | 26 (44.1%) | 33 (56.9%) | ||
| Atrial Fibrillation | 77 (22.3%) | 26 (19.3%) | 18 (19.6%) | 17 (28.8%) | 16 (27.1%) | 0.606 | 0.423 |
| COPD | 36 (10.4%) | 10 (7.41%) | 10 (10.9%) | 5 (8.47%) | 11 (18.6%) | 0.459 | 0.243 |
| Amputation Type | 0.476 | 0.701 | |||||
| Minor | 187 (54.2%) | 71 (52.6%) | 46 (50.0%) | 39 (66.1%) | 31 (52.5%) | ||
| Major | 158 (45.8%) | 64 (47.4%) | 46 (50.0%) | 20 (33.9%) | 28 (47.5%) |
| [ALL] | 2006–2010 | 2011–2015 | 2016–2019 | 2020–2022 | p.overall | p.trend | |
|---|---|---|---|---|---|---|---|
| N = 762 | N = 226 | N = 198 | N = 191 | N = 147 | |||
| Age (years) | 71.4 [63.0; 79.3] | 68.1 [60.1; 76.6] | 71.7 [64.5; 77.9] | 72.3 [63.0; 80.7] | 73.5 [66.0; 81.2] | 0.001 | <0.001 |
| <Median | 438 (57.5%) | 146 (64.6%) | 113 (57.1%) | 105 (55.0%) | 74 (50.3%) | 0.065 | 0.010 |
| >Median | 324 (42.5%) | 80 (35.4%) | 85 (42.9%) | 86 (45.0%) | 73 (49.7%) | ||
| BMI (kg/m2) | 25.1 [22.6; 28.5] | 25.6 [23.1; 28.6] | 24.4 [21.8; 27.7] | 26.6 [23.1; 28.9] | 24.5 [22.3; 29.0] | 0.007 | 0.779 |
| Risk factors | |||||||
| Smoking | 214 (31.0%) | 59 (36.4%) | 64 (33.3%) | 50 (26.2%) | 41 (28.1%) | 0.001 | 0.010 |
| Diabetes | 441 (58.0%) | 154 (68.4%) | 93 (47.0%) | 112 (58.6%) | 82 (55.8%) | 0.001 | 0.098 |
| LDL-C (mg/dL) | 77.0 [57.0; 98.0] | 87.5 [68.0; 107] | 76.5 [53.8; 98.0] | 75.0 [56.8; 95.5] | 70.0 [52.0; 89.0] | 0.001 | <0.001 |
| Hypertension | 590 (77.6%) | 160 (71.4%) | 147 (74.2%) | 155 (81.2%) | 128 (87.1%) | 0.003 | <0.001 |
| Statin usage | 421 (55.2%) | 87 (38.5%) | 116 (58.6%) | 123 (64.4%) | 95 (64.6%) | <0.001 | <0.001 |
| Comorbidities | |||||||
| CHD | 307 (40.3%) | 81 (36.0%) | 63 (31.8%) | 87 (45.5%) | 76 (51.7%) | 0.001 | 0.001 |
| Heart failure | 131 (17.3%) | 38 (17.0%) | 23 (11.6%) | 42 (22.0%) | 28 (19.0%) | 0.075 | 0.261 |
| CKD | 302 (40.3%) | 86 (38.9%) | 87 (44.2%) | 81 (42.9%) | 48 (33.8%) | 0.272 | 0.537 |
| Creatinine (mg/dL) | 1.12 [0.85; 1.65] | 1.10 [0.82; 1.71] | 1.15 [0.88; 1.87] | 1.19 [0.87; 1.59] | 1.04 [0.81; 1.40] | 0.110 | 0.365 |
| eGFR (mL/min/1.73 m2) | 0.385 | 0.261 | |||||
| <30 | 110 (14.7%) | 36 (16.3%) | 33 (16.8%) | 27 (14.3%) | 14 (9.86%) | ||
| 30–60 | 192 (25.6%) | 50 (22.6%) | 54 (27.4%) | 54 (28.6%) | 34 (23.9%) | ||
| >60 | 447 (59.7%) | 135 (61.1%) | 110 (55.8%) | 108 (57.1%) | 94 (66.2%) | ||
| Atrial Fibrillation | 190 (25.0%) | 39 (17.3%) | 44 (22.2%) | 63 (33.2%) | 44 (29.9%) | 0.002 | 0.001 |
| COPD | 141 (18.6%) | 35 (15.6%) | 35 (17.7%) | 41 (21.6%) | 30 (20.5%) | 0.423 | 0.193 |
| Amputation Type | 0.806 | 0.756 | |||||
| Minor | 565 (74.1%) | 169 (74.8%) | 142 (71.7%) | 142 (74.3%) | 112 (76.2%) | ||
| Major | 197 (25.9%) | 57 (25.2%) | 56 (28.3%) | 49 (25.7%) | 35 (23.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaser, S.; Radlinger, B.; Blasinger, J.; Koellenberger, N.; Streitberger, V.; Kopp, L.; Bifano, E.; Aziz, F.; Sourij, H.; Goebel, G.; et al. Non-Traumatic Lower-Limb Amputations: Outcome, Sex-Differences, Comorbidity Patterns and Temporal Trends from 2006 to 2022. J. Clin. Med. 2025, 14, 4030. https://doi.org/10.3390/jcm14124030
Kaser S, Radlinger B, Blasinger J, Koellenberger N, Streitberger V, Kopp L, Bifano E, Aziz F, Sourij H, Goebel G, et al. Non-Traumatic Lower-Limb Amputations: Outcome, Sex-Differences, Comorbidity Patterns and Temporal Trends from 2006 to 2022. Journal of Clinical Medicine. 2025; 14(12):4030. https://doi.org/10.3390/jcm14124030
Chicago/Turabian StyleKaser, Susanne, Bernhard Radlinger, Jana Blasinger, Nicolas Koellenberger, Verena Streitberger, Lena Kopp, Elena Bifano, Faisal Aziz, Harald Sourij, Georg Goebel, and et al. 2025. "Non-Traumatic Lower-Limb Amputations: Outcome, Sex-Differences, Comorbidity Patterns and Temporal Trends from 2006 to 2022" Journal of Clinical Medicine 14, no. 12: 4030. https://doi.org/10.3390/jcm14124030
APA StyleKaser, S., Radlinger, B., Blasinger, J., Koellenberger, N., Streitberger, V., Kopp, L., Bifano, E., Aziz, F., Sourij, H., Goebel, G., & Klocker, J. (2025). Non-Traumatic Lower-Limb Amputations: Outcome, Sex-Differences, Comorbidity Patterns and Temporal Trends from 2006 to 2022. Journal of Clinical Medicine, 14(12), 4030. https://doi.org/10.3390/jcm14124030