
History of an Insidious Case of Metastatic Insulinoma

 , , , and
, , , and
Abstract
1. Introduction
2. Case Description
3. Timeline
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hofland, J.; Falconi, M.; Christ, E.; Castaño, J.P.; Faggiano, A.; Lamarca, A.; Perren, A.; Petrucci, S.; Prasad, V.; Ruszniewski, P.; et al. European Neuroendocrine Tumor Society 2023 Guidance Paper for Functioning Pancreatic Neuroendocrine Tumour Syndromes. J. Neuroendocrinol. 2023, 35, e13318. [Google Scholar] [CrossRef]
- Sada, A.; Glasgow, A.E.; Vella, A.; Thompson, G.B.; McKenzie, T.J.; Habermann, E.B. Malignant Insulinoma: A Rare Form of Neuroendocrine Tumor. World J. Surg. 2020, 44, 2288–2294. [Google Scholar] [CrossRef]
- Maggio, I.; Mollica, V.; Brighi, N.; Lamberti, G.; Manuzzi, L.; Ricci, A.D.; Campana, D. The Functioning Side of the Pancreas: A Review on Insulinomas. J. Endocrinol. Investig. 2020, 43, 139–148. [Google Scholar] [CrossRef] [PubMed]
- De Herder, W.W. Insulinoma. Neuroendocrinology 2004, 80, 20–22. [Google Scholar] [CrossRef]
- Shin, J.J.; Gorden, P.; Libutti, S.K. Insulinoma: Pathophysiology, Localization and Management. Future Oncol. 2010, 6, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Mehrabi, A.; Fischer, L.; Hafezi, M.; Dirlewanger, A.; Grenacher, L.; Diener, M.K.; Fonouni, H.; Golriz, M.; Garoussi, C.; Fard, N.; et al. A Systematic Review of Localization, Surgical Treatment Options, and Outcome of Insulinoma. Pancreas 2014, 43, 675–686. [Google Scholar] [CrossRef]
- Anderson, C.W.; Bennett, J.J. Clinical Presentation and Diagnosis of Pancreatic Neuroendocrine Tumors. Surg. Oncol. Clin. N. Am. 2016, 25, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Okabayashi, T.; Shima, Y.; Sumiyoshi, T.; Kozuki, A.; Ito, S.; Ogawa, Y.; Kobayashi, M.; Hanazaki, K. Diagnosis and Management of Insulinoma. World J. Gastroenterol. 2013, 19, 829–837. [Google Scholar] [CrossRef]
- Di Martino, M.; García Sanz, I.; Delgado Valdueza, J.; Martín-Pérez, E. Giant Malignant Insulinoma. J. Gastrointest. Surg. 2016, 20, 1530–1531. [Google Scholar] [CrossRef]
- O’Toole, D.; Abbasakoor, N.O.; Healy, M.L.; O’Shea, D.; Maguire, D.; Muldoon, C.; Sheahan, K. Metastatic Insulinoma in a Patient with Type 2 Diabetes Mellitus: Case Report and Review of the Literature. Int. J. Endocrinol. 2011, 2011, 124078. [Google Scholar] [CrossRef]
- Mathur, A.; Gorden, P.; Libutti, S.K. Insulinoma. Surg. Clin. N. Am. 2009, 89, 1105–1121. [Google Scholar] [CrossRef]
- Hirshberg, B.; Cochran, C.; Skarulis, M.C.; Libutti, S.K.; Alexander, H.R.; Wood, B.J.; Chang, R.; Kleiner, D.E.; Gorden, P. Malignant Insulinoma: Spectrum of Unusual Clinical Features. Cancer 2005, 104, 264–272. [Google Scholar] [CrossRef]
- Sada, A.; Yamashita, T.S.; Glasgow, A.E.; Habermann, E.B.; Thompson, G.B.; Lyden, M.L.; Dy, B.M.; Halfdanarson, T.R.; Vella, A.; McKenzie, T.J. Comparison of Benign and Malignant Insulinoma. Am. J. Surg. 2021, 221, 437–447. [Google Scholar] [CrossRef]
- De Herder, W.W.; Van Schaik, E.; Kwekkeboom, D.; Feelders, R.A. New Therapeutic Options for Metastatic Malignant Insulinomas. Clin. Endocrinol. 2011, 75, 277–284. [Google Scholar] [CrossRef]
- Moris, D.; Giannis, D.; Karachaliou, G.-S.; Tsilimigras, D.I.; Karaolanis, G.; Papalampros, A.; Felekouras, E. Insulinomas: From Diagnosis to Treatment. A Review of the Literature. JBUON 2020, 25, 1302–1314. [Google Scholar]
- Brown, E.; Watkin, D.; Evans, J.; Yip, V.; Cuthbertson, D.J. Multidisciplinary Management of Refractory Insulinomas. Clin. Endocrinol. 2018, 88, 615–624. [Google Scholar] [CrossRef]
- Gursan, N.; Yildirgan, M.I.; Atamanalp, S.S.; Sahin, O.; Gursan, M.S. Solid Pseudopapillary Tumor of the Pancreas. Eurasian J. Med. 2009, 41, 129–132. [Google Scholar]
- Galvin, A.; Sutherland, T.; Little, A.F. Part 1: CT Characterisation of Pancreatic Neoplasms: A Pictorial Essay. Insights Imaging 2011, 2, 379–388. [Google Scholar] [CrossRef]
- Service, F.J.; McMahon, M.M.; O’Brien, P.C.; Ballard, D.J. Functioning Insulinoma—Incidence, Recurrence, and Long-Term Survival of Patients: A 60-Year Study. Mayo Clin. Proc. 1991, 66, 711–719. [Google Scholar] [CrossRef]
- Zhang, J.; Jiang, R.; Hong, X.; Wu, H.; Han, X.; Wu, W. Metastatic Insulinoma: Exploration from Clinicopathological Signatures and Genetic Characteristics. Front. Oncol. 2023, 13, 1109330. [Google Scholar] [CrossRef]
- Yu, J.; Ping, F.; Zhang, H.; Li, W.; Yuan, T.; Fu, Y.; Feng, K.; Xia, W.; Xu, L.; Li, Y. Clinical Management of Malignant Insulinoma: A Single Institution’s Experience over Three Decades. BMC Endocr. Disord. 2018, 18, 92. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Saldarriaga, C.; Builes-Montaño, C.E.; Arango-Toro, C.M.; Manotas-Echeverry, C.; Pérez-Cadavid, J.C.; Álvarez-Payares, J.C.; Rodríguez-Arrieta, L.A. Insulinoma-Related Endogenous Hypoglycaemia with a Negative Fasting Test: A Case Report and Literature Review. Eur. J. Case Rep. Intern. Med. 2022, 9, 65–68. [Google Scholar] [CrossRef]
- D’alessandro, M.; Mariani, P.; Lomanto, D.; Carlei, F.; Lezoche, E.; Speranza, V. Serum Neuron-Specific Enolase in Diagnosis and Follow-Up of Gastrointestinal Neuroendocrine Tumors. Tumor Biol. 1992, 13, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Iwase, K.; Kato, K.; Nagasaka, A.; Miura, K.; Kawase, K.; Miyakawa, S.; Tei, T.; Ohtani, S.; Inagaki, M.; Shinoda, S.; et al. Immunohistochemical Study of Neuron-Specific Enolase and CA 19-9 in Pancreatic Disorders. The Value of Neuron-Specific Enolase as a Marker for Islet Cell and Nerve Tissue. Gastroenterology 1986, 91, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Magi, L.; Marasco, M.; Rinzivillo, M.; Faggiano, A.; Panzuto, F. Management of Functional Pancreatic Neuroendocrine Neoplasms. Curr. Treat. Options Oncol. 2023, 24, 725–741. [Google Scholar] [CrossRef]
- Polowczyk, B.; Kaluzny, M.; Bolanowski, M. Somatostatin Analogues in the Therapy of Neuroendocrine Tumors: Indications, Contraindications, Side-Effects. Postep. Hig. Med. Dosw. 2020, 74, 271–281. [Google Scholar] [CrossRef]
- Kos-Kudła, B.; Ćwikła, J.; Jarząb, B.; Jeziorski, K.; Królicki, L.; Krzakowski, M.; Nasierowska-Guttmejer, A.; Rydzewska, G.; Stachura, J.; Szawłowski, A. Polish Recommendation for Diagnosis and Treatment of Gastroenteropancreatic Tumors (GEP NET). Oncol. Clin. Pract. 2006, 2, 73–78. [Google Scholar]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177 Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Iglesias, P.; Martínez, A.; Gajate, P.; Alonso, T.; Navarro, T.; Díez, J.J. Long-Term Effect of 177Lu-Dotatate on Severe and Refractory Hypoglycemia Associated with Malignant Insulinoma. AACE Clin. Case Rep. 2019, 5, e330–e333. [Google Scholar] [CrossRef]
- Costa, R.; Costa, R.; Bacchi, C.E.; Almeida Filho, P. Metastatic Insulinoma Managed with Radiolabeled Somatostatin Analog. Case Rep. Endocrinol. 2013, 2013, 252159. [Google Scholar] [CrossRef]
- Makis, W.; Mccann, K.; Mcewan, A.J.B. Metastatic Insulinoma Pancreatic Neuroendocrine Tumor Treated with 177Lu-DOTATATE Induction and Maintenance Peptide Receptor Radionuclide Therapy: A Suggested Protocol. Clin. Nucl. Med. 2016, 41, 53–54. [Google Scholar] [CrossRef]
- Novruzov, F.; Mehmetbeyli, L.; Aliyev, J.A.; Abbasov, B.; Mehdi, E. Metastatic Insulinoma Controlled by Targeted Radionuclide Therapy with 177Lu-DOTATATE in a Patient with Solitary Kidney and MEN-1 Syndrome. Clin. Nucl. Med. 2019, 44, E415–E417. [Google Scholar] [CrossRef]
- Di Franco, M.; Fortunati, E.; Zanoni, L.; Fanti, S.; Ambrosini, V. The Role of Combined FDG and SST PET/CT in Neuroendocrine Tumors. J. Neuroendocrinol. 2025, 37, e13474. [Google Scholar] [CrossRef]
- Chan, D.L.; Hayes, A.R.; Karfis, I.; Conner, A.; Furtado O’Mahony, L.; Mileva, M.; Bernard, E.; Roach, P.; Marin, G.; Pavlakis, N.; et al. Dual [68Ga]DOTATATE and [18F]FDG PET/CT in Patients with Metastatic Gastroenteropancreatic Neuroendocrine Neoplasms: A Multicentre Validation of the NETPET Score. Br. J. Cancer 2023, 128, 549–555. [Google Scholar] [CrossRef]
- Zalewska, E.; Kłosowski, P.; Dubowik, M.; Pȩksa, R.; Sworczak, K. Endoscopic Ultrasound-Guided Ethanol Ablation of Insulinoma. Endokrynol. Pol. 2020, 71, 585–586. [Google Scholar] [CrossRef]
- Kim, D.; Viswanathan, K.; Goyal, A.; Rao, R. Insulinoma-Associated Protein 1 (INSM1) Is a Robust Marker for Identifying and Grading Pancreatic Neuroendocrine Tumors. Cancer Cytopathol. 2020, 128, 269–277. [Google Scholar] [CrossRef]
- Guan, Y.; Sun, Y.; Liu, Z.; Zhang, Y.; Cao, M.; Wang, W.; Tao, J.; Yao, Y. INSM1 Promotes Breast Carcinogenesis by Regulating C-MYC. Am. J. Cancer Res. 2023, 13, 3500–3516. [Google Scholar]
- Razvi, H.; Tsang, J.Y.; Poon, I.K.; Chan, S.K.; Cheung, S.Y.; Shea, K.H.; Tse, G.M. INSM1 Is a Novel Prognostic Neuroendocrine Marker for Luminal B Breast Cancer. Pathology 2021, 53, 170–178. [Google Scholar] [CrossRef]
- Hesdorffer, C.S.; Stoopler, M.; Javitch, J. Aggressive Insulinoma with Bone Metastases. Am. J. Clin. Oncol. 1989, 12, 498–501. [Google Scholar] [CrossRef]
- Libutti, S.; Taye, A. Diagnosis and Management of Insulinoma: Current Best Practice and Ongoing Developments. Res. Rep. Endocr. Disord. 2015, 5, 125–133. [Google Scholar] [CrossRef]
- Lewicki, M.; Urbanczuk, M.; Zwolak, A.; Dudzinska, M.; Lenart-Lipinska, M.; Tarach, J.S. Insulinoma- from Diagnosis to Full Recovery. Case Study. Endocr. Abstr. 2017, 49, EP144. [Google Scholar] [CrossRef]
- Yu, Z.; Wang, Y.; Sun, Y.; Wang, Y.; Tian, Y.; Ma, Q.; Fu, Y. Case Report: Insulinoma Presenting as Excessive Daytime Somnolence. Front. Endocrinol. 2021, 12, 712392. [Google Scholar] [CrossRef]
- Oziel-Taieb, S.; Maniry-Quellier, J.; Chanez, B.; Poizat, F.; Ewald, J.; Niccoli, P. Pasireotide for Refractory Hypoglycemia in Malignant Insulinoma- Case Report and Review of the Literature. Front. Endocrinol. 2022, 13, 860614. [Google Scholar] [CrossRef]
- Williams, B.A.; Lampart, S.; Metzger, J.; Fischli, S. Case Report of a Pancreatic Insulinoma Misdiagnosed as Epilepsy. BMJ Case Rep. 2021, 14, 2020–2022. [Google Scholar] [CrossRef]
- Vinhosa Bastos, M.A.; da Silva Caires, I.; Boschi Portella, R.; Nascimento Martins, R.; Reverdito, R.; Reverdito, S.; Moro, N. Insulinoma with Peripheral Neuropathy: A Case Report. J. Med. Case Rep. 2023, 17, 241. [Google Scholar] [CrossRef]
- AlKhamisy, A.; Nasani, M. A Rare Case of Insulinoma Presented with Neurological Manifestations: A Case Report. Int. J. Surg. Case Rep. 2023, 108, 108397. [Google Scholar] [CrossRef]
- Topaloglu, O.; Sendur, M.A.; Dumlu, G.; Yildirim, F.; Taskaldiran, I.; Soydal, C.; Ersoy, R.; Cakir, B. Case Report: Management of a Patient with Malignant Insulinoma. Endocr. Abstr. 2018, 56, EP9. [Google Scholar] [CrossRef]
- Nashidengo, P.R.; Quayson, F.W.; Abebrese, J.T.; Negumbo, L.; Enssle, C.; Kidaaga, F. Varied Presentations of Pancreatic Insulinoma: A Case Report. Pan Afr. Med. J. 2022, 42, 69. [Google Scholar] [CrossRef]
- Amiri, F.; Moradi, L. Pancreatic Insulinoma: Case Report and Review of the Literature. Clin. Case Rep. Rev. 2018, 4, 377–379. [Google Scholar] [CrossRef]
- Tarris, G.; Rouland, A.; Guillen, K.; Loffroy, R.; Lariotte, A.C.; Rat, P.; Bouillet, B.; Andrianiaina, H.; Petit, J.M.; Martin, L. Case Report: Giant Insulinoma, a Very Rare Tumor Causing Hypoglycemia. Front. Endocrinol. 2023, 14, 1125772. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Test | Outcome |
|---|---|
| Vimentin Ab2 | +/− |
| Cytokeratin Clone AE1/AE3 | − |
| Cytokeratin 7 | − |
| Chromogranin A | + |
| Neuron-Specific Enolase (NSE) | + |
| Synaptophysin | + |
| Marker | Result | Normal Range |
|---|---|---|
| Chromatogranin A | 43.2 µg/dL | 0–100 µg/dL |
| Gastrin | 69.7 pg/mL | 13–115 pg/mL |
| NSE | 13.3 µg/dL | 0–18.3 µg/dL |
| Calcitonin | 104 pg/mL | 0–11.5 pg/mL |
| 0 min. | 30 min. | 60 min. | 120 min. | 180 min. | 240 min. | |
|---|---|---|---|---|---|---|
| Glucose (mg/dL) | 124 (N: 70–99) | 217 | 260 | 373 | 299 | 189 |
| Insulin (μIU/mL) | 2 (N: <29) | 3.52 | 2 | 5.95 | 11.2 | 75.1 |
| Blood Test | Result |
|---|---|
| Glucose | 33 mg/dL |
| Insulin | 27.1 μIU/mL |
| C-peptide | 6.8 ng/mL |
| 0 min. | 60 min. | 120 min. | 180 min. | 240 min | |
|---|---|---|---|---|---|
| Glucose mg/dL | 160 | 137 | 158 | 143 | 133 |
| Insulin μIU/mL | <2 | <2 | <2 | <2 | <2 |
| Result | Normal Range | |
|---|---|---|
| Chromogranin A | 337.3 µg/dL | <100 µg/dL |
| NSE | 75.85 ng/dL | <18.3 ng/dL |
| 5HIAA | 7.15 mg/24 h | 2–9 mg/24 h |
| Ki67 | Synaptophysin | Chromogranin A | |
|---|---|---|---|
| Left side | 30% | + | + |
| Right side | 50% | + | + |
| Date | Event |
|---|---|
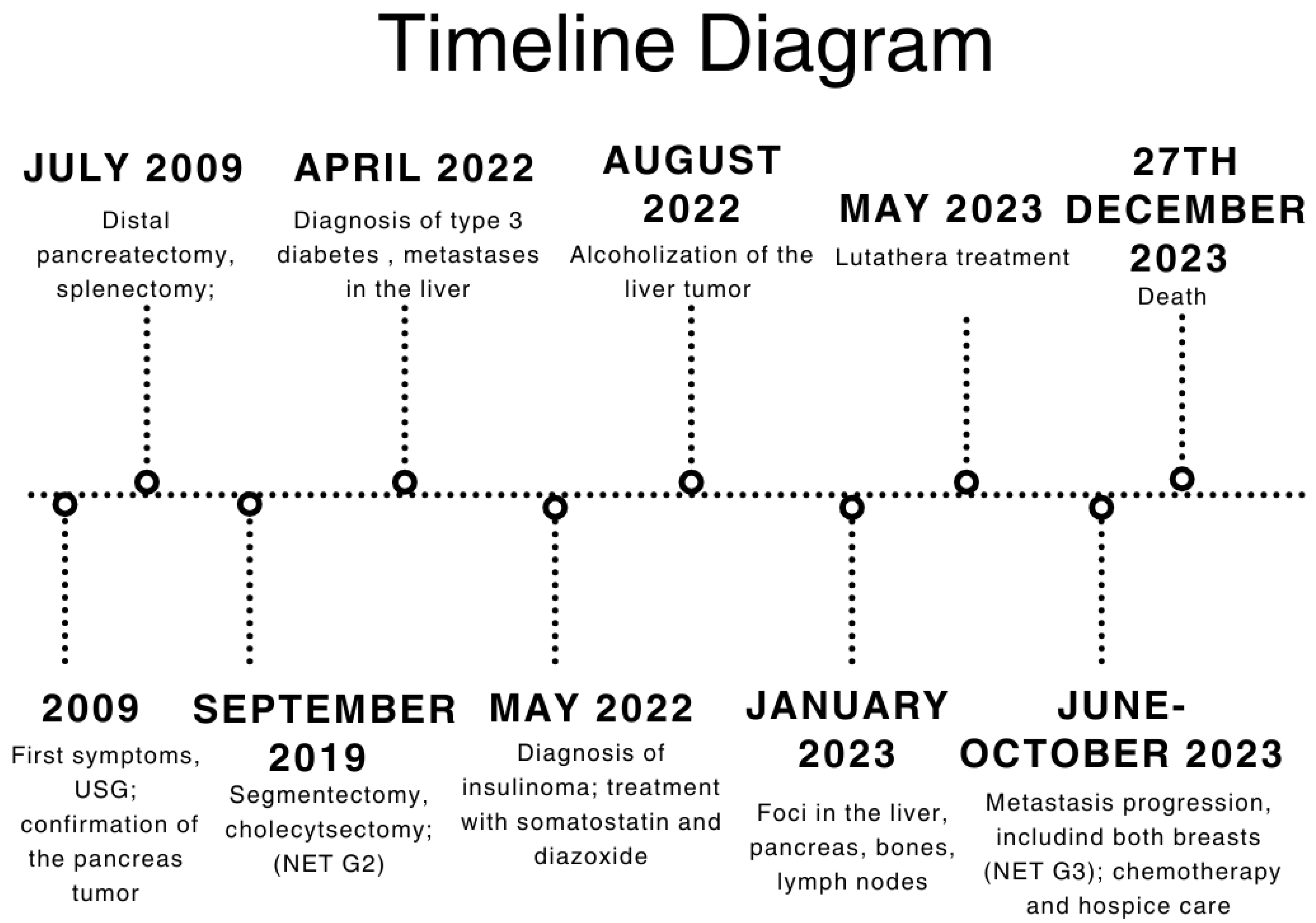
| 2009 | First symptoms: abdominal pain; pancreatic tumor confirmed in USG examination |
| July 2009 | Distal pancreatectomy with splenectomy; histopathological exam: solid pseudopapillary tumor of the pancreas |
| September 2019 | Segmentectomy (S5-S4b) with cholecystectomy with the histopathological recognition of neuroendocrine tumor (NET) metastasis to the liver characterized as NET G2, Ki67—5% |
| January 2022 | Short episode of loss of consciousness with convulsion due to hypoglycemia; repeated states of hypoglycemia—hospitalization at the Neurology Department in Wroclaw |
| April 2022 | Diagnostic at the Department of Endocrinology, Diabetes and Isotope Therapy in Wrocław—72 h fasting test excluding insulinoma; diagnosis of type 3 diabetes; metastatic process found in the liver in PET-FDG |
| May 2022 | Persistent hypoglycemia with elevated insulin and C-peptide levels → diagnosis of insulinoma; start of treatment using somatostatin and diazoxide; metastatic tumor in segment I of the liver confirmed in MRI |
| June 2022 | EUS with hepatic biopsy → NET with higher malignancy, G2/G3, Ki67—up to 20%. |
| August 2022 | Median upper relaparotomy with alcoholization of the liver tumor |
| November 2022 | Follow-up CT showing new metastases in S2, S3, and S6 of the liver |
| January 2023 | Follow-up PET showing foci in the liver, head of the pancreas, bones, and cervical lymph nodes |
| May 2023 | Beginning of Lutathera treatment CT scan: metastases in the liver, bone sclerosis, enlarged lymph nodes |
| June 2023 | Administration of continuous glucose monitoring with FSM Breast ultrasound and mammography: lesion found in both of the mammary glands (right breast—BIRADS4; left breast—BIRADS2) |
| July and August 2023 | Biopsy of the mammary glands: metastases with high proliferation markers (triple negative malignant neoplasm) NET G3, Ki67—30% for left breast and 50% for right breast Administration of a second dose of Lutathera |
| October 2023 | Significant progression of metastases in the liver and bones (spine, ribs, pelvis), and periaortic and pelvic lymphadenopathy The patient was referred to palliative hospice care, resigned from further PRPRT treatment |
| November 2023 | Chemotherapy with temozolomide—I cycle |
| 27 December 2023 | Patient died |
| Similar Cases | |||||
|---|---|---|---|---|---|
| Patient Data | Symptoms | Type of Treatment | Effect of Treatment | Citation | |
| 1 | A 16-year-old male, South America |
| Surgical treatment—enucleation of the tumor. No metastases were detected. | The patient feels a significant improvement in his condition.The symptoms have completely disappeared. | [45] |
| 2 | A 47-year-old female, Asia |
| Surgical treatment—laparoscopic partial distal pancreatectomy. No metastases were detected. | Three months after surgery, the patient reported feeling well, and follow-up tests (glucose, insulin, C-peptide) showed normal results. | [46] |
| 3 | A 41-year-old female, Europe |
| Surgical treatment—distal pancreatectomy and splenectomy. Pharmacological treatment:
Hepatic and lymph node metastases have been reported. Tumor infiltration of the perihilar tissues was found. | The patient experienced respiratory distress likely due to infection or drug-associated pneumonitis. She developed acute respiratory distress syndrome. Unfortunately, she died three months after the initial diagnosis due to ARDS. | [47] |
| 4 | A 26-year-old female, Africa |
| Surgical treatment—enucleation of the tumor. No metastases were detected. | Following the surgery, the patient had a full recovery. The patient no longer experienced symptoms such as fatigue, increased appetite, seizures, or loss of consciousness. | [48] |
| 5 | A 43-year-old female, Asia |
| Surgical treatment—enucleation of the tumor. No metastases were detected. | After the surgical treatment, her glucose levels rose to the diabetic range, suggesting that the hypoglycemic symptoms were effectively managed. | [49] |
| 6 | A 38-year-old female, Europe |
| Surgical treatment—laparoscopic partial distal pancreatectomy. Pharmacological treatment:
| After surgery, the patient’s insulin, proinsulin, C-peptide, and glucose levels returned to normal. After 16 months, the patient had lost 4.2 kg and did not report any specific complaints. | [50] |
| 7 | A 53-year-old male, Europe |
| Surgical treatment—removal of the tumor. No metastases were detected. | After the surgery, all symptoms subsided, and the patient did not require any additional treatment. | [41] |
| 8 | A 14-year-old female, Asia |
| Surgical treatment—laparoscopic partial distal pancreatectomy. No metastases were detected. | Symptoms improved significantly, including the disappearance of daytime sleepiness and abnormal behavior during sleep. The patient’s blood glucose levels normalized. | [42] |
| 9 | A 64-year-old female, Europe |
| Pharmacological treatment:
| Patient’s glycemic control improved significantly, and hypoglycemic episodes became much less frequent and severe. Blood glucose levels were completely normalized for over 18 months, resulting in a significant improvement in her quality of life. | [43] |
| 10 | A 55-year-old female, Europe |
| Surgical treatment—removal of the tumor. Pharmacological treatment:
| Postoperatively, the patient’s glucose level and insulin regulation normalized, leading to an overall improvement in her health. | [44] |
| 11 | A 65-year-old male, South America |
| Surgical treatment—Subtotal pancreatectomy (90%) with splenectomy. No metastases were detected. | Improvement in glucose control after surgery. Initial postoperative hyperglycemia managed with insulin | [22] |
| 12 | A 54-year-old male, Asia |
| Pharmacological treatment:
| After treatment, the size and activity of the lesions decreased. Hypoglycemic episodes, which previously occurred daily, decreased to 1 episode per year during a 1-year follow-up. | [32] |
| 13 | A 72-year-old female, Europe |
| EUS-guided ethanol ablation (two sessions). No metastases were detected. | After the first session, partial improvement was observed: hypoglycemic episodes occurred less frequently, and the symptoms were milder. After the second session, the treatment appeared to be fully effective, with no hypoglycemic episodes for five months. Adverse effects: mild abdominal pain on the day of the procedure and a transient six-fold elevation of lipase activity, which normalized within 72 h. | [35] |
| 14 | A 60-year-old male, North America |
| Pharmacological treatment:
Metastatic lesion was demonstrated in the liver and bones. | Despite the treatment administered, hypoglycemic symptoms progressed. Sepsis appeared. The patient died after 11 months of diagnosis. | [39] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antosz-Popiołek, K.; Koga-Batko, J.; Suchecki, W.; Stopa, M.; Zawadzka, K.; Hajac, Ł.; Bolanowski, M.; Jawiarczyk-Przybyłowska, A. History of an Insidious Case of Metastatic Insulinoma. J. Clin. Med. 2025, 14, 4028. https://doi.org/10.3390/jcm14124028
Antosz-Popiołek K, Koga-Batko J, Suchecki W, Stopa M, Zawadzka K, Hajac Ł, Bolanowski M, Jawiarczyk-Przybyłowska A. History of an Insidious Case of Metastatic Insulinoma. Journal of Clinical Medicine. 2025; 14(12):4028. https://doi.org/10.3390/jcm14124028
Chicago/Turabian StyleAntosz-Popiołek, Katarzyna, Joanna Koga-Batko, Wojciech Suchecki, Małgorzata Stopa, Katarzyna Zawadzka, Łukasz Hajac, Marek Bolanowski, and Aleksandra Jawiarczyk-Przybyłowska. 2025. "History of an Insidious Case of Metastatic Insulinoma" Journal of Clinical Medicine 14, no. 12: 4028. https://doi.org/10.3390/jcm14124028
APA StyleAntosz-Popiołek, K., Koga-Batko, J., Suchecki, W., Stopa, M., Zawadzka, K., Hajac, Ł., Bolanowski, M., & Jawiarczyk-Przybyłowska, A. (2025). History of an Insidious Case of Metastatic Insulinoma. Journal of Clinical Medicine, 14(12), 4028. https://doi.org/10.3390/jcm14124028