
Comparison of Hidden Blood Loss in Biportal Endoscopic Spine Surgery and Open Surgery in the Lumbar Spine: A Retrospective Multicenter Study
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
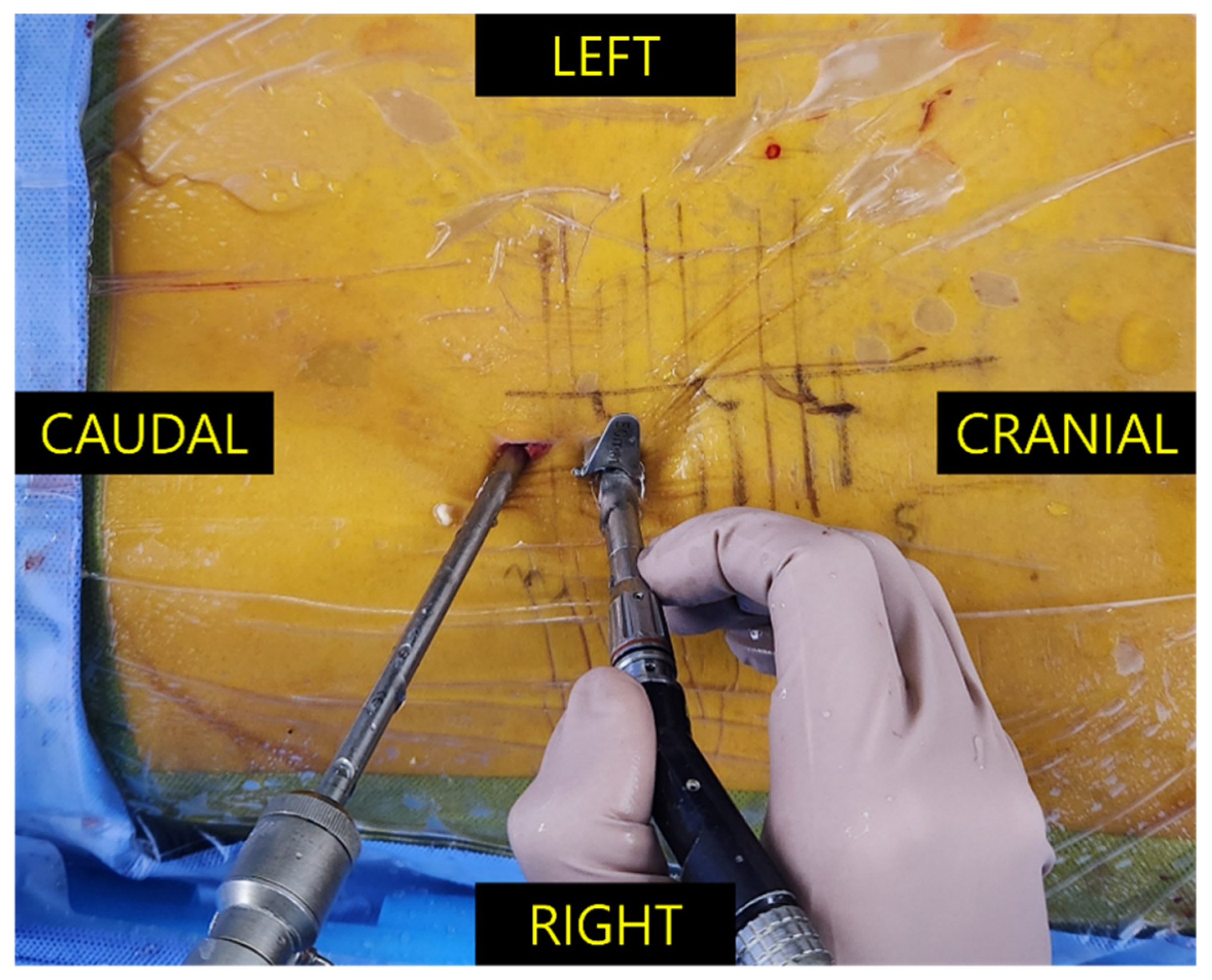
2.2. Surgical Technique
2.2.1. Biportal Endoscopic Spine Surgery (BESS) Group
2.2.2. Open Surgery Group
2.3. Data Collection
2.4. Calculation of Blood Loss
- Men: PBV (liter) = (0.3669 × H3) + (0.03219 × W) + 0.6041;
- Women: PBV = (0.3561 × H3) + (0.03308 × W) + 0.1833;
- H: height (meter); W: weight (kilogram).
- TBL (liter) = PBV × (Hctpre − Hctpost)/Hctave;
- Hctpre: preoperative hematocrit level;
- Hctpost: postoperative lowest hematocrit level;
- Hctave: average of the Hctpre and Hctpost.
- HBL = TBL − VBL;
- VBL = intraoperative bleeding + postoperative drainage.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BESS | Biportal endoscopic spine surgery |
| VBL | Visible blood loss |
| HBL | Hidden blood loss |
| TBL | Total blood loss |
| Hct | Hematocrit |
| MISS | Minimally invasive spine surgery |
| HNP | Herniation of nucleus pulposus |
| PBV | Predicted blood volume |
| FESS | Full endoscopic spine surgery |
| UBE | Unilateral biportal endoscopy |
References
- Hofstetter, C.P.; Ahn, Y.; Choi, G.; Gibson, J.N.A.; Ruetten, S.; Zhou, Y.; Li, Z.Z.; Siepe, C.J.; Wagner, R.; Lee, J.H.; et al. AOSpine Consensus Paper on Nomenclature for Working-Channel Endoscopic Spinal Procedures. Global Spine J. 2020, 10, 111S–121S. [Google Scholar] [CrossRef] [PubMed]
- Junjie, L.; Jiheng, Y.; Jun, L.; Haixiong, L.; Haifeng, Y. Comparison of Unilateral Biportal Endoscopy Decompression and Microscopic Decompression Effectiveness in Lumbar Spinal Stenosis Treatment: A Systematic Review and Meta-analysis. Asian Spine J. 2023, 17, 418–430. [Google Scholar] [CrossRef] [PubMed]
- Min, W.K.; Kim, J.E.; Choi, D.J.; Park, E.J.; Heo, J. Clinical and radiological outcomes between biportal endoscopic decompression and microscopic decompression in lumbar spinal stenosis. J. Orthop. Sci. 2020, 25, 371–378. [Google Scholar] [CrossRef]
- Wang, H.; Wang, K.; Lv, B.; Li, W.; Fan, T.; Zhao, J.; Kang, M.; Dong, R.; Qu, Y. Analysis of risk factors for perioperative hidden blood loss in unilateral biportal endoscopic spine surgery: A retrospective multicenter study. J. Orthop. Surg. Res. 2021, 16, 559. [Google Scholar] [CrossRef]
- Sehat, K.R.; Evans, R.; Newman, J.H. How much blood is really lost in total knee arthroplasty?. Correct blood loss management should take hidden loss into account. Knee 2000, 7, 151–155. [Google Scholar] [CrossRef]
- Elgafy, H.; Bransford, R.J.; McGuire, R.A.; Dettori, J.R.; Fischer, D. Blood loss in major spine surgery: Are there effective measures to decrease massive hemorrhage in major spine fusion surgery? Spine 2010, 35, S47–S56. [Google Scholar] [CrossRef]
- Zhou, Y.; Fu, X.; Yang, M.; Ke, S.; Wang, B.; Li, Z. Hidden blood loss and its possible risk factors in minimally invasive transforaminal lumbar interbody fusion. J. Orthop. Surg. Res. 2020, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Yu, Z.; Wang, C.; Zhong, M.; Wang, R.; Hu, Y.; Wang, C.; Li, S. Risk Factors of Hidden Blood Loss in Unilateral Biportal Endoscopic Surgery for Patients with Lumbar Spinal Stenosis. Orthop. Surg. 2024, 16, 842–850. [Google Scholar] [CrossRef]
- Ogura, Y.; Dimar Ii, J.R.; Gum, J.L.; Crawford, C.H., 3rd; Djurasovic, M.; Glassman, S.D.; Carreon, L.Y. Hidden blood loss following 2- to 3-level posterior lumbar fusion. Spine J. 2019, 19, 2003–2006. [Google Scholar] [CrossRef]
- Ge, Z.; Zhao, W.; Wu, Z.; He, J.; Zhu, G.; Song, Z.; Cui, J.; Jiang, X.; Yu, W. Hidden Blood Loss and Its Possible Risk Factors in Full Endoscopic Lumbar Interbody Fusion. J. Pers. Med. 2023, 13, 674. [Google Scholar] [CrossRef]
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar] [PubMed]
- Gross, J.B. Estimating allowable blood loss: Corrected for dilution. Anesthesiology 1983, 58, 277–280. [Google Scholar] [CrossRef]
- Jiang, H.W.; Chen, C.D.; Zhan, B.S.; Wang, Y.L.; Tang, P.; Jiang, X.S. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: A retrospective study. J. Orthop. Surg. Res. 2022, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Li, J.; Guo, S.; An, N.; Fan, Z.; Tan, H.; Lin, J.; Su, N.; Yang, Y.; Fei, Q.; et al. Hidden blood loss in three different endoscopic spinal procedures for lumbar disc herniation. Ann. Med. Surg. 2024, 86, 655–659. [Google Scholar] [CrossRef]
- Lotke, P.A.; Faralli, V.J.; Orenstein, E.M.; Ecker, M.L. Blood loss after total knee replacement. Effects of tourniquet release and continuous passive motion. J. Bone Jt. Surg. Am. Vol. 1991, 73, 1037–1040. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, L.; Shan, Y.; Feng, X.; Zhang, W. Analysis of Hidden Blood Loss and its Risk Factors in Oblique Lateral Interbody Fusion Surgery. Clin. Spine Surg. 2021, 34, E501–E505. [Google Scholar] [CrossRef]
- Mima, Y.; Yagi, M.; Suzuki, S.; Tsuji, O.; Nagoshi, N.; Okada, E.; Fujita, N.; Nakamura, M.; Matsumoto, M.; Watanabe, K. Hidden blood loss in extreme lateral interbody fusion for adult spinal deformity. J. Orthop. Sci. 2023, 28, 509–514. [Google Scholar] [CrossRef]
- Li, Y.; Ge, M.; Tian, J.; Zhou, J.; Kang, Y.; Xia, C.; Shao, H.; Wang, Y.; Huang, Y.; Zhao, T. Effect of Tranexamic Acid on Hidden Blood Loss in Percutaneous Endoscopic Transforaminal Lumbar Interbody Fusion: A Retrospective Study. Ther. Clin. Risk Manag. 2024, 20, 325–334. [Google Scholar] [CrossRef]
- Xu, D.; Ren, Z.; Chen, X.; Zhuang, Q.; Hui, S.; Sheng, L.; Li, S. The further exploration of hidden blood loss in posterior lumbar fusion surgery. Orthop. Traumatol. Surg. Res. 2017, 103, 527–530. [Google Scholar] [CrossRef]
- Dai, Z.; Feng, D.P.; Wu, K.L.; Zhu, J.Y.; Li, Z.W. Hidden blood loss of minimally invasive hybrid lumbar interbody fusion: An analysis of influencing factors. BMC Musculoskelet. Disord. 2022, 23, 1099. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahn, Y. Percutaneous endoscopic decompression for lumbar spinal stenosis. Expert Rev. Med. Devices 2014, 11, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.M.; Chung, J.T.; Lee, S.J.; Choi, D.J. How I do it? Biportal endoscopic spinal surgery (BESS) for treatment of lumbar spinal stenosis. Acta Neurochir. 2016, 158, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Park, C.K. Uni-portal and Bi-portal Techniques in Endoscopic Lumbar Spine Surgery: Their Reciprocal Relations. J. Minim. Invasive Spine Surg. Tech. 2021, 6, S75–S76. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Total (n = 88) | BESS Group (n = 66) | Open Surgery Group (n = 17) | p-Value |
|---|---|---|---|---|
| Age (years) | 65.11 ± 13.86 | 66.64 ± 14.18 | 59.18 ± 10.98 | 0.007 |
| Gender | 0.484 | |||
| Male | 50 (60.2) | 38 (57.6) | 12 (70.6) | |
| Female | 33 (39.8) | 28 (42.4) | 5 (29.4) | |
| Height | 1.63 ± 0.09 | 1.63 ± 0.10 | 1.66 ± 0.06 | 0.054 |
| Weight | 66.71 ± 13.77 | 66.58 ± 14.65 | 67.21 ± 10.00 | 0.534 |
| BMI | 24.84 ± 3.79 | 24.99 ± 3.99 | 24.23 ± 2.91 | 0.461 |
| Smoking | 0.228 | |||
| No | 69 (83.1) | 61 (92.4) | 9 (52.9) | |
| Yes | 7 (8.4) | 5 (7.6) | 2 (11.8) | |
| Anticoagulant agent usage | 0.004 | |||
| No | 58 (69.9) | 42 (63.6) | 16 (94.1) | |
| Yes | 24 (28.9) | 24 (36.4) | 0 (0.0) | |
| Diagnosis | 0.089 | |||
| CS | 36 (43.4) | 32 (48.5) | 4 (23.5) | |
| CS and FS and HNP | 1 (1.2) | 1 (1.5) | 0 (0.0) | |
| CS and HNP | 5 (6.0) | 5 (7.6) | 0 (0.0) | |
| CS and isthmic SPL | 1 (1.2) | 1 (1.5) | 0 (0.0) | |
| FS | 4 (4.8) | 4 (6.1) | 0 (0.0) | |
| FS and isthmic SPL | 2 (2.4) | 2 (3.0) | 0 (0.0) | |
| HNP | 33 (39.8) | 20 (30.3) | 13 (76.5) | |
| Facet cyst | 1 (1.2) | 1 (1.5) | 0 (0.0) | |
| Operative type | 0.022 | |||
| Decompression (unilateral decompression) | 7 (8.4) | 6 (9.1) | 1 (5.9) | |
| Decompression (bilateral, ULBD) | 36 (43.4) | 32 (48.5) | 4 (23.5) | |
| Decompression (bilateral, ULBD) and discectomy | 8 (9.6) | 8 (12.1) | 0 (0.0) | |
| Discectomy | 32 (38.6) | 20 (30.3) | 12 (70.6) | |
| Index level | 0.650 | |||
| L1–2 | 1 (1.2) | 1 (1.5) | 0 (0.0) | |
| L2–3 | 7 (8.4) | 7 (10.6) | 0 (0.0) | |
| L3–4 | 19 (22.9) | 16 (24.2) | 3 (17.6) | |
| L4–5 | 40 (48.2) | 29 (43.9) | 11 (64.7) | |
| L5–S1 | 14 (16.9) | 11 (16.7) | 3 (17.6) | |
| T11–12 | 2 (2.4) | 2 (3.0) | 0 (0.0) | |
| Primary vs. Revision | 0.458 | |||
| Primary | 63 (75.9) | 47 (71.2) | 16 (94.1) | |
| Revision | 2 (2.4) | 1 (1.5) | 1 (5.9) | |
| PBV (L) | 4.20 ± 0.79 | 4.17 ± 0.83 | 4.34 ± 0.59 | 0.425 |
| Preop Hct (mL) | 389.40 ± 45.66 | 380.21 ± 41.93 | 425.06 ± 42.92 | <0.001 |
| Postop Hct (mL) | 366.41 ± 46.99 | 358.91 ± 44.20 | 395.53 ± 47.38 | 0.028 |
| Hct average (mL) | 377.90 ± 43.96 | 369.56 ± 40.43 | 410.29 ± 43.13 | <0.001 |
| TBL (mL) | 257.72 ± 329.66 | 247.16 ± 346.88 | 298.71 ± 256.65 | 0.568 |
| VBL (mL) | 103.77 ± 59.96 | 97.71 ± 57.52 | 127.29 ± 65.16 | <0.001 |
| Operative time (min) | 114.67 ± 32.75 | 124.26 ± 28.97 | 77.47 ± 15.41 | <0.001 |
| Intraoperative blood loss | 36.22 ± 25.53 | 29.11 ± 23.11 | 63.82 ± 12.31 | <0.001 |
| Postop 1 day drain (mL) | 37.41 ± 38.95 | 37.74 ± 27.18 | 36.12 ± 69.07 | 0.021 |
| Postop 2 day drain (mL) | 28.97 ± 25.76 | 29.40 ± 28.11 | 27.35 ± 14.47 | 0.491 |
| Postop 3 day drain (mL) | 13.21 ± 10.36 | 13.21 ± 10.36 | 0.00 ± 0.00 | - |
| Total drain amount (mL) | 67.55 ± 53.27 | 68.61 ± 50.14 | 63.47 ± 65.64 | 0.513 |
| HBL (mL) | t | p-Value | |
|---|---|---|---|
| BESS group | 149.44 ± 344.08 | −0.302 | 0.764 |
| Open surgery group | 171.42 ± 243.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-G.; Park, E.J.; Min, W.-K.; Kim, S.-B.; Lee, G.; Choi, S. Comparison of Hidden Blood Loss in Biportal Endoscopic Spine Surgery and Open Surgery in the Lumbar Spine: A Retrospective Multicenter Study. J. Clin. Med. 2025, 14, 3878. https://doi.org/10.3390/jcm14113878
Kim D-G, Park EJ, Min W-K, Kim S-B, Lee G, Choi S. Comparison of Hidden Blood Loss in Biportal Endoscopic Spine Surgery and Open Surgery in the Lumbar Spine: A Retrospective Multicenter Study. Journal of Clinical Medicine. 2025; 14(11):3878. https://doi.org/10.3390/jcm14113878
Chicago/Turabian StyleKim, Dae-Geun, Eugene J. Park, Woo-Kie Min, Sang-Bum Kim, Gaeun Lee, and Sung Choi. 2025. "Comparison of Hidden Blood Loss in Biportal Endoscopic Spine Surgery and Open Surgery in the Lumbar Spine: A Retrospective Multicenter Study" Journal of Clinical Medicine 14, no. 11: 3878. https://doi.org/10.3390/jcm14113878
APA StyleKim, D.-G., Park, E. J., Min, W.-K., Kim, S.-B., Lee, G., & Choi, S. (2025). Comparison of Hidden Blood Loss in Biportal Endoscopic Spine Surgery and Open Surgery in the Lumbar Spine: A Retrospective Multicenter Study. Journal of Clinical Medicine, 14(11), 3878. https://doi.org/10.3390/jcm14113878