
The Effect of Sphincter Pressure and Anal Length on Surgical Decision in Chronic Anal Fissure

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAF | chronic anal fissure |
| LIS | lateral internal sphincterotomy |
| VAS | visual analog scale |
| EAUS | endoanal ultrasonography |
| HRAM | high-resolution anal manometry |
| RAIR | rectoanal inhibitory reflex |
| JWIS | Jorge-Wexner Incontinence Score |
| HPZ | high-pressure zone |
| ASCRS | The American Society of Colon and Rectal Surgeons |
| FI | fecal incontinence |
| NSVD | normal spontaneous vaginal delivery |
References
- Brady, J.T.; Althans, A.R.; Neupane, R. Treatment for anal fissure: Is there a safe option? Am. J. Surg. 2017, 214, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Davids, J.S.; Hawkins, A.T.; Bhama, A.R.; Feinberg, A.E.; Grieco, M.J.; Lightner, A.L.; Feingold, D.L.; Paquette, I.M.; On behalf of the Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anal Fissures. Dis. Colon Rectum 2022, 66, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, J.; Fowler, G.E.; Zahid, A.; Brown, K.; Young, C.J. Treatment of anal fissure: A survey of surgical practice in Australia and New Zealand. Color. Dis. 2019, 21, 226–233. [Google Scholar] [CrossRef]
- Boland, P.A.; Kelly, M.E.; Donlon, N.E.; Bolger, J.C.; Larkin, J.O.; Mehigan, B.J.; McCormick, P.H. Management options for chronic anal fissure: A systematic review of randomised controlled trials. Int. J. Color. Dis. 2020, 35, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Balla, A.; Saraceno, F.; Shalaby, M. Surgeons’ practice and preferences for the anal fissure treatment: Results from an inter-national survey. Updates Surg. 2023, 75, 2279–2290. [Google Scholar] [CrossRef]
- Notaras, M.J. Lateral subcutaneous sphincterotomy for anal fissure—A new technique. Proc. R. Soc. Med. 1969, 62, 713. [Google Scholar] [CrossRef]
- Beaty, J.S.; Shashidharan, M. Anal Fissure. Clin. Colon Rectal Surg. 2016, 29, 30–37. [Google Scholar] [PubMed]
- Poh, A.; Tan, K.-Y.; Seow-Choen, F. Innovations in chronic anal fissure treatment: A systematic review. World J. Gastrointest. Surg. 2010, 2, 231–241. [Google Scholar] [CrossRef]
- Madalinski, M.H. Identifying the best therapy for chronic anal fissure. World J. Gastrointest. Pharmacol. Ther. 2011, 2, 9–16. [Google Scholar] [CrossRef]
- Jones, O.M.; Ramalingam, T.; Lindsey, I.; Cunningham, C.; George, B.D.; Mortensen, N.J.M. Digital rectal examination of sphincter pressures in chronic anal fissure is unreliable. Dis. Colon Rectum 2005, 48, 349–352. [Google Scholar] [CrossRef]
- Mihmanli, I.; Kantarci, F.; Dogra, V.S. Endoanorectal ultrasonography. Ultrasound Q. 2011, 27, 87–104. [Google Scholar] [CrossRef] [PubMed]
- Acar, T.; Acar, N.; Güngör, F. Treatment of chronic anal fissure: Is open lateral internal sphincterotomy (LIS) a safe and adequate option? Asian J. Surg. 2019, 42, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Perry, W.B.; Dykes, S.L.; Buie, W.D.; Rafferty, J.F. Standards Practice Task Force of the American Society of Colon and Rectal Surgeons, Practice parameters for the management of anal fissures (3rd revision). Dis. Colon Rectum 2010, 53, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, H.; Hafez, E.A.; Saeed, A.; Ibrahim, S.; Hanna, Y. Study of Anorectal Manometry changes in Anal Fissure. Benha J. Appl. Sci. 2020, 5, 307–314. [Google Scholar] [CrossRef]
- Salem, A.E.; Mohamed, E.A.; Elghadban, H.M.; Abdelghani, G.M. Potential combination topical therapy of anal fissure: Development, evaluation, and clinical study. Drug Deliv. 2018, 25, 1672–1682. [Google Scholar] [CrossRef]
- Casillas, S.; Hull, T.L.; Zutshi, M.; Trzcinski, R.; Bast, J.F.; Xu, M. Incontinence after a lateral internal sphincterotomy: Are we underestimating it? Dis. Colon Rectum 2005, 48, 1193–1199. [Google Scholar] [CrossRef]
- Elsebae, M.M.A. A Study of fecal incontinence in patients with chronic anal fissure: Prospective, randomized, controlled trial of the extent of internal anal sphincter division during lateral sphincterotomy. World J. Surg. 2007, 31, 2052–2057. [Google Scholar] [CrossRef]
- D’orazio, B.; Geraci, G.; Bonventre, S.; Calì, D.; Di Vita, G. Safety and effectiveness of saving sphincter procedure in the treatment of chronic anal fissure in female patients. BMC Surg. 2021, 21, 350. [Google Scholar] [CrossRef]
- Kumar, L.; Emmanuel, A. Internal anal sphincter: Clinical perspective. Surgeon 2017, 15, 211–226. [Google Scholar] [CrossRef]
- Brillantino, A.; Izzo, D.; Iacobellis, F.; Maglio, M.; Grillo, M.; Vicenzo, L.; Bottino, V.; Renzi, A. Safety and effectiveness of minimal sphincterotomy in the treatment of female patients with chronic anal fissure. Updat. Surg. 2020, 73, 1829–1836. [Google Scholar] [CrossRef]
- Yucel, E.; Akin, M.L.; Sucullu, I.; Filiz, A.I.; Ozdemir, Y.; Yildiz, M. Endoanal ultrasonographic evaluation of an unhealed anal fissure after the lateral internal sphincterotomy. Bratisl. Med. J. 2013, 114, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, A.; Kusanagi, H. Enhanced Approach to Treating Chronic Anal Fissures: Fissurectomy with Vertical Non-full-thickness Midline Sphincterotomy and Mucosal Advancement Flap. J. Anus Rectum Colon 2024, 8, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Gaj,, F.; Biviano, I.; Candeloro, L.; Andreuccetti, J. Anal self-massage in the treatment of acute anal fissure: a randomized prospective study. Ann. Gastroenterol. 2017, 30, 438–441. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameter | External Sphincter Thickness (mm) | Internal Sphincter Thickness (mm) | Localization Where the Internal Sphincter Is Thickest Thickness (mm) | Length Between the End of the External Sphincter and Puborectal (mm) | ||||
|---|---|---|---|---|---|---|---|---|
| Top | Middle | Bottom | Top | Middle | Bottom | |||
| N | 4.88 ± 1.19 | 3.13 ± 0.86 | 3.39 ± 0.96 | 3.23 ± 0.73 | 8 | 11 | 2 | 40.00 ± 7.61 |
| % | 4.9 (2.8–7) | 3 (2–5.1) | 3.6 (2.2–5.1) | 3.2 (1.8–4.7) | (38.10) | (52.38) | (9.52) | (10.50) |
| N | % | ||
|---|---|---|---|
| Fissure length (mm) | 11.62 ± 2.80 | 12 (8–20) | |
| Anatomical anal canal length measured from the anal verge to the dentate line (mm) | 24.48 ± 4.45 | 25 (18–33) | |
| Anatomical anal canal | ≤2 | 7 | (33.33) |
| >2 | 14 | (66.67) | |
| Length from toothed line to puborectal (mm) | 18.48 ± 3.33 | 19 (12–25) | |
| Surgical anal canal length Measured from the anal verge to the puborectalis muscle (mm) | 42.95 ± 5.22 | 44 (31–50) | |
| Surgical anal canal | ≤4 | 8 | (38.10) |
| >4 | 13 | (61.90) | |
| Distance from the intersphincteric groove to the dentate line (mm) | 17.57 ± 4.31 | 18 (10–24) | |
| o’clock position | 6 o’clock position | 17 | (80.95) |
| 12 o’clock position | 2 | (9.52) | |
| 6 + 12 o’clock position | 2 | (9.52) | |
| Preoperative | Postoperative Day 1 | Postoperative Month 1 | Postoperative Month 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| JWIS | 0 | 21 | (100.00) | 19 | (90.48) | 21 | (100.00) | 21 | (100.00) |
| 1 | 2 | (9.52) | |||||||
| Preoperative | Postoperative Day 1 | Postoperative Day 10 | Postoperative Month 1 | ||
|---|---|---|---|---|---|
| VAS | Mean ± s.s. | 7.57 ± 0.93 | 5.48 ± 0.60 | 1.95 ± 1.12 | 0.14 ± 0.36 |
| Median (Min–Max) | 7 (6–10) | 6 (4–6) | 2 (0–3) | 0 (0–1) |
| Preop | Postop | p | ||||
|---|---|---|---|---|---|---|
| Mean ± s.s. | Median | Mean ± s.s. | Median | |||
| Weight | 73.9 ± 19.2 | 72.0 | 78.1 ± 20.8 | 75.0 | 0.000 | W |
| Length to HPZ | 3.3 ± 1.1 | 3.5 | 3.2 ± 0.9 | 3.3 | 0.415 | E |
| Verge-Center (cm) | 1.4 ± 0.7 | 1.2 | 1.5 ± 0.9 | 1.3 | 0.468 | E |
| Sphincter Pressure at Rest (mmHg) Rectal Reflex | ||||||
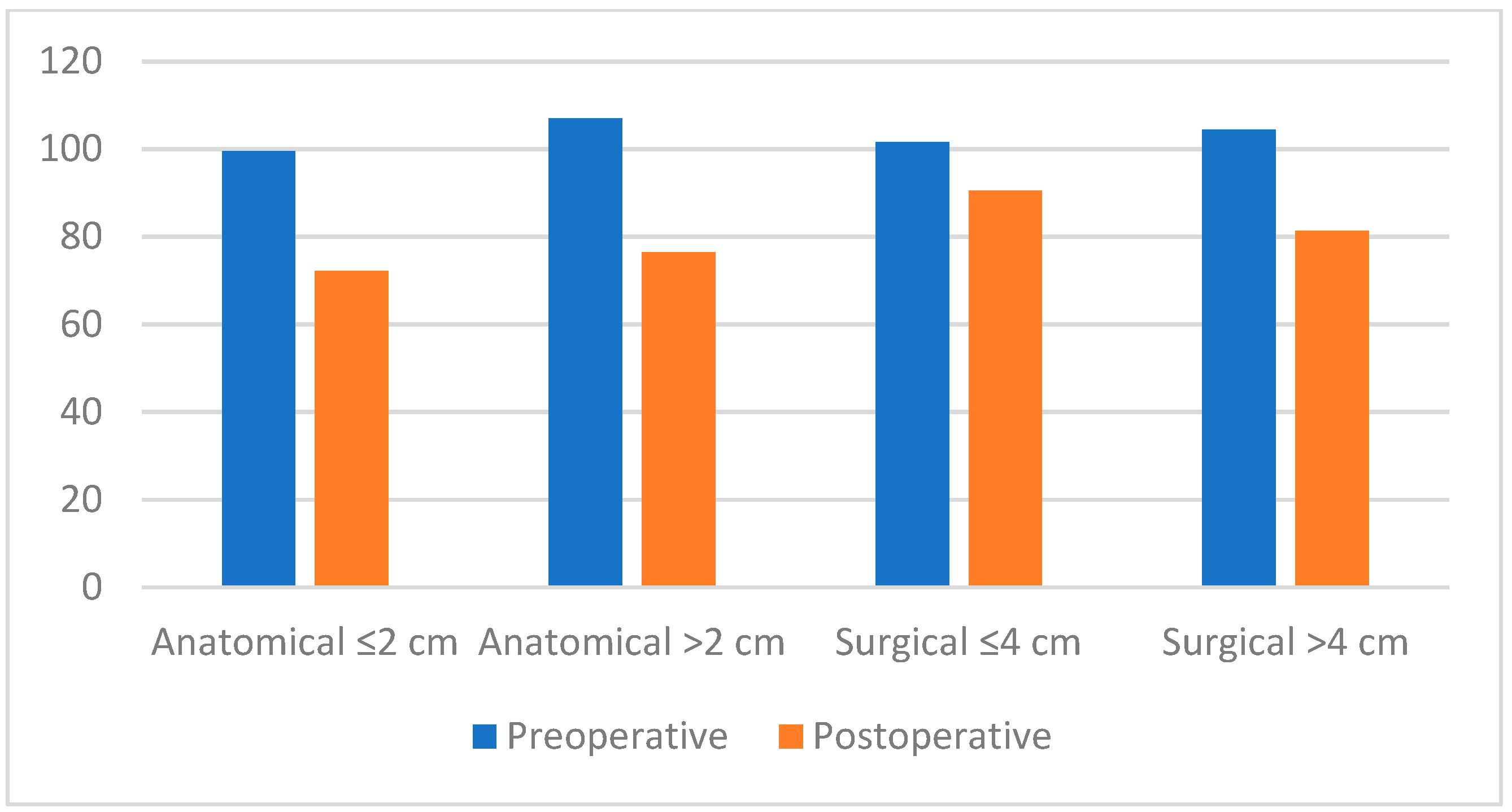
| Average | 103.2 ± 23.5 | 105.9 | 85.5 ± 28.1 | 82.5 | 0.014 | E |
| Maximum | 117.2 ± 37.0 | 115.6 | 92.2 ± 28.4 | 91.7 | 0.017 | E |
| Sphincter Pressure (mmHg) Absolute Reflex | ||||||
| Average | 86.3 ± 15.7 | 89.6 | 66.5 ± 15.0 | 67.0 | 0.000 | W |
| Maximum | 146.6 ± 201.8 | 106.7 | 73.4 ± 17.3 | 74.9 | 0.000 | W |
| Defecation Attempt | ||||||
| Waste Anal Pressure (mmHg) Absolute Pressure | 74.3 ± 30.5 | 76.9 | 67.7 ± 27.6 | 65.0 | 0.084 | W |
| Anal Relaxation % | 27.8 ± 25.7 | 27.0 | 17.5 ± 28.6 | 19.5 | 0.091 | W |
| Intrarectal Pressure (mmHg) | 36.4 ± 34.5 | 28.2 | 41.4 ± 28.7 | 38.5 | 0.616 | W |
| RAIR Relaxation % | 37.6 ± 11.9 | 35.0 | 40.7 ± 13.0 | 39.0 | 0.325 | E |
| Rectal Compliance (cc/mmHg) | 3.2 ± 8.8 | 1.6 | 1.5 ± 0.6 | 1.3 | 0.157 | W |
| Spontaneous Vaginal Birth (−) | Spontaneous Vaginal Birth (+) | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± s.s. | Median | Mean ± s.s. | Median | |||||||
| Weight | ||||||||||
| Preoperative | 71.2 | ± | 9.6 | 71.5 | 94.3 | ± | 23.9 | 97.5 | 0.146 | t |
| Postoperative | 73.0 | ± | 11.5 | 72.0 | 99.0 | ± | 25.4 | 99.5 | 0.078 | t |
| Length to HPZ | ||||||||||
| Preoperative | 4.20 | ± | 0.67 | 4.20 | 2.85 | ± | 0.51 | 2.75 | 0.009 | t |
| Postoperative | 3.84 | ± | 0.59 | 3.70 | 2.43 | ± | 0.94 | 2.25 | 0.028 | t |
| Verge-Center (cm) | ||||||||||
| Preoperative | 1.42 | ± | 0.34 | 1.55 | 1.08 | ± | 0.43 | 1.05 | 0.194 | t |
| Postoperative | 1.66 | ± | 0.30 | 1.70 | 0.75 | ± | 0.26 | 0.80 | 0.002 | t |
| Mean Sphincter Pressure at Rest Sphincter Pressure Rectal Ref. | ||||||||||
| Preoperative | 117.5 | ± | 12.2 | 120.3 | 84.7 | ± | 23.2 | 89.0 | 0.018 | t |
| Postoperative | 105.7 | ± | 19.6 | 115.3 | 79.1 | ± | 5.2 | 80.6 | 0.036 | t |
| Defecation Attempt Waste Anal Pressure | ||||||||||
| Preoperative | 71.3 | ± | 29.9 | 76.4 | 87.6 | ± | 42.9 | 98.8 | 0.201 | m |
| Postoperative | 60.4 | ± | 41.7 | 51.8 | 73.3 | ± | 32.4 | 82.8 | 0.712 | m |
| Defecation Attempt % Anal Relaxation | ||||||||||
| Preoperative | 30.3 | ± | 29.3 | 27.0 | 11.8 | ± | 22.5 | 2.5 | 0.285 | m |
| Postoperative | 40.1 | ± | 22.3 | 38.4 | 9.8 | ± | 29.2 | 3.5 | 0.142 | m |
| RAIR Relaxation % | ||||||||||
| Preoperative | 35.8 | ± | 4.1 | 35.0 | 25.5 | ± | 10.8 | 25.0 | 0.130 | m |
| Postoperative | 37.8 | ± | 8.4 | 32.0 | 27.8 | ± | 7.9 | 25.5 | 0.085 | m |
| Rectal Compliance (cc/mmHg) | ||||||||||
| Preoperative | 3.15 | ± | 1.24 | 2.93 | 1.24 | ± | 0.31 | 1.36 | 0.012 | t |
| Postoperative | 1.78 | ± | 0.55 | 1.84 | 1.66 | ± | 0.96 | 1.26 | 0.817 | t |
| Surgical Anal Canal ≤40 (n = 9) | Surgical Anal Canal >40 (n = 14) | p | ||||
|---|---|---|---|---|---|---|
| Mean ± s.s. | Median | Mean ± s.s. | Median | |||
| Weight | ||||||
| Preoperative | 69.2 ± 17.4 | 72.0 | 76.9 ± 20.4 | 72.5 | 0.361 | |
| Postoperative | 71.9 ± 18.0 | 72.0 | 82.8 ± 22.3 | 75.5 | 0.243 | |
| Length to HPZ | ||||||
| Preoperative | 3.41 ± 1.11 | 3.30 | 3.31 ± 1.09 | 3.60 | 0.827 | |
| Postoperative | 3.39 ± 0.87 | 3.60 | 2.99 ± 0.85 | 3.10 | 0.315 | |
| Verge-Center(cm) | ||||||
| Preoperative | 1.48 ± 1.00 | 1.20 | 1.33 ± 0.36 | 1.37 | 0.617 | |
| Postoperative | 1.52 ± 1.10 | 1.20 | 1.50 ± 0.64 | 1.40 | 0.970 | |
| Mean Sphincter Pressure at Rest Sphincter Pressure | ||||||
| Preoperative | 101.5 ± 23.3 | 95.2 | 104.4 ± 24.4 | 106.5 | 0.778 | |
| Postoperative | 90.5 ± 33.0 | 85.4 | 81.3 ± 24.2 | 81.4 | 0.483 | |
| Defecation Attempt Waste Anal Pressure | ||||||
| Preoperative | 79.8 ± 18.1 | 76.9 | 70.8 ± 36.5 | 76.3 | 0.505 | t |
| Postoperative | 75.0 ± 22.7 | 81.7 | 61.8 ± 30.8 | 60.9 | 0.297 | t |
| Defecation Attempt % Anal Relaxation | ||||||
| Preoperative | 20.2 ± 12.0 | 19.0 | 32.6 ± 31.0 | 27.0 | 0.517 | t |
| Postoperative | 12.8 ± 18.4 | 13.0 | 21.4 ± 35.3 | 22.0 | 0.585 | t |
| RAIR Relaxation % | ||||||
| Preoperative | 44.3 ± 10.3 | 43.0 | 33.3 ± 11.1 | 34.0 | 0.011 | m |
| Postoperative | 48.0 ± 10.5 | 48.0 | 34.1 ± 11.6 | 31.5 | 0.014 | m |
| Rectal Compliance (cc/mmHg) | ||||||
| Preoperative | 0.99 ± 3.50 | 1.56 | 4.54 ± 10.93 | 1.92 | 0.682 | m |
| Postoperative | 1.39 ± 0.44 | 1.30 | 1.63 ± 0.69 | 1.50 | 0.624 | m |
| Parameter | Anatomical Anal Canal | p | |||
|---|---|---|---|---|---|
| ≤2 cm | >2 cm | ||||
| Mean ± s.s. | Median (Min–Max) | Mean ± s.s. | Median (Min–Max) | ||
| Weight | 64.29 ± 15.61 | 72 (42–85) | 81.5 ± 21.17 | 78 (52–117) | 0.199 |
| 66.43 ± 15.69 | 70 (40–87) | 85.5 ± 22.48 | 82 (55–127) | ||
| Length to HPZ | 3.04 ± 0.91 | 2.8 (2.1–4.3) | 3.66 ± 0.86 | 3.75 (2.2–5.2) | 0.163 |
| 3.19 ± 0.78 | 3.6 (1.8–3.9) | 3.31 ± 0.89 | 3.35 (1.5–4.8) | ||
| Verge–center (cm) | 1.53 ± 1.12 | 1.2 (0.4–3.9) | 1.28 ± 0.41 | 1.2 (0.6–1.8) | 0.432 |
| 1.44 ± 0.88 | 1.2 (0.6–3.1) | 1.43 ± 0.64 | 1.4 (0.4–2.6) | ||
| Mean Sphincter at Rest Pressure (mmHg) | 99.54 ± 23.57 | 105.9 (73.5–134.4) | 107.03 ± 25.23 | 110.45 (54.3–152.1) | 0.824 |
| 72.21 ± 29.66 | 65.4 (36.4–128.4) | 76.47 ± 24.37 | 72.5 (44.7–127.6) | ||
| Attempted Defecation % Anal Relaxation | 18.71 ± 12.45 | 19 (−3–36) | 29.17 ± 38.11 | 22.5 (−28–102) | 0.743 |
| 10.43 ± 20.57 | 13 (−24–40) | 16.84 ± 32.22 | 17.5 (−55–61) | ||
| Attempted Defecation Intrathecal Pressure (mmHg) | 16.23 ± 20.69 | 22.5 (−12.6–39.1) | 50.22 ± 38.49 | 61.2 (−6.7–109.5) | 0.535 |
| 23.81 ± 18.25 | 23.5 (−0.25–42.8) | 51.68 ± 29.53 | 54.55 (−3.8–109) | ||
| Rectoanal Pressure Difference (mmHg) | −60.7 ± 27.19 | −48.3 (−113–35.9) | −27.03 ± 55.25 | −26.2 (−106.3–93.4) | 0.392 |
| −37.3 ± 19.66 | −40.7 (−72.9–15.6) | −21.25 ± 24.44 | −22.5 (−69–19.8) | ||
| RAIR Relaxation (%) | 45.14 ± 11.07 | 43 (33–60) | 33.17 ± 19.28 | 35 (3–80) | 0.242 |
| 37.29 ± 19.18 | 39 (6–67) | 34.75 ± 15.21 | 30 (17–65) | ||
| Rectal Compliance (cc/mmHg) | 0.81 ± 4.02 | 2.28 (−8.16–3.15) | 5.54 ± 11.86 | 1.8 (−11.53–38.85) | 0.708 |
| 1.5 ± 0.30 | 1.45 (1.08–1.84) | 4.14 ± 6.55 | 1.46 (0.91–24) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutluk, F.; Ergün, S.; Mihmanli, İ.; Demiryas, S.; Hamid, R.; Perek, A. The Effect of Sphincter Pressure and Anal Length on Surgical Decision in Chronic Anal Fissure. J. Clin. Med. 2025, 14, 3805. https://doi.org/10.3390/jcm14113805
Kutluk F, Ergün S, Mihmanli İ, Demiryas S, Hamid R, Perek A. The Effect of Sphincter Pressure and Anal Length on Surgical Decision in Chronic Anal Fissure. Journal of Clinical Medicine. 2025; 14(11):3805. https://doi.org/10.3390/jcm14113805
Chicago/Turabian StyleKutluk, Fadime, Sefa Ergün, İsmail Mihmanli, Süleyman Demiryas, Rauf Hamid, and Asiye Perek. 2025. "The Effect of Sphincter Pressure and Anal Length on Surgical Decision in Chronic Anal Fissure" Journal of Clinical Medicine 14, no. 11: 3805. https://doi.org/10.3390/jcm14113805
APA StyleKutluk, F., Ergün, S., Mihmanli, İ., Demiryas, S., Hamid, R., & Perek, A. (2025). The Effect of Sphincter Pressure and Anal Length on Surgical Decision in Chronic Anal Fissure. Journal of Clinical Medicine, 14(11), 3805. https://doi.org/10.3390/jcm14113805