
Risk of Pneumoconiosis in Workers Exposed to Crystalline Silica from Lava Rock Dust from Mount Etna


 , , , ,
, , , ,  , ,
, , 
Abstract
1. Introduction
2. Subjects and Methods
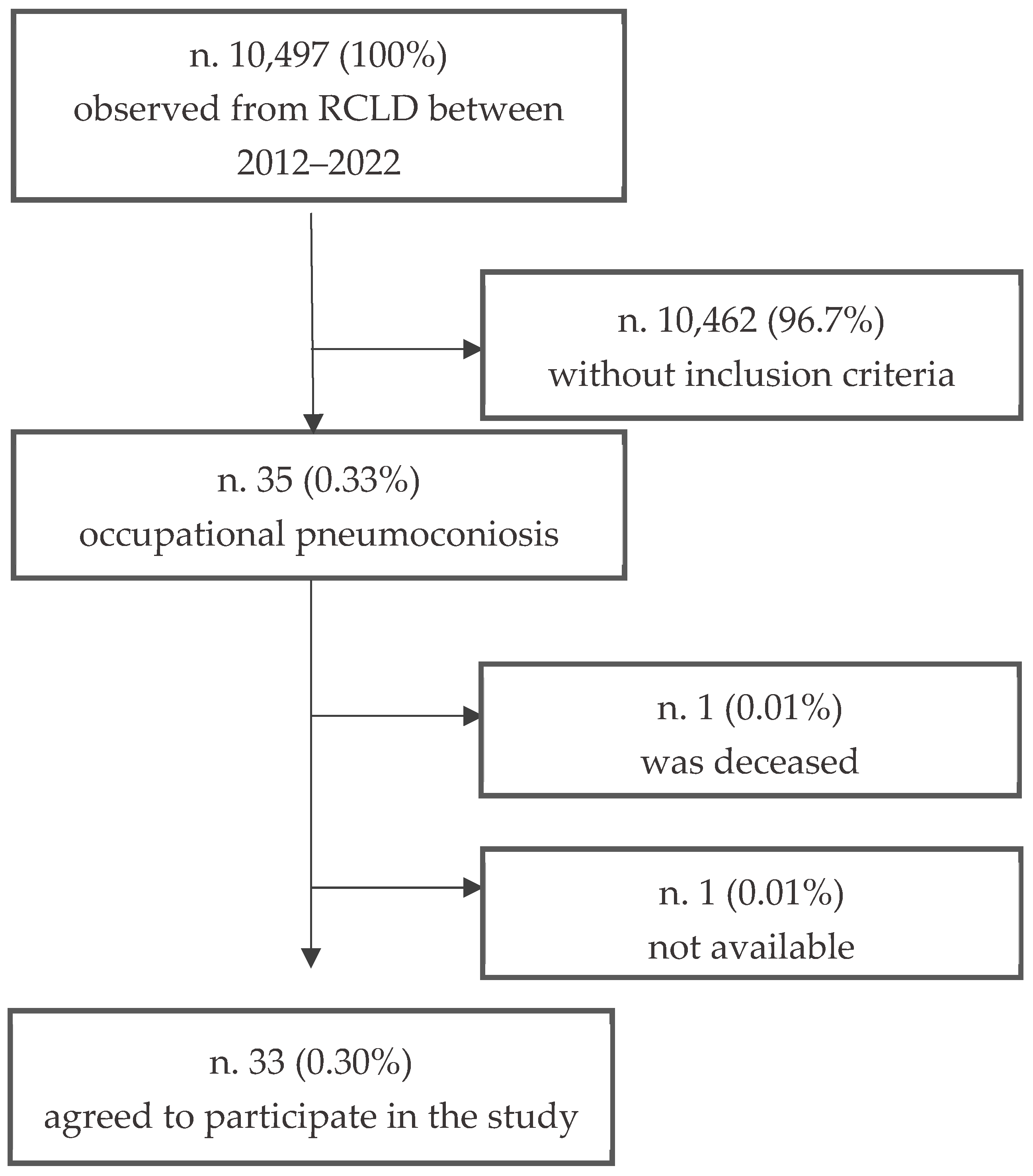
2.1. Sample from RCLD
2.2. Workers Occupational Exposed to Volcanic Dust
2.3. Exposure Measurements RCS
2.4. Statistical Analysis
3. Results
3.1. RCLD Group
3.2. Workers Occupational Exposed to Volcanic Dust
3.3. Volcanic Dust Occupational Exposure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qi, X.M.; Luo, Y.; Song, M.Y.; Liu, Y.; Shu, T.; Liu, Y.; Pang, J.L.; Wang, J.; Wang, C. Pneumoconiosis: Current status and future prospects. Chin. Med. J. 2021, 134, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Perlman, D.M.; Maier, L.A. Occupational Lung Disease. Med. Clin. N. Am. 2019, 103, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Karataş, M.; Gündüzöz, M.; Öziş, T.N.; Özakıncı, O.G.; Ergün, D. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as haematological indices of inflammatory response in ceramic workers’ silicosis. Clin. Respir. J. 2019, 13, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Li, C.; Wang, X.; Sun, X.; Zhang, R.; Chen, C.; Yu, M.; Liu, Y.; Zhu, Y.; Chen, J. Oridonin attenuates lung inflammation and fibrosis in silicosis via covalent targeting iNOS. Biomed. Pharmacother. 2022, 153, 113532. [Google Scholar] [CrossRef]
- Raanan, R.; Zack, O.; Ruben, M.; Perluk, I.; Moshe, S. Occupational Silica Exposure and Dose-Response for Related Disorders-Silicosis, Pulmonary TB, AIDs and Renal Diseases: Results of a 15-Year Israeli Surveillance. Int. J. Environ. Res. Public Health 2022, 19, 15010. [Google Scholar] [CrossRef]
- Aghilinejad, M.; Naserbakht, A.; Naserbakht, M.; Attari, G. Silicosis among stone-cutter workers: A cross-sectional study. Tanaffos 2012, 11, 38–41. [Google Scholar]
- Lai, H.; Liu, Y.; Zhou, M.; Shi, T.; Zhou, Y.; Weng, S.; Chen, W. Combined effect of silica dust exposure and cigarette smoking on total and cause-specific mortality in iron miners: A cohort study. Environ. Health 2018, 17, 46. [Google Scholar] [CrossRef] [PubMed]
- Gbondo, D.; Zhao, Y.; Pham, M.; Rumchev, K. Trends in Exposure to respirable dust and respirable crystalline silica among lithium mine workers in Western Australia. Saf. Health Work 2024, 15, 481–490. [Google Scholar] [CrossRef]
- Su, X.; Kong, X.; Yu, X.; Zhang, X. Incidence and influencing factors of occupational pneumoconiosis: A systematic review and meta-analysis. BMJ Open 2023, 13, e065114. [Google Scholar] [CrossRef]
- Tjoe-Nij, E.; de Meer, G.; Smit, J.; Heederik, D. Lung function decrease in relation to pneumoconiosis and exposure to quartz-containing dust in construction workers. Am. J. Ind. Med. 2003, 43, 574–583. [Google Scholar] [CrossRef]
- Vinnikov, D.; Abenova, A.; Raushanova, A.; Rapisarda, V. Occupational exposure to fine particulate matter in the reinforced concrete production and its association with respiratory symptoms and lung function. BMC Public Health 2023, 23, 1813. [Google Scholar] [CrossRef] [PubMed]
- CHEST Interstitial and Diffuse Lung Disease Patient Questionnaire. Available online: https://foundation.chestnet.org/wp-content/uploads/2020/04/interstitial-diffuse-lung-disease-patient-questionnaire.pdf (accessed on 20 September 2024).
- Vinnikov, D.; Romanova, Z.; Raushanova, A.; Beisbekova, A.; Vitale, E.; Bimuratova, G.; Rapisarda, V. Exposure to respirable particulate matter and its association with respiratory outcomes in beauty salon personnel. Int. J. Environ. Res. Public Health 2023, 20, 2429. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization (ILO). Guidelines for the Use of the ILO International Classification of Radiographs of Pneumoconsioses Revised Edition 2022; Occupational Safety and Health Series 22; International Labour Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Vella, F.; Filetti, V.; Cirrincione, L.; Rapisarda, V.; Matera, S.; Skerjanc, A.; Cannizzaro, E.; Vitale, E. Work Ability after breast cancer: Study of healthcare personnel operating in a hospital of South Italy. Int. J. Environ. Res. Public Health 2022, 19, 10835. [Google Scholar] [CrossRef]
- Filetti, V.; Lombardo, C.; Loreto, C.; Dounias, G.; Bracci, M.; Matera, S.; Rapisarda, L.; Rapisarda, V.; Ledda, C.; Vitale, E. Small RNA-Seq transcriptome profiling of mesothelial and mesothelioma cell lines revealed microRNA dysregulation after exposure to asbestos-like fibers. Biomedicines 2023, 11, 538. [Google Scholar] [CrossRef]
- Ledda, C.; Cocuzza, S.; Salerno, M.; Senia, P.; Matera, S.; Rapisarda, V.; Loreto, C. Occupational exposure to Mount Etna’s basaltic dust: Assessment of mutagenic and cytotoxic effects. Mol. Med. Rep. 2017, 15, 3350–3354. [Google Scholar] [CrossRef]
- Liu, Y.; Rong, Y.; Steenland, K.; Christiani, D.C.; Huang, X.; Wu, T. Long-term exposure to crystalline silica and risk of heart disease mortality. Epidemiology 2014, 25, 689–696. [Google Scholar] [CrossRef]
- Guo, J.; Shi, T.; Cui, X.; Rong, Y.; Zhou, T.; Zhang, Z. Effects of silica exposure on the cardiac and renal inflammatory and fibrotic response and the antagonistic role of interleukin-1 beta in C57BL/6 mice. Arch. Toxicol. 2016, 90, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Li, X.; Cai, S.; Chen, Y.; Dai, W.; Liu, W.; Zhou, Z.; Duan, J.; Chen, P. Prevalence and characteristics of COPD among pneumoconiosis patients at an occupational disease prevention institute: A cross-sectional study. BMC Pulm. Med. 2018, 18, 22. [Google Scholar] [CrossRef]
- Vicari, F.; Randazzo, S.; López, J.; Fernández de Labastida, M.; Vallès, V.; Micale, G.; Tamburini, A.; D’Alì Staiti, G.; Cortina, J.L.; Cipollina, A. Mining minerals and critical raw materials from bittern: Understanding metal ions fate in saltwork ponds. Sci. Total Environ. 2022, 847, 157544. [Google Scholar] [CrossRef]
- Fazzo, L.; Cernigliaro, A.; De Santis, M.; Quattrone, G.; Bruno, C.; Zona, A.; Tumino, R.; Cascone, G.; Scondotto, S.; Comba, P. Occupational cohort study of asbestos-cement workers in a contaminated site in Sicily (Italy). Epidemiol. E Prev. 2020, 44, 137–144. [Google Scholar] [CrossRef]
- Apollaro, C.; Fuoco, I.; Gennaro, E.; Giuliani, L.; Iezzi, G.; Marini, L.; Radica, F.; Di Luccio, F.; Ventura, G.; Vespasiano, G. Advanced argillic alteration at Cave di Caolino, Lipari, Aeolian Islands (Italy): Implications for the mitigation of volcanic risks and the exploitation of geothermal resources. Sci. Total Environ. 2023, 889, 164333. [Google Scholar] [CrossRef]
- Rapisarda, V.; Loreto, C.; Castorina, S.; Romano, G.; Garozzo, S.F.; Musumeci, A.; Migliore, M.; Avola, R.; Cinà, D.; Pomara, C.; et al. Occupational exposure to fluoro-edenite and prevalence of anti-nuclear autoantibodies. Future Oncol. 2018, 14, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Howlett, P.; Gan, J.; Lesosky, M.; Feary, J. Relationship between cumulative silica exposure and silicosis: A systematic review and dose-response meta-analysis. Thorax 2024, 79, 934–942. [Google Scholar] [CrossRef]
- Vitale, E.; Vella, F.; Indelicato, G.; Canalella, A.; Briguglio, S.; Pittari, V.; Senia, P.; Vinnikov, D.; Floresta, D.; Rapisarda, V.; et al. SARS-CoV-2 Transmission Prevention Model Application in a Large Retail Company Before the Vaccine Introduction. Front. Public Health 2022, 10, 908690. [Google Scholar] [CrossRef]
- Censi, P.; Zuddas, P.; Randazzo, L.A.; Tamburo, E.; Speziale, S.; Cuttitta, A.; Punturo, R.; Aricò, P.; Santagata, R. Source and nature of inhaled atmospheric dust from trace element analyses of human bronchial fluids. Environ. Sci. Technol. 2011, 45, 6262–6267. [Google Scholar] [CrossRef] [PubMed]
- Nandedkar, R.H.; Ulmer, P.; Müntener, O. Fractional crystallization of primitive, hydrous arc magmas: An experimental study at 0.7 GPa. Contrib. Miner. Pet. 2014, 167, 1015. [Google Scholar] [CrossRef]
- Ulmer, P.; Kaegi, R.; Müntener, O. Experimentally derived intermediate to silica-rich arc magmas by fractional and equilibrium crystallization at 1·0 GPa: An evaluation of phase relationships, compositions, liquid lines of descent and oxygen fugacity. J. Petrol. 2018, 59, 11–58. [Google Scholar] [CrossRef]
- Ledda, C.; Loreto, C.; Bracci, M.; Mangano, D.; Migliore, M.; Ricceri, V.; Musumeci, A.; Costa, C.; Pomara, C.; Rapisarda, V. High risk of pleural plaques and parenchymal abnormalities in women living in Biancavilla (Italy). Future Oncol. 2016, 12, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Filetti, V.; Vitale, E.; Broggi, G.; Hagnäs, M.P.; Candido, S.; Spina, A.; Lombardo, C. Update of in vitro, in vivo and ex vivo fluoro-edenite effects on malignant mesothelioma: A systematic review (Review). Biomed. Rep. 2020, 13, 60. [Google Scholar] [CrossRef]
- Ledda, C.; Loreto, C.; Filetti, V.; Matera, S.; Vitale, E.; Bracci, M.; Rapisarda, V. Abnormal plasma cell disorders in refinery waste workers. J. Clin. Med. 2018, 7, 221. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, P.; Scoccianti, G.; Schiavo, A.; Tortolini, V.; Wigley, C.; Muratori, F.; Matera, D.; Kukushkina, M.; Funovics, P.T.; Lingitz, M.T.; et al. Extra-abdominal desmoid tumor fibromatosis: A multicenter EMSOS study. BMC Cancer 2021, 21, 437. [Google Scholar] [CrossRef] [PubMed]
- Matera, D.; Campanacci, D.A.; Caldora, P.; Mazza, E.; Capanna, R. Osteoid osteoma of the femur with a double nidus: A case report. Chir. Organi. Mov. 2005, 90, 75–79, (In English, Italian). [Google Scholar] [PubMed]

{kind=link}
| CW | SW | QW | p-Value | |
|---|---|---|---|---|
| Subjects 33 (100%) | 18 (55%) | 9 (27%) | 6 (18%) | - |
| Mean age yrs | 65.4 ± 4.9 | 66.8 ± 3.6 | 67.1 ± 6.7 | n.s |
| Sex | Male (100%) | Male (100%) | Male (100%) | n.s |
| BMI | 25.8 ± 3.2 | 26.1 ± 3.5 | 26.2 ± 2.8 | n.s |
| Smokers | 17 (%) | 8 (%) | 5 (%) | n.s |
| Pack-years | 29.15 ± 11.38 | 28.41 ± 13.11 | 29.07 ± 16.92 | n.s. |
| Age at first exposure (yrs) | 18.15 ± 4.12 | 19.54 ± 7.37 | 19.19 ± 6.90 | n.s. |
| RCS source material (n.) | Bricks (18), sandstone (18), clay (10), marble (18), cement (18), artificial stone (14), lava stone (3), and sand (15) | Marble (9), limestone rock (9), and granite (9) | Sandstone (2), marble (2), and lava stone (2) | - |
| Duration of dust exposure (yrs) | 27.4 ± 6.8 | 26.7 ± 5.3 | 25.5 ± 3.1 | n.s. |
| Use of airways PPE (yrs) | 4.7 ± 1.2 | 5.3 ± 2.1 | 5.1 ± 1.3 | n.s. |
| Age at pneumoconiosis diagnosis (yrs) | 50.3 ± 9.2 | 52.1 ± 4.3 | 51.7 ± 8.4 | n.s. |
| Latency of pneumoconiosis (yrs) | 25.6 ± 4.8 | 23.3 ± 8.6 | 24.2 ± 6.5 | n.s. |
| Symptoms | ChCh −/+ sputum (43/57%), dyspnea (77%), ChTi (31%), and wheezing (34%) | ChCh −/+ sputum (41/49%), dyspnea (75%), ChTi (25%), and wheezing (37%) | ChCh −/+ sputum (45/50%), dyspnea (82%), ChTi (27%), and wheezing (32%) | n.s. |
| Pneumoconiosis profusion category | ≥2/2 (7) *; ≥2/3 (4); ≥3/2 (3); ≥3/2 (2) | ≥2/3 (3); ≥3/2 (3); ≥3/2 (3) | ≥2/3 (3); ≥3/2 (2); ≥3/2 (1) | p < 0.05 n.s. |
| CW | LSW | QW | p-Values | |
|---|---|---|---|---|
| Workers, n (%) | 110 (100%) | 56 (100%) | 34 (100%) | - |
| Age (years) | 40.3 ± 6.7 | 41.2 ± 4.4 | 40.9 ± 5.2 | n.s. |
| Sex (male) | 100% | 100% | 100% | n.s. |
| Exposed to volcanic dust (years) | 13.4 ± 3.9 | 14.5 ± 6.4 | 14.1 ± 2.2 | n.s. |
| Smoking habits | 90 (81%) | 44 (79%) | 28 (82%) | n.s. |
| Pack/years | 28.25 ± 13.59 | 27.92 ± 12.21 | 29.01 ± 17.53 | n.s. |
| BMI | 26.9 ± 2.4 | 27.2 ± 2.3 | 26.1 ± 3.2 | n.s. |
| Used respiratory PPE (years) | 5.1 ± 3.2 | 5.5 ± 2.9 | 5.2 ± 3.4 | n.s. |
| CW | LSW | QW | p-Values | |
|---|---|---|---|---|
| FVC, % | 98.2 ± 5.7 | 97.7 ± 1.3 | 96.9 ± 1.4 | n.s. |
| FEV1, % | 98.8 ± 7.8 | 96.5 ± 1.7 | 93.4 ± 2.3 | n.s. |
| PEF, % | 97.6 ± 7.9 | 96.7 ± 5.4 | 92.3 ± 4.6 | n.s. |
| MEF25–75, % | 94.5 ± 8.6 | 93.3 ± 5.2 | 91.5 ± 6.8 | n.s. |
| TLC, % | 96.6 ± 5.6 | 94.2 ± 2.9 | 92.8 ± 3.9 | n.s. |
| TC findings | (2) Outcomes of COVID-19 pneumonia; (8) mild thickening of BAN hilar area | (1) Outcomes of COVID-19 pneumonia; (1) outcomes of previous pleurisy | (2) Mild thickening of BAN hilar area; (1) outcomes of previous pleurisy | n.s. |
| DLCO % | n.p. | n.p. | n.p. | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vella, F.; Filetti, V.; Matera, S.; Spinello, S.; Vinnikov, D.; Muscato, G.; Rapisarda, V.; Matera, D.; Rapisarda, L.; Vitale, E. Risk of Pneumoconiosis in Workers Exposed to Crystalline Silica from Lava Rock Dust from Mount Etna. J. Clin. Med. 2025, 14, 3781. https://doi.org/10.3390/jcm14113781
Vella F, Filetti V, Matera S, Spinello S, Vinnikov D, Muscato G, Rapisarda V, Matera D, Rapisarda L, Vitale E. Risk of Pneumoconiosis in Workers Exposed to Crystalline Silica from Lava Rock Dust from Mount Etna. Journal of Clinical Medicine. 2025; 14(11):3781. https://doi.org/10.3390/jcm14113781
Chicago/Turabian StyleVella, Francesca, Veronica Filetti, Serena Matera, Salvatore Spinello, Denis Vinnikov, Giuseppe Muscato, Venerando Rapisarda, Davide Matera, Lucia Rapisarda, and Ermanno Vitale. 2025. "Risk of Pneumoconiosis in Workers Exposed to Crystalline Silica from Lava Rock Dust from Mount Etna" Journal of Clinical Medicine 14, no. 11: 3781. https://doi.org/10.3390/jcm14113781
APA StyleVella, F., Filetti, V., Matera, S., Spinello, S., Vinnikov, D., Muscato, G., Rapisarda, V., Matera, D., Rapisarda, L., & Vitale, E. (2025). Risk of Pneumoconiosis in Workers Exposed to Crystalline Silica from Lava Rock Dust from Mount Etna. Journal of Clinical Medicine, 14(11), 3781. https://doi.org/10.3390/jcm14113781