

Post-Traumatic Osteoarthritis and Functional Outcomes After Volar Plating vs. Casting of Unstable Distal Radius Fractures: A Minimum 2-Year Follow-Up of the VOLCON Randomized Controlled Trial

 ,
,
Abstract
1. Introduction
2. Materials and Methods
Explorative Outcomes of the Original RCT
- Sensory disturbance, including carpal tunnel syndrome and chronic regional pain syndrome;
- Flexor tendon rupture and irritation;
- Extensor tendon rupture and irritation;
- Hardware failure, e.g., osteosynthesis loosening;
- Infection: superficial (treated with antibiotics only) or deep (requiring a surgical intervention);
- Reoperation with hardware replacement;
- Reoperation with hardware removal (partial or total), which is not routinely performed in our country.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DRF | Distal radius fracture |
| NCG | National clinical guideline |
| ED | Emergency department |
| ORIF | Open reduction internal fixation |
| PROMs | Patient-related outcome measures |
| OA | Osteoarthritis |
| Quick-DASH | Quick-disabilities of the arm, shoulder and hand |
| PRWHE | Patient-rated wrist/hand evaluation |
| MCID | Minimal clinical important difference |
| NRS | Numeric rating scale |
| ROM | Range of motion |
| ASA | American Society of Anaesthesiologists |
| EQ5D | EuroQol-5 Domain |
| RCT | Randomized controlled trial |
References
- Bäßgen, K.; Westphal, T.; Haar, P.; Kundt, G.; Mittlmeier, T.; Schober, H.-C. Population-based prospective study on the incidence of osteoporosis-associated fractures in a German population of 200 413 inhabitants. J. Public Health 2012, 35, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Nellans, K.W.; Kowalski, E.; Chung, K.C. The epidemiology of distal radius fractures. Hand Clin. 2012, 28, 113–125. [Google Scholar] [CrossRef]
- Sundhedsstyrelsen. National Klinisk Retningslinje for Behandling af Håndledsnære Brud (Distal Radiusfraktur) 2017. 2022. Available online: https://www.sst.dk/-/media/Udgivelser/2014/NKR-H%C3%A5ndledsn%C3%A6re-underarmsbrud/National-klinisk-retningslinie-for-behandling-af-haandledsnaere-brud.ashx?la=da&hash=7CB223E245904E51A3B96DB08180CB01A17D229A (accessed on 10 January 2025).
- (AAOS) AA of, OS. Management of Distal Radius Fractures Evidence-Based Clinical Practice Guideline 2020. Available online: www.aaos.org/drfcpg (accessed on 10 January 2025).
- Mellstrand-Navarro, C.; Pettersson, H.J.; Tornqvist, H.; Ponzer, S. The operative treatment of fractures of the distal radius is increasing: Results from a nationwide Swedish study. Bone Joint J. 2014, 96-b, 963–969. [Google Scholar] [CrossRef]
- Chung, K.C.; Shauver, M.J.; Birkmeyer, J.D. Trends in the United States in the treatment of distal radial fractures in the elderly. J. Bone Joint Surg. Am. 2009, 91, 1868–1873. [Google Scholar] [CrossRef] [PubMed]
- Egol, K.A.; Walsh, M.; Romo-Cardoso, S.; Dorsky, S.; Paksima, N. Distal radial fractures in the elderly: Operative compared with nonoperative treatment. J. Bone Joint Surg. Am. 2010, 92, 1851–1857. [Google Scholar] [CrossRef]
- Wæver, D.; Madsen, M.L.; Rölfing, J.H.D.; Borris, L.C.; Henriksen, M.; Nagel, L.L.; Thorninger, R. Distal radius fractures are difficult to classify. Injury 2018, 49 (Suppl. 1), S29–S32. [Google Scholar] [CrossRef]
- Hassellund, S.S.; Williksen, J.H.; Laane, M.M.; Pripp, A.; Rosales, C.P.; Karlsen, Ø.; Madsen, J.E.; Frihagen, F. Cast immobilization is non-inferior to volar locking plates in relation to QuickDASH after one year in patients aged 65 years and older: A randomized controlled trial of displaced distal radius fractures. Bone Joint J. 2021, 103-b, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Luokkala, T.; Laitinen, M.K.; Hevonkorpi, T.P.; Raittio, L.; Mattila, V.M.; Launonen, A.P. Distal radius fractures in the elderly population. EFORT Open Rev. 2020, 5, 361–370. [Google Scholar] [CrossRef]
- Lawson, A.; Naylor, J.M.; Buchbinder, R.; Ivers, R.; Balogh, Z.J.; Smith, P.; Xuan, W.; Howard, K.; Vafa, V.; Perriman, D.; et al. Surgical Plating vs Closed Reduction for Fractures in the Distal Radius in Older Patients: A Randomized Clinical Trial. JAMA Surg. 2021, 156, 229–237. [Google Scholar] [CrossRef]
- Li, Q.; Ke, C.; Han, S.; Xu, X.; Cong, Y.X.; Shang, K.; Liang, J.D.; Zhang, B.F. Nonoperative treatment versus volar locking plate fixation for elderly patients with distal radial fracture: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2020, 15, 263. [Google Scholar] [CrossRef] [PubMed]
- Thorninger, R.; Wæver, D.; Tjørnild, M.; Lind, M.; Rölfing, J.D. VOLCON: A randomized controlled trial investigating complications and functional outcome of volar plating vs casting of unstable distal radius fractures in patients older than 65 years. J. Orthop. Traumatol. 2022, 23, 54. [Google Scholar] [CrossRef] [PubMed]
- Südow, H.; Severin, S.; Wilcke, M.; Saving, J.; Sköldenberg, O.; Navarro, C.M. Non-operative treatment or volar locking plate fixation for dorsally displaced distal radius fractures in patients over 70 years—A three year follow-up of a randomized controlled trial. BMC Musculoskelet. Disord. 2022, 23, 447. [Google Scholar] [CrossRef]
- Martinez-Mendez, D.; Lizaur-Utrilla, A.; de-Juan-Herrero, J. Intra-articular distal radius fractures in elderly patients: A randomized prospective study of casting versus volar plating. J. Hand Surg. Eur. Vol. 2018, 43, 142–147. [Google Scholar] [CrossRef]
- Lawson, A.; Naylor, J.; Buchbinder, R.; Ivers, R.; Balogh, Z.J.; Smith, P.; Xuan, W.; Howard, K.; Vafa, A.; Perriman, D.; et al. Plating vs Closed Reduction for Fractures in the Distal Radius in Older Patients. JAMA Surg. 2022, 157, 563. [Google Scholar] [CrossRef]
- Pedersen, J.; Mortensen, S.O.; Rölfing, J.D.; Thorninger, R. A protocol for a single-center, single-blinded randomized-controlled trial investigating volar plating versus conservative treatment of unstable distal radius fractures in patients older than 65 years. BMC Musculoskelet. Disord. 2019, 20, 309. [Google Scholar] [CrossRef]
- Knirk, J.L.; Jupiter, J.B. Intra-articular fractures of the distal end of the radius in young adults. J. Bone Joint Surg. Am. 1986, 68, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef]
- Mintken, P.E.; Glynn, P.; Cleland, J.A. Psychometric properties of the shortened disabilities of the Arm, Shoulder, and Hand Questionnaire (QuickDASH) and Numeric Pain Rating Scale in patients with shoulder pain. J. Shoulder Elbow Surg. 2009, 18, 920–926. [Google Scholar] [CrossRef]
- Schønnemann, J.O.; Eggers, J. Validation of the Danish version of the Quick-Disabilities of Arm, Shoulder and Hand Questionnaire. Dan. Med. J. 2016, 63, A5306. [Google Scholar]
- Hansen, A.Ø.; Knygsand-Roenhoej, K.; Ardensø, K. Danish version of the Patient-Rated Wrist/Hand Evaluation questionnaire: Translation, cross-cultural adaptation, test–retest reliability and construct validity. Hand Ther. 2018, 24, 22–30. [Google Scholar] [CrossRef]
- Walenkamp, M.M.; de Muinck Keizer, R.J.; Goslings, J.C.; Vos, L.M.; Rosenwasser, M.P.; Schep, N.W. The Minimum Clinically Important Difference of the Patient-rated Wrist Evaluation Score for Patients With Distal Radius Fractures. Clin. Orthop. Relat. Res. 2015, 473, 3235–3241. [Google Scholar] [CrossRef] [PubMed]
- Visser, D.; Mathijssen, N.M.C.; van Outeren, M.V.; Colaris, J.W.; de Vries, M.R.; Kraan, G.A. Long-term follow-up of distal radius fractures, an evaluation of the current guideline: The relation between malunion, osteoarthritis and functional outcome. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 1357–1362. [Google Scholar] [CrossRef]
- Home, J.G.; Devane, P.; Purdie, G. A Prospective Randomized Trial of External Fixation and Plaster Cast Immobilization in the Treatment of Distal Radial Fractures. J. Orthop. Trauma. 1990, 4, 30–34. [Google Scholar] [CrossRef]
- Lutz, M.; Arora, R.; Krappinger, D.; Wambacher, M.; Rieger, M.; Pechlaner, S. Arthritis predicting factors in distal intraarticular radius fractures. Arch. Orthop. Trauma. Surg. 2011, 131, 1121–1126. [Google Scholar] [CrossRef]
- Andersson, J.K.; Hagert, E.; Brittberg, M. Cartilage Injuries and Posttraumatic Osteoarthritis in the Wrist: A Review. Cartilage 2021, 13, 156S–168S. [Google Scholar] [CrossRef]
- Driban, J.B.; Eaton, C.B.; Lo, G.H.; Ward, R.J.; Lu, B.; McAlindon, T.E. Association of Knee Injuries With Accelerated Knee Osteoarthritis Progression: Data From the Osteoarthritis Initiative. Arthritis Care Res. 2014, 66, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Driban, J.B.; Harkey, M.S.; Barbe, M.F.; Ward, R.J.; MacKay, J.W.; Davis, J.E.; Lu, B.; Price, L.L.; Eaton, C.B.; Lo, G.H.; et al. Risk factors and the natural history of accelerated knee osteoarthritis: A narrative review. BMC Musculoskelet. Disord. 2020, 21, 332. [Google Scholar] [CrossRef]
- Logli, A.L.; Evans, C.H.; Duryea, J.; Larson, D.R.; Bakri, K.; Carlsen, B.T.; Dennison, D.G.; Karim, K.E.; Pulos, N.A.; Rhee, P.C.; et al. Investigation Into the Effects of Intra-Articular Steroid on Post-Traumatic Osteoarthritis in Distal Radius Fractures: A Randomized Controlled Pilot Study. J. Hand Surg. Am. 2024, 49, 757–765. [Google Scholar] [CrossRef]
- Davies, J.; Centomo, H.; Leduc, S.; Beaumont, P.; Laflamme, G.-Y.; Rouleau, D. Preexisting Carpal and Carpometacarpal Osteoarthritis Has No Impact on Function after Distal Radius Fractures. J. Wrist Surg. 2017, 6, 301–306. [Google Scholar] [CrossRef]
- Arora, R.; Lutz, M.; Deml, C.; Krappinger, D.; Haug, L.; Gabl, M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J. Bone Joint Surg. Am. 2011, 93, 2146–2153. [Google Scholar] [CrossRef] [PubMed]
- Woolnough, T.; Axelrod, D.; Bozzo, A.; Koziarz, A.; Koziarz, F.; Oitment, C.; Gyemi, L.; Gormley, J.; Gouveia, K.; Johal, H. What Is the Relative Effectiveness of the Various Surgical Treatment Options for Distal Radius Fractures? A Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Clin. Orthop. Relat. Res. 2021, 479, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, X.; Li, Z.; Yan, H.; Zhou, F.; Gao, W. Safety and Efficacy of Operative Versus Nonsurgical Management of Distal Radius Fractures in Elderly Patients: A Systematic Review and Meta-analysis. J. Hand Surg. Am. 2016, 41, 404–413. [Google Scholar] [CrossRef]
- Bell, K.; Oliver, W.; White, T.; Molyneux, S.; Clement, N.; Duckworth, A. OPERATIVE VERSUS NONOPERATIVE MANAGEMENT OF DISTAL RADIUS FRACTURES IN ADULTS: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CONTROLLED TRIALS WITH AN ELDERLY SUBGROUP ANALYSIS. Orthop. Proc. 2023, 105-B, 50. [Google Scholar] [CrossRef]
- Saving, J.; Severin Wahlgren, S.; Olsson, K.; Enocson, A.; Ponzer, S.; Sköldenberg, O.; Wilcke, M.; Navarro, C.M. Nonoperative Treatment Compared with Volar Locking Plate Fixation for Dorsally Displaced Distal Radial Fractures in the Elderly: A Randomized Controlled Trial. J. Bone Joint Surg. Am. 2019, 101, 961–969. [Google Scholar] [CrossRef]
- Ochen, Y.; Peek, J.; van der Velde, D.; Beeres, F.J.P.; van Heijl, M.; Groenwold, R.H.H.; Houwert, R.M.; Heng, M. Operative vs Nonoperative Treatment of Distal Radius Fractures in Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e203497. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Chen, Y.-J.; Fang, E.; Wong, T.-M.; Liu, Z.-H.; Lau, T.-W.; Fok, M.W.M.; Yee, D.K.; Pun, T.; Luo, C.-F.; et al. Patient expectations predict outcomes following distal radius fracture: A prospective cohort study using the TEFTOM questionnaire. Injury 2021, 52, 877–882. [Google Scholar] [CrossRef]
- Jayakumar, P.; Teunis, T.; Vranceanu, A.-M.; Lamb, S.; Williams, M.; Ring, D.; Gwilym, S. Construct Validity and Precision of Different Patient-reported Outcome Measures During Recovery After Upper Extremity Fractures. Clin. Orthop. Relat. Res. 2019, 477, 2521–2530. [Google Scholar] [CrossRef]
- van Leerdam, R.H.; Huizing, F.; Termaat, F.; Kleinveld, S.; Rhemrev, S.J.; Krijnen, P.; Schipper, I.B. Patient-reported outcomes after a distal radius fracture in adults: A 3–4 years follow-up. Acta Orthop. 2019, 90, 129–134. [Google Scholar] [CrossRef]
- Bhandari, M.; Guyatt, G.H.; Tong, D.; Adili, A.; Shaughnessy, S.G. Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: A systematic overview and meta-analysis. J. Orthop. Trauma. 2000, 14, 2–9. [Google Scholar] [CrossRef]
- Bhandari, M.; Guyatt, G.H.; Swiontkowski, M.F.; Schemitsch, E.H. Treatment of open fractures of the shaft of the tibia. J. Bone Joint Surg. Br. 2001, 83, 62–68. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Available at Follow-Up at 2 Years | Lost to Follow-Up 1–2 Years | |||
|---|---|---|---|---|
| n = 60 | n = 25 | |||
| Non-Operative | Operative | Non-Operative | Operative | |
| n = 32 | n = 28 | n = 14 | n = 11 | |
| Women [n/N (%)] | 26/32 (81%) | 22/28 (78%) | 11/14 (79%) | 8/11 (73%) |
| Fractured dominant side [n/N (%)] | 13/32 (41%) | 13/28 (46%) | 8/14 (57%) | 4/11 (36%) |
| Median age (range) [years] | 73 (66–92) | 72 (65–87) | 78 (65–91) | 78 (69–91) |
| Retired | 31/32 (97%) | 28/28 (100%) | 14/14 (100%) | 11/11 (100%) |
| ASA 1/ASA 2/ASA 3 [n] | 10/19/3 | 11/16/1 | 2/9/3 | 3/7/1 |
| Non-Operative | Operative | |||
|---|---|---|---|---|
| PA Grade | 5 Weeks | 2 Years | 5 Weeks | 2 Years |
| 0 | 22 | 14 | 30 | 7 |
| 1 | 4 | 7 | 1 | 16 |
| 2 | 1 | 5 | 0 | 6 |
| 3 | 0 | 1 | 0 | 2 |
| Quick-DASH | PRWHE | Pain (NRS 0–10) | ||||
|---|---|---|---|---|---|---|
| Non-Operative | Operative | Non-Operative | Operative | Non-Operative | Operative | |
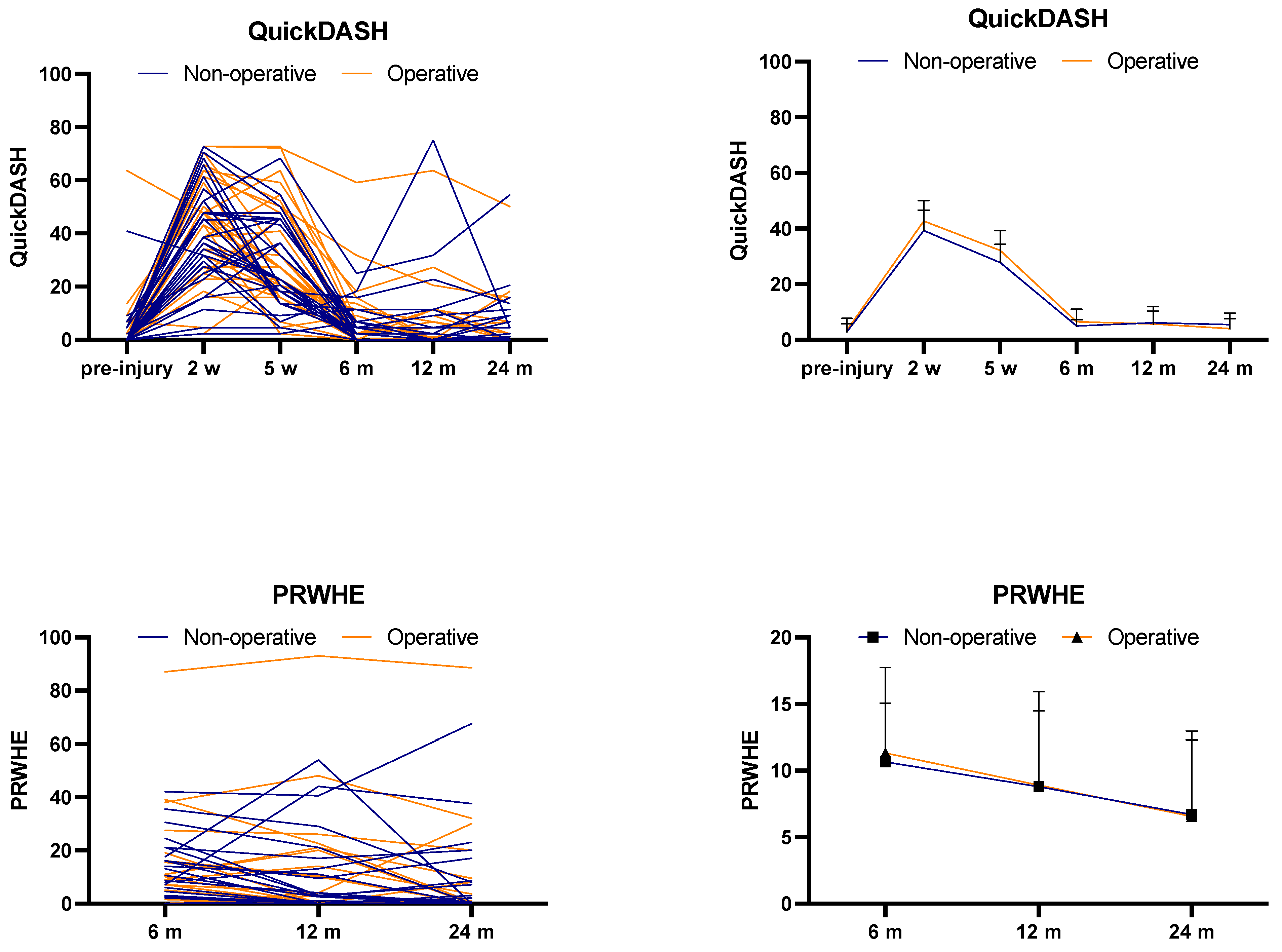
| 6 months | 2.3 (0.0; 0.0–6.8; 25) | 2.3 (0.0; 0.0–6.8; 59) | 6.5 (0.0; 0.5–16; 42) | 7.0 (0.0; 0.0–15; 87) | 0 (0; 0–1; 5) | 0 (0; 0–1; 5) |
| 1 year | 0.0 (0.0; 0.0–4.5; 75) | 0.0 (0.0; 0.0–6.2; 64) | 0.5 (0.0; 0.0–13; 54) | 0.0 (0.0; 0.0–10; 93) | 0 (0; 0–0; 5) | 0 (0; 0–0; 7) |
| 2 years | 0.5 (0.0; 0.0–8.5; 55) | 0.0 (0.0; 0.0–2.3; 50) | 0.0 (0.0; 0.0–8; 68) | 0.0 (0.0; 0.0–3; 89) | 0 (0; 0–0; 5) | 0 (0; 0–0; 5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wæver, D.; Thorninger, R.; Romme, K.L.; Tjørnild, M.; Rölfing, J.D. Post-Traumatic Osteoarthritis and Functional Outcomes After Volar Plating vs. Casting of Unstable Distal Radius Fractures: A Minimum 2-Year Follow-Up of the VOLCON Randomized Controlled Trial. J. Clin. Med. 2025, 14, 3766. https://doi.org/10.3390/jcm14113766
Wæver D, Thorninger R, Romme KL, Tjørnild M, Rölfing JD. Post-Traumatic Osteoarthritis and Functional Outcomes After Volar Plating vs. Casting of Unstable Distal Radius Fractures: A Minimum 2-Year Follow-Up of the VOLCON Randomized Controlled Trial. Journal of Clinical Medicine. 2025; 14(11):3766. https://doi.org/10.3390/jcm14113766
Chicago/Turabian StyleWæver, Daniel, Rikke Thorninger, Karen Larsen Romme, Michael Tjørnild, and Jan Duedal Rölfing. 2025. "Post-Traumatic Osteoarthritis and Functional Outcomes After Volar Plating vs. Casting of Unstable Distal Radius Fractures: A Minimum 2-Year Follow-Up of the VOLCON Randomized Controlled Trial" Journal of Clinical Medicine 14, no. 11: 3766. https://doi.org/10.3390/jcm14113766
APA StyleWæver, D., Thorninger, R., Romme, K. L., Tjørnild, M., & Rölfing, J. D. (2025). Post-Traumatic Osteoarthritis and Functional Outcomes After Volar Plating vs. Casting of Unstable Distal Radius Fractures: A Minimum 2-Year Follow-Up of the VOLCON Randomized Controlled Trial. Journal of Clinical Medicine, 14(11), 3766. https://doi.org/10.3390/jcm14113766