
The Prognostic Impact of Kidney Dysfunction in Unselected Patients Undergoing Coronary Angiography: In What Subgroups Does Kidney Dysfunction Matter?
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Patients, Design, and Data Collection
2.2. Inclusion and Exclusion Criteria
2.3. Risk Stratification
2.4. Study Endpoints
2.5. Statistical Methods
3. Results
3.1. Study Population
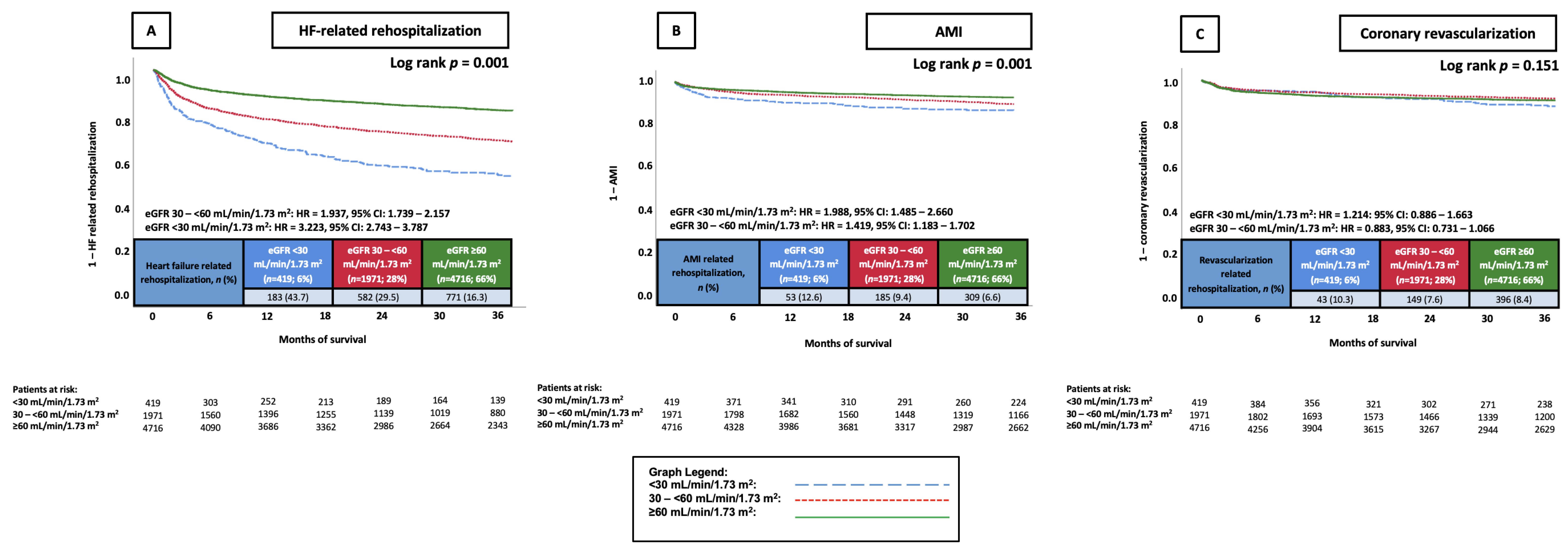
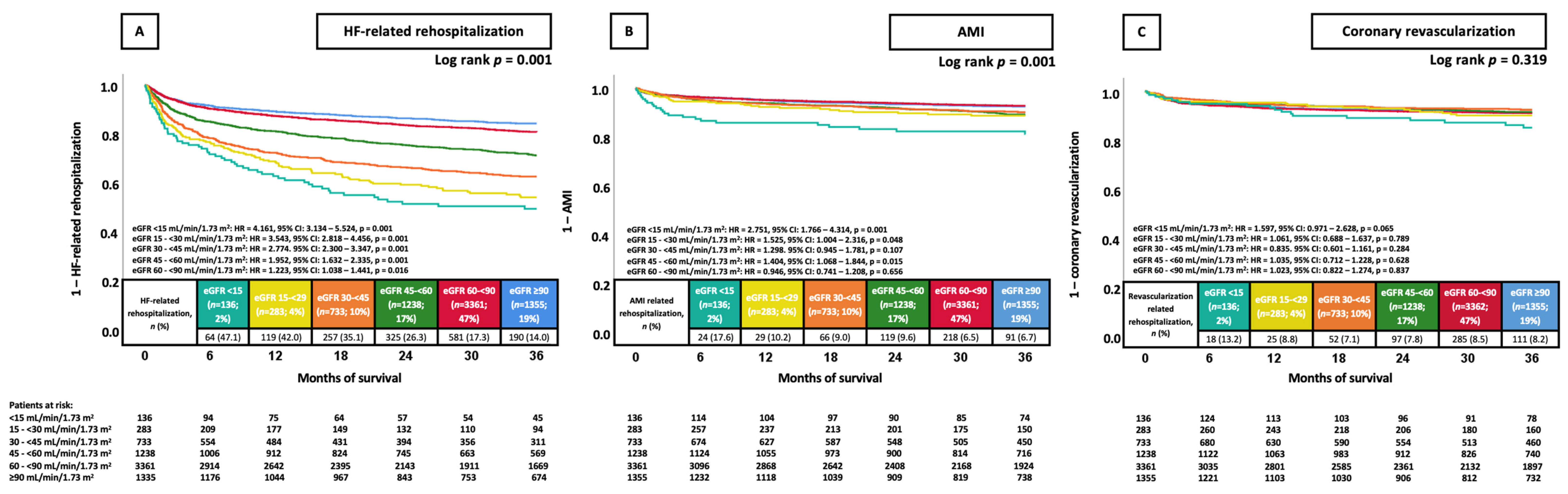
3.2. Prognostic Value of Reduced Kidney Function in Patients Undergoing CA
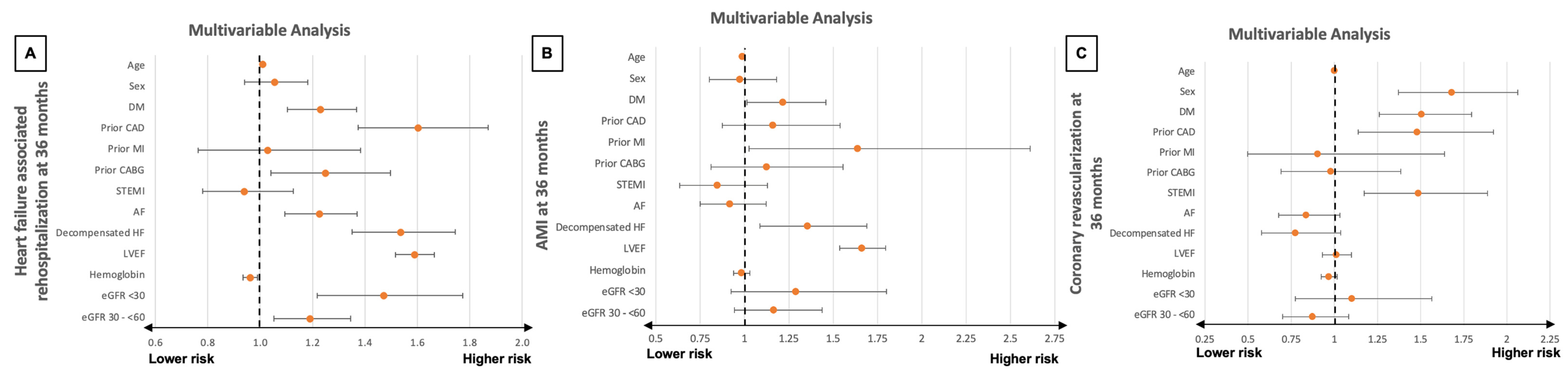
3.3. Multivariable Cox Regression Analyses
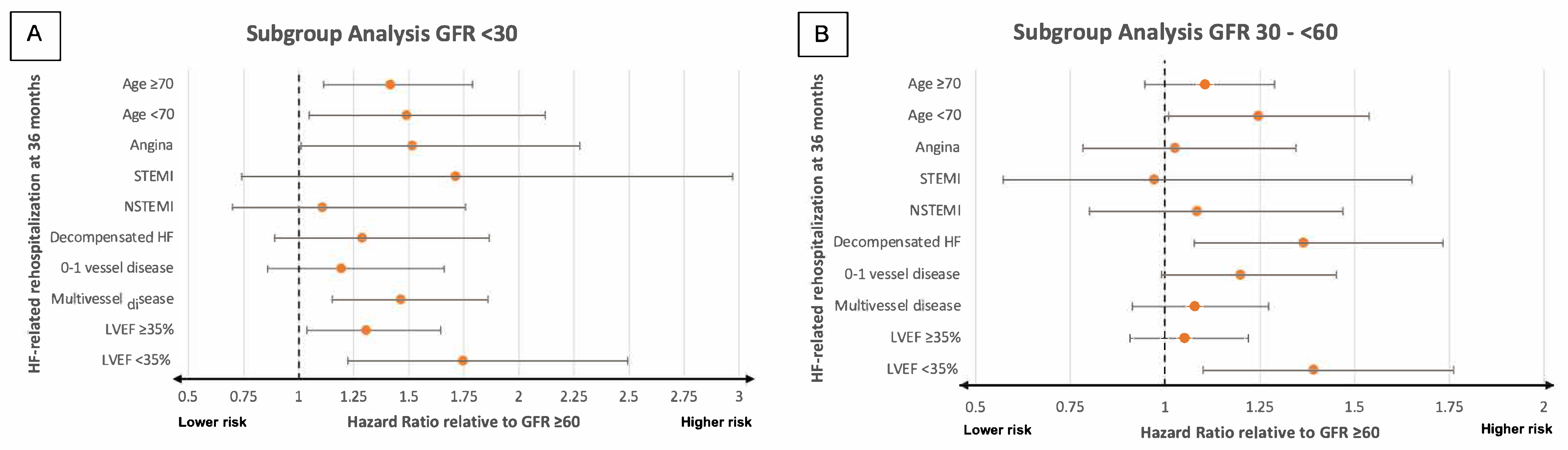
3.4. Prognostic Impact of Kidney Dysfunction in Pre-Specified Subgroups
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khera, A.V.; Kathiresan, S. Genetics of coronary artery disease: Discovery, biology and clinical translation. Nat. Rev. Genet. 2017, 18, 331–344. [Google Scholar] [CrossRef]
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef]
- Brown, J.C.; Gerhardt, T.E.; Kwon, E. Risk Factors for Coronary Artery Disease; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. [Google Scholar]
- Nakamura, M.; Yamashita, T.; Yajima, J.; Oikawa, Y.; Ogasawara, K.; Kirigaya, H.; Sagara, K.; Koike, A.; Sawada, H.; Aizawa, T. Impact of reduced renal function on prognosis in Japanese patients with coronary artery disease: A prospective cohort of Shinken Database 2007. Hypertens. Res. 2009, 32, 920–926. [Google Scholar] [CrossRef]
- Manjunath, G.; Tighiouart, H.; Ibrahim, H.; MacLeod, B.; Salem, D.N.; Griffith, J.L.; Coresh, J.; Levey, A.S.; Sarnak, M.J. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J. Am. Coll. Cardiol. 2003, 41, 47–55. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef]
- Shantouf, R.S.; Budoff, M.J.; Ahmadi, N.; Ghaffari, A.; Flores, F.; Gopal, A.; Noori, N.; Jing, J.; Kovesdy, C.P.; Kalantar-Zadeh, K. Total and individual coronary artery calcium scores as independent predictors of mortality in hemodialysis patientes. Am. J. Nephrol. 2010, 31, 419–425. [Google Scholar] [CrossRef]
- Rear, R.; Meier, P.; Bell, R.M. Implications of Kidney Disease in the Cardiac Patient. Interv. Cardiol. Clin. 2014, 3, 317–331. [Google Scholar] [CrossRef]
- Culleton, B.F.; Larson, M.G.; Wilson, P.W.F.; Evans, J.C.; Parfrey, P.S.; Levy, D. Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int. 1999, 56, 2214–2219. [Google Scholar] [CrossRef]
- Luke, R.G. Chronic Renal Failure—A Vasculopathic State. N. Engl. J. Med. 1998, 339, 841–843. [Google Scholar] [CrossRef]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Liao, L.; Aw, T.Y.; Kvietys, P.R.; Granger, D.N. Oxidized LDL–Induced Microvascular Dysfunction. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 2305–2311. [Google Scholar] [CrossRef]
- Bakris, G.L. Lipid Disorders in Uremia and Dialysis. Contrib. Nephrol. 2012, 178, 100–105. [Google Scholar]
- Krane, V.; Wanner, C. Statins, inflammation and kidney disease. Nat. Rev. Nephrol. 2011, 7, 385–397. [Google Scholar] [CrossRef]
- Schiffrin, E.L.; Lipman, M.L.; Mann, J.F.E. Chronic Kidney Disease. Circulation 2007, 116, 85–97. [Google Scholar] [CrossRef]
- Pannier, B.; Guérin, A.P.; Marchais, S.J.; Safar, M.E.; London, G.R.M. Stiffness of Capacitive and Conduit Arteries. Hypertension 2005, 45, 592–596. [Google Scholar] [CrossRef]
- Kestenbaum, B.R.; Adeney, K.L.; De Boer, I.H.; Ix, J.H.; Shlipak, M.G.; Siscovick, D.S. Incidence and progression of coronary calcification in chronic kidney disease: The Multi-Ethnic Study of Atherosclerosis. Kidney Int. 2009, 76, 991–998. [Google Scholar] [CrossRef]
- Budoff, M.J.; Rader, D.J.; Reilly, M.P.; Mohler, E.R.; Lash, J.; Yang, W.; Rosen, L.; Glenn, M.; Teal, V.; Feldman, H.I.; et al. Relationship of Estimated GFR and Coronary Artery Calcification in the CRIC (Chronic Renal Insufficiency Cohort) Study. Am. J. Kidney. Dis. 2011, 58, 519–526. [Google Scholar] [CrossRef]
- Bundy, J.D.; Chen, J.; Yang, W.; Budoff, M.; Go, A.S.; Grunwald, J.E.; Kallem, R.R.; Post, W.S.; Reilly, M.P.; Ricardo, A.C.; et al. Risk factors for progression of coronary artery calcification in patients with chronic kidney disease: The CRIC study. Atherosclerosis 2018, 271, 53–60. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.; Dweck, M.R.; Galbrait, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart. J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Doganer, Y.C.; Rohrer, J.E.; Aydogan, U.; Barcin, C.; Cayci, T.; Saglam, K. Association of renal function, estimated by four equations, with coronary artery disease. Int. Urol. Nephrol. 2015, 47, 663–671. [Google Scholar] [CrossRef]
- Chen, S.; Zhou, Y.; Liang, G.; Wu, W.; Huang, Z.; Shi, L.; Gao, Y.; Gu, X.; Wang, D. Predictive effect of estimated glomerular filtrate rate by creatinine or cystatin C on mortality in patients with coronary artery disease. Ren. Fail. 2024, 46, 2327494. [Google Scholar] [CrossRef]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease—Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Carrero, J.J.; Axelsson, J.; Lindholm, B.; Heimbürger, O.; Massy, Z.A. Emerging biomarkers for evaluating cardiovascular risk in the chronic kidney disease patient: How do new pieces fit into the uremic puzzle? J. Intern. Med. 2008, 264, 517–532. [Google Scholar] [CrossRef]
- Duranton, F.; Cohen, G.; De Smet, R.; Rodriguez, M.; Jankowski, J.; Vanholder, R.; Argilés, A. Normal and pathologic concentrations of uremic toxins. J. Am. Soc. Nephrol. 2012, 23, 1258–1270. [Google Scholar] [CrossRef]
- Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A. Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef]
- Lindner, A.; Charra, B.; Sherrard, D.J.; Scribner, B.H. Accelerated atherosclerosis in prolonged maintenance hemodialysis. N. Engl. J. Med. 1974, 290, 697–701. [Google Scholar] [CrossRef]
- Christoffersen, C.B.E.; Aarup, A.; Nielsen, L.B.; Pedersen, T.X. ApoB and apoM—New aspects of lipoprotein biology in uremia-induced atherosclerosis. Eur. J. Pharmocol. 2017, 816, 154–160. [Google Scholar] [CrossRef]
- Massy, Z.A.; Ivanovski, O.; Nguyen-Khoa, T.; Angulo, J.; Szumilak, D.; Mothu, N.; Phan, O.; Daudon, M.; Lacour, B.; Drüeke, T.; et al. Uremia Accelerates both Atherosclerosis and Arterial Calcification in Apolipoprotein E Knockout Mice. J. Am. Soc. Nephrol. 2005, 16, 109–116. [Google Scholar] [CrossRef]
- Kawtharany, L.; Bessueille, L.; Issa, H.; Hamade, E.; Zibara, K.; Magne, D. Inflammation and Microcalcification: A Never-Ending Vicious Cycle in Atherosclerosis? J. Vas. Res. 2022, 59, 137–150. [Google Scholar] [CrossRef]
- Zoccali, C.; Bode-Böger, S.M.; Mallamaci, F.; Benedetto, F.A.; Tripepi, G.; Malatino, L.S.; Cataliotti, A.; Bellanuova, I.; Fermo, I.; Frolich, J.C.; et al. Plasma concentration of asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: A prospective study. Lancet 2001, 358, 2113–2117. [Google Scholar] [CrossRef]
- Mazzaferro, S.; Pasquali, M.; Taggi, F.; Baldinelli, M. Progression of coronary artery calcification in predialysis patients with CKD: A prospective study. Kidney Int. 2014, 86, 668–675. [Google Scholar]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Piscitelli, P.; D’Errico, M.M.; Mirijello, A.; Santoliquido, M.; Salvatori, M.; Vigna, C.; Marchese, N.; Vendemiale, G.; Copetti, M.; Pontremoli, R.; et al. Low GFR amplifies the association between coronary three-vessel disease and all-cause mortality. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 402–409. [Google Scholar] [CrossRef]
- D’Errico, M.M.; Mangiacotti, A.; Graziano, D.; Massa, V.; Piscitelli, P.; Vendemiale, G.; Viazzi, F.; Pontremoli, R.; Russo, A.; Marchese, N.; et al. Kidney disease measures are associated with the burden of coronary atherosclerosis, independently of diabetes. Acta. Diabetol. 2017, 54, 1065–1068. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 2003, 42, 1050–1065. [Google Scholar] [CrossRef]
- Dupuis, M.E.; Nadeau-Fredette, A.C.; Madore, F.; Agharazii, M.; Goupil, R. Association of Glomerular Hyperfiltration and Cardiovascular Risk in Middle-Aged Healthy Individuals. JAMA Netw. Open 2020, 3, e202377. [Google Scholar] [CrossRef]
- Astor, B.C.; Levey, A.S.; Stevens, L.A.; Van Lente, F.; Selvin, E.; Coresh, J. Method of glomerular filtration rate estimation affects prediction of mortality risk. J. Am. Soc. Nephrol. 2009, 20, 2214–2222. [Google Scholar] [CrossRef]
- Donfrancesco, C.; Palleschi, S.; Palmieri, L.; Rossi, B.; Lo Noce, C.; Pannozzo, F.; Spoto, B.; Tripepi, G.; Zoccali, C.; Giampaoli, S. Estimated glomerular filtration rate, all-cause mortality and cardiovascular diseases incidence in a low risk population: The MATISS study. PLoS ONE 2013, 8, e78475. [Google Scholar] [CrossRef]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [PubMed]
- Consortium Kidney Disease Prognosis Consortium; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [PubMed]
- Park, M.; Yoon, E.; Lim, Y.H.; Kim, H.; Choi, J.; Yoon, H.J. Renal hyperfiltration as a novel marker of all-cause mortality. J. Am. Soc. Nephrol. 2015, 26, 1426–1433. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, B.O.; Løchen, M.L.; Arntzen, K.A.; Bertelsen, G.; Eilertsen, B.A.; von Hanno, T.; Herder, M.; Jenssen, T.G.; Mathisen, U.D.; Melsom, T.; et al. Subclinical cardiovascular disease is associated with a high glomerular filtration rate in the nondiabetic general population. Kidney Int. 2014, 86, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.M.; Hyun, Y.Y.; Lee, K.B.; Kim, H. High estimated glomerular filtration rate is associated with coronary artery calcification in middle-aged Korean men without chronic kidney disease. Nephrol. Dial. Transplant. 2015, 30, 996–1001. [Google Scholar] [CrossRef]
- Spadafora, L.; Betti, M.; D’Ascenzo, F.; De Ferrari, G.; De Filippo, O.; Gaudio, C.; Collet, C.; Sabouret, P.; Agostoni, P.; Zivelonghi, C.; et al. Impact of In-Hospital Bleeding on Post-Discharge Therapies and Prognosis in Acute Coronary Syndromes. J. Cardiovasc. Pharmacol. 2025, 85, 322–328. [Google Scholar] [CrossRef]
- Hakopian, N.N.; Gharibian, D.; Nashed, M.M. Prognostic Impact of Chronic Kidney Disease in Patients with Heart Failure. Perm. J. 2019, 23, 18–273. [Google Scholar] [CrossRef]
- Park, C.S.; Park, J.J.; Oh, I.Y.; Yoon, C.H.; Choi, D.J.; Park, H.A.; Kang, S.M.; Yoo, E.S.; Kim, J.J.; Cho, M.C.; et al. Relation of Renal Function with Left Ventricular Systolic Function and NT-proBNP Level and Its Prognostic Implication in Heart Failure with Preserved versus Reduced Ejection Fraction: An analysis from the Korean Heart Failure (KorHF) Registry. Korean Circ. J. 2017, 47, 727–741. [Google Scholar] [CrossRef]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Ostergren, J.; Cornel, J.H.; et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006, 113, 671–678. [Google Scholar] [CrossRef]
- McAlister, F.A.; Ezekowitz, J.; Tarantini, L.; Squire, I.; Komajda, M.; Bayes-Genis, A.; Gotsman, I.; Whalley, G.; Earle, N.; Poppe, K.K.; et al. Renal dysfunction in patients with heart failure with preserved versus reduced ejection fraction: Impact of the new Chronic Kidney Disease-Epidemiology Collaboration Group formula. Circ. Heart. Fail. 2012, 5, 309–314. [Google Scholar] [CrossRef]
- Ahmed, A.; Rich, M.W.; Sanders, P.W.; Perry, G.J.; Bakris, G.L.; Zile, M.R.; Love, T.E.; Aban, I.B.; Shlipak, M.G. Chronic kidney disease associated mortality in diastolic versus systolic heart failure: A propensity matched study. Am. J. Cardiol. 2007, 99, 393–398. [Google Scholar] [CrossRef]
- Damman, K.; Valente, M.A.E.; Voors, A.A.; O’Connor, C.M.; van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur. Heart J. 2013, 35, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Schupp, T.; Weidner, K.; Lau, F.; Forner, J.; Schmitt, A.; Reinhardt, M.; Abel, N.; Ayasse, N.; Bertsch, T.; Akin, M.; et al. Effect of severity and etiology of chronic kidney disease in patients with heart failure with mildly reduced ejection fraction. Clin. Res. Cardiol. 2024, 113, 1565–1575. [Google Scholar] [CrossRef]
- Mielniczuk, L.M.; Pfeffer, M.A.; Lewis, E.F.; Blazing, M.A.; de Lemos, J.A.; Shui, A.; Mohanavelu, S.; Califf, R.M.; Braunwald, E. Estimated glomerular filtration rate, inflammation, and cardiovascular events after an acute coronary syndrome. Am. Heart J. 2008, 155, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Anavekar, N.S.; McMurray, J.J.; Velazquez, E.J.; Solomon, S.D.; Kober, L.; Rouleau, J.L.; White, H.D.; Nordlander, R.; Maggioni, A.; Dickstein, K.; et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N. Engl. J. Med. 2004, 351, 1285–1295. [Google Scholar] [CrossRef]
- Yandrapalli, S.; Christy, J.; Malik, A.; Wats, K.; Harikrishnan, P.; Aronow, W.; Frishman, W. Impact of Acute and Chronic Kidney Disease on Heart Failure Hospitalizations After Acute Myocardial Infarction. Am. J. Cardiol. 2022, 165, 1–11. [Google Scholar] [CrossRef]
- Moukarbel, G.V.; Yu, Z.F.; Dickstein, K.; Hou, Y.R.; Wittes, J.T.; McMurray, J.J.; Pitt, B.; Zannad, F.; Pfeffer, M.A.; Solomon, S.D. The impact of kidney function on outcomes following high risk myocardial infarction: Findings from 27 610 patients. Eur. J. Heart. Fail. 2014, 16, 289–299. [Google Scholar] [CrossRef]
- Li, C.; Hu, D.; Ma, C.; Yang, J.; Song, L.; Shi, X. The impact of admission renal dysfunction on in-hospital and long-term outcome of patients with ST-elevation myocardial infarction in Beijing. Chin. J. Intern. Med. 2015, 54, 501–505. [Google Scholar]
- Pasha, K.; Ali, M.A.; Habib, M.A.; Debnath, R.C.; Islam, M.N. In-hospital outcome of patients with acute STEMI with impaired renal function. Mymensingh Med. J. 2011, 20, 425–430. [Google Scholar] [PubMed]
- Pavlovic, A.S.; Milasinovic, D.; Mehmedbegovic, Z.; Dedovic, V.; Jelic, D.; Zaharijev, S.; Zobenica, V.; Zivkovic, I.; Dudic, J.; Vukcevic, V.; et al. Synergistic impact of renal failure and left ventricular dysfunction on short- and long-term mortality in patients with STEMI undergoing primary PCI. Eur. Heart J. 2019, 40, 950. [Google Scholar] [CrossRef]
- Bernard, V.; El Khoury, C.; Fraticelli, L.; OSCAR Research Group. Impact of renal dysfunction in patients with acute myocardial infarction on early management and outcome: A first observational French study. Eur. Heart J. 2019, 40, 3614. [Google Scholar] [CrossRef]
- Goldenberg, I.; Subirana, I.; Boyko, V.; Vila, J.; Elosua, R.; Permanyer-Miralda, G.; Ferreira-Gonzalez, I.; Benderly, M.; Guetta, V.; Behar, S.; et al. Relation between renal function and outcomes in patients with non-ST-segment elevation acute coronary syndrome: Real-world data from the European Public Health Outcome Research and Indicators Collection Project. Arch. Intern. Med. 2010, 170, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Hanna, E.B.; Chen, A.Y.; Roe, M.T.; Wiviott, S.D.; Fox, C.S.; Saucedo, J.F. Characteristics and in-hospital outcomes of patients with non-ST-segment elevation myocardial infarction and chronic kidney disease undergoing percutaneous coronary intervention. JACC Cardiovasc. Interv. 2011, 4, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Flores-Blanco, P.J.; López-Cuenca, Á.; Januzzi, J.L.; Marín, F.; Sánchez-Martínez, M.; Quintana-Giner, M.; Romero-Aniorte, A.I.; Valdés, M.; Manzano-Fernández, S. Comparison of Risk Prediction With the CKD-EPI and MDRD Equations in Non-ST-Segment Elevation Acute Coronary Syndrome. Clin. Cardiol. 2016, 39, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.T.; Chen, Y.L.; Wu, C.J. Impact of chronic kidney disease on clinical outcomes in patients with non-ST elevation myocardial infarction receiving percutaneous coronary intervention—A five-year observational study. Int. J. Cardiol. 2016, 220, 166–172. [Google Scholar] [CrossRef]
- Vavalle, J.P.; van Diepen, S.; Clare, R.M.; Hochman, J.S.; Weaver, W.D.; Mehta, R.H.; Pieper, K.S.; Patel, M.R.; Patel, U.D.; Armstrong, P.W.; et al. Renal failure in patients with ST-segment elevation acute myocardial infarction treated with primary percutaneous coronary intervention: Predictors, clinical and angiographic features, and outcomes. Am. Heart J. 2016, 173, 57–66. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Cesaro, A.; Gallinoro, E.; Gragnano, F.; Sardu, C.; Mileva, N.; Foà, A.; Armillotta, M.; Sansonetti, A.; et al. Impact of SGLT2-inhibitors on contrast-induced acute kidney injury in diabetic patients with acute myocardial infarction with and without chronic kidney disease: Insight from SGLT2-I AMI PROTECT registry. Diabetes Res. Clin. Pract. 2023, 202, 110766. [Google Scholar] [CrossRef]
- Schupp, T.; Behnes, M.; Rusnak, J.; Weidner, K.; Ruka, M.; Dudda, J.; Schmitt, A.; Forner, J.; Egner-Walter, S.; Ayasse, N.; et al. Predictors and Prognostic Impact of Early Acute Kidney Injury in Cardiogenic Shock: Results from a Monocentric, Prospective Registry. Cardiorenal Med. 2024, 14, 81–93. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| eGFR < 30 mL/min (n = 554) | eGFR 30–<60 mL/min (n = 2213) | eGFR ≥ 60 mL/min (n = 4857) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Age, median (IQR) | 76 | (68–82) | 77 | (69–82) | 65 | (56–75) | 0.001 |
| Male sex, n (%) | 333 | (60.1) | 1235 | (55.8) | 3391 | (69.8) | 0.001 |
| Body mass index, kg/m2, median (IQR) | 27.8 | (24.2–31.9) | 27.7 | (24.6–31.3) | 27.2 | (24.4–30.7) | 0.002 |
| Cardiovascular risk factors, n (%) | |||||||
| Arterial hypertension | 436 | (78.7) | 1915 | (86.5) | 4148 | (85.4) | 0.001 |
| Diabetes mellitus | 238 | (43.0) | 863 | (39.0) | 1193 | (24.6) | 0.001 |
| Hyperlipidemia | 156 | (28.2) | 695 | (31.4) | 1862 | (38.3) | 0.001 |
| Prior medical history, n (%) | |||||||
| Congestive heart failure | 120 | (21.7) | 303 | (13.7) | 249 | (5.1) | 0.001 |
| Pacemaker | 16 | (2.9) | 62 | (2.8) | 38 | (0.8) | 0.001 |
| COPD | 38 | (6.9) | 121 | (5.5) | 138 | (2.8) | 0.001 |
| Liver cirrhosis | 9 | (1.6) | 33 | (1.5) | 46 | (0.9) | 0.078 |
| Malignancy | 46 | (8.3) | 174 | (7.9) | 224 | (4.6) | 0.001 |
| Stroke | 6 | (1.1) | 29 | (1.3) | 25 | (0.5) | 0.002 |
| Comorbidities at index hospitalization, n (%) | |||||||
| Acute coronary syndrome | |||||||
| Unstable angina | 100 | (18.1) | 503 | (22.7) | 1423 | (29.3) | 0.001 |
| STEMI | 50 | (9.0) | 202 | (9.1) | 656 | (13.5) | 0.001 |
| NSTEMI | 111 | (20.0) | 375 | (16.9) | 899 | (18.5) | 0.142 |
| Atrial fibrillation | 202 | (36.5) | 805 | (36.4) | 994 | (20.5) | 0.001 |
| Atrial flutter | 13 | (2.3) | 59 | (2.7) | 88 | (1.8) | 0.061 |
| Acute decompensated heart failure | 112 | (20.2) | 419 | (18.9) | 394 | (8.1) | 0.001 |
| Cardiogenic shock | 66 | (11.9) | 151 | (6.8) | 104 | (2.1) | 0.001 |
| Atrioventricular block | 18 | (3.2) | 74 | (3.3) | 102 | (2.1) | 0.005 |
| Cardiopulmonary resuscitation | 83 | (15.0) | 191 | (8.6) | 277 | (5.7) | 0.001 |
| Out-of-hospital | 53 | (9.6) | 137 | (6.2) | 194 | (4.0) | 0.001 |
| In-hospital | 30 | (5.4) | 54 | (2.4) | 83 | (1.7) | 0.001 |
| Valvular heart disease | 143 | (25.8) | 530 | (23.9) | 618 | (12.7) | 0.001 |
| Stroke | 11 | (2.0) | 76 | (3.4) | 201 | (4.1) | 0.025 |
| LVEF, n (%) | |||||||
| >55 | 150 | (31.8) | 781 | (39.7) | 2387 | (54.2) | 0.001 |
| 45–55% | 95 | (20.1) | 442 | (22.5) | 997 | (22.6) | |
| 35–44% | 88 | (18.6) | 330 | (16.8) | 542 | (12.3) | |
| <35% | 139 | (29.4) | 414 | (21.0) | 477 | (10.8) | |
| Not documented | 82 | 246 | 454 | ||||
| eGFR < 30 mL/min (n = 554) | eGFR 30–<60 mL/min (n = 2213) | eGFR ≥ 60 mL/mi (n = 4857) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Coronary angiography, n (%) | |||||||
| No evidence of coronary artery disease | 110 | (19.9) | 600 | (27.1) | 1611 | (33.2) | 0.001 |
| One-vessel disease | 104 | (18.8) | 400 | (18.1) | 1015 | (20.9) | |
| Two-vessel disease | 121 | (21.8) | 449 | (20.3) | 987 | (20.3) | |
| Three-vessel disease | 219 | (39.5) | 764 | (34.5) | 1244 | (25.6) | |
| Right coronary artery | 311 | (56.1) | 1126 | (50.9) | 2113 | (43.5) | 0.001 |
| Left main trunk | 90 | (16.2) | 294 | (13.3) | 455 | (9.4) | 0.001 |
| Left anterior descending | 354 | (63.9) | 1297 | (58.6) | 2488 | (51.2) | 0.001 |
| Left circumflex | 299 | (54.0) | 1030 | (46.5) | 1845 | (38.0) | 0.001 |
| Ramus intermedius | 92 | (16.6) | 277 | (12.5) | 476 | (9.8) | 0.001 |
| CABG | 37 | (6.7) | 100 | (4.5) | 87 | (1.8) | 0.001 |
| Chronic total occlusion | 53 | (9.6) | 199 | (9.0) | 358 | (7.4) | 0.024 |
| PCI, n (%) | 242 | (43.7) | 945 | (42.7) | 2086 | (42.9) | 0.916 |
| Right coronary artery | 93 | (16.8) | 351 | (15.9) | 828 | (17.0) | 0.462 |
| Left main trunk | 30 | (5.4) | 106 | (4.8) | 152 | (3.1) | 0.001 |
| Left anterior descending | 116 | (20.9) | 496 | (22.4) | 1091 | (22.5) | 0.713 |
| Left circumflex | 78 | (14.1) | 315 | (14.2) | 688 | (14.2) | 0.995 |
| Ramus intermedius | 14 | (2.5) | 39 | (1.8) | 83 | (1.7) | 0.385 |
| CABG | 10 | (1.8) | 24 | (1.1) | 20 | (0.4) | 0.001 |
| Sent to CABG, n (%) | 26 | (4.7) | 95 | (4.3) | 216 | (4.4) | 0.909 |
| Procedural data | |||||||
| Number of stents, median (IQR) | 2 | (1–3) | 2 | (1–3) | 2 | (1–3) | 0.620 |
| Stent length, median (IQR) | 44 | (24–76) | 44 | (24–76) | 44 | (24–76) | 0.597 |
| Contrast, median (IQR) | 128 | (74–200) | 120 | (72–200) | 110 | (70–190) | 0.003 |
| Baseline laboratory values, median (IQR) | |||||||
| Sodium, mmol/L | 139 | 137–141) | 139 | (138–141) | 140 | (138–141) | 0.001 |
| Potassium, mmol/L | 4.3 | (4.0–4.7) | 4.0 | (3.7–4.3) | 3.9 | (3.7–4.1) | 0.001 |
| Calcium, mmol/L | 2.2 | (2.1–2.3) | 2.2 | (2.1–2.3) | 2.2 | (2.1–2.3) | 0.001 |
| Creatinine, mg/dL | 3.1 | (2.3–4.6) | 1.4 | (1.2–1.7) | 0.9 | (0.8–1.0) | 0.001 |
| eGFR, mL/min/1.73 m2 | 21.6 | (13.6–26.7) | 47.8 | (40.3–54.0) | 79.7 | (70.1–92.4) | 0.001 |
| Urea, mg/dL | 93.6 | (72.7–122.3) | 51.2 | (40.2–67.8) | 32.5 | (26.9–40.1) | 0.001 |
| Hemoglobin, g/dL | 10.8 | (9.4–12.0) | 12.5 | (10.9–13.9) | 13.7 | (12.4–14.8) | 0.001 |
| WBC count, x 109/L | 9.5 | (7.4–12.7) | 9.0 | (7.2–11.6) | 8.9 | (7.1–11.1) | 0.001 |
| Platelet count, x 109/L | 212 | (167–262) | 229 | (185–279) | 240 | (199–288) | 0.001 |
| HbA1c, % | 6.2 | (5.5–7.2) | 6.1 | (5.6–7.2) | 5.7 | (5.4–6.3) | 0.001 |
| LDL cholesterol, mg/dL | 82 | (61–106) | 95 | (72–124) | 111 | (84–141) | 0.001 |
| HDL cholesterol, mg/dL | 39 | (31–48) | 42 | (35–53) | 42 | (35–53) | 0.001 |
| Triglycerides, mg/dL | 136 | (101–201) | 129 | (97–178) | 124 | (92–173) | 0.001 |
| C-reactive protein, mg/L | 56 | (15–127) | 31 | (11–86) | 21 | (8–73) | 0.001 |
| Procalcitonin, µg/L | 0.90 | (0.30–4.27) | 0.43 | (0.15–1.93) | 0.26 | (0.10–1.25) | 0.001 |
| Albumin, g/L | 29.8 | (25.9–33.1) | 33.3 | (29.3–36.3) | 35.1 | (31.8–37.8) | 0.001 |
| INR | 1.10 | (1.02–1.29) | 1.08 | (1.02–1.22) | 1.05 | (1.00–1.11) | 0.001 |
| NT-pro BNP, pg/mL | 11,261 | (4395–31,255) | 3287 | (1237–7904) | 1168 | (284–3172) | 0.001 |
| Creatin Kinase, U/L | 134 | (72–353) | 125 | (78–250) | 138 | (85–312) | 0.001 |
| Creatin Kinase MB, U/L | 39 | (21–85) | 31 | (21–61) | 31 | (21–65) | 0.031 |
| Medication at discharge, n (%) | |||||||
| ACE-inhibitor | 160 | (38.2) | 927 | (47.0) | 2537 | (53.8) | 0.001 |
| ARB | 140 | (33.4) | 622 | (31.6) | 940 | (19.9) | 0.001 |
| Beta-blocker | 339 | (80.9) | 1513 | (76.8) | 3184 | (67.5) | 0.001 |
| Aldosterone antagonist | 54 | (12.9) | 426 | (21.6) | 590 | (12.5) | 0.001 |
| ARNI | 5 | (1.2) | 39 | (2.0) | 34 | (0.7) | 0.001 |
| SGLT2-inhibitor | 6 | (1.4) | 106 | (5.4) | 235 | (5.0) | 0.003 |
| Statin | 311 | (74.2) | 1455 | (73.8) | 3493 | (74.1) | 0.973 |
| ASA | 281 | (67.1) | 1163 | (59.0) | 3147 | (66.7) | 0.001 |
| P2Y12-inhibitor | 211 | (50.4) | 898 | (45.6) | 2260 | (47.9) | 0.097 |
| OAC | 133 | (31.7) | 820 | (41.6) | 1030 | (21.8) | 0.001 |
| Follow-up data, median (IQR) | |||||||
| Hospitalization time | 10 | (4–18) | 8 | (4–14) | 6 | (4–11) | 0.001 |
| ICU time | 0 | (0–0) | 0 | (0–0) | 0 | (0–0) | 0.032 |
| Primary endpoint, n (%) | |||||||
| Heart failure, at 36 months | 183 | (43.7) | 582 | (29.5) | 771 | (16.3) | 0.001 |
| Secondary endpoints, n (%) | |||||||
| Acute myocardial infarction, at 36 months | 53 | (12.6) | 185 | (9.4) | 309 | (6.6) | 0.001 |
| Coronary revascularization, at 36 months | 43 | (10.3) | 149 | (7.6) | 396 | (8.4) | 0.165 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinke, P.; Akin, I.; Kuhn, L.; Bertsch, T.; Weidner, K.; Abumayyaleh, M.; Dudda, J.; Rusnak, J.; Jannesari, M.; Siegel, F.; et al. The Prognostic Impact of Kidney Dysfunction in Unselected Patients Undergoing Coronary Angiography: In What Subgroups Does Kidney Dysfunction Matter? J. Clin. Med. 2025, 14, 3753. https://doi.org/10.3390/jcm14113753
Steinke P, Akin I, Kuhn L, Bertsch T, Weidner K, Abumayyaleh M, Dudda J, Rusnak J, Jannesari M, Siegel F, et al. The Prognostic Impact of Kidney Dysfunction in Unselected Patients Undergoing Coronary Angiography: In What Subgroups Does Kidney Dysfunction Matter? Journal of Clinical Medicine. 2025; 14(11):3753. https://doi.org/10.3390/jcm14113753
Chicago/Turabian StyleSteinke, Philipp, Ibrahim Akin, Lasse Kuhn, Thomas Bertsch, Kathrin Weidner, Mohammad Abumayyaleh, Jonas Dudda, Jonas Rusnak, Mahboubeh Jannesari, Fabian Siegel, and et al. 2025. "The Prognostic Impact of Kidney Dysfunction in Unselected Patients Undergoing Coronary Angiography: In What Subgroups Does Kidney Dysfunction Matter?" Journal of Clinical Medicine 14, no. 11: 3753. https://doi.org/10.3390/jcm14113753
APA StyleSteinke, P., Akin, I., Kuhn, L., Bertsch, T., Weidner, K., Abumayyaleh, M., Dudda, J., Rusnak, J., Jannesari, M., Siegel, F., Weiß, C., Duerschmied, D., Behnes, M., & Schupp, T. (2025). The Prognostic Impact of Kidney Dysfunction in Unselected Patients Undergoing Coronary Angiography: In What Subgroups Does Kidney Dysfunction Matter? Journal of Clinical Medicine, 14(11), 3753. https://doi.org/10.3390/jcm14113753