
Amniotic Membrane Coverage for Intractable Large Macular Holes: A First Report with Japanese Patients
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design
- Patients who have previously undergone PPV and ILM peeling for macular hole (MH) but have not achieved healing.
- The size of the macular hole must be >400 µm.
2.3. Surgical Procedure
- Initial Setup: The surgery begins with the insertion of 27-gauge instruments through the conjunctiva into the vitreous cavity, ensuring optimal access to the macular region.
- Confirmation of ILM: The presence or absence of the Internal Limiting Membrane (ILM) can be confirmed by applying Brilliant Blue G (BBG, Sigma-Aldrich, St. Louis, MO, USA) to the retina.
- Positioning the First Layer of Amniotic Membrane: A piece of amniotic membrane is gently placed over the center of the macular hole, supported by a dispersive viscoelastic material (Viscoat, Alcon). This crucial step promotes proper adherence and healing.
- Adding the Second Layer: A second layer of amniotic membrane is then meticulously positioned over the first layer, creating a double-layered coverage that enhances the efficacy of closure.
- Sealing and Tamponade: Following the placement of the membranes, viscoelastic material (Viscoat, Alcon) was applied on top of the amniotic membrane, and a slow air exchange was performed to ensure that the amniotic membranes settled correctly. The procedure concluded with a 20% SF6 gas tamponade to stabilize the repair.
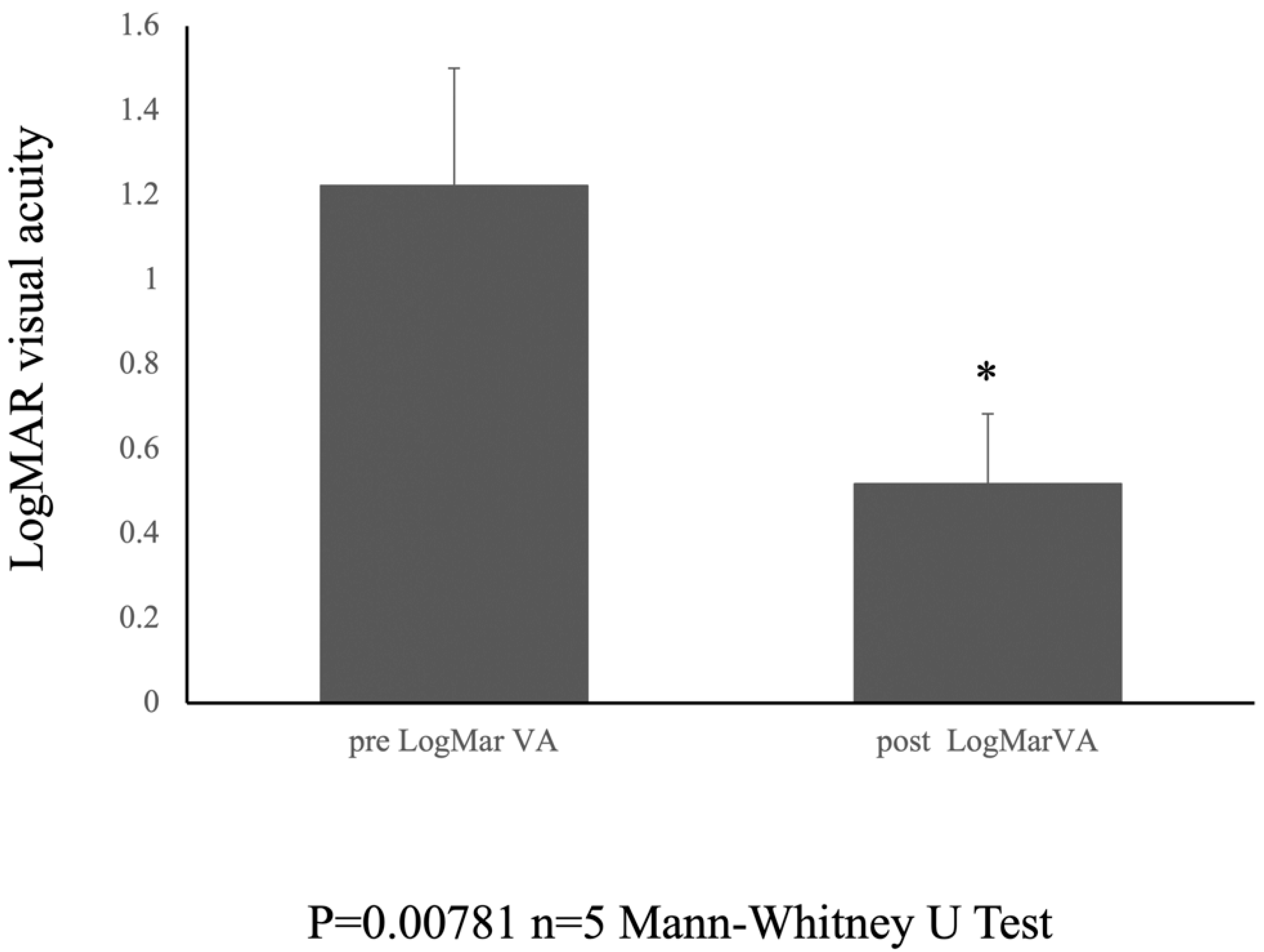
2.4. Statical Analysis
3. Results
4. Discussion
- -
- Anti-inflammatory properties: The amniotic membrane effectively reduces inflammation by inhibiting the production of pro-inflammatory cytokines such as IL-1 and IL-6. It also suppresses the release of chemoattractants, such as IL-8, which prevents the recruitment of inflammatory cells to the wound site. This anti-inflammatory effect minimizes the tissue damage caused by excessive inflammation, thus fostering a more conducive environment for healing [15].
- -
- Growth factor and cytokine delivery: The amniotic membrane is a rich source of various growth factors, such as epidermal growth factor (EGF), fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF), and cytokines. These factors stimulate cell proliferation, migration, and differentiation and promote tissue regeneration and angiogenesis. The presence of these bioactive molecules in the amniotic membrane expedites wound closure and tissue repair [16].
- -
- Extracellular matrix remodeling: The amniotic membrane contains essential components of the extracellular matrix (ECM), such as collagen, elastin, and hyaluronic acid. These components provide structural support to the wound site and facilitate the formation of a new ECM, contributing to tissue repair and restoration of the normal tissue architecture [17].
- -
- Immunomodulatory effects: Amniotic membranes have immunomodulatory properties that suppress immune responses and reduce the risk of rejection. This is achieved by inhibiting the activation of immune cells and promoting the production of anti-inflammatory cytokines. This makes it particularly useful for corneal transplantation, where rejection is a major concern [18].
- -
- Anti-angiogenic effects: The amniotic membrane can suppress angiogenesis, which involves the formation of new blood vessels. This effect is particularly beneficial for treating conditions involving abnormal angiogenesis, such as diabetic retinopathy and corneal neovascularization [19].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zong, Y.; Wu, K.; Yu, J.; Zhou, C.; Jiang, C. Internal Limiting Membrane Peeling and Flap Inverting under Air in Large Idiopathic Macular Hole Surgery. J. Ophthalmol. 2021, 2021, 2003001. [Google Scholar] [CrossRef] [PubMed]
- Ramtohul, P.; Parrat, E.; Denis, D.; Lorenzi, U. Inverted internal limiting membrane flap technique versus complete internal limiting membrane peeling in large macular hole surgery: A comparative study. BMC Ophthalmol. 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, Z.; Yu, Y.; Yang, X.; Qi, B.; Zhang, K.; Liu, W. Microstructural and microperimetric comparison of internal limiting membrane peeling and insertion in large idiopathic macular hole. BMC Ophthalmol. 2023, 23, 274. [Google Scholar] [CrossRef] [PubMed]
- Baumann, C.; Kaye, S.; Iannetta, D.; Sultan, Z.; Dwivedi, R.; Pearce, I. Effect of inverted internal limiting membrane flap on closure rate, postoperative visual acuity, and restoration of outer retinal layers in primary idiopathic macular hole surgery. Retina 2020, 40, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- McCannel, C.A.; Ensminger, J.L.; Diehl, N.N. HodgeDN Population-based incidence of macular holes. Ophthalmology 2009, 116, 1366–1369. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xu, L.; Jonas, J.B. Prevalence of full-thickness macular holes in urban and rural adult Chinese: The Beijing Eye Study. Am. J. Ophthalmol. 2006, 141, 589–591. [Google Scholar] [CrossRef]
- Ip, M.S.; Baker, B.J.; Duker, J.S.; Reichel, E.; Baumal, C.R.; Gangnon, R.; Puliafito, C.A. Anatomical outcomes of surgery for idiopathic macular hole as determined by optical coherence tomography. Arch. Ophthalmol. 2002, 120, 29–35. [Google Scholar] [CrossRef]
- Madi, H.A.; Masri, I. SteelDH Optimal management of idiopathic macular holes. Clin. Ophthalmol. 2016, 10, 97–116. [Google Scholar] [CrossRef] [PubMed]
- Galletero Pandelo, L.; Olaso Fernández, H.; Sánchez Aparicio, J.A.; Rodríguez Vidal, C.; Martínez-Alday, N. Results of large macular hole surgery using different interposition techniques. A report on 9 cases. Arch. Soc. Esp. Oftalmol. 2022, 97, 457–463. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Y.; Chen, G.; Han, F.; Jiang, W. Human amniotic membrane graft for refractory macular hole: A single-arm meta-analysis and systematic review. J. Fr. Ophtalmol. 2023, 46, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Caporossi, T.; Tartaro, R.; Bacherini, D.; Pacini, B.; De Angelis, L.; Governatori, L.; Di Leo, L.; Oliverio, L.; Rizzo, S. Applications of the Amniotic Membrane in Vitreoretinal Surgery. J. Clin. Med. 2020, 9, 2675. [Google Scholar] [CrossRef] [PubMed]
- Bamberger, M.D.; Felfeli, T.; Politis, M.; Mandelcorn, E.D.; Galic, I.J.; Chen, J.C. Human Amniotic Membrane Plug for Chronic or Persistent Macular Holes. Ophthalmol. Retina 2022, 6, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Cisiecki, S.; Bonińska, K.; Bednarski, M. Autologous Lens Capsule Flap Transplantation for Persistent Macular Holes. J. Ophthalmol. 2021, 2021, 8148792. [Google Scholar] [CrossRef] [PubMed]
- Yepez, J.B.; Murati, F.A.; De Yepez, J.; Petitto, M.; Arevalo, J.F. Anterior lens capsule in the management of chronic full-thickness macular hole. Retin. Cases Brief. Rep. 2018, 12, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.; Pereira, M.; Rana, H.; Stout, B.; Lewis, C.; Abramson, S.; Labazzo, K.; Ray, C.; Liu, Q.; Hofgartner, W.; et al. The Mechanism of Cell Interaction and Response on Decellularized Human Amniotic Membrane: Implications in Wound Healing. Wounds 2007, 19, 207–217. [Google Scholar] [PubMed]
- Grzywocz, Z.; Pius-Sadowska, E.; Klos, P.; Gryzik, M.; Wasilewska, D.; Aleksandrowicz, B.; Dworczynska, M.; Sabalinska, S.; Hoser, G.; Machalinski, B.; et al. Growth factors and their receptors derived from human amniotic cells in vitro. Folia Histochem. Cytobiol. 2014, 52, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Rastegar Adib, F.; Bagheri, F.; Sharifi, A.M. Osteochondral regeneration in rabbit using xenograft decellularized ECM in combination with different biological products; platelet-rich fibrin, amniotic membrane extract, and mesenchymal stromal cells. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 2089–2099. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.W.; Koo, H.C.; Hwang, S.Y.; Kang, S.K.; Ra, J.C.; Lee, M.H.; Park, Y.H. Immunomodulatory effects of human amniotic membrane-derived mesenchymal stem cells. J. Vet. Sci. 2012, 13, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Thomasen, H.; Pauklin, M.; Noelle, B.; Geerling, G.; Vetter, J.; Steven, P.; Steuhl, K.P.; Meller, D. The effect of long-term storage on the biological and histological properties of cryopreserved amniotic membrane. Curr. Eye Res. 2011, 36, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Garcin, T.; Gain, P.; Thuret, G. Femtosecond laser-cut autologous anterior lens capsule transplantation to treat refractory macular holes. Eye 2023, 37, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Karanfil, F.C.; Toklu, Y.; Yorgun, M.A. Amniotic Membrane Transplantation for Macular Hole Closure. Beyoglu Eye J. 2023, 8, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Felfeli, T.; Corrin, M.; Papanikolaou, J.; Mandelcorn, E.D. Macular hole hydrodissection technique with human amniotic membrane for repair of large macular holes. Retin. Cases Brief. Rep. 2023, 17, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Elkhenany, H.; El-Derby, A.; Abd Elkodous, M.; Salah, R.A.; Lotfy, A.; El-Badri, N. Applications of the amniotic membrane in tissue engineering and regeneration: The hundred-year challenge. Stem Cell Res. Ther. 2022, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Toda, A.; Okabe, M.; Yoshida, T.; Nikaido, T. The potential of amniotic membrane/amnion-derived cells for regeneration of various tissues. J. Pharmacol. Sci. 2007, 105, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cañada, C.; Bernabé-García, Á.; Liarte, S.; Insausti, C.L.; Angosto, D.; Moraleda, J.M.; Castellanos, G.; Nicolás, F.J. Amniotic membrane stimulates cell migration by modulating transforming growth factor-beta signalling. J. Tissue Eng. Regen. Med. 2018, 12, 808–820. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Ren, K.K.; Zhang, W.J.; Xiao, L.; Wu, H.Y.; Liu, Q.Y.; Ding, T.; Zhang, X.C.; Nie, W.J.; Ke, Y.; et al. Human amniotic mesenchymal stem cells and their paracrine factors promote wound healing by inhibiting heat stress-induced skin cell apoptosis and enhancing their proliferation through activating PI3K/AKT signaling pathway. Stem Cell Res. Ther. 2019, 10, 247. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Age | Pre LogMar VA | MH Diameter | Post LogMar VA |
|---|---|---|---|---|---|
| 1 | Female | 78 | 1.699 | 1330 | 0.699 |
| 2 | Female | 87 | 1.097 | 1038 | 0.398 |
| 3 | Male | 56 | 1.222 | 1174 | 0.398 |
| 4 | Male | 74 | 1.000 | 832 | 0.699 |
| 5 | Male | 58 | 1.097 | 987 | 0.398 |
| average | 70.6 | 1.222 | 1072.2 | 0.518 | |
| STDEV | 13.3 | 0.278 | 189.0 | 0.165 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayakawa, Y.; Inada, T. Amniotic Membrane Coverage for Intractable Large Macular Holes: A First Report with Japanese Patients. J. Clin. Med. 2025, 14, 3708. https://doi.org/10.3390/jcm14113708
Hayakawa Y, Inada T. Amniotic Membrane Coverage for Intractable Large Macular Holes: A First Report with Japanese Patients. Journal of Clinical Medicine. 2025; 14(11):3708. https://doi.org/10.3390/jcm14113708
Chicago/Turabian StyleHayakawa, Yasunari, and Takayuki Inada. 2025. "Amniotic Membrane Coverage for Intractable Large Macular Holes: A First Report with Japanese Patients" Journal of Clinical Medicine 14, no. 11: 3708. https://doi.org/10.3390/jcm14113708
APA StyleHayakawa, Y., & Inada, T. (2025). Amniotic Membrane Coverage for Intractable Large Macular Holes: A First Report with Japanese Patients. Journal of Clinical Medicine, 14(11), 3708. https://doi.org/10.3390/jcm14113708