
New Technique of Double-Layer Alveolar Ridge Preservation Using Collagen Matrix on Periodontally Collapsed Extraction Region: Proof-of-Concept Case Study


Abstract
1. Introduction
2. Materials and Methods
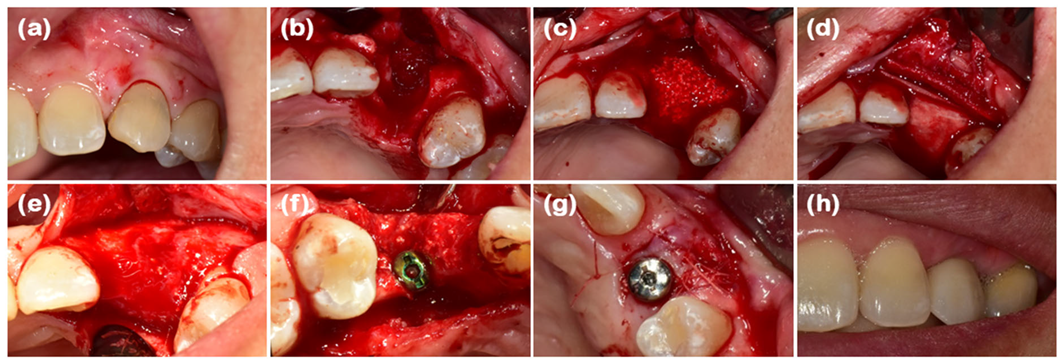
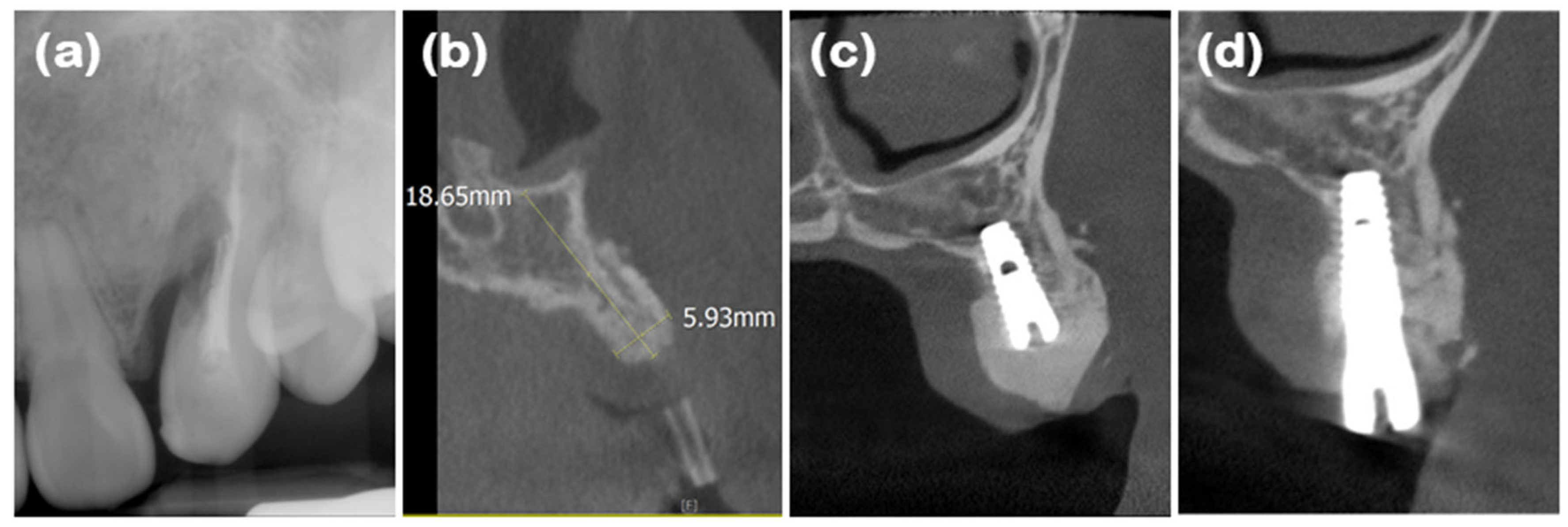
2.1. Case 1 (Single Tooth, Severe Buccal Bone Loss, and Cystic Lesion on the Extraction Region)
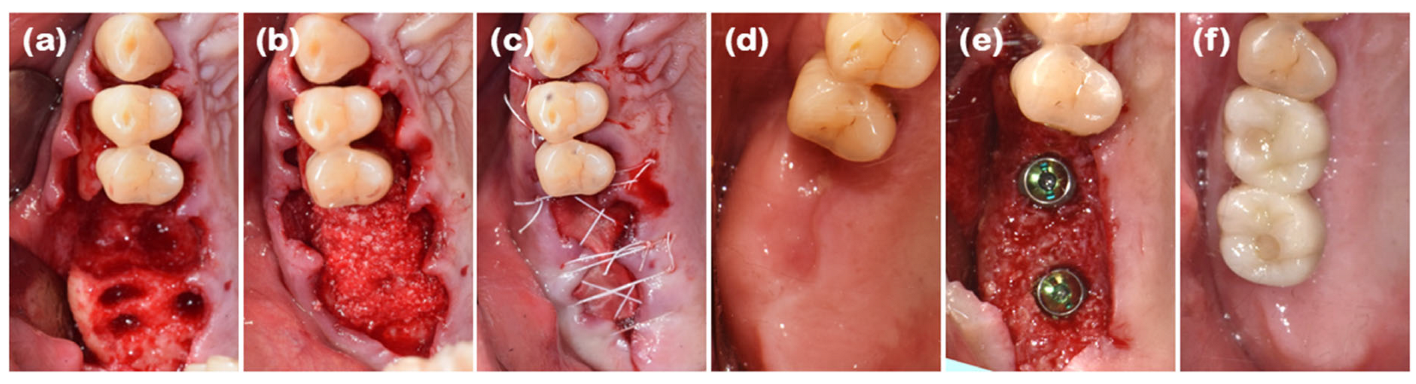
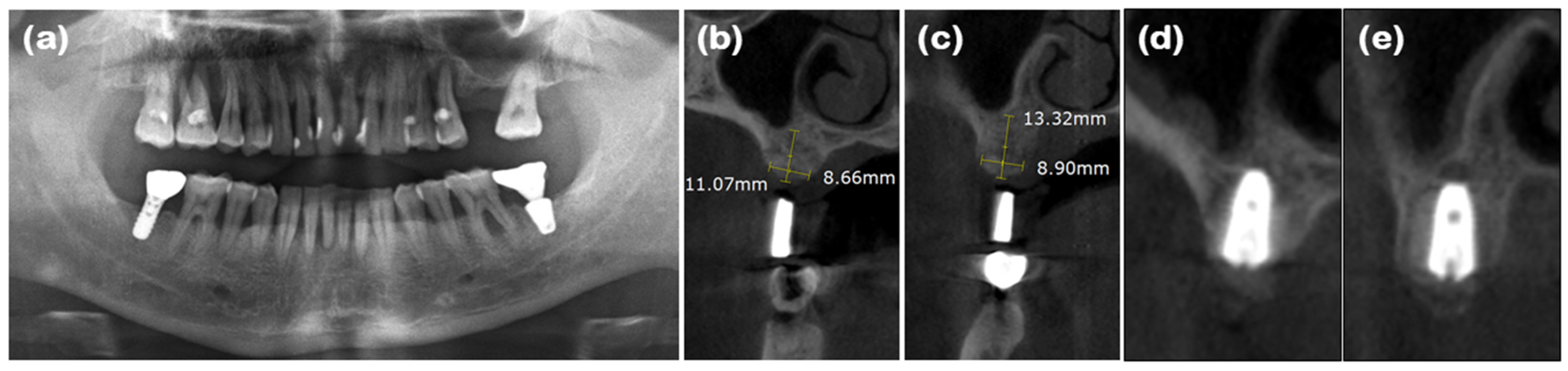
2.2. Case 2 (Multiple Posterior Teeth, Periodontitis, and Bucco-Palatal Collapsed Extraction Region)
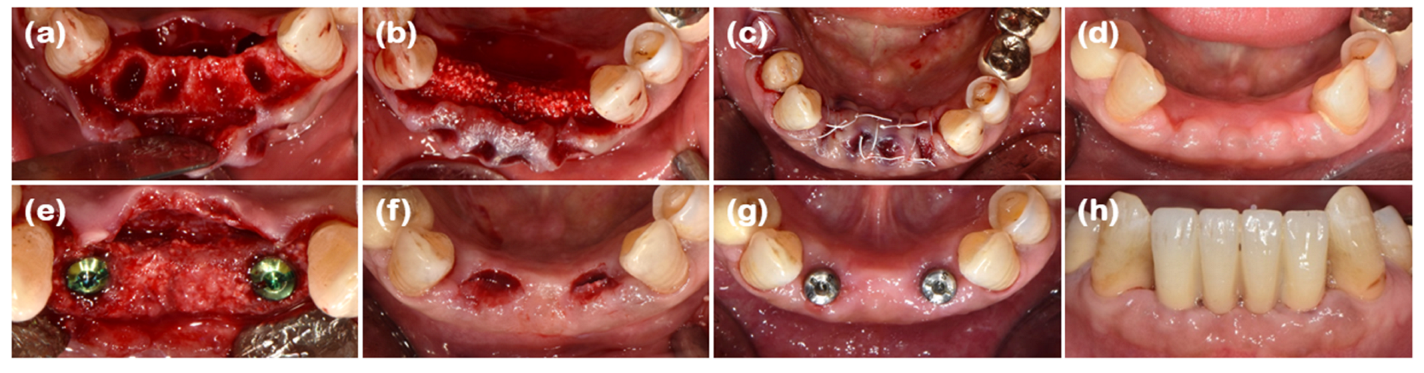
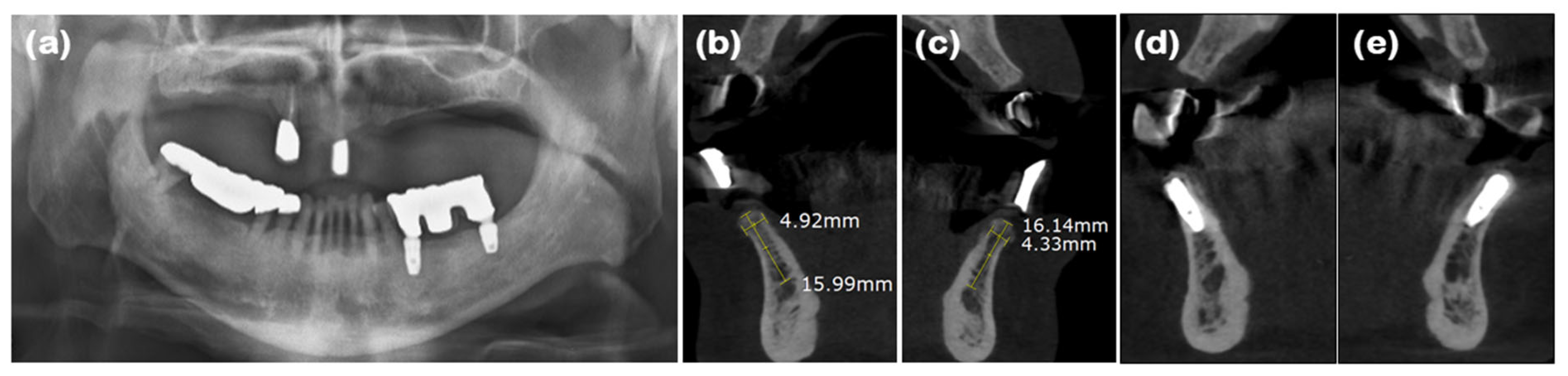
2.3. Case 3 (Multiple Anterior Teeth, Periodontitis, and Labio-Lingual Collapsed Extraction Region)
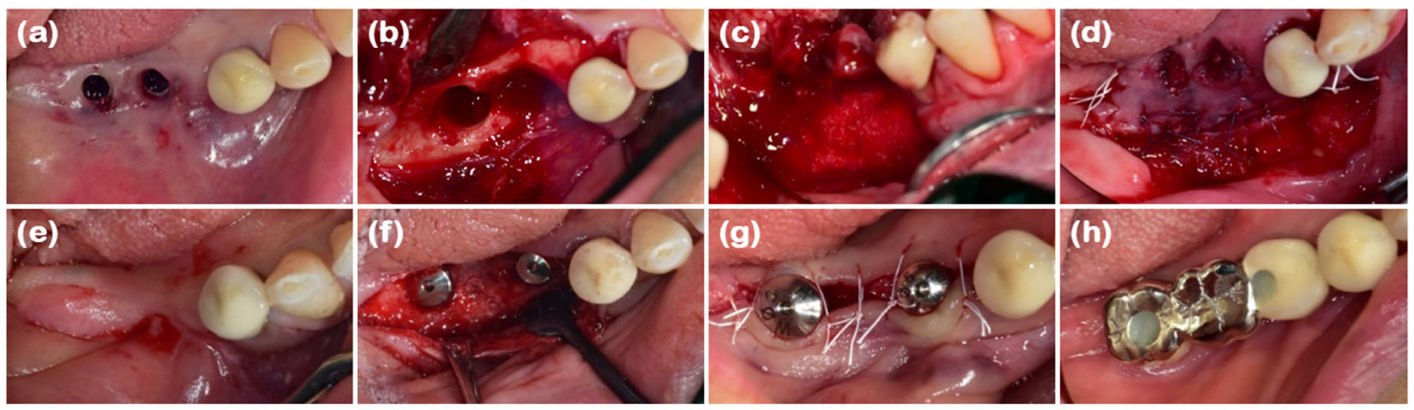
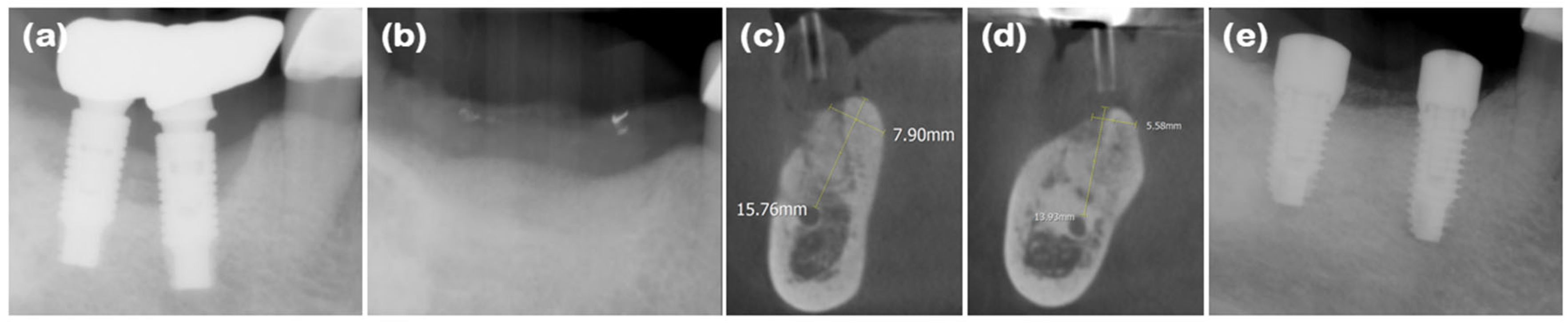
2.4. Case 4 (Multiple Posterior Implants, Peri-Implantitis, and Collapsed Ridge of Implant Removal Region)
2.5. Clinical and Radiographic Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mardas, N.; Trullenque-Eriksson, A.; MacBeth, N.; Petrie, A.; Donos, N. Does ridge preservation following tooth extraction improve implant treatment outcomes: A systematic review: Group 4: Therapeutic concepts & methods. Clin. Oral Implants Res. 2015, 26 (Suppl. S11), 180–201. [Google Scholar] [CrossRef] [PubMed]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Kim, J.H.; Susin, C.; Min, J.H.; Suh, H.Y.; Sang, E.J.; Ku, Y.; Wikesjö, U.M.; Koo, K.T. Extraction sockets: Erratic healing impeding factors. J. Clin. Periodontol. 2014, 41, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 195–223. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Cho, H.Y.; Lee, S.J.; Cho, I.W.; Shin, H.S.; Koo, K.T.; Lim, H.C.; Park, J.C. Alveolar ridge preservation with an open-healing approach using single-layer or double-layer coverage with collagen membranes. J. Periodontal Implant. Sci. 2017, 47, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alnaqbi, M.; Abdunabi, F.; Lin, L.; Alsabeeha, N.H.M. Alveolar ridge preservation in extraction sockets of periodontally compromised teeth: A systematic review and meta-analysis. Clin. Oral Implants Res. 2022, 33, 869–885. [Google Scholar] [CrossRef]
- Martin-Thome, H.; Bourdin, D.; Strube, N.; Saffarzadeh, A.; Morlock, J.F.; Campard, G.; Evanno, C.; Hoornaert, A.; Layrolle, P. Clinical Safety of a New Synthetic Resorbable Dental Membrane: A Case Series Study. J. Oral Implantol. 2018, 44, 138–145. [Google Scholar] [CrossRef]
- Mizraji, G.; Davidzohn, A.; Gursoy, M.; Gursoy, U.; Shapira, L.; Wilensky, A. Membrane barriers for guided bone regeneration: An overview of available biomaterials. Periodontol. 2000 2023, 93, 56–76. [Google Scholar] [CrossRef]
- Alauddin, M.S.; Abdul Hayei, N.A.; Sabarudin, M.A.; Mat Baharin, N.H. Barrier Membrane in Regenerative Therapy: A Narrative Review. Membranes 2022, 12, 444. [Google Scholar] [CrossRef]
- Abtahi, S.; Chen, X.; Shahabi, S.; Nasiri, N. Resorbable Membranes for Guided Bone Regeneration: Critical Features, Potentials, and Limitations. ACS Mater. Au 2023, 3, 394–417. [Google Scholar] [CrossRef]
- Tal, H.; Kozlovsky, A.; Artzi, Z.; Nemcovsky, C.E.; Moses, O. Cross-linked and non-cross-linked collagen barrier membranes disintegrate following surgical exposure to the oral environment: A histological study in the cat. Clin. Oral Implants Res. 2008, 19, 760–766. [Google Scholar] [CrossRef]
- Verardi, S.; Simion, M. Management of the exposure of e-PTFE membranes in guided bone regeneration. Pract. Proced. Aesthet. Dent. 2007, 19, 111–117. [Google Scholar]
- Han, H.-s.; Kim, S.; Cho, Y.-D. Alveolar Ridge Preservation in the Severely Damaged Sockets of the Anterior Maxilla Followed by Delayed Implant Placement. J. Implantol. Appl. Sci. 2023, 27, 96–102. [Google Scholar] [CrossRef]
- Ghanaati, S.; Schlee, M.; Webber, M.J.; Willershausen, I.; Barbeck, M.; Balic, E.; Görlach, C.; Stupp, S.I.; Sader, R.A.; Kirkpatrick, C.J. Evaluation of the tissue reaction to a new bilayered collagen matrix in vivo and its translation to the clinic. Biomed. Mater. 2011, 6, 015010. [Google Scholar] [CrossRef]
- Park, J.C.; Koo, K.T.; Lim, H.C. The hidden X suture: A technical note on a novel suture technique for alveolar ridge preservation. J. Periodontal Implant. Sci. 2016, 46, 415–425. [Google Scholar] [CrossRef]
- Decker, A.M.; Sheridan, R.; Lin, G.H.; Sutthiboonyapan, P.; Carroll, W.; Wang, H.L. A Prognosis System for Periimplant Diseases. Implant. Dent. 2015, 24, 416–421. [Google Scholar] [CrossRef]
- Decker, A.M.; Suarez-Lopez Del Amo, F.; Urban, I.A.; Miller, P.D., Jr.; Wang, H.L. Prognostic Classification System for Implant Recession Defects. Implant. Dent. 2017, 26, 848–852. [Google Scholar] [CrossRef]
- Belser, U.C.; Grutter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef]
- Kozlovsky, A.; Aboodi, G.; Moses, O.; Tal, H.; Artzi, Z.; Weinreb, M.; Nemcovsky, C.E. Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin. Oral Implants Res. 2009, 20, 1116–1123. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, D.Y.; Kim, K.H.; Ku, Y.; Rhyu, I.C.; Lee, Y.M. The efficacy of a double-layer collagen membrane technique for overlaying block grafts in a rabbit calvarium model. Clin. Oral Implants Res. 2009, 20, 1124–1132. [Google Scholar] [CrossRef]
- Garcia, J.; Dodge, A.; Luepke, P.; Wang, H.L.; Kapila, Y.; Lin, G.H. Effect of membrane exposure on guided bone regeneration: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Eskan, M.A.; Girouard, M.E.; Morton, D.; Greenwell, H. The effect of membrane exposure on lateral ridge augmentation: A case-controlled study. Int. J. Implant. Dent. 2017, 3, 26. [Google Scholar] [CrossRef]
- Sanz, M.; Lorenzo, R.; Aranda, J.J.; Martin, C.; Orsini, M. Clinical evaluation of a new collagen matrix (Mucograft prototype) to enhance the width of keratinized tissue in patients with fixed prosthetic restorations: A randomized prospective clinical trial. J. Clin. Periodontol. 2009, 36, 868–876. [Google Scholar] [CrossRef]
- MacBeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implants Res. 2017, 28, 982–1004. [Google Scholar] [CrossRef]
- Becker, W.; Becker, B.E. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences: Surgical techniques and case report. Int. J. Periodontics Restor. Dent. 1990, 10, 376–391. [Google Scholar]
- Rosenquist, B. A comparison of various methods of soft tissue management following the immediate placement of implants into extraction sockets. Int. J. Oral Maxillofac. Implants 1997, 12, 43–51. [Google Scholar]
- Schmitt, C.M.; Moest, T.; Lutz, R.; Wehrhan, F.; Neukam, F.W.; Schlegel, K.A. Long-term outcomes after vestibuloplasty with a porcine collagen matrix (Mucograft(®)) versus the free gingival graft: A comparative prospective clinical trial. Clin. Oral Implants Res. 2016, 27, e125–e133. [Google Scholar] [CrossRef]
- Basegmez, C.; Karabuda, Z.C.; Demirel, K.; Yalcin, S. The comparison of acellular dermal matrix allografts with free gingival grafts in the augmentation of peri-implant attached mucosa: A randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 145–152. [Google Scholar]
- Monje, A.; Blasi, G. Significance of keratinized mucosa/gingiva on peri-implant and adjacent periodontal conditions in erratic maintenance compliers. J. Periodontol. 2019, 90, 445–453. [Google Scholar] [CrossRef]
- Kungsadalpipob, K.; Supanimitkul, K.; Manopattanasoontorn, S.; Sophon, N.; Tangsathian, T.; Arunyanak, S.P. The lack of keratinized mucosa is associated with poor peri-implant tissue health: A cross-sectional study. Int. J. Implant. Dent. 2020, 6, 28. [Google Scholar] [CrossRef]
- Mahardawi, B.; Jiaranuchart, S.; Damrongsirirat, N.; Arunjaroensuk, S.; Mattheos, N.; Somboonsavatdee, A.; Pimkhaokham, A. The lack of keratinized mucosa as a risk factor for peri-implantitis: A systematic review and meta-analysis. Sci. Rep. 2023, 13, 3778. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pink Esthetic Score (PES) | White Esthetic Score (WES) | ||
| Mesial papilla | 2 | Tooth form | 1 |
| Distal papilla | 2 | Tooth volume/outline | 1 |
| Curvature of facial mucosa | 1 | Color (hue/value) | 2 |
| Level of facial mucosa | 1 | Surface texture | 2 |
| Soft tissue color and texture | 1 | Translucency | 1 |
| Total | 7 | 7 | |
| Pink Esthetic Score (PES) | White Esthetic Score (WES) | ||
| Mesial papilla | 1 | Tooth form | 1 |
| Distal papilla | 1 | Tooth volume/outline | 1 |
| Curvature of facial mucosa | 2 | Color (hue/value) | 2 |
| Level of facial mucosa | 2 | Surface texture | 2 |
| Soft tissue color and texture | 2 | Translucency | 2 |
| Total | 8 | 8 | |
| Case 1 | Case 2 | Case 3 | Case 4 | ||||
| Tooth position | #23 | #16 | #17 | #32 | #42 | #45 | #47 |
| Ridge width (mm) 1 | 5.93 | 8.66 | 8.90 | 4.92 | 4.33 | 7.90 | 5.58 |
| Keratinized mucosa width (mm) 2 | 4 | 6 | 6 | 4 | 4 | 3 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-J.; Lee, J.-B. New Technique of Double-Layer Alveolar Ridge Preservation Using Collagen Matrix on Periodontally Collapsed Extraction Region: Proof-of-Concept Case Study. J. Clin. Med. 2025, 14, 3617. https://doi.org/10.3390/jcm14113617
Kim Y-J, Lee J-B. New Technique of Double-Layer Alveolar Ridge Preservation Using Collagen Matrix on Periodontally Collapsed Extraction Region: Proof-of-Concept Case Study. Journal of Clinical Medicine. 2025; 14(11):3617. https://doi.org/10.3390/jcm14113617
Chicago/Turabian StyleKim, Yu-Jin, and Jong-Bin Lee. 2025. "New Technique of Double-Layer Alveolar Ridge Preservation Using Collagen Matrix on Periodontally Collapsed Extraction Region: Proof-of-Concept Case Study" Journal of Clinical Medicine 14, no. 11: 3617. https://doi.org/10.3390/jcm14113617
APA StyleKim, Y.-J., & Lee, J.-B. (2025). New Technique of Double-Layer Alveolar Ridge Preservation Using Collagen Matrix on Periodontally Collapsed Extraction Region: Proof-of-Concept Case Study. Journal of Clinical Medicine, 14(11), 3617. https://doi.org/10.3390/jcm14113617