
Psychosocial Impact of Maxilla-For-All® Treatment Using Standard and Long Implants (Pterygoid, Trans-Sinus and Zygomatic) on Patients with Severe Maxillary Atrophies: A 1-Year Prospective Study with PIDAQ-23 and OHIP-14

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.1.1. Inclusion Criteria
- Available radiographs before implant placement and 12 months after implant loading;
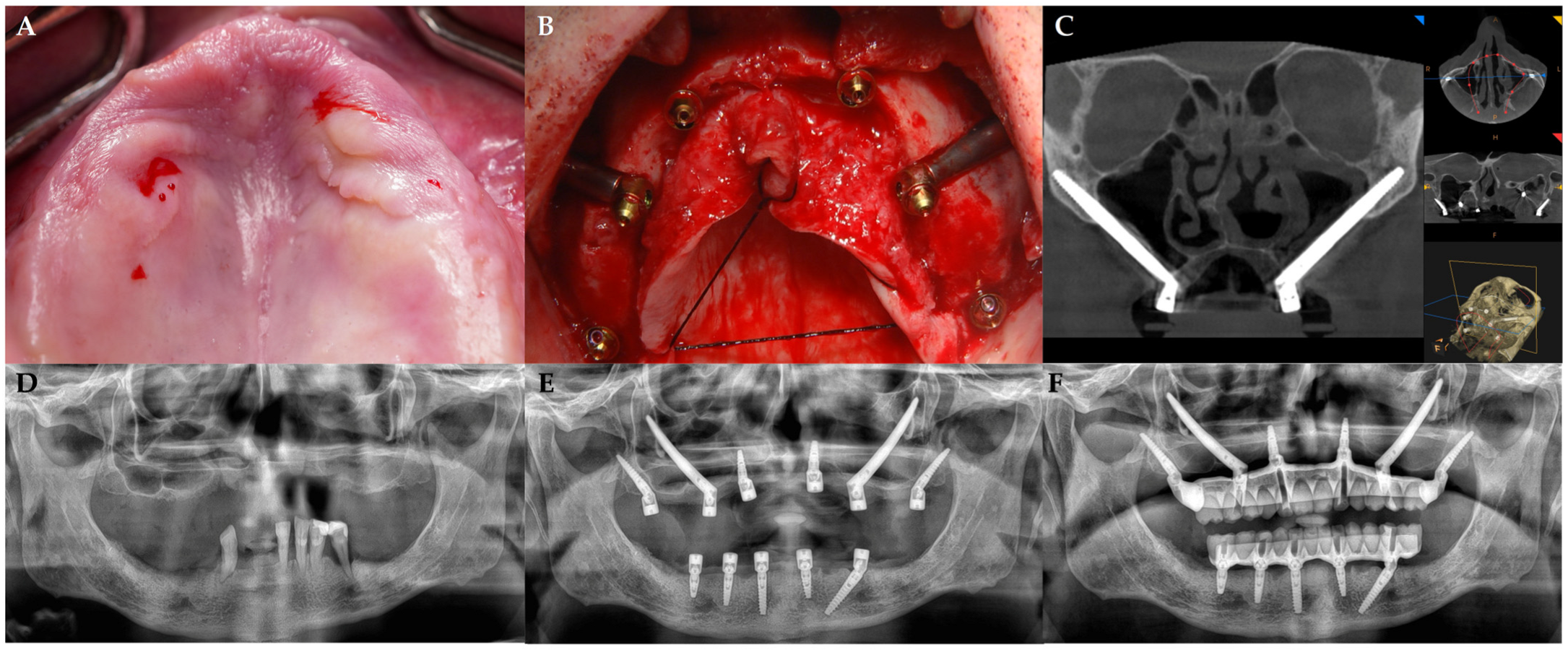
- Treatments with immediate functional loading of the implants and full-arch rehabilitation supported by standard, trans-sinus, pterygoid, and zygomatic implants;
- Age ≥ 18 years at surgery;
- Completed questionnaires.
2.1.2. Exclusion Criteria
- Undergoing any augmentation surgery;
- Medical records showing a history of systemic diseases that would have contraindicated oral surgery;
- Using bisphosphonate medications;
- Receiving bone resection or radiation therapy;
- Experiencing emotional instability;
- Abusing drugs or alcohol;
- Smoking heavily (more than 20 cigarettes a day).
2.2. Instrumentation/Surgery
2.3. Measurement
2.3.1. Predictors
2.3.2. Primary
- OHIP-14: A short version of the OHIP 49-item questionnaire suggested by Slade and co-workers is called the OHIP-14 [17]. Its seven domains are the following: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap. The Oral Health Impact Profile-14 comprises a total of 14 items rated on a scale of 0–4 (0 = “never”, 1 = “rarely”, 2 = “occasionally”, 3 = “often”, 4 = “very often”).
- The Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ), a psychometric tool developed by Klages, is used to evaluate aspects of quality of life specific to orthodontics [18]. The questionnaire assesses the influence of aesthetic perception of teeth in daily life and consists of 23 items grouped into four factors: dental self-confidence (DSC), social impact (SI), psychological impact (PI), and aesthetic concern (AC). The responses to aesthetic-negative statements were rated on a scale of 0–4 (0 = “not at all”, 1 = “a little”, 2 = “somewhat”, 3 = “strongly”, or 4 = “very strongly”). Since the subgroup “dental self-confidence” consisted of aesthetic-positive statements, the scale was reverse-coded for the first component. Thus, a total score of 0 would represent absolute satisfaction with aesthetics, and a maximum total score of 92 would represent absolute dissatisfaction.
2.3.3. Secondary
- Biological: Clinical examination of sinusitis symptoms and signs using the Lanza–Kennedy score assessed how surgery, implant placement, and potential sinus membrane perforation affected the ipsilateral upper respiratory tract (ear, nose, and throat) [19]. A criterion for soft tissue infection or inflammation was the appearance of clinical symptoms, infection, and dehiscence following implant implantation.
- Mechanical or Technical: Any fractures (generally including chipping of the veneering materials, components, frameworks, and structures) could be the cause of mechanical issues with an implant abutment or prosthesis. Prosthesis detachment, decementation, debonding, or loss of a retention screw were defined as technical issues [20].
2.4. Statistical Procedures
3. Results
3.1. OHIP
3.2. PIDAQ
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OHIP | Oral Health Impact Profile |
| PIDAQ | Psychosocial Impact of Dental Aesthetics Questionnaire |
| NSAID | Nonsteroidal anti-inflammatory drug |
| DSC | Dental self-confidence |
| SI | Social impact |
| PI | Psychological impact |
| AC | Aesthetic concern |
| ANOVA | ANalysis Of VAriance |
References
- Siadat, H.; Alikhasi, M.; Beyabanaki, E. Interim Prosthesis Options for Dental Implants. J. Prosthodont. 2017, 26, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lim, Y.J.; Kim, B.; Lee, J. How Do Parameters of Implant Primary Stability Correspond with CT-Evaluated Bone Quality in the Posterior Maxilla? A Correlation Analysis. Materials 2021, 14, 270. [Google Scholar] [CrossRef] [PubMed]
- Messias, A.; Nicolau, P.; Guerra, F. Different Interventions for Rehabilitation of the Edentulous Maxilla with Implant-Supported Prostheses: An Overview of Systematic Reviews. Int. J. Prosthodont. 2021, 34, s63–s84. [Google Scholar] [CrossRef]
- Rossi, F.; Tuci, L.; Ferraioli, L.; Ricci, E.; Suerica, A.; Botticelli, D.; Pellegrino, G.; Felice, P. Two-Year Follow-Up of 4-mm-Long Implants Used as Distal Support of Full-Arch FDPs Compared to 10-mm Implants Installed after Sinus Floor Elevation. A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3846. [Google Scholar] [CrossRef]
- Thoma, D.S.; Zeltner, M.; Hüsler, J.; Hämmerle, C.H.; Jung, R.E. EAO Supplement Working Group 4—EAO CC 2015 Short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral Implants Res. 2015, 26 (Suppl. S11), 154–169. [Google Scholar] [CrossRef]
- Niedermaier, R.; Stelzle, F.; Riemann, M.; Bolz, W.; Schuh, P.; Wachtel, H. Implant-Supported Immediately Loaded Fixed Full-Arch Dentures: Evaluation of Implant Survival Rates in a Case Cohort of up to 7 Years. Clin. Implant Dent. Relat. Res. 2017, 19, 4–19. [Google Scholar] [CrossRef]
- Riemann, M.; Wachtel, H.; Beuer, F.; Bolz, W.; Schuh, P.; Niedermaier, R.; Stelzle, F. Biologic and Technical Complications of Implant-Supported Immediately Loaded Fixed Full-Arch Prostheses: An Evaluation of Up to 6 Years. Int. J. Oral Maxillofac. Implants 2019, 34, 1482–1492. [Google Scholar] [CrossRef]
- Grandi, T.; Toti, P.; Covani, U.; Paoleschi, C.; Paoleschi, L.; Menchini-Fabris, G.B. Hybrid Full-Arch Rehabilitation Using Conventional and Zygomatic Implants: A Short-Term Retrospective Analysis. Eur. J. Prosthodont. Restor. Dent. 2025, 33, 11–23. [Google Scholar]
- Aalam, A.A.; Krivitsky-Aalam, A.; Kurtzman, G.M.; Mahesh, L. The severely atrophic maxilla: Decision making with zygomatic and pterygoid dental implants. J. Oral Biol. Craniofac. Res. 2023, 13, 202–206. [Google Scholar] [CrossRef]
- Şahin, O. Treatment of Severely Atrophic Maxilla by Using Zygomatic; Pterygoid; and Transnasal Implants. J. Craniofac. Surg. 2024, 35, e145–e146. [Google Scholar] [CrossRef]
- Wang, Y.; Bäumer, D.; Ozga, A.K.; Körner, G.; Bäumer, A. Patient satisfaction and oral health-related quality of life 10 years after implant placement. BMC Oral Health 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Candel-Marti, E.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Satisfaction and quality of life with palatal positioned implants in severely atrophic maxillae versus conventional implants supporting fixed full-arch prostheses. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e751–e756. [Google Scholar] [CrossRef] [PubMed]
- Topçu, A.O.; Yamalik, N.; Güncü, G.N.; Tözüm, T.F.; El, H.; Uysal, S.; Hersek, N. Implant-Site Related and Patient-Based Factors With the Potential to Impact Patients’ Satisfaction, Quality of Life Measures and Perceptions Toward Dental Implant Treatment. Implant Dent. 2017, 26, 581–591. [Google Scholar] [CrossRef] [PubMed]
- García-Minguillán, G.; Del Río, J.; Preciado, A.; Lynch, C.D.; Castillo-Oyagüe, R. Impact of the retention system of implant fixed dental restorations on the peri-implant health, state of the prosthesis, and patients’ oral health-related quality of life. J. Dent. 2020, 94, 103298. [Google Scholar] [CrossRef]
- Menchini-Fabris, G.B.; Toti, P.; Tommaso, G.; Paoleschi, C.; Paoleschi, L.; Covani, U. Immediate Full-Arch Restorations Supported by Conventional Implants Plus Uni- or Bilateral Zygomatic Implants: A Three to Five Years Retrospective Radiologic and Clinical Comparison. Int. J. Periodont. Restor. Dent. 2025; in press. [Google Scholar] [CrossRef]
- Graves, S.L. The pterygoid plate implant: A solution for restoring the posterior maxilla. Int. J. Periodont. Restor. Dent. 1994, 14, 512–523. [Google Scholar]
- Slade, G.D.; Spencer, J.A. Development and evaluation of the oral health impact profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar]
- Klages, U.; Claus, N.; Wehrbein, H.; Zentner, A. Development of a Questionnaire for Assessment of the Psychosocial Impact of Dental Aesthetics in Young Adults. Eur. J. Orthod. 2006, 28, 103–111. [Google Scholar] [CrossRef]
- Aparicio, C.; López-Piriz, R.; Albrektsson, T. ORIS Criteria of Success for the Zygoma-Related Rehabilitation: The (Revisited) Zygoma Success Code. Int. J. Oral Maxillofac. Implants 2020, 35, 366–378. [Google Scholar] [CrossRef]
- Anusavice, K.J. Standardizing failure; success; and survival decisions in clinical studies of ceramic and metal-ceramic fixed dental prostheses. Dent. Mater. 2012, 28, 102–111. [Google Scholar] [CrossRef]
- Davo, R.; Malevez, C.; Rojas, J. Immediate function in the atrophic maxilla using zygoma implants: A preliminary study. J. Prosthet. Dent. 2007, 97, s44–s51. [Google Scholar] [CrossRef]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Franch, M. Immediate/Early loading of zygomatic implants: Clinical experiences after 2 to 5 years of follow-up. Clin. Implant Dent. Relat. Res. 2010, 12, e77–e82. [Google Scholar] [CrossRef]
- Aparicio, C.; Manresa, C.; Francisco, K.; Aparicio, A.; Nunes, J.; Claros, P.; Potau, J.M. Zygomatic implants placed using the zygomatic anatomy-guided approach versus the classical technique. A proposed system to report rhinosinusitis diagnosis. Clin. Implant Dent. Relat. Res. 2014, 16, 627–642. [Google Scholar] [CrossRef]
- Becktor, J.P.; Isaksson, S.; Abrahamsson, P.; Sennerby, L. Evaluation of 31 zygomatic implants and 74 regular dental implants used in 16 patients for prosthetic reconstruction of the atrophic maxilla with cross-arch fixed bridges. Clin. Implant Dent. Relat. Res. 2005, 7, 159–165. [Google Scholar] [CrossRef]
- Aparicio, C. A proposed classification for zygomatic implant patient based on the zygoma anatomy guided approach (ZAGA): A cross-sectional survey. Eur. J. Oral Implantol. 2011, 4, 269–275. [Google Scholar]
- Papaspyridakos, P.; Bordin, T.B.; Natto, Z.S.; El-Rafie, K.; Pagni, S.E.; Chochlidakis, K.; Ercoli, C.; Weber, H.P. Complications and survival rates of 55 metal-ceramic implant-supported fixed complete-arch prostheses: A cohort study with mean 5-year follow-up. J. Prosthet. Dent. 2019, 122, 441–449. [Google Scholar] [CrossRef]
- Gonzalez-Gonzalez, I.; deLlanos-Lanchares, H.; Brizuela-Velasco, A.; Alvarez-Riesgo, J.A.; Llorente-Pendas, S.; Herrero-Climent, M.; Alvarez-Arenal, A. Complications of Fixed Full-Arch Implant-Supported Metal-Ceramic Prostheses. Int. J. Environ. Res. Public Health 2020, 17, 4250. [Google Scholar] [CrossRef]
- Sánchez-Siles, M.; Ballester-Ferrandis, J.F.; Salazar-Sánchez, N.; Gómez-García, F.J.; Moraleja-Ruiz, R.; Camacho-Alonso, F. Long-term evaluation of quality of life and satisfaction between implant bar overdentures and conventional complete dentures: A 23 years retrospective study. Clin. Implant. Dent. Relat. Res. 2018, 20, 208–214. [Google Scholar] [CrossRef]
- Fernández-Ruiz, J.A.; Sánchez-Siles, M.; Guerrero-Sánchez, Y.; Pato-Mourelo, J.; Camacho-Alonso, F. Evaluation of Quality of Life and Satisfaction in Patients with Fixed Prostheses on Zygomatic Implants Compared with the All-on-Four Concept: A Prospective Randomized Clinical Study. Int. J. Environ. Res. Public Health 2021, 18, 3426. [Google Scholar] [CrossRef]
- Sheats, R.D.; McGorray, S.P.; Keeling, S.D.; Wheeler, T.T.; King, G.J. Occlusal traits and perception of orthodontic need in eighth grade students. Angle Orthod. 1998, 68, 107–114. [Google Scholar]
- Carlsson, G.E.; Johansson, A.; Johansson, A.K.; Ordell, S.; Ekbäck, G.; Unell, L. Attitudes toward dental appearance in 50- and 60-year-old subjects living in Sweden. J. Esthet. Restor. Dent. 2008, 20, 46–55. [Google Scholar] [CrossRef]
- Xiao, J.; Zhou, X.; Zhu, W.D.; Zhang, B.; Li, J.Y.; Xu, X. The prevalence of tooth discolouration and the selfsatisfaction with tooth colour in a Chinese urban population. J. Oral Rehabil. 2007, 34, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Akarslan, Z.; Sadik, B.; Erten, H.; Karabulut, E. Dental esthetic satisfaction, received and desired dental treatments for improvement of esthetics. Indian J. Dent. Res 2009, 20, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Corbella, S.; Del Fabbro, M.; Taschieri, S.; De Siena, F.; Francetti, L. Clinical evaluation of an implant maintenance protocol for the prevention of peri-implant diseases in patients treated with immediately loaded full-arch rehabilitations. Int. J. Dent. Hyg. 2011, 9, 216–222. [Google Scholar] [CrossRef] [PubMed]
 : mechanical complications.
: mechanical complications.
: mechanical complications.
: mechanical complications.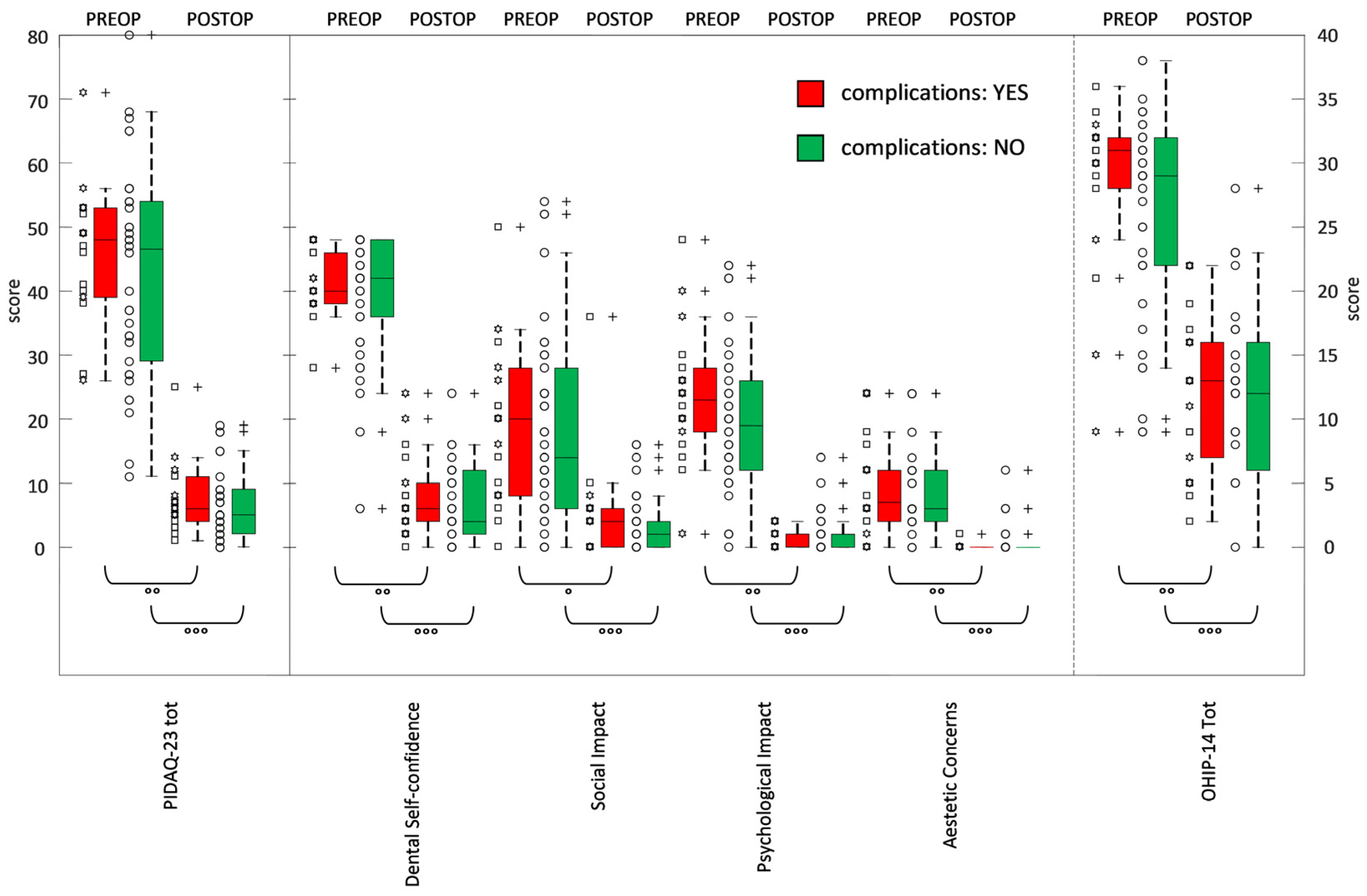

{kind=link}
{kind=link}
| Times | Preoperative | Postoperative (12 Months) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| factors | PIDAQ-23 items | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 |
| (reverse) Dental Self- confidence | 1. I am NOT proud of my teeth | 0 | 2 | 2 | 12 | 40 | 33 | 21 | 2 | 0 | 0 |
| 2. I DON’T like to show my teeth when I smile | 1 | 3 | 9 | 16 | 27 | 30 | 24 | 2 | 0 | 0 | |
| 3. I am NOT pleased when I see my teeth in the mirror | 2 | 2 | 5 | 17 | 30 | 37 | 17 | 2 | 0 | 0 | |
| 4. My teeth are NOT attractive to others | 0 | 1 | 1 | 21 | 33 | 17 | 27 | 9 | 3 | 0 | |
| 5. I am NOT satisfied with the appearance of my teeth | 3 | 2 | 4 | 13 | 34 | 25 | 25 | 5 | 0 | 1 | |
| 6. I find my tooth position to be NOT very nice | 1 | 3 | 7 | 13 | 32 | 32 | 20 | 4 | 0 | 0 | |
| percent (%) | 2.1 | 3.9 | 8.3 | 27.4 | 58.3 | 51.8 | 39.9 | 7.1 | 0.9 | 0.3 | |
| Social Impact | 7. I hold myself back when I smile so my teeth don’t show so much | 13 | 8 | 18 | 11 | 6 | 40 | 14 | 1 | 1 | 0 |
| 8. If I don’t know people well I am sometimes concerned what they might think about my teeth | 12 | 16 | 15 | 10 | 3 | 39 | 15 | 1 | 1 | 0 | |
| 9. I’m afraid other people could make offensive remarks about my teeth | 27 | 14 | 10 | 2 | 3 | 46 | 9 | 1 | 0 | 0 | |
| 10. I am somewhat inhibited in social contacts because of my teeth | 21 | 13 | 17 | 3 | 2 | 47 | 8 | 1 | 0 | 0 | |
| 11. I sometimes catch myself holding my hand in front of my mouth to hide my teeth | 20 | 16 | 10 | 7 | 3 | 39 | 16 | 0 | 1 | 0 | |
| 12. Sometimes I think people are staring at my teeth | 28 | 14 | 7 | 3 | 4 | 38 | 17 | 1 | 0 | 0 | |
| 13. Remarks about my teeth irritate me even when they are meant jokingly | 35 | 8 | 6 | 5 | 2 | 45 | 10 | 1 | 0 | 0 | |
| 14. I sometimes worry about what members of the opposite sex think about my teeth | 28 | 9 | 12 | 6 | 1 | 50 | 5 | 1 | 0 | 0 | |
| percent (%) | 41.1 | 21.9 | 21.2 | 10.5 | 5.4 | 76.8 | 21.0 | 1.5 | 0.7 | 0 | |
| Psychological Impact | 15. I envy the nice teeth of other people | 5 | 12 | 18 | 13 | 8 | 30 | 23 | 3 | 0 | 0 |
| 16. I am somewhat distressed when I see other people’s teeth | 26 | 17 | 6 | 5 | 2 | 49 | 7 | 0 | 0 | 0 | |
| 17. Sometimes I am somewhat unhappy about the appearance of my teeth | 12 | 14 | 21 | 4 | 5 | 53 | 3 | 0 | 0 | 0 | |
| 18. I think most people I know have nicer teeth than I do | 9 | 10 | 21 | 10 | 6 | 50 | 6 | 0 | 0 | 0 | |
| 19. I feel bad when I think about what my teeth look like | 19 | 10 | 18 | 2 | 7 | 53 | 3 | 0 | 0 | 0 | |
| 20. I wish my teeth looked better | 7 | 9 | 5 | 16 | 19 | 51 | 5 | 0 | 0 | 0 | |
| percent (%) | 23.2 | 21.4 | 26.5 | 14.9 | 14.0 | 85.1 | 14.0 | 0.9 | 0 | 0 | |
| Aesthetic Concerns | 21. I don’t like to see my teeth in the mirror | 10 | 22 | 12 | 4 | 8 | 54 | 2 | 0 | 0 | 0 |
| 22. I don’t like to see my teeth in photographs | 11 | 21 | 14 | 3 | 7 | 52 | 3 | 0 | 1 | 0 | |
| 23. I don’t like to see my teeth when I look at a video of myself | 13 | 18 | 14 | 4 | 7 | 51 | 4 | 0 | 1 | 0 | |
| percent (%) | 20.2 | 36.3 | 23.8 | 6.6 | 13.1 | 93.4 | 5.4 | 0 | 1.2 | 0 | |
| factors | OHIP-14 items | 0 | 1 | 2 | 3 | 4 | 0 | 1 | 2 | 3 | 4 |
| Functional limitation | 1. Have you had trouble pronouncing any words because of problems with your teeth, mouth or dentures? | 7 | 12 | 23 | 12 | 2 | 7 | 24 | 21 | 4 | 0 |
| 2. Have you felt that your sense of taste has worsened because of problems with your teeth, mouth or dentures? | 2 | 14 | 35 | 5 | 0 | 15 | 32 | 6 | 2 | 1 | |
| Physical pain | 3. Have you had painful aching in your mouth? | 0 | 7 | 13 | 35 | 1 | 9 | 13 | 27 | 7 | 0 |
| 4. Have you found it uncomfortable to eat any foods because of problems with your teeth, mouth or dentures? | 0 | 6 | 20 | 30 | 0 | 6 | 21 | 25 | 4 | 0 | |
| Psychological discomfort | 5. Have you been self-conscious because of your teeth, mouth or dentures? | 4 | 3 | 15 | 29 | 5 | 23 | 25 | 7 | 1 | 0 |
| 6. Have you felt tense because of problems with your teeth, mouth or dentures? | 6 | 4 | 37 | 8 | 1 | 23 | 27 | 6 | 0 | 0 | |
| Physical disability | 7. Has your diet been unsatisfactory because of problems with your teeth, mouth or dentures? | 1 | 14 | 16 | 25 | 0 | 8 | 20 | 27 | 1 | 0 |
| 8. Have you had to interrupt meals because of problems with your teeth mouth or dentures? | 4 | 18 | 28 | 5 | 1 | 20 | 27 | 8 | 1 | 0 | |
| Psychological disability | 9. Have you found it difficult to relax because of problems with your teeth, mouth or dentures? | 5 | 12 | 33 | 6 | 0 | 21 | 31 | 4 | 0 | 0 |
| 10. Have you been a bit embarrassed because of problems with your teeth, mouth or dentures? | 4 | 4 | 17 | 24 | 7 | 25 | 26 | 5 | 0 | 0 | |
| Social disability | 11. Have you been a bit irritable with other people because of problems with your teeth mouth or dentures? | 6 | 13 | 27 | 9 | 1 | 29 | 24 | 3 | 0 | 0 |
| 12. Have you had difficulty doing your usual jobs because of problems with your teeth mouth and dentures? | 8 | 31 | 10 | 7 | 0 | 42 | 11 | 3 | 0 | 0 | |
| Handicap | 13. Have you felt that life in general was less satisfying because of problems with your teeth mouth and dentures? | 7 | 13 | 15 | 20 | 1 | 39 | 13 | 4 | 0 | 0 |
| 14. Have you been totally unable to function because of problems with your teeth, mouth or dentures? | 23 | 15 | 12 | 4 | 2 | 37 | 15 | 4 | 0 | 0 | |
| percent (%) | 9.8 | 21.2 | 38.4 | 27.9 | 2.7 | 38.8 | 39.4 | 19.1 | 2.6 | 0.1 | |
| Time | Preoperative | Postoperative (12 Months) | Wilcoxon Test | ||
|---|---|---|---|---|---|
| PIDAQ-23 | mean ± std | [min max] | mean ± std | [min max] | signed-rank p-value |
| Dental Self-Confidence | 20.2 ± 4.3 | [3–24] | 3.5 ± 3.0 | [0–12] | <0.0001 |
| Social Impact | 9.4 ± 7.2 | [0–27] | 2.1 ± 3.0 | [0–18] | <0.0001 |
| Psychological Impact | 10.5 ± 5.7 | [0–24] | 1.0 ± 1.3 | [0–7] | <0.0001 |
| Aesthetic Concerns | 4.7 ± 3.6 | [0–12] | 0.3 ± 1.0 | [0–6] | <0.0001 |
| PIDAQ tot | 44.7 ± 16.6 | [11–84] | 6.8 ± 5.3 | [0–25] | <0.0001 |
| OHIP-14 | mean ± std | [min max] | mean ± std | [min max] | signed-rank test |
| Functional limitation | 3.6 ± 1.4 | [1–7] | 2.4 ± 1.3 | [0–6] | <0.0001 |
| Physical pain | 5.0 ± 1.3 | [2–7] | 3.1 ± 1.5 | [0–5] | <0.0001 |
| Psychological discomfort | 4.4 ± 1.7 | [0–8] | 1.5 ± 1.3 | [0–5] | <0.0001 |
| Physical disability | 3.8 ± 1.5 | [0–7] | 2.2 ± 1.3 | [0–5] | <0.0001 |
| Psychological disability | 4.2 ± 1.6 | [0–7] | 1.3 ± 1.2 | [0–4] | <0.0001 |
| Social disability | 3.0 ± 1.6 | [0–6] | 0.8 ± 1.1 | [0–4] | <0.0001 |
| Handicap | 3.0 ± 1.7 | [0–7] | 0.8 ± 1.2 | [0–4] | <0.0001 |
| OHIP Tot | 27.0 ± 7.6 | [9–38] | 12.0 ± 6.4 | [0–28] | <0.0001 |
| Time | Groups | Preoperative | Postoperative (12 Months) | |||||
|---|---|---|---|---|---|---|---|---|
| PIDAQ-23 | complications | mean ± std | [min max] | variance | mean ± std | [min max] | variance | p-value |
| Dental Self-confidence | YES | 20.6 ± 2.7 | [14–24] | 7.19 | 4.1 ± 3.3 | [0–12] | 10.87 | 0.0002 ° |
| NO | 19.9 ± 5.0 | [3–24] | 24.59 | 3.2 ± 2.9 | [0–12] | 8.27 | <0.0001 ° | |
| p-value | YES vs. NO | 0.9089 # | 0.5554 # | |||||
| Social Impact | YES | 9.8 ± 6.5 | [0–25] | 41.67 | 2.7 ± 4.1 | [0–18] | 16.91 | 0.0013 ° |
| NO | 9.2 ± 7.6 | [0–27] | 58.02 | 1.8 ± 2.3 | [0–8] | 5.19 | <0.0001 ° | |
| p-value | YES vs. NO | 0.4988 # | 0.9628 # | |||||
| Psychological Impact | YES | 11.8 ± 5.3 | [1–24] | 28.14 | 0.7 ± 0.6 | [0–2] | 0.70 | 0.0002 ° |
| NO | 9.9 ± 5.8 | [0–22] | 33.73 | 1.1 ± 1.5 | [0–7] | 2.23 | <0.0001 ° | |
| p-value | YES vs. NO | 0.9281 # | 0.9801 # | |||||
| Aesthetic Concerns | YES | 4.7 ± 3.7 | [0–12] | 13.35 | 0.1 ± 0.2 | [0–1] | 0.05 | 0.0004 ° |
| NO | 4.6 ± 3.7 | [0–12] | 13.42 | 0.4 ± 1.2 | [0–6] | 1.37 | <0.0001 ° | |
| p-value | YES vs. NO | 1 # | 0.7588 # | |||||
| PIDAQ tot | YES | 44.1 ± 14.6 | [26–84] | 212.17 | 7.5 ± 5.7 | [1–25] | 31.91 | 0.0002 ° |
| NO | 43.6 ± 17.6 | [11–84] | 308.40 | 6.5 ± 5.1 | [0–19] | 26.41 | <0.0001 ° | |
| p-value | YES vs. NO | 0.7013 # | 0.5270 # | |||||
| OHIP-14 | complications | mean ± std | [min max] | Variance | mean ± std | [min max] | variance | signed-rank test |
| Functional limitation | YES | 4.0 ± 1.3 | [2–7] | 1.64 | 2.7 ± 1.4 | [1–6] | 1.88 | 0.0054 ° |
| NO | 3.4 ± 1.4 | [1–6] | 1.86 | 2.2 ± 1.2 | [0–4] | 1.52 | 0.0004 ° | |
| p-value | YES vs. NO | 0.8521 # | 0.8894 # | |||||
| Physical pain | YES | 5.2 ± 1.2 | [2–6] | 1.35 | 3.1 ± 1.6 | [0–5] | 2.64 | 0.0023 ° |
| NO | 4.8 ± 1.4 | [2–7] | 1.97 | 3.1 ± 1.4 | [0–5] | 2.05 | <0.0001 ° | |
| p-value | YES vs. NO | 0.2258 # | 0.8011 # | |||||
| Psychological discomfort | YES | 4.2 ± 1.9 | [0–7] | 3.47 | 1.3 ± 1.3 | [0–5] | 1.76 | 0.0006 ° |
| NO | 4.5 ± 1.6 | [0–8] | 2.68 | 1.5 ± 1.3 | [0–4] | 1.55 | <0.0001 ° | |
| p-value | YES vs. NO | 0.5221 # | 0.8147 # | |||||
| Physical disability | YES | 3.9 ± 1.8 | [0–7] | 3.11 | 2.0 ± 1.4 | [0–4] | 2.00 | 0.0080 ° |
| NO | 3.8 ± 1.4 | [1–6] | 1.86 | 2.3 ± 1.2 | [0–5] | 1.40 | 0.0004 ° | |
| p-value | YES vs. NO | 0.5785 # | 0.4190 # | |||||
| Psychological disability | YES | 4.4 ± 1.7 | [0–6] | 2.95 | 1.2 ± 0.9 | [0–4] | 0.85 | 0.0005 ° |
| NO | 4.1 ± 1.6 | [0–7] | 2.39 | 1.4 ± 1.2 | [0–4] | 1.54 | <0.0001 ° | |
| p-value | YES vs. NO | 0.5582 # | 1 # | |||||
| Social disability | YES | 3.3 ± 1.8 | [0–6] | 3.27 | 1.0 ± 1.2 | [0–4] | 1.52 | 0.0042 ° |
| NO | 2.9 ± 1.4 | [0–6] | 2.07 | 0.8 ± 1.0 | [0–4] | 0.94 | <0.0001 ° | |
| p-value | YES vs. NO | 0.9813 # | 0.8271 # | |||||
| Handicap | YES | 3.2 ± 1.8 | [0–7] | 3.12 | 0.9 ± 1.2 | [0–4] | 1.46 | 0.0032 ° |
| NO | 2.8 ± 1.7 | [0–7] | 2.78 | 0.7 ± 1.1 | [0–4] | 1.29 | <0.0001 ° | |
| p-value | YES vs. NO | 0.8515 # | 0.7641 # | |||||
| OHIP Tot | YES | 28.2 ± 6.9 | [9–36] | 47.74 | 12.2 ± 6.1 | [2–22] | 37.08 | 0.0005 ° |
| NO | 26.3 ± 7.9 | [9–38] | 63.08 | 12.0 ± 6.6 | [0–28] | 43.78 | <0.0001 ° | |
| p-value | YES vs. NO | 0.7328 # | 0.8920 # | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grandi, T.; Toti, P.; Paoleschi, C.; Giorgi, M.; Covani, U.; Menchini-Fabris, G.B. Psychosocial Impact of Maxilla-For-All® Treatment Using Standard and Long Implants (Pterygoid, Trans-Sinus and Zygomatic) on Patients with Severe Maxillary Atrophies: A 1-Year Prospective Study with PIDAQ-23 and OHIP-14. J. Clin. Med. 2025, 14, 3544. https://doi.org/10.3390/jcm14103544
Grandi T, Toti P, Paoleschi C, Giorgi M, Covani U, Menchini-Fabris GB. Psychosocial Impact of Maxilla-For-All® Treatment Using Standard and Long Implants (Pterygoid, Trans-Sinus and Zygomatic) on Patients with Severe Maxillary Atrophies: A 1-Year Prospective Study with PIDAQ-23 and OHIP-14. Journal of Clinical Medicine. 2025; 14(10):3544. https://doi.org/10.3390/jcm14103544
Chicago/Turabian StyleGrandi, Tommaso, Paolo Toti, Cesare Paoleschi, Matteo Giorgi, Ugo Covani, and Giovanni Battista Menchini-Fabris. 2025. "Psychosocial Impact of Maxilla-For-All® Treatment Using Standard and Long Implants (Pterygoid, Trans-Sinus and Zygomatic) on Patients with Severe Maxillary Atrophies: A 1-Year Prospective Study with PIDAQ-23 and OHIP-14" Journal of Clinical Medicine 14, no. 10: 3544. https://doi.org/10.3390/jcm14103544
APA StyleGrandi, T., Toti, P., Paoleschi, C., Giorgi, M., Covani, U., & Menchini-Fabris, G. B. (2025). Psychosocial Impact of Maxilla-For-All® Treatment Using Standard and Long Implants (Pterygoid, Trans-Sinus and Zygomatic) on Patients with Severe Maxillary Atrophies: A 1-Year Prospective Study with PIDAQ-23 and OHIP-14. Journal of Clinical Medicine, 14(10), 3544. https://doi.org/10.3390/jcm14103544