
Compliance with the European Pregnancy Prevention Programme in Isotretinoin Treatment: Safety Outcomes and Dose-Related Correlations

 ,
,  , and
, and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Classification by European Pregnancy Prevention Programme Adherence
2.3. Treatment, Monitoring, and Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Group
3.2. Statistical Analysis of Treatment by Study Group
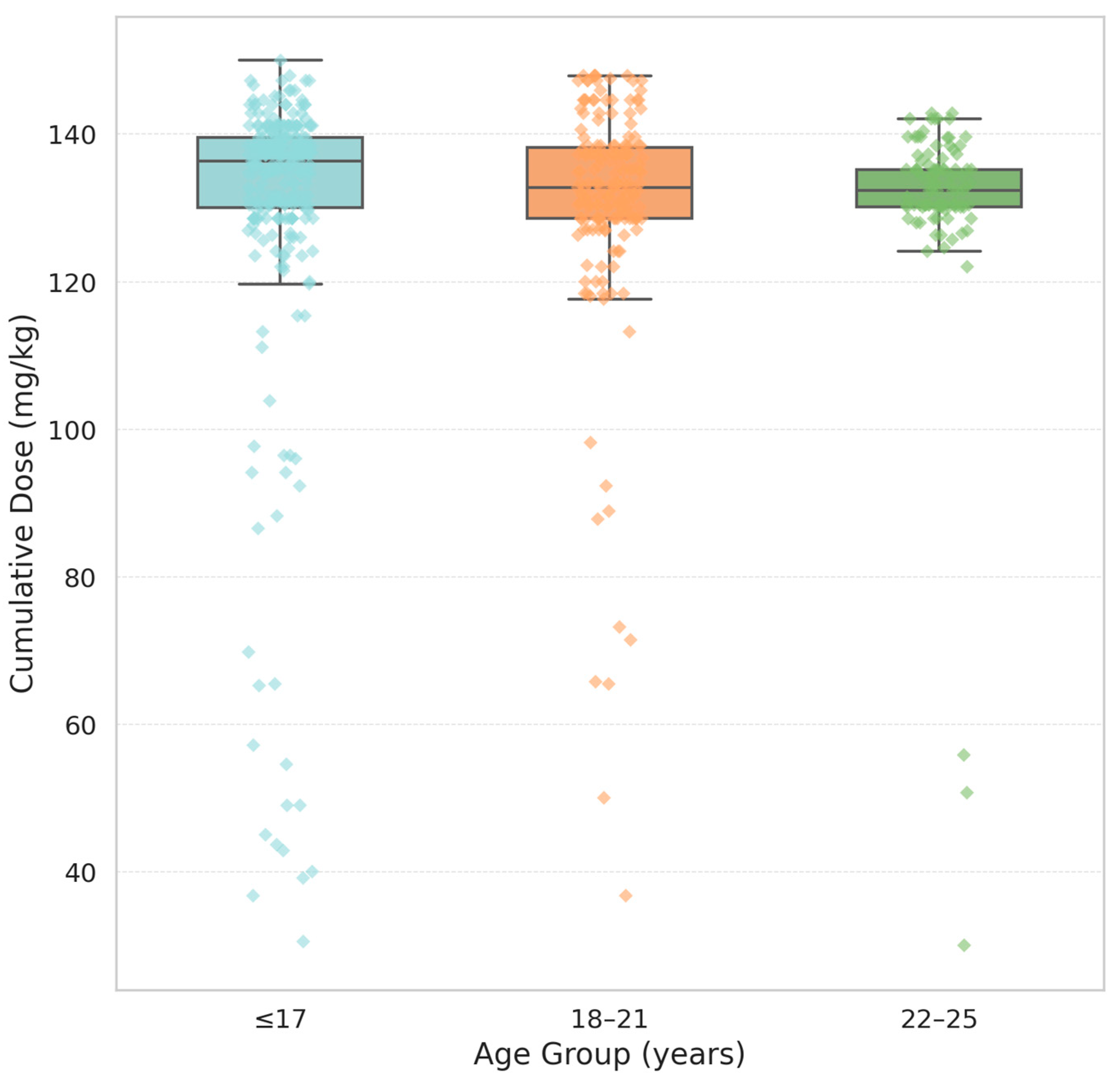
3.3. Age-Related Differences in Treatment Outcomes
4. Discussion
4.1. Overview of Risk Mitigation Systems: iPLEDGE and PPP
4.2. Interpreting Partial PPP Compliance
4.3. Contraceptive Strategies
4.4. Patient Age and Cumulative Dose: Statistical Correlation
4.5. Treatment Discontinuation
4.6. Biochemical Monitoring and Laboratory Findings
4.7. Patient Reporting and Behavioural Discrepancies
4.8. Limitations of Zero-Event Data Interpretation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reynolds, R.V.; Yeung, H.; Cheng, C.E.; Cook-Bolden, F.; Desai, S.R.; Druby, K.M.; Freeman, E.E.; Keri, J.E.; Stein Gold, L.F.; Tan, J.K.L.; et al. Guidelines of care for the management of acne vulgaris. J. Am. Acad. Dermatol. 2024, 90, 1006.e1–1006.e30. [Google Scholar] [CrossRef]
- Nofal, A.A.; Hussein, G.H.; Ahmed, N.; Ibrahim, A.M. Inflammatory biomarkers and clinical adverse effects associated with Isotretinoin treatment: A prospective study. Egypt. J. Dermatol. Venerol. 2024, 44, 209–214. [Google Scholar] [CrossRef]
- Bagatin, E.; Costa, C.S. The Use of Isotretinoin for Acne—An Update on Optimal dosing, surveillance, and Adverse Effects. Expert Rev. Clin. Pharmacol. 2020, 13, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Sanjel, K.; Zhang, X.M. Progress of different treatment modalities to limit the use of antibiotics in the treatment of acne. Our Dermatol. Online 2022, 13, 92–97. [Google Scholar] [CrossRef]
- Soundarya, B.S.; Jayakar, T. Acne mimickers: Differential diagnosis of open comedones: A short review. Our Dermatol. Online 2023, 14, 230–235. [Google Scholar] [CrossRef]
- Incel Uysal, P. Rapid-onset oral isotretinoin-induced acne fulminans without systemic symptoms in a male adolescent. Our Dermatol. Online 2021, 12, 417–418. [Google Scholar] [CrossRef]
- Yao, Q.H.; Liu, Z.H. Rosacea Fulminans in Pregnancy: A Case Report and Review. Clin. Cosmet. Investig. Dermatol. 2024, 17, 1999–2007. [Google Scholar] [CrossRef]
- Melnik, B.C. Acne Transcriptomics: Fundamentals of Acne Pathogenesis and Isotretinoin Treatment. Cells 2023, 12, 2600. [Google Scholar] [CrossRef]
- Tan, T.H.; Hallett, R.; Yesudian, P.D. Efficacy and relapse rates of different Isotretinoin dosages in treating acne vulgaris: Systemic review. Clin. Med. 2016, 16 (Suppl. S3), s34. [Google Scholar] [CrossRef]
- Ünlü Açıkel, S.; Sadettin Burak, A. Bibliometric analysis of studies investigating the association between isotretinoin use and depression and suicide. Clin. Exp. Dermatol. 2025, 50, 779–787. [Google Scholar] [CrossRef]
- Kawczak, P.; Feszak, I.; Brzeziński, P.; Bączek, T. Structure-Activity Relationships and Therapeutic Applications of Retinoids in View of Potential Benefits from Drug Repurposing Process. Biomedicines 2024, 12, 1059. [Google Scholar] [CrossRef] [PubMed]
- Mahsoub, N.I.I.; Elsohafy, M.A.; Hasan, A.M.; Ismael, A.F. Most Common Isotretinoin Therapy Side Effects on Egyptian Acne Females in Dakahlia Governorate. Egypt. J. Hosp. Med. 2024, 96, 2860–2870. [Google Scholar]
- Topal, I.O.; Otunctemur, A. An investigation of the effects of acitretin on erectile function. Our Dermatol. Online 2020, 11 (Suppl. S3), 1–5. [Google Scholar] [CrossRef]
- Kouotou, E.A.; Nguena Feungue, U.; Tounouga, D.N.; Ngoune Madjoukeng, A.S.; Nkoro, G.A.; Sigha, B.O.; Ekambi, R.K.; Zoung-Kanyi Bissek, A.C. Severity of acne and quality of life of patients treated at Cameroonian hospitals (sub-Saharan Africa). Our Dermatol. Online 2023, 14, 16–22. [Google Scholar] [CrossRef]
- Alghamdi, W.A.F.; Alwesaibie, H.S.; Albesher, M.A.; Alghamdi, F.K.; Albaqshi, A.A. Knowledge, Attitude, and Practice Regarding the Use of Isotretinoin in Saudi Arabia. Cureus 2023, 15, e50516. [Google Scholar] [CrossRef]
- Rademaker, M. Isotretinoin: Dose, duration and relapse. What does 30 years of usage tell us? Australas. J. Dermatol. 2013, 54, 157–162. [Google Scholar] [CrossRef]
- Almarri, F.H.; Al Dhafiri, M.; Albejais, R.A.; Albaqshi, M.A.; Alotaibi, W.D. The Perception of Contraceptive Practice Among Female Patients Treated with Isotretinoin in Saudi Arabia. Cureus 2024, 16, e69390. [Google Scholar] [CrossRef]
- Al-Sheyab, R.F.; Alshiyab, D.; Al-Shagarin, R.A.; Murshidi, R.; ALSalamat, H.A.; Abu-Rayyan, H.; Abu-Arja, Y.; Ghunaim, S.; Altamimi, S. Prescribing Patterns of Isotretinoin for Acne Among Dermatologists in Central Jordan. Cureus 2024, 16, e58840. [Google Scholar] [CrossRef]
- Tkachenko, E.; Singer, S.; Sharma, P.; Barbieri, J.; Mostaghimi, A. US Food and Drug Administration Reports of Pregnancy and Pregnancy-Related Adverse Events Associated with Isotretinoin. JAMA Dermatol. 2019, 155, 1175–1179. [Google Scholar] [CrossRef]
- Shin, J.; Cheetham, T.C.; Wong, L.; Niu, F.; Kass, E.; Yoshinaga, M.A.; Sorel, M.; McCombs, J.S.; Sidney, S. The impact of the iPLEDGE program on isotretinoin fetal exposure in an integrated health care system. J. Am. Acad. Dermatol. 2011, 65, 1117–1125. [Google Scholar] [CrossRef]
- Barbieri, J.S.; Roe, A.H.; Mostaghimi, A. Simplifying contraception requirements for iPLEDGE: A decision analysis. J. Am. Acad. Dermatol. 2020, 83, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Durán, C.E.; Riera-Arnau, J.; Abtahi, S.; Pajouheshnia, R.; Hoxhaj, V.; Gamba, M.; Alsina, E.; Martin-Perez, M.; Garcia-Poza, P.; Llorente-Garcia, A.; et al. Impact of the 2018 revised Pregnancy Prevention Programme by the European Medicines Agency on the use of oral retinoids in females of childbearing age. Front. Pharmacol. 2023, 14, 1207976. [Google Scholar] [CrossRef]
- Ivask, M.; Kurvits, K.; Uusküla, M.; Juppo, A.; Laius, O.; Siven, M. Compliance with Pregnancy Prevention Recommendations for Isotretinoin Following the Amendment of the European Union Pregnancy Prevention Program: A Repeat Study in Estonia. Drugs Real World Outcomes 2024, 11, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Havet, A.; Bouvard, C.; Moskal, A.; Chanelière, M.; Massardier, J.; Lebrun-Vignes, B.; Jonville-Bera, A.P.; Payet, C.; Viprey, M. Compliance with the pregnancy prevention program among women initiating isotretinoin treatment between 2014 and 2021: A nationwide cohort study on the French Health Data System (SNDS). J. Eur. Acad. Dermatol. Venereol. 2025, 39, 806–814. [Google Scholar] [CrossRef]
- Zane, L.T.; Leyden, W.A.; Marqueling, A.L.; Manos, M.M. A population-based analysis of laboratory abnormalities during isotretinoin therapy for acne vulgaris. Arch. Dermatol. 2006, 142, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Zaenglein, A.L.; Pathy, A.L.; Schlosser, B.J.; Alikhan, A.; Baldwin, H.E.; Berson, D.S.; Bowe, W.P.; Graber, E.M.; Harper, J.C.; Kang, S.; et al. Guidelines of care for the management of acne vulgaris. J. Am. Acad. Dermatol. 2016, 74, 945–973.e33. [Google Scholar] [CrossRef]
- Hughes, L.M.; Schuler, A.; Sharmuk, M.; Schauer, J.M.; Pavone, M.E.; Bernardi, L.A. Early β-hCG levels predict live birth after single embryo transfer. J. Assist. Reprod. Genet. 2022, 39, 2355–2364. [Google Scholar] [CrossRef]
- Ozer, G. Initial β-hCG levels and 2-day-later increase rates effectively predict pregnancy outcomes in single blastocyst transfer in frozen-thawed or fresh cycles: A retrospective cohort study. Medicine 2023, 102, e35605. [Google Scholar] [CrossRef]
- Del Rosso, J.Q. Face to face with oral isotretinoin: A closer look at the spectrum of therapeutic outcomes and why some patients need repeated courses. J. Clin. Aesthet. Dermatol. 2012, 5, 17–24. [Google Scholar]
- Brzezinski, P.; Borowska, K.; Chiriac, A.; Smigielski, J. Adverse effects of isotretinoin: A large, retrospective review. Dermatol. Ther. 2017, 30, e12483. [Google Scholar] [CrossRef]
- Jakobi, A.U.; Bircher, A.J.; Pagnamenta, A.; Terrani, I. Isotretinoin Concerns in Switzerland: A Student-Based Transversal Study. J. Clin. Med. 2025, 14, 1801. [Google Scholar] [CrossRef] [PubMed]
- Hebebrand, M. Isotretinoin Often Continued Despite Mood Concerns, Dermatology Times. 2025. Available online: https://www.dermatologytimes.com/view/isotretinoin-often-continued-despite-mood-concerns (accessed on 13 May 2025).
- Raguideau, F.; Mezzarobba, M.; Zureik, M.; Weill, A.; Ricordeau, P.; Alla, F. Compliance with pregnancy prevention plan recommendations in 8672 French women of childbearing potential exposed to acitretin. Pharmacoepidemiol. Drug Saf. 2015, 24, 526–533. [Google Scholar] [CrossRef]
- British Association of Dermatologists. Guidelines for Isotretinoin Use and Monitoring; BAD: London, UK, 2019. [Google Scholar]
- Emtenani, S.; Abdelghaffar, M.; Ludwig, R.J.; Schmidt, E.; Kridin, K. Risk and timing of isotretinoin-related laboratory disturbances: A population-based study. Int. J. Dermatol. 2024, 63, 1740–1747. [Google Scholar] [CrossRef] [PubMed]
- On, S.C.; Zeichner, J. Isotretinoin updates. Dermatol. Ther. 2013, 26, 377–389. [Google Scholar] [CrossRef]
- Werner, C.A.; Papic, M.J.; Ferris, L.K.; Lee, J.K.; Borrero, S.; Prevost, N.; Schwarz, E.B. Women’s experiences with isotretinoin risk reduction counseling. JAMA Dermatol. 2014, 150, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, J.S.; Shin, D.B.; Wang, S.; Margolis, D.J.; Takeshita, J. The clinical utility of laboratory monitoring during isotretinoin therapy for acne and changes to monitoring practices over time. J. Am. Acad. Dermatol. 2020, 82, 72–79. [Google Scholar] [CrossRef]
- Murshidi, R.; Bani Hamad, S.; Al Refaei, A.; Shewaikani, N.; Shaf’ei, M.; Alshoubaki, S.N.; Haddad, T.A.; Khasawneh, T.; Fkheideh, T.; Abdallat, M. A novel predictive method for risk stratification in acne patients receiving isotretinoin: An analysis of laboratory abnormalities and changes in inflammatory parameters. J. Dermatol. Treat. 2024, 35, 2301435. [Google Scholar] [CrossRef]
- Pinheiro, S.P.; Kang, E.M.; Kim, C.Y.; Governale, L.A.; Zhou, E.H.; Hammad, T.A. Concomitant use of isotretinoin and contraceptives before and after iPledge in the United States. Pharmacoepidemiol. Drug Saf. 2013, 22, 1251–1257. [Google Scholar] [CrossRef]
- Schaefer, C.; Meister, R.; Weber-Schoendorfer, C. Isotretinoin exposure and pregnancy outcome: An observational study of the Berlin Institute for Clinical Teratology and Drug Risk Assessment in Pregnancy. Arch. Gynecol. Obstet. 2010, 281, 221–227. [Google Scholar] [CrossRef]
- Lelubre, M.; Hamdani, J.; Senterre, C.; Amighi, K.; Peres, M.; Schneider, M.P.; Bugnon, O.; De Vriese, C. Evaluation of compliance with isotretinoin PPP recommendations and exploration of reasons for non-compliance: Survey among French-speaking health care professionals and patients in Belgium. Pharmacoepidemiol. Drug Saf. 2018, 27, 668–673. [Google Scholar] [CrossRef]
- Ghosh, I.; Marques, F.; Chakraborty, S. A new bivariate Poisson distribution via conditional specification: Properties and applications. J. Appl. Stat. 2020, 48, 3025–3047. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Method of Treatment: Group I | Method of Treatment: Group IIA | Method of Treatment: Group IIB | Total |
|---|---|---|---|---|
| Number of respondents | 113 | 270 | 186 | 569 |
| Minimum | 30.00 | 88.89 | 94.12 | 30.00 |
| Maximum | 147.94 | 147.94 | 150.00 | 150.00 |
| Median | 130.43 | 135.21 | 134.69 | 134.69 |
| The arithmetic mean | 115.89 | 133.74 | 134.10 | 130.31 |
| Standard deviation | 34.70 | 9.66 | 7.07 | 18.69 |
| Asymmetry factor | −1.34 | −2.24 | −0.81 | −3.39 |
| Statistical analysis tests | ANOVA Kruskal–Wallis H = 19.89 p < 0.001 (p = 0.000) ZI,IIA Mann–Whitney = −4.37 p > 0.001(p = 0.0000) ZI,IIB Mann–Whitney = −3.26 p < 0.01 (p = 0.0011) ZIIA,IIB Mann–Whitney = 1.33 p > 0.05 (p = 0.1824) | |||
| Parameters | Discontinuation of Therapy: Yes | Discontinuation of Therapy: No | Total |
|---|---|---|---|
| Number of respondents | 27 | 86 | 113 |
| Minimum | 30.00 | 118.40 | 30.00 |
| Maximum | 97.67 | 147.94 | 147.94 |
| Median | 54.54 | 133.33 | 130.43 |
| The arithmetic mean | 57.30 | 134.29 | 115.89 |
| Standard deviation | 18.58 | 6.94 | 34.70 |
| Asymmetry factor | 0.53 | −0.10 | −1.34 |
| Statistical analysis test | Z Mann–Whitney = 7.81 p < 0.001 (p = 0.0000) | ||
| Age Group | N | Mean Dose (mg/kg) | SD | Median | Min | Max |
|---|---|---|---|---|---|---|
| ≤17 | 283 | 129.97 | 21.08 | 136.36 | 30.51 | 150.00 |
| 18–21 | 183 | 130.62 | 16.29 | 132.78 | 36.73 | 147.94 |
| 22–25 | 103 | 130.71 | 15.62 | 132.35 | 30.00 | 142.85 |
| Who the Programme Applies to: | Requirements: |
|---|---|
| All Patients |
|
| Female Patients of Childbearing Potential (FCBP) |
|
| Patients Declaring Abstinence |
|
| Male Patients |
|
| Prescribers (Physicians) |
|
| Pharmacies |
|
| Wholesalers/Distributors |
|
| Who the Programme Applies to: | Requirements: |
|---|---|
| All Patients |
|
| Female Patients of Childbearing Potential (FCBP) |
|
| Patients Declaring Abstinence |
|
| Male Patients |
|
| Prescribers (Physicians) |
|
| Pharmacies |
|
| Wholesalers/Distributors |
|
| Category: | iPLEDGE (USA): | PPP (EU): |
|---|---|---|
| Programme Type | REMS, mandated by FDA | RMM, mandated by EMA |
| Patient Enrollment | Mandatory central registration | No central system; local documentation |
| Patient Education | Counselling + signed form + printed materials | Same as iPLEDGE |
| Pregnancy Test (PRE) | Required within 7 days before prescribing | Ideally within 3 days before treatment |
| Pregnancy Test (Ongoing) | Required monthly, logged in system | Recommended monthly |
| Pregnancy Test (Post) | Not required, but contraception must continue 1 month after | Required after treatment to confirm no pregnancy |
| Contraception | Two methods of abstinence | One effective or two complementary methods |
| Contraception Timing | Start ≥1 month before, during, and 1 month after | Same as iPLEDGE |
| Prescription Limit | 30-day supply; expires in 7 days | 30-day limit; renewal only with updated documentation |
| Prescriber Duties | Monthly documentation in system; verify all requirements | Complete checklist; ensure all measures are met |
| Pharmacist Duties | Confirm compliance in iPLEDGE; electronic authorization | Verify checklist; dispense max 30 days |
| If Pregnancy Occurs | Stop treatment; refer to specialist | Same as iPLEDGE |
| Gender Policy (Post-2021) | Based on reproductive potential (gender-neutral) | Based on biological sex; no EU-wide gender-neutral approach |
| Digital Burden/Access | Online system often cited as barrier | Less centralised; variable implementation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzeziński, P.; Feszak, I.J.; Śmigielski, J.; Kawczak, P.; Bączek, T. Compliance with the European Pregnancy Prevention Programme in Isotretinoin Treatment: Safety Outcomes and Dose-Related Correlations. J. Clin. Med. 2025, 14, 3497. https://doi.org/10.3390/jcm14103497
Brzeziński P, Feszak IJ, Śmigielski J, Kawczak P, Bączek T. Compliance with the European Pregnancy Prevention Programme in Isotretinoin Treatment: Safety Outcomes and Dose-Related Correlations. Journal of Clinical Medicine. 2025; 14(10):3497. https://doi.org/10.3390/jcm14103497
Chicago/Turabian StyleBrzeziński, Piotr, Igor Jarosław Feszak, Janusz Śmigielski, Piotr Kawczak, and Tomasz Bączek. 2025. "Compliance with the European Pregnancy Prevention Programme in Isotretinoin Treatment: Safety Outcomes and Dose-Related Correlations" Journal of Clinical Medicine 14, no. 10: 3497. https://doi.org/10.3390/jcm14103497
APA StyleBrzeziński, P., Feszak, I. J., Śmigielski, J., Kawczak, P., & Bączek, T. (2025). Compliance with the European Pregnancy Prevention Programme in Isotretinoin Treatment: Safety Outcomes and Dose-Related Correlations. Journal of Clinical Medicine, 14(10), 3497. https://doi.org/10.3390/jcm14103497