
Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
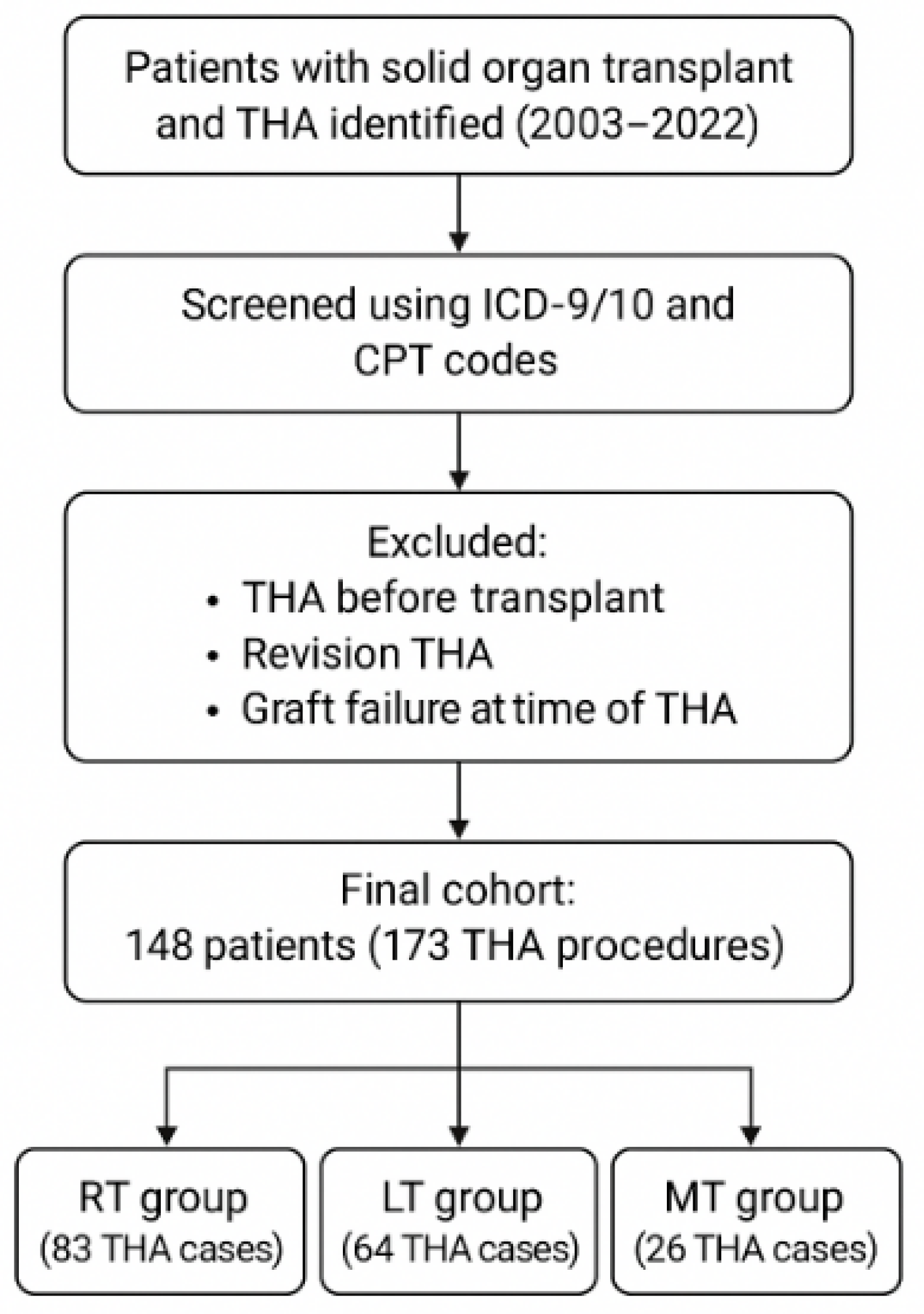
2.1. Study Design and Setting
2.2. Data Collection
2.3. Data Analyses
3. Results
3.1. Cohort Characteristics
3.2. Complications and Risk Factors
3.3. Reoperations and Revisions
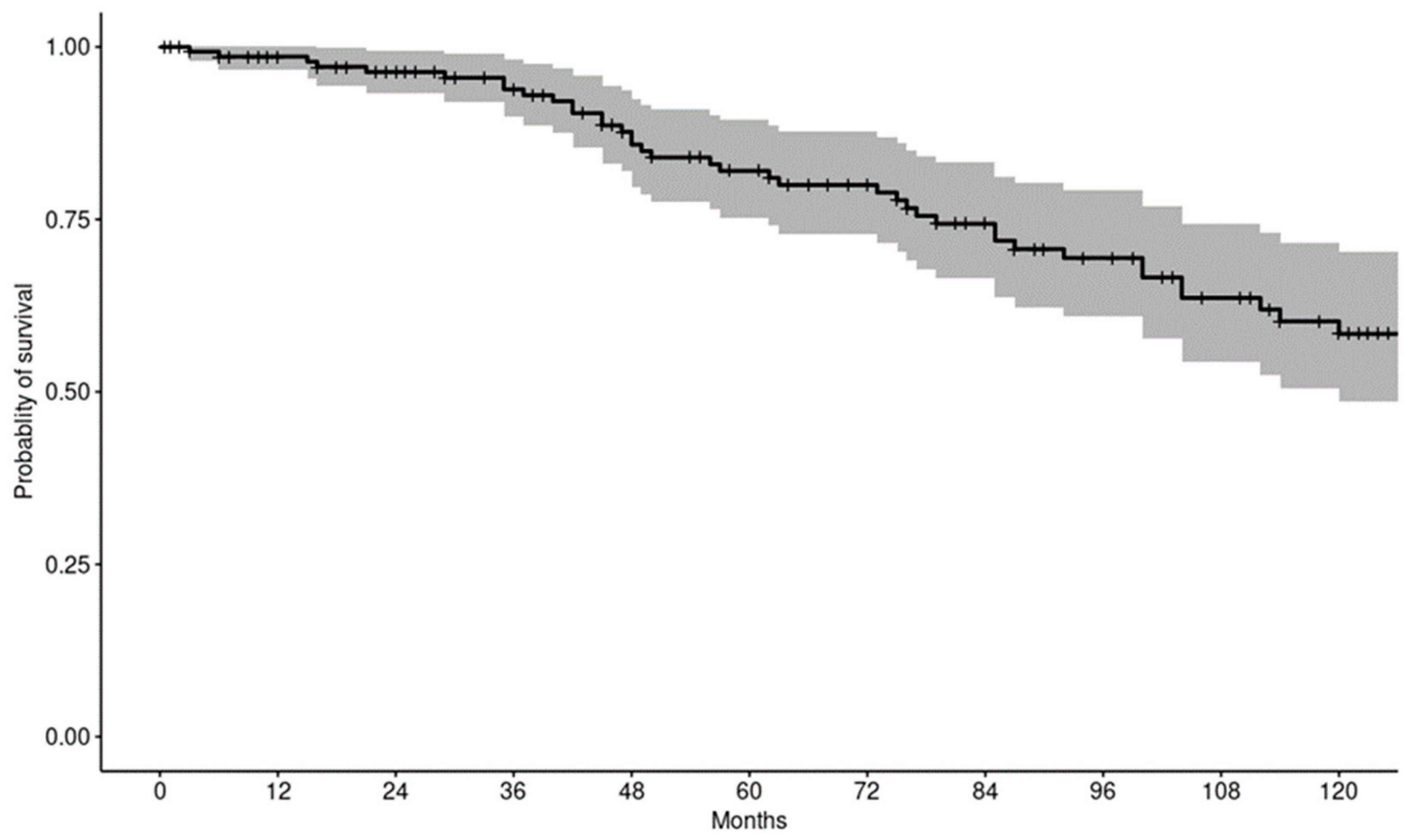
3.4. Patient Survivorship
4. Discussion
4.1. Study Context and Novelty
4.2. Patient Demographics and Donor Characteristics
4.3. Comorbidities
4.4. Complications
4.5. Reoperations and Revisions
4.6. Patient Survival
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Network for Organ Sharing (UNOS) Website. Organ Transplantation Community and UNOS Member Community. Available online: https://unos.org/news/2022-organ-transplants-again-set-annual-records/ (accessed on 1 January 2025).
- Israni, A.K.; Zaun, D.; Hadley, N.; Rosendale, J.D.; Schaffhausen, C.; McKinney, W.; Snyder, J.J.; Kasiske, B.L. OPTN/SRTR 2018 Annual Data Report: Deceased Organ Donation. Am. J. Transplant. 2020, 20, 509–541. [Google Scholar] [CrossRef] [PubMed]
- Scientific Registry of Transplant Recipients (SRTR) Website. The OPTN/SRTR Annual Data Report. 2021. Available online: https://srtr.transplant.hrsa.gov/adr/adr2021 (accessed on 1 January 2025).
- Navale, S.M.; Szubski, C.R.; Klika, A.K.; Schiltz, N.K.; Desai, P.P.; Barsoum, W.K. The impact of solid organ transplant history on inpatient complications, mortality, length of stay, and cost for primary total hip arthroplasty admissions in the United States. J. Arthroplast. 2017, 32, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Bucci, J.R.; Oglesby, R.J.; Agodoa, L.Y.; Abbott, K.C. Hospitalizations for total hip arthroplasty after renal transplantation in the United States. Am. J. Transplant. 2002, 2, 999–1004. [Google Scholar] [CrossRef]
- Rasanen, P.; Paavolainen, P.; Sintonen, H.; Koivisto, A.; Blom, M.; Ryynänen, O.P.; Roine, R.P. Effectiveness of hip or knee replacement surgery in terms of quality-adjusted life years and costs. Acta Orthop. 2007, 78, 108–115. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons. American Academy of Orthopaedic Surgeons. American Joint Replacement Registry (AJRR): 2022 Annual Report. In The Ninth Annual Report of the AJRR on Hip and Knee Arthroplasty; American Academy of Orthopaedic Surgeons: Rosemont, IL, USA, 2022. [Google Scholar]
- Ledford, C.K.; Watters, T.S.; Wellman, S.S.; Attarian, D.E.; Bolognesi, M.P. Risk versus reward: Total joint arthroplasty outcomes after various solid organ transplantations. J. Arthroplast. 2014, 29, 1548–1552. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Sato, T.; Hasegawa, Y.; Futamura, K.; Hiramitsu, T.; Ichimori, T.; Goto, N.; Narumi, S.; Takeda, A.; Watarai, Y. Persistent hyperparathyroidism after preemptive kidney transplantation. Clin. Exp. Nephrol. 2023, 27, 882–889. [Google Scholar] [CrossRef]
- Hauer, G.; Rasic, L.; Klim, S.; Leitner, L.; Leithner, A.; Sadoghi, P. Septic complications are on the rise and aseptic loosening has decreased in total joint arthroplasty: An updated complication-based analysis using worldwide arthroplasty registers. Arch. Orthop. Trauma Surg. 2024, 144, 5199–5204. [Google Scholar] [CrossRef]
- Zhou, H.; Yang, Y.; Zhang, Y.; Li, F.; Shen, Y.; Qin, L.; Huang, W. Current status and perspectives of diagnosis and treatment of periprosthetic joint infection. Infect. Drug Resist. 2024, 17, 2417–2429. [Google Scholar] [CrossRef]
- Mundi, R.; Pincus, D.; Schemitsch, E.; Ekhtiari, S.; Paterson, J.M.; Chaudhry, H.; Leis, J.A.; Redelmeier, D.A.; Ravi, B. Association Between Periprosthetic Joint Infection and Mortality Following Primary Total Hip Arthroplasty. J. Bone Joint Surg. Am. 2024, 106, 1546–1552. [Google Scholar] [CrossRef]
- Pegios, V.F.; Kenanidis, E.; Tsotsolis, S.; Potoupnis, M.; Tsiridis, E. Bisphosphonates’ use and risk of aseptic loosening following total hip arthroplasty: A systematic review. EFORT Open Rev. 2023, 8, 798–808. [Google Scholar] [CrossRef]
- Hodges, N.A.; Sussman, E.M.; Stegemann, J.P. Aseptic and septic prosthetic joint loosening: Impact of biomaterial wear on immune cell function, inflammation, and infection. Biomaterials 2021, 278, 121127. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.B.; Konttinen, Y.T.; Takagi, M. Joint replacement surgery and the innate immune system. J. Long-Term Eff. Med. Implant. 2014, 24, 253–257. [Google Scholar] [CrossRef]
- Connors, J.P.; Stelzer, J.W.; Garvin, P.M.; Wellington, I.J.; Solovyova, O. The Role of the Innate Immune System in Wear Debris-Induced Inflammatory Peri-Implant Osteolysis in Total Joint Arthroplasty. Bioengineering 2022, 9, 764. [Google Scholar] [CrossRef]
- Gries, C.M.; Kielian, T. Staphylococcal Biofilms and Immune Polarization During Prosthetic Joint Infection. J. Am. Acad. Orthop. Surg. 2017, 25, S20–S24. [Google Scholar] [CrossRef]
- Portillo, M.E.; Salvadó, M.; Alier, A.; Sorli, L.; Martínez, S.; Horcajada, J.P.; Puig, L. Prosthesis failure within 2 years of implantation is highly predictive of infection. Clin. Orthop. Relat. Res. 2013, 471, 3672–3678. [Google Scholar] [CrossRef]
- Jafari, S.M.; Coyle, C.; Mortazavi, S.M.J.; Sharkey, P.F.; Parvizi, J. Revision hip arthroplasty: Infection is the most common cause of failure. Clin. Orthop. Relat. Res. 2010, 468, 2046–2051. [Google Scholar] [CrossRef]
- Chalmers, B.P.; Ledford, C.K.; Statz, J.M.; Perry, K.I.; Mabry, T.M.; Hanssen, A.D.; Abdel, M.P. Survivorship after primary total hip arthroplasty in solid-organ transplant patients. J. Arthroplast. 2016, 31, 2525–2529. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Yang, Y.; Luk, J.; Sofair, A. Epidemiology of chronic liver disease in the United States. In Clinical Epidemiology of Chronic Liver Diseases; Springer: Berlin/Heidelberg, Germany, 2019; pp. 57–74. [Google Scholar]
- Klement, M.R.; Penrose, C.T.; Bala, A.; Green, C.L.; Mather, R.C.; Wellman, S.S.; Bolognesi, M.P.; Seyler, T.M. Complications of total hip arthroplasty following solid organ transplantation. J. Orthop. Sci. 2017, 22, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Lim, E.J.; Lee, J. Clinical outcomes following primary hip replacement arthroplasties in patients with solid organ transplantation: A systematic review and meta-analysis. Hip Pelvis 2022, 34, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Duplantier, N.L.; Rivere, A.E.; Cohen, A.J.; Chimento, G.F. Hip and knee arthroplasty outcomes after abdominal organ transplantation. J. Surg. Orthop. Adv. 2018, 27, 119–124. [Google Scholar] [PubMed]
- Douglas, S.J.; Pervaiz, S.S.; Sax, O.C.; Mohamed, N.S.; Delanois, R.E.; Johnson, A.J. Comparing primary total hip arthroplasty in renal transplant recipients to patients on dialysis for end-stage renal disease: A nationally matched analysis. J. Bone Jt. Surg. Am. 2021, 103, 2215–2220. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.C.; Son, M.S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are we winning or losing the battle with periprosthetic joint infection: Trends in periprosthetic joint infection and mortality risk for the Medicare population. J. Arthroplast. 2018, 33, 3238–3245. [Google Scholar] [CrossRef]
- Bradford, D.S.; Janes, P.C.; Simmons, R.S.; Najarian, J.S. Total hip arthroplasty in renal transplant recipients. Clin. Orthop. Relat. Res. 1983, 181, 107–114. [Google Scholar] [CrossRef]
- Nowicki, P.; Chaudhary, H. Total hip replacement in renal transplant patients. J. Bone Jt. Surg. Br. 2007, 89, 1561–1566. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.R.; Gu, A.; Mawn, J.; Fassihi, S.C.; Wang, K.Y.; Golladay, G.J.; Thakkar, S.C. Increased medical complications following primary total hip arthroplasty in patients with solid organ transplant: A matched cohort analysis. J. Arthroplast. 2022, 37, 57–61. [Google Scholar] [CrossRef]
- Khatod, M.; Inacio, M.; Dell, R.M.; Bini, S.A.; Paxton, E.W.; Namba, R.S. Association of bisphosphonate use and risk of revision after THA: Outcomes from a US total joint replacement registry. Clin. Orthop. Relat. Res. 2015, 473, 3412–3420. [Google Scholar] [CrossRef]
- Douglas, S.J.; Remily, E.A.; Sax, O.C.; Pervaiz, S.S.; Mohamed, N.S.; Kelemen, M.N.; Delanois, R.E.; Johnson, A.J. Primary total hip arthroplasty complications and costs in liver transplant recipients: A matched analysis using a national database. HIP Int. 2023, 33, 178–183. [Google Scholar] [CrossRef]
- Reynolds, C.A.; Issa, T.Z.; Manning, D.W. Patients who have pre-existing atrial fibrillation require increased postoperative care following total joint arthroplasty. J. Arthroplast. 2024, 39, 60–67. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Type of Transplant | Kidney (N = 83) | Liver (N = 64) | Multiple (N = 26) | Total (N = 173) | p Value |
|---|---|---|---|---|---|
| Age at Time of THA | 0.011 1 | ||||
| Mean (range) | 65.1 (30–80) | 64.9 (47–78) | 57.6 (35–89) | 63.9 (30–89) | |
| BMI at Time of THA | 0.666 1 | ||||
| Mean (range) | 29.7 (19.1–43.2) | 30.3 (19.1–48.2) | 28.6 (20.0–34.9) | 29.7 (19.1–48.2) | |
| ASA Score at Time of THA | 0.352 2 | ||||
| 2 | 11 (14%) | 4 (7%) | 2 (8%) | 17 (10%) | |
| 3 | 66 (82%) | 51 (85%) | 20 (80%) | 137 (83%) | |
| 4 | 3 (4%) | 5 (8%) | 3 (12%) | 11 (7%) | |
| Interval from SOT (months) | 0.217 1 | ||||
| Mean (range) | 63.4 (5–255) | 71.3 (0–252) | 92.9 (4–281) | 70.7 (0–281) | |
| Cemented (Y/N) | 0.805 2 | ||||
| No | 62 (75%) | 50 (78%) | 21 (81%) | 133 (77%) | |
| Yes | 21 (25%) | 14 (22%) | 5 (19%) | 40 (23%) | |
| Preoperative Cr | 0.038 1 | ||||
| Mean (range) | 1.6 (0.8–6.2) | 1.3 (0.7–3.1) | 1.7 (0.8–3.7) | 1.5 (0.7–6.2) |
| Type of Transplant | Kidney (N = 83) | Liver (N = 64) | Multiple (N = 26) | Total (N = 173) | p Value |
|---|---|---|---|---|---|
| Induction Therapy | <0.001 1 | ||||
| Thymoglobulin | 38 (46%) | 0 (0%) | 14 (54%) | 52 (30%) | |
| Alemtuzumab | 15 (18%) | 0 (0%) | 0 (0%) | 15 (9%) | |
| Basiliximab | 24 (29%) | 13 (20%) | 5 (19%) | 42 (24%) | |
| Daclizumab | 3 (4%) | 2 (3%) | 0 (0%) | 5 (3%) | |
| Corticosteroids | 3 (4%) | 45 (70%) | 5 (19%) | 53 (31%) | |
| None Maintenance Therapy | 0 (0%) | 4 (6%) | 2 (8%) | 6 (3%) | |
| Tacrolimus | 78 (94%) | 60 (94%) | 24 (92%) | 162 (94%) | 0.915 1 |
| Mycophenolate | 79 (95%) | 36 (56%) | 24 (92%) | 139 (80%) | <0.001 1 |
| Sirolimus | 9 (11%) | 7 (11%) | 6 (23%) | 22 (13%) | 0.259 1 |
| Everolimus | 0 (0%) | 1 (2%) | 2 (8%) | 3 (2%) | 0.030 1 |
| Azathioprine | 0 (0%) | 7 (11%) | 5 (19%) | 12 (7%) | <0.001 1 |
| Belatacept | 4 (5%) | 0 (0%) | 0 (0%) | 4 (2%) | 0.210 1 |
| Cyclosporine | 1 (1%) | 7 (11%) | 5 (19%) | 13 (8%) | 0.005 1 |
| Ongoing Corticosteroid | 79 (95%) | 54 (84%) | 26 (100%) | 159 (92%) | 0.021 1 |
| Type of Transplant | Kidney (N = 83) | Liver (N = 64) | Multiple (N = 26) | Total (N = 173) | p Value |
|---|---|---|---|---|---|
| Acute Medical Complications | |||||
| DVT/Thrombophlebitis | 1 (1%) | 1 (2%) | 0 (0%) | 2 (1%) | 1.000 1 |
| Anemia | 13 (16%) | 11 (17%) | 6 (23%) | 30 (17%) | 0.657 1 |
| Kidney Injury | 3 (4%) | 2 (3%) | 1 (4%) | 6 (3%) | 1.000 1 |
| PE | 1 (1%) | 1 (2%) | 0 (0%) | 2 (1%) | 1.000 1 |
| AFib or Flutter | 1 (1%) | 4 (6%) | 0 (0%) | 5 (3%) | 0.187 1 |
| Pneumonia/Lung Injury | 3 (4%) | 2 (3%) | 1 (4%) | 6 (3%) | 1.000 1 |
| Pancreatitis | 0 (0%) | 0 (0%) | 1 (4%) | 1 (1%) | 0.150 1 |
| Sepsis/Shock | 1 (1%) | 0 (0%) | 0 (0%) | 1 (1%) | 1.000 1 |
| Electrolyte Imbalance | 1 (1%) | 0 (0%) | 1 (4%) | 2 (1%) | 0.414 1 |
| MI/Unstable Angina | 1 (1%) | 0 (0%) | 1 (4%) | 2 (1%) | 0.414 1 |
| Seizure | 1 (1%) | 0 (0%) | 0 (0%) | 1 (1%) | 1.000 1 |
| Stroke | 1(1%) | 0(0%) | 0(0%) | 1(1%) | 1.000 |
| UTI | 4 (5%) | 2 (3%) | 0 (0%) | 6 (3%) | 0.747 1 |
| Acute Surgical Complications | |||||
| Wound Infection | 1 (1%) | 1 (2%) | 2 (8%) | 4 (2%) | 0.155 1 |
| Wound Dehiscence/Excess Wound Drainage | 1 (1%) | 0 (0%) | 1 (4%) | 2 (1%) | 0.414 1 |
| Periprosthetic Fracture | 0 (0%) | 1 (2%) | 0 (0%) | 1 (1%) | 0.520 1 |
| Chronic Surgical Complications | |||||
| Wound Infection | 0 (0%) | 0 (0%) | 1 (4%) | 1 (1%) | 0.150 1 |
| Joint Infection | 1 (1%) | 0 (0%) | 1 (4%) | 2 (1%) | 0.414 1 |
| Dislocation | 2 (2%) | 0 (0%) | 1 (4%) | 3 (2%) | 0.275 1 |
| Periprosthetic Fracture | 0 (0%) | 2 (3%) | 0 (0%) | 2 (1%) | 0.269 1 |
| Kidney (N = 77) | Liver (N = 77) | Multiple (N = 22) | Total (N = 176) | p Value | |
|---|---|---|---|---|---|
| Revisions | 1 (1%) | 0 (0%) | 1 (4%) | 2 (1%) | 0.414 1 |
| Reoperations (including Revisions) | 3 (4%) | 0 (0%) | 2 (8%) | 5 (3%) | 0.104 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gill, V.S.; Boddu, S.P.; Mansour, E.; Abu Jawdeh, B.G.; Khan, M.A.; McGary, A.; Clarke, H.; Spangehl, M.; Abdel, M.P.; Ledford, C.K.; et al. Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty. J. Clin. Med. 2025, 14, 3486. https://doi.org/10.3390/jcm14103486
Gill VS, Boddu SP, Mansour E, Abu Jawdeh BG, Khan MA, McGary A, Clarke H, Spangehl M, Abdel MP, Ledford CK, et al. Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty. Journal of Clinical Medicine. 2025; 14(10):3486. https://doi.org/10.3390/jcm14103486
Chicago/Turabian StyleGill, Vikram S., Sayi P. Boddu, Elie Mansour, Bassam G. Abu Jawdeh, Muhammad Ali Khan, Alyssa McGary, Henry Clarke, Mark Spangehl, Matthew P. Abdel, Cameron K. Ledford, and et al. 2025. "Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty" Journal of Clinical Medicine 14, no. 10: 3486. https://doi.org/10.3390/jcm14103486
APA StyleGill, V. S., Boddu, S. P., Mansour, E., Abu Jawdeh, B. G., Khan, M. A., McGary, A., Clarke, H., Spangehl, M., Abdel, M. P., Ledford, C. K., & Bingham, J. S. (2025). Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty. Journal of Clinical Medicine, 14(10), 3486. https://doi.org/10.3390/jcm14103486