
Health Status of Tsimihety Women: Sexually Transmitted Infections and Schistosomiasis, Northern Madagascar



Abstract
1. Introduction
2. Materials and Methods
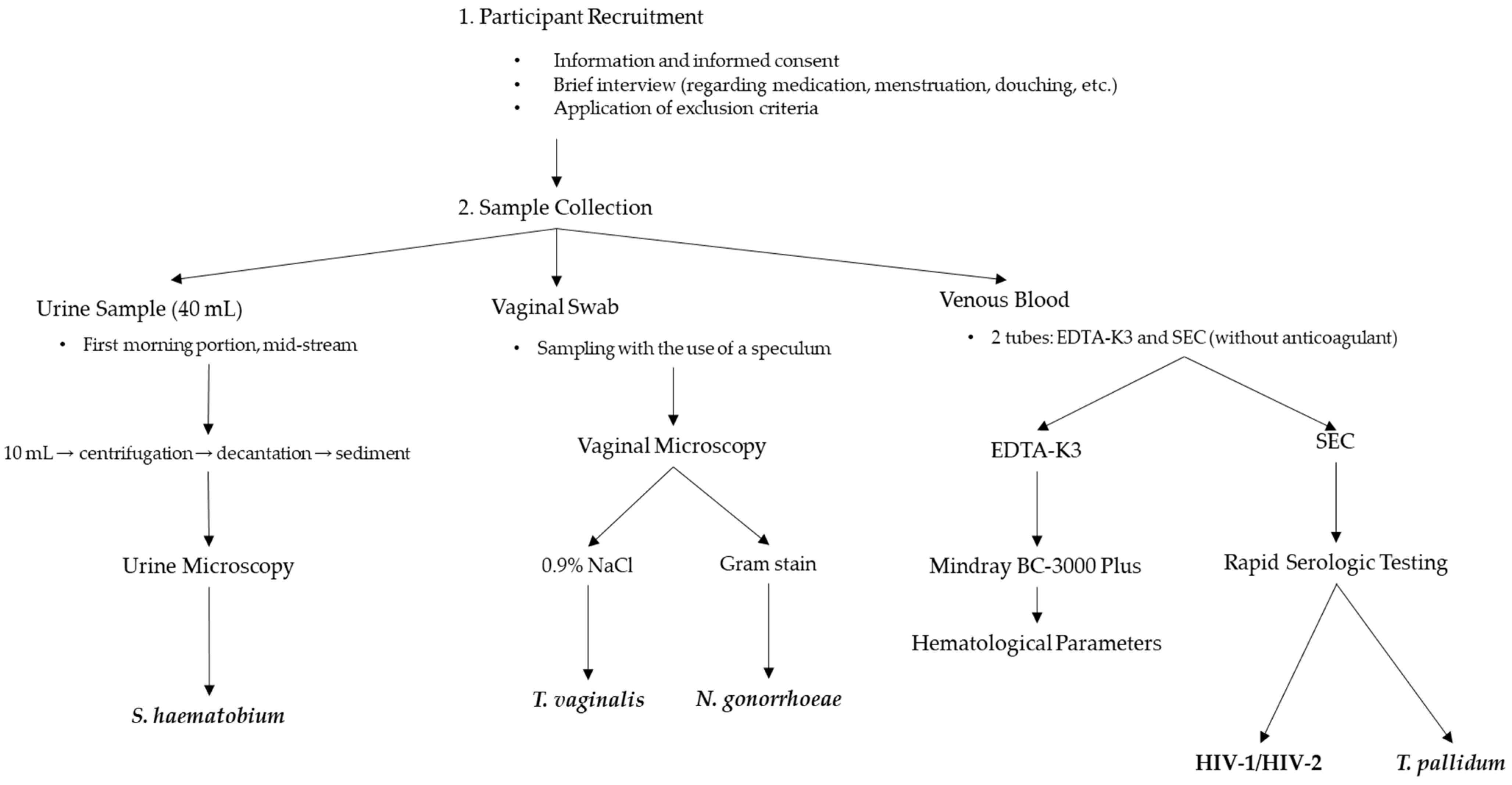
2.1. Study Group and Sample Collection
2.2. Sociocultural and Economic Barriers to Healthcare Access
2.2.1. Light Microscopy
Urine Sediment Examination
Vaginal Swab Examination
2.2.2. Measurement of Hematological Parameters
2.2.3. Immunochromatographic Tests
2.3. Statistical Analysis
2.4. Ethical Approval
2.5. Study Variables
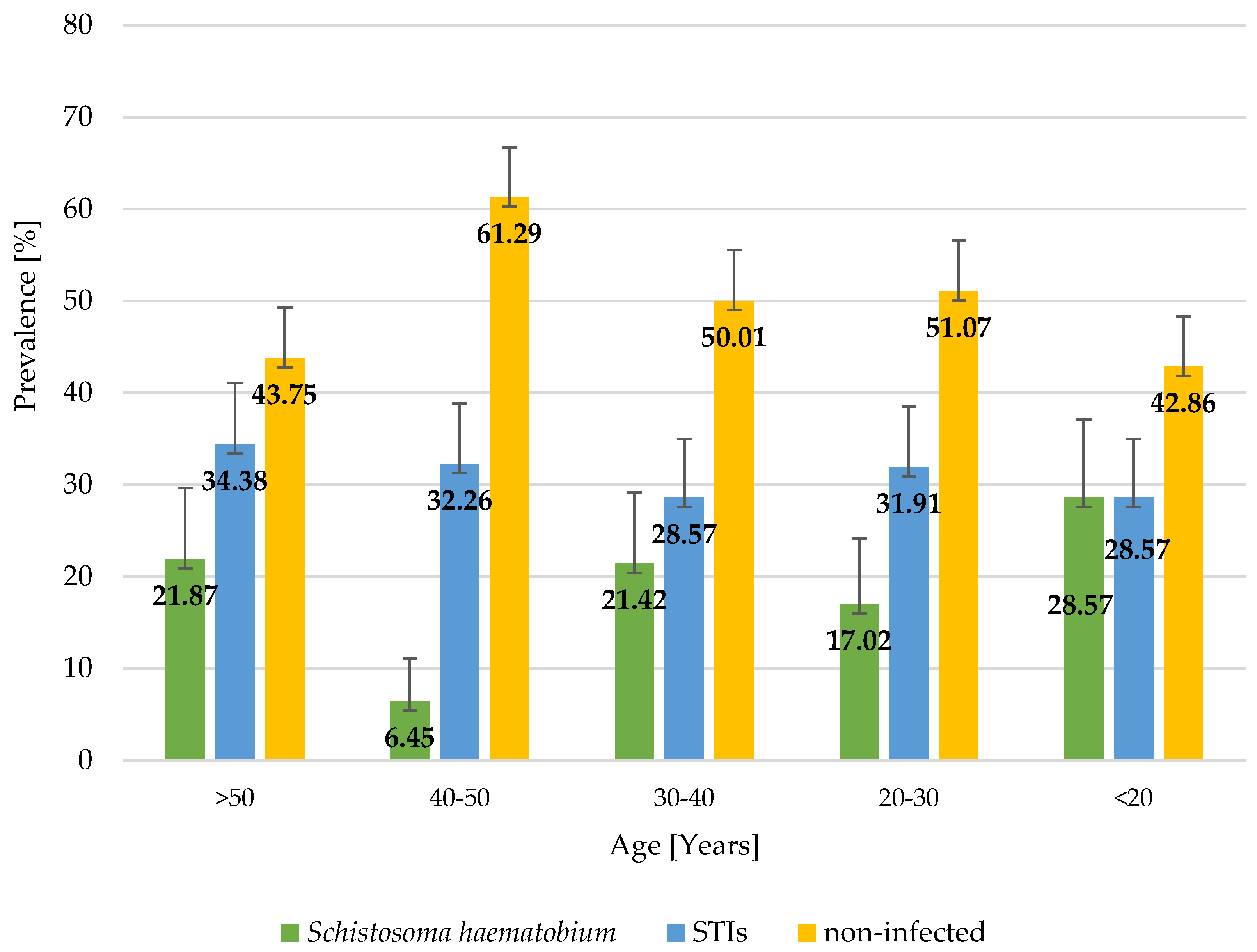
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Madagascar. Overview. World Bank, 2024. Available online: https://data.worldbank.org/country/madagascar (accessed on 29 December 2024).
- Andrianantoandro, V.T.; Pourette, D.; Rakotomalala, O.; Ramaroson, H.J.V.; Ratovoson, R.; Rakotoarimanana, F.M.J. Factors influencing maternal healthcare seeking in a highland region of Madagascar: A mixed methods analysis. BMC Pregnancy Childbirth. 2021, 21, 428. [Google Scholar] [CrossRef] [PubMed]
- Razakamanana, M.V.; Andrianatoandro, V.T.; Ramiandrisoa, T.O. Do public health expenditures affect maternal and child health in Madagascar? Health Econ. Rev. 2023, 13, 47. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chayakulkeeree, M.; Chakrabarti, A.; Gan, G.G.; Kwong, Y.L.; Liu, W.-L.; Tan, B.H.; Todi, S. Unmet needs and practical solutions in the management of invasive mould infections in Asia. J. Antimicrob. Chemother. 2022, 77, 2579–2585. [Google Scholar] [CrossRef]
- Institute National de la Statistique (INSTAT). Madagascar DHS, 2021—Final Report (in French). Available online: https://dhsprogram.com/publications/publication-FR376-DHS-Final-Reports.cfm (accessed on 18 December 2024).
- Rejoice Puthuchira, R.; Kulasekaran, R.A. Care seeking behaviour and barriers to accessing services for sexual health problems among women in rural areas of Tamilnadu state in India. J. Sex. Transm. Dis. 2014, 2014, 292157. [Google Scholar] [CrossRef]
- Robson, L.; Morris, J.; Andriatsihosena, M. Barriers to preventing unintended pregnancies and sexually transmitted infections as experienced by women in Fort Dauphin, southeast Madagascar. Eur. J. Contracept. Reprod. Health Care 2015, 20, 451–462. [Google Scholar] [CrossRef]
- Madagascar, Comité National de Lutte Contre le SIDA. Rapport D’activité sur la Riposte au SIDA à Madagascar, 2014. Available online: https://www.unaids.org/sites/default/files/country/documents/MDG_narrative_report_2014.pdf (accessed on 20 December 2024).
- Garchitorena, A.; Miller, A.C.; Cordier, L.F.; Ramananjato, R.; Rabeza, V.R.; Murray, M.; Cripps, A.; Hall, L.; Farmer, P.; Rich, M.; et al. In Madagascar, Use Of Health Care Services Increased When Fees Were Removed: Lessons For Universal Health Coverage. Health Aff. 2017, 36, 1443–1451. [Google Scholar] [CrossRef] [PubMed]
- Garchitorena, A.; Miller, A.C.; Cordier, L.F.; Randriamanambintsoa, M.; Razanadrakato, H.R.; Randriamihaja, M.; Razafinjato, B.; Finnegan, K.E.; Haruna, J.; Rakotonirina, L.; et al. District-level health system strengthening for universal health coverage: Evidence from a longitudinal cohort study in rural Madagascar, 2014-2018. BMJ Glob. Health 2020, 5, e003647. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schuster, A.; Randrianasolo, B.S.; Rabozakandraina, O.O.; Ramarokoto, C.E.; Brønnum, D.; Feldmeier, H. Knowledge, experiences, and practices of women affected by female genital schistosomiasis in rural Madagascar: A qualitative study on disease perception, health impairment and social impact. PLoS Negl. Trop. Dis. 2022, 16, e0010901. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morris, J.L.; Short, S.; Robson, L.; Andriatsihosena, M.S. Maternal health practices, beliefs and traditions in southeast Madagascar. Afr. J. Reprod. Health 2014, 18, 101–117. [Google Scholar]
- Institut Pasteur de Madagascar. Manuel de Prélèvement des Échantillons Primaires, 2023. Available online: https://www.pasteur.mg/wp-content/uploads/2023/11/CBC_MP_001_Manuel_de_pre-levement_des_echantillons_primaires_V14.pdf (accessed on 20 December 2024).
- Avni, A. Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. J. Int. AIDS Soc. 2015, 18, 20302. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Report on Global Sexually Transmitted Infection Surveillance. Geneva, Switzerland, 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 20 December 2024).
- World Health Organization (WHO). Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021: Toward ending STIs, 2016. Available online: https://www.who.int/publications/i/item/WHO-RHR-16.09 (accessed on 20 December 2024).
- Mbizvo, M.T.; Zaidi, S. Addressing critical gaps in achieving universal access to sexual and reproductive health (SRH): The case for improving adolescent SRH, preventing unsafe abortion, and enhancing linkages between SRH and HIV interventions. Int. J. Gynecol. Obstet. 2010, 110, S3–S6. [Google Scholar] [CrossRef] [PubMed]
- Newton-Levinson, A.; Leichliter, J.S.; Chandra-Mouli, V. Help and care seeking for sexually transmitted infections among youth in low- and middle-income countries. Sex. Transm. Dis. 2017, 44, 319. [Google Scholar] [CrossRef]
- Asres, A.W.; Endalew, M.M.; Mengistu, S.Y. Prevalence and trends of sexually transmitted infections among pregnant women in Mizan Tepi University Teaching Hospital, Southwest Ethiopia: A cross-sectional study. Pan Afr. Med. J. 2022, 42, 111. [Google Scholar] [CrossRef]
- Semwogerere, M.; Dear, N.; Tunnage, J.; Dear, N.; Tunnage, J.; Reed, D.; Kibuuka, H.; Kiweewa, F.; Iroezindu, M.; Bahemana, E.; et al. Factors associated with sexually transmitted infections among care-seeking adults in the African Cohort Study. BMC Public Health 2021, 21, 738. [Google Scholar] [CrossRef] [PubMed]
- Torrone, E.A.; Morrison, C.S.; Chen, P.L.; Kwok, C.; Francis, S.C.; Hayes, R.J.; Looker, K.J.; McCormack, S.; McGrath, N.; van de Wijgert, J.H.H.M.; et al. Prevalence of sexually transmitted infections and bacterial vaginosis among women in sub-Saharan Africa: An individual participant data meta-analysis of 18 HIV prevention studies. PLoS Med. 2018, 15, 1–38. [Google Scholar] [CrossRef]
- Shewarega, E.S.; Fentie, E.A.; Asmamaw, D.B.; Negash, W.D.; Fetene, S.M.; Teklu, R.E.; Aragaw, F.M.; Alemu, T.G.; Eshetu, H.B.; Belay, D.G. Sexually transmitted infections related care-seeking behavior and associated factors among reproductive age women in East Africa: A multilevel analysis of demographic and health surveys. BMC Public Health 2022, 22, 1714. [Google Scholar] [CrossRef] [PubMed]
- Isara, A.; Baldeh, A.K. Prevalence of sexually transmitted infections among pregnant women attending antenatal clinics in West Coast Region of The Gambia. Afr. Health Sci. 2021, 21, 585–592. [Google Scholar] [CrossRef]
- Leutscher, P.D.; Jensen, J.S.; Hoffmann, S.; Berthelsen, L.; Ramarakoto, C.-E.; Ramaniraka, V.; Randrianasolo, B.; Raharisolo, C.; Böttiger, B.; Rousset, D.; et al. Sexually transmitted infections in rural Madagascar at an early stage of the HIV epidemic: A 6-month community-based follow-up study. Sex. Transm. Dis. 2005, 32, 150–155. [Google Scholar] [CrossRef]
- Behets, F.; Andriamiadana, J.; Rasamilalao, D.; Ratsimbazafy, N.; Randrianasolo, D.; Dallabetta, G.; Cohen, M. Sexually transmitted infections and associated socio-demographic and behavioural factors in women seeking primary care suggest Madagascar’s vulnerability to rapid HIV spread. Trop. Med. Int. Health 2001, 6, 202–211. [Google Scholar] [CrossRef]
- Behets, F.M.; Andriamiadana, J.; Randrianasolo, D.; Rasamilalao, D.; Ratsimbazafy, N.; Dallabetta, G.; Cohen, M.S. Laboratory diagnosis of sexually transmitted infections in women with genital discharge in Madagascar: Implications for primary care. Int. J. STD AIDS. 2002, 13, 606–611. [Google Scholar] [CrossRef]
- Frickmann, H.; Schwarz, N.G.; Girmann, M.; Hagen, R.M.; Poppert, S.; Crusius, S.; Podbielski, A.; Heriniaina, J.N.; Razafindrabe, T.; Rakotondrainiarivelo, J.P.; et al. Serological survey of HIV and syphilis in pregnant women in Madagascar. Trop. Med. Int. Health 2013, 18, 35–39. [Google Scholar] [CrossRef]
- Xueref, S.; Holianjavony, J.; Daniel, R.; Kerouedan, D.; Fabry, J.; Vanhems, P. The absence of HIV seropositivity contrasts with a high prevalence of markers of sexually transmitted infections among registered female sex workers in Toliary, Madagascar. Trop. Med. Int. Health 2003, 8, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Banque Mondiale. Programme Global de Lutte Contre le VIH/SIDA. VIH/SIDA—Obtenir des Résultats, 2008. Available online: http://siteresources.worldbank.org/INTHIVAIDS/Resources/375798-1132695455908/M&EGRMadagascarFR.pdf (accessed on 19 December 2024).
- Fortas, C.; Harimanana, A.N.; Rasoanandrianina, S.B.; Rasoanaivo, T.F.; Razanadranaivo, H.L.; Mangahasimbola, R.T.; Rasolon, D.T.; Rafetrarivony, L.F.; Rasolofomanana, T.T.; Rabarisoa, L.; et al. Sexually transmitted infections and bacterial vaginosis in women of child-bearing age in Antananarivo, Madagascar: Prevalence and risk factors from a cross-sectional study. BMC Infect. Dis. 2025, 25, 262. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bigoni, J.; Catarino, R.; Benski, C.; Viviano, M.; Munoz, M.; Tilahizandry, H.; Petignat, P.; Vassilakos, P. High Burden of Human Papillomavirus Infection in Madagascar: Comparison With Other Sexually Transmitted Infections. Infect. Dis. Res. Treat. 2018, 11, 1178633717752686. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Sexually Transmitted Infections in Developing Countries. 2023. Available online: http://web.worldbank.org/archive/website01213/WEB/IMAGES/AAGSTIFI.PDF (accessed on 19 December 2024).
- Sullivan, P.S.; Hanson, D.L.; Chu, S.Y.; Jones, J.L.; Ward, J.W. Epidemiology of anemia in human immunodeficiency virus (HIV)-infected persons: Results from the multistate adult and adolescent spectrum of HIV disease surveillance project. Blood 1998, 91, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Adapen, C.; Réot, L.; Menu, E. Role of the human vaginal microbiota in the regulation of inflammation and sexually transmitted infection acquisition: Contribution of the non-human primate model to a better understanding? Front. Reprod. Health 2022, 4, 992176. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Leutscher, P.D.; Ramarokoto, C.E.; Hoffmann, S.; Jensen, J.S.; Ramaniraka, V.; Randrianasolo, B.; Raharisolo, C.; Migliani, R.; Christensen, N. Coexistence of urogenital schistosomiasis and sexually transmitted infection in women and men living in an area where Schistosoma haematobium is endemic. Clin. Infect. Dis. 2008, 47, 775–782. [Google Scholar] [CrossRef]
- Gruninger, S.K.; Rasamoelina, T.R.; Rakotoarivelo, R.A.; Razafindrakoto, A.R.; Rasolojaona, Z.T.; Rakotozafy, R.M.; Soloniaina, P.R.; Rakotozandrindrainy, N.; Rausche, P.; Doumbia, C.O.; et al. Prevalence and risk distribution of schistosomiasis among adults in Madagascar: A cross-sectional study. Infect. Dis. Poverty 2023, 12, 44. [Google Scholar] [CrossRef]
- Rollinson, D.; Knopp, S.; Levitz, S.; Stothard, J.R.; Tchuem Tchuenté, L.A.; Garba, A.; Mohammed, K.A.; Schur, N.; Person, B.; Colley, D.G.; et al. Time to set the agenda for schistosomiasis elimination. Acta Trop. 2013, 128, 423–440. [Google Scholar] [CrossRef]
- Hotez, P.J.; Engels, D.; Gyapong, M.; Ducker, C.; Malecela, M.N. Female genital schistosomiasis. N. Engl. J. Med. 2019, 381, 2493–2495. [Google Scholar] [CrossRef]
- Patel, P.; Rose, C.E.; Kjetland, E.F.; Downs, J.A.; Mbabazi, P.S.; Sabin, K.; Chege, W.; Watts, D.H.; Secor, W.E. Association of schistosomiasis and HIV infections: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 102, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Kutz, J.M.; Rausche, P.; Rasamoelina, T.; Ratefiarisoa, S.; Razafindrakoto, R.; Klein, P.; Jaeger, A.; Rakotomalala, R.S.; Rakotomalala, Z.; Randrianasolo, B.S.; et al. Female genital schistosomiasis, human papilloma virus infection, and cervical cancer in rural Madagascar: A cross sectional study. Infect. Dis. Poverty 2023, 12, 89. [Google Scholar] [CrossRef] [PubMed]
- Mazigo, H.D.; Samson, A.; Lambert, V.J.; Kosia, A.L.; Ngoma, D.D.; Murphy, R.; Matungwa, D.J. “We know about schistosomiasis but we know nothing about FGS”: A qualitative assessment of knowledge gaps about female genital schistosomiasis among communities living in Schistosoma haematobium endemic districts of Zanzibar and northwestern Tanzania. PLoS Negl. Trop. Dis. 2021, 15, e0009789. [Google Scholar] [CrossRef] [PubMed]
- Rausche, P.; Rakotoarivelo, R.A.; Rakotozandrindrainy, R.; Rakotomalala, R.S.; Ratefiarisoa, S.; Rasamoelina, T.; Kutz, J.-M.; Jaeger, A.; Hoeppner, Y.; Lorenz, E.; et al. Awareness and knowledge of female genital schistosomiasis in a population with high endemicity: A cross-sectional study in Madagascar. Front. Microbiol. 2023, 14, 1278974. [Google Scholar] [CrossRef]
- Angora, E.K.; Boissier, J.; Menan, H.; Rey, O.; Tuo, K.; Touré, A.O.; Coulibaly, J.T.; Méité, A.; Raso, G.; N’Goran, E.K.; et al. Prevalence and Risk Factors for Schistosomiasis among Schoolchildren in two Settings of Côte d’Ivoire. Trop. Med. Infect. Dis. 2019, 4, 110. [Google Scholar] [CrossRef]
- Huang, Q.; Gurarie, D.; Ndeffo-Mbah, M.; Li, E.; King, C.H. Schistosoma Transmission in a Dynamic Seasonal Environment and its Impact on the Effectiveness of Disease Control. J. Infect. Dis. 2022, 225, 1050–1061. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rakotomamonjy, L.; Andréambeloson, T.; Randriamihaja, M.; Ihantamalala, F.; Cordier, L.; Cowley, G.; Finnegan, K.; Hanitriniaina, F.; Miller, A.C.; Marovavy, L.; et al. Healthcare Access in Rural Madagascar: A Study of Barriers in the Tsimihety Region. Health Policy Plan. 2020, 35, 134–141. [Google Scholar]

{kind=link}
{kind=link}
| Variables | Anemia | BMI | Education | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | Hb < 12 | Hb ≥ 12 | Underweight (<18.5) | Normal (18.5–24.9) | Over-Weight (25–29.9) | Obese (30–34.9) | Extremely Obese (>35) | NON | CEPE | BEPC + BACC | LICENCE/M2 | No Data | |
| Total | 159 (100.0) | 105 (66.0) | 54 (34.0) | 35 (22.0) | 86 (54.1) | 31 (19.5) | 6 (3.8) | 1 (0.6) | 30 (18.9) | 67 (42.1) | 50 (31.4) | 11 (6.9) | 1 (0.6) |
| STIs | 50 (31.5) | 30 (28.6) | 20 (37.0) | 14 (40.0) | 21 (24.4) | 10 (32.3) | 4 (66.7) | 1 (100.0) | 8 (26.7) | 25 (37.3) | 13 (26.0) | 3 (27.3) | 1 (100.0) |
| Trichomonas vaginalis | 14 (8.8) | 10 (9.5) | 4 (7.4) | 4 (11.4) | 5 (5.8) | 4 (12.9) | 1 (16.7) | 0 (0.0) | 2 (6.7) | 5 (7.5) | 6 (12.0) | 0 (0.0) | 1 (100.0) |
| Treponema pallidum | 12 (7.6) | 8 (7.6) | 5 (7.4) | 8 (22.9) | 3 (3.5) | 0 (0.0) | 1 (16.7) | 0 (0.0) | 5 (16.7) | 6 (9.0) | 0 (0.0) | 1 (9.1) | 0 (0.0) |
| Neisseria gonorrhoeae | 32 (20.1) | 17 (16.2) | 15 (27.8) | 6 (17.1) | 16 (18.6) | 7 (22.6) | 2 (33.3) | 1 (100.0) | 3 (10.0) | 19 (28.4) | 8 (16.0) | 2 (18.2) | 0 (0.0) |
| HIV | 1 (0.6) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.0) | 0 (0.0) | 0 (0.0) |
| Schistosoma haematobium | 28 (17.6) | 19 (18.1) | 9 (16.7) | 5 (14.3) | 17 (19.8) | 5 (16.1) | 1 (16.7) | 0 (0.0) | 12 (40.0) | 13 (19.4) | 3 (6.0) | 0 (0.0) | 0 (0.0) |
| Co-infections | 12 (7.6) | 8 (7.6) | 4 (7.4) | 4 (11.4) | 5 (5.8) | 2 (6.5) | 1 (16.7) | 0 (0.0) | 4 (13.3) | 5 (7.5) | 3 (6.0) | 0 (0.0) | 0 (0.0) |
| S. haematobium + T. vaginalis | 2 (1.2) | 1 (0.9) | 1 (1.9) | 0 (0.0) | 1 (1.2) | 1 (3.2) | 0 (0.0) | 0 (0.0) | 1 (3.3) | 0 (0.0) | 1 (2.0) | 0 (0.0) | 0 (0.0) |
| S. haematobium + T. vaginalis + N. gonorrhoeae | 1 (0.6) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (1.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| S. haematobium + T. pallidum | 2 (0.6) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (16.7) | 0 (0.0) | 1 (3.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| S. haematobium + T. pallidum + N. gonorrhoeae | 3 (0.6) | 0 (0.0) | 1 (1.9) | 0 (0.0) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| T. vaginalis + N. gonorrhoeae | 2 (1.2) | 2 (1.9) | 0 (0.0) | 0 (0.0) | 1 (1.2) | 1 (3.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (4.0) | 0 (0.0) | 0 (0.0) |
| T. pallidum + N. gonorrhoeae | 5 (3.1) | 3 (2.9) | 2 (3.7) | 4 (11.4) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.3) | 4 (6.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Variables | Total (n = 159) | STIs (−) (n = 109) | STIs (+) (n = 50) | p-Value | S. haematobium (−) (n = 131) | S. haematobium (+) (n = 28) | p-Value |
|---|---|---|---|---|---|---|---|
| Age | 0.959 1 | 0.889 1 | |||||
| Range | 15–80 | 15–71 | 18–80 | 16–80 | 15–71 | ||
| Median | 34 | 34 | 34 | 34 | 33.5 | ||
| 95%Cl | [35.1–39.3] | [34.6–39.6 | [33.6–41.5] | [35.0–39.5] | [31.8–42.8] | ||
| BMI | 0.840 1 | 0.791 1 | |||||
| Range | 14.4–38.2 | 15.9–34.1 | 14.4–38.2 | 14.4–38.2 | 16.1–33.0 | ||
| Median | 21.3 | 21.3 | 21.4 | 21.6 | 25.8 | ||
| 95%Cl | [21.3–22.7] | [21.1–22.5] | [20.9–24.0] | [21.2–22.8] | [20.6–23.4] | ||
| HGB | 0.575 1 | 0.867 1 | |||||
| Range | 5.5–15.1 | 5.7–14.8 | 5.5–2 | 5.5–2 | 8.7–12.9 | ||
| Median | 11.5 | 11.4 | 11.7 | 11.5 | 11.4 | ||
| 95%Cl | [11.1–11.5] | [11.0–11.6] | [10.8–11.8] | [11.0–11.6] | [10.9–11.7] | ||
| HTC | 0.271 1 | 0.566 1 | |||||
| Range | 20.6–46.0 | 21.2–46.0 | 20.6–45.7 | 20.6–46 | 27.6–41.3 | ||
| Median | 36.5 | 36.4 | 37.15 | 36.9 | 36.3 | ||
| 95%Cl | [35.5–36.9] | [35.3–36.8] | [35.0–37.8] | [35.4–37.0] | [34.9–37.2] | ||
| WBC | 0.012 1 | 0.269 1 | |||||
| Range | 2.2–13.5 | 2.2–13.5 | 2.3–12 | 2.2–13.5 | 3.6–11.2 | ||
| Median | 5.6 | 5.3 | 6.3 | 5.6 | 5.9 | ||
| 95%Cl | [5.7–6.3] | [5.4–6.1] | [5.9–7.0] | [5.6–6.3] | [5.6–6.9] | ||
| RBC | 0.845 2 | 0.636 2 | |||||
| Mean (SD) | 4.4 | 4.4 | 4.4 | 4.4 | 4.4 | ||
| Range | 2.8–5.6 | 2.8–5.5 | 3.2–5.6 | 2.8–5.6 | 3.4–5.0 | ||
| 95%Cl | [4.3–4.5] | [4.3–4.5] | [4.3–4.5] | [4.3–4.5] | [4.2–4.5] | ||
| MCV | 0.668 1 | 0.844 1 | |||||
| Range | 51.8–95.9 | 51.8–93.5 | 58–95.9 | 51.8–95.9 | 66.9–93.5 | ||
| Median | 82.9 | 83.2 | 82.5 | 83.3 | 82.4 | ||
| 95%Cl | [81.0–83.3] | [80.6–83.4] | [80.5–84.7] | [80.7–83.4] | [80.5–85.1] | ||
| MCH | 0.881 1 | 0.707 1 | |||||
| Range | 13.9–30.3 | 13.9–30.1 | 15.4–30.3 | 13.0–30.3 | 19.9–29.7 | ||
| Median | 25.8 | 25.9 | 25.8 | 25.9 | 25.6 | ||
| 95%Cl | [25.1–26.0] | [25.0–26.1] | [24.7–26.4] | [25.0–26.0] | [25.1–26.7] | ||
| MCHC | 0.237 1 | 0.228 1 | |||||
| Range | 26.5–31.4 | 26.5–32.9 | 26.6–32.8 | 26.5–32.9 | 29.7–32.4 | ||
| Median | 31.2 | 31.3 | 31.1 | 31.2 | 31.5 | ||
| 95%Cl | [31.0–31.3] | [31.0–31.4] | [30.6–31.2] | [30.9–31.2] | [31.1–31.6] | ||
| PLT | 0.179 2 | 0.108 2 | |||||
| Mean (SD) | 248.2 | 246.8 | 262.2 | 255.6 | 233.3 | ||
| Range | 107–490 | 109–372 | 107–490 | 107–490 | 109–372 | ||
| 95%Cl | 241.3–262.0] | [235.0–258.6] | [241.5–282.8] | [244.2–266.9] | [208.1–258.4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasprowicz, D.; Wilczyńska, W.; Korzeniewski, K. Health Status of Tsimihety Women: Sexually Transmitted Infections and Schistosomiasis, Northern Madagascar. J. Clin. Med. 2025, 14, 3479. https://doi.org/10.3390/jcm14103479
Kasprowicz D, Wilczyńska W, Korzeniewski K. Health Status of Tsimihety Women: Sexually Transmitted Infections and Schistosomiasis, Northern Madagascar. Journal of Clinical Medicine. 2025; 14(10):3479. https://doi.org/10.3390/jcm14103479
Chicago/Turabian StyleKasprowicz, Daniel, Wanesa Wilczyńska, and Krzysztof Korzeniewski. 2025. "Health Status of Tsimihety Women: Sexually Transmitted Infections and Schistosomiasis, Northern Madagascar" Journal of Clinical Medicine 14, no. 10: 3479. https://doi.org/10.3390/jcm14103479
APA StyleKasprowicz, D., Wilczyńska, W., & Korzeniewski, K. (2025). Health Status of Tsimihety Women: Sexually Transmitted Infections and Schistosomiasis, Northern Madagascar. Journal of Clinical Medicine, 14(10), 3479. https://doi.org/10.3390/jcm14103479