
Impact of the COVID-19 Pandemic on the Everyday Life and Healthcare of Patients with Congenital Heart Defects: Insights from Pandemic Onset to One Year Later
 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Cohort
2.2. National Register for Congenital Heart Defects
2.3. Statistical Analyses
3. Results
3.1. Study Cohort/Patient Characteristics
3.2. Medical and Disease-Related Patient Data
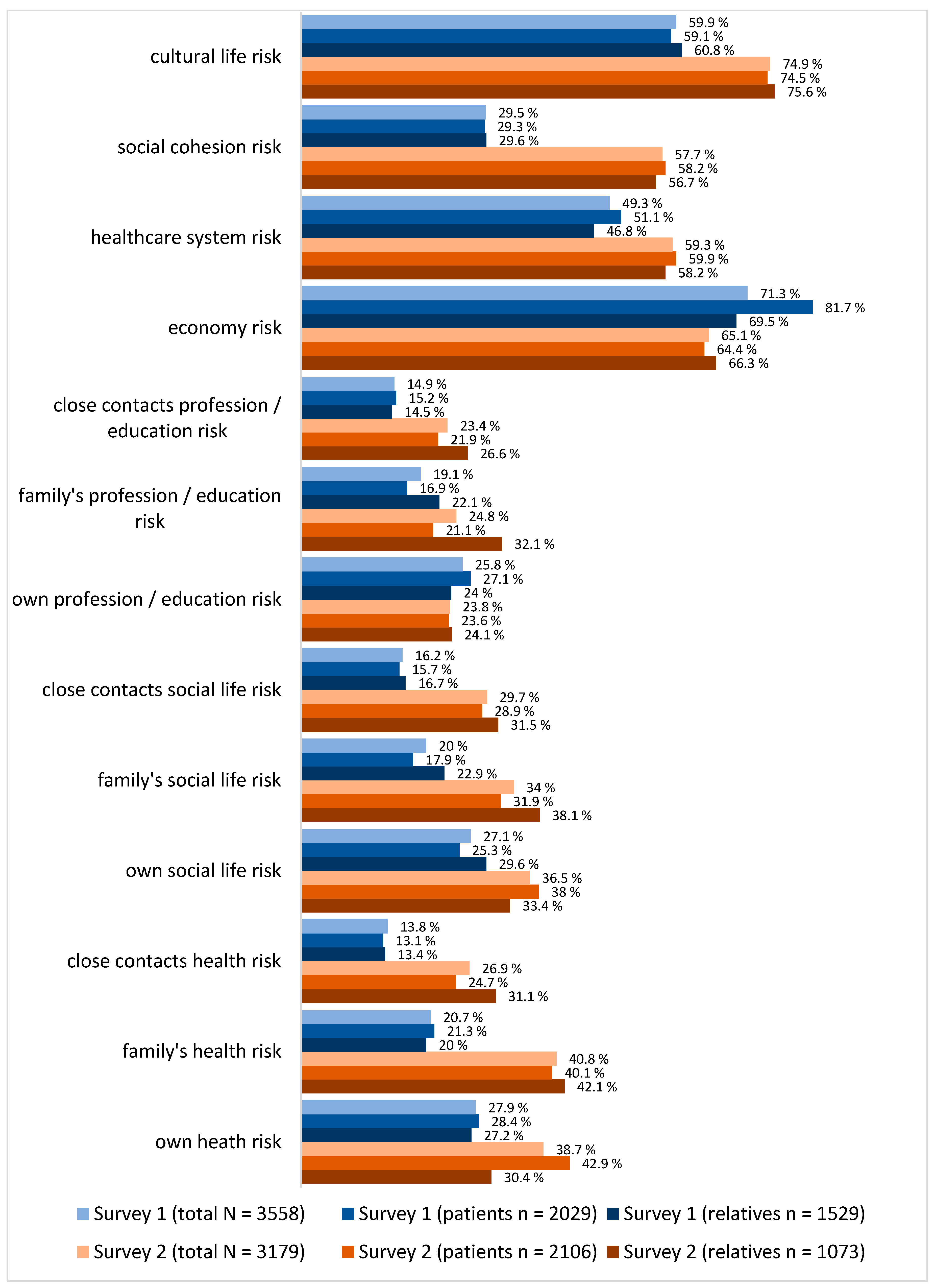
3.3. Risk Perception
3.4. COVID-19-Related Knowledge
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaye, A.D.; Okeagu, C.N.; Pham, A.D.; Silva, R.A.; Hurley, J.J.; Arron, B.L.; Sarfraz, N.; Lee, H.N.; Ghali, G.E.; Gamble, J.W.; et al. Economic impact of COVID-19 pandemic on healthcare facilities and systems: International perspectives. Best. Pract. Res. Clin. Anaesthesiol. 2021, 35, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Legido-Quigley, H.; Asgari, N.; Teo, Y.Y.; Leung, G.M.; Oshitani, H.; Fukuda, K.; Cook, A.R.; Hsu, L.Y.; Shibuya, K.; Heymann, D. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet 2020, 395, 848–850. [Google Scholar] [CrossRef]
- Schilling, J.; Tolksdorf, K.; Marquis, A.; Faber, M.; Pfoch, T.; Buda, S.; Haas, W.; Schuler, E.; Altmann, D.; Grote, U.; et al. [The different periods of COVID-19 in Germany: A descriptive analysis from January 2020 to February 2021]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 1093–1106. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel. Med. 2020, 27, taaa020. [Google Scholar] [CrossRef]
- Kim, H.H.; Jung, J.H. Social Isolation and Psychological Distress During the COVID-19 Pandemic: A Cross-National Analysis. Gerontologist 2021, 61, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Mangiapane, S.; Zhu, L.; Kretschmann, J.; Czihal, T.; von Stillfried, D. Veränderung der Vertragsärztlichen Leistungsinanspruchnahme Während der COVID-Krise; Zentralinstitut für die kassenärztliche Versorgung in der Bundesrepublik Deutschland: Berlin, Germany, 2021. [Google Scholar]
- Günster, C.; Drogan, D.; Hentschker, C.; Klauber, J.; Malzahn, J.; Schillinger, G.; Mostert, C. WIdO-Report: Entwicklung der Krankenhausfallzahlen Während des Coronavirus-Lockdowns. Nach ICD-Diagnosekapiteln und Ausgewählten Behandlungsanlässen; Wissenschaftlichen Institut der AOK: Berlin, Germany, 2020. [Google Scholar]
- Xu, S.; Glenn, S.; Sy, L.; Qian, L.; Hong, V.; Ryan, D.S.; Jacobsen, S. Impact of the COVID-19 Pandemic on Health Care Utilization in a Large Integrated Health Care System: Retrospective Cohort Study. J. Med. Internet Res. 2021, 23, e26558. [Google Scholar] [CrossRef]
- Schafer, I.; Haack, A.; Neumann, M.; Koch-Gromus, U.; Scherer, M.; Petersen, E. [Non-utilisation of medical services during the COVID-19 pandemic among persons with chronic diseases]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2023, 66, 275–282. [Google Scholar] [CrossRef]
- Hacker, K.A.; Briss, P.A.; Richardson, L.; Wright, J.; Petersen, R. COVID-19 and Chronic Disease: The Impact Now and in the Future. Prev. Chronic Dis. 2021, 18, E62. [Google Scholar] [CrossRef]
- Heidemann, C.; Reitzle, L.; Schmidt, C.; Fuchs, J.; Prutz, F.; Scheidt-Nave, C. Non-utilisation of health care services during the COVID-19 pandemic: Results of the CoMoLo study. J. Health Monit. 2022, 7, 2–17. [Google Scholar] [CrossRef]
- König, S.; Ueberham, L.; Pellissier, V.; Hohenstein, S.; Meier-Hellmann, A.; Thiele, H.; Ahmadli, V.; Borger, M.A.; Kuhlen, R.; Hindricks, G.; et al. Hospitalization deficit of in- and outpatient cases with cardiovascular diseases and utilization of cardiological interventions during the COVID-19 pandemic: Insights from the German-wide helios hospital network. Clin. Cardiol. 2021, 44, 392–400. [Google Scholar] [CrossRef]
- Cousino, M.K.; Pasquali, S.K.; Romano, J.C.; Norris, M.D.; Yu, S.; Reichle, G.; Lowery, R.; Viers, S.; Schumacher, K.R. Impact of the COVID-19 pandemic on CHD care and emotional wellbeing. Cardiol. Young 2021, 31, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Warnes, C.A.; Williams, R.G.; Bashore, T.M.; Child, J.S.; Connolly, H.M.; Dearani, J.A.; Del Nido, P.; Fasules, J.W.; Graham, T.P., Jr.; Hijazi, Z.M.; et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2008, 52, e143–e263. [Google Scholar] [CrossRef]
- COSMO—COVID-19 Snapshot Monitoring. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/ (accessed on 26 May 2024).
- Bauer, U.; Niggemeyer, E.; Lange, P.E. [The competence network for congenital heart defects. Networking instead of isolated efforts for optimized research and care]. Med. Klin. 2006, 101, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Kompetenznetz-AHF. Das Nationale Register für angeborene Herzfehler 2023. Available online: https://www.kompetenznetz-ahf.de/wir/register/. (accessed on 11 March 2024).
- Helm, P.C.; Koerten, M.A.; Abdul-Khaliq, H.; Baumgartner, H.; Kececioglu, D.; Bauer, U.M. Representativeness of the German National Register for Congenital Heart Defects: A clinically oriented analysis. Cardiol. Young 2016, 26, 921–926. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef]
- Bender, R.; Lange, S. Adjusting for multiple testing--when and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef]
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef]
- Perneger, T.V. What’s wrong with Bonferroni adjustments. BMJ 1998, 316, 1236–1238. [Google Scholar] [CrossRef] [PubMed]
- Seidel, L.; Nebel, K.; Achenbach, S.; Bauer, U.; Ewert, P.; Freilinger, S.; Gundlach, U.; Kaemmerer, H.; Nagdyman, N.; Oberhoffer, R.; et al. Facts about the General Medical Care of Adults with Congenital Heart Defects: Experience of a Tertiary Care Center. J. Clin. Med. 2020, 9, 1943. [Google Scholar] [CrossRef]
- Salanti, G.; Peter, N.; Tonia, T.; Holloway, A.; White, I.R.; Darwish, L.; Low, N.; Egger, M.; Haas, A.D.; Fazel, S.; et al. The Impact of the COVID-19 Pandemic and Associated Control Measures on the Mental Health of the General Population: A Systematic Review and Dose-Response Meta-analysis. Ann. Intern. Med. 2022, 175, 1560–1571. [Google Scholar] [CrossRef]
- Ahmed, I.; Tegenu, K.; Tilahun, D.; Awel, S. Health-related quality of life among patients with chronic diseases during COVID-19 pandemic: A cross-sectional study. Pan Afr. Med. J. 2022, 43, 2. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease 2019 (COVID-19) Daily Situation Report of the Robert Koch Institute. Available online: https://www.rki.de/DE/Themen/Infektionskrankheiten/Infektionskrankheiten-A-Z/C/COVID-19-Pandemie/Situationsberichte/Maerz-Aug_2020/2020-04-28-en.pdf?__blob=publicationFile&v=1 (accessed on 26 May 2024).
- Täglicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). Available online: https://www.rki.de/DE/Themen/Infektionskrankheiten/Infektionskrankheiten-A-Z/C/COVID-19-Pandemie/Situationsberichte/April_2021/2021-04-30-de.pdf?__blob=publicationFile&v=1 (accessed on 26 May 2024).
- Robinson, E.; Daly, M. Explaining the rise and fall of psychological distress during the COVID-19 crisis in the United States: Longitudinal evidence from the Understanding America Study. Br. J. Health Psychol. 2021, 26, 570–587. [Google Scholar] [CrossRef]
- Ganesan, B.; Al-Jumaily, A.; Fong, K.N.K.; Prasad, P.; Meena, S.K.; Tong, R.K. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak Quarantine, Isolation, and Lockdown Policies on Mental Health and Suicide. Front. Psychiatry 2021, 12, 565190. [Google Scholar] [CrossRef]
- Zum gesellschaftlichen Umgang mit der Corona-Pandemie—Ergebnisse der Mannheimer Corona-Studie. Available online: https://www.bpb.de/shop/zeitschriften/apuz/314345/zum-gesellschaftlichen-umgang-mit-der-corona-pandemie/ (accessed on 26 May 2024).
- Zomer, A.C.; Vaartjes, I.; Uiterwaal, C.S.; van der Velde, E.T.; Sieswerda, G.J.; Wajon, E.M.; Plomp, K.; van Bergen, P.F.; Verheugt, C.L.; Krivka, E.; et al. Social burden and lifestyle in adults with congenital heart disease. Am. J. Cardiol. 2012, 109, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Die Folgen der Corona-Pandemie in 10 Zahlen. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2021/03/PD21_N023_p001.html (accessed on 26 May 2024).
- Mata, J.; Wenz, A.; Rettig, T.; Reifenscheid, M.; Mohring, K.; Krieger, U.; Friedel, S.; Fikel, M.; Cornesse, C.; Blom, A.G.; et al. Health behaviors and mental health during the COVID-19 pandemic: A longitudinal population-based survey in Germany. Soc. Sci. Med. 2021, 287, 114333. [Google Scholar] [CrossRef] [PubMed]
- Kroll, C.; McQueen, A.; De La Vega, V.; Marsh, A.K.; Poor, T.; Verdecias, N.; Caburnay, C.; Kreuter, M.W. Trusted sources for COVID-19 testing and vaccination: Lessons for future health communication. J. Commun. Healthc. 2023, 16, 350–357. [Google Scholar] [CrossRef]
- Finset, A.; Bosworth, H.; Butow, P.; Gulbrandsen, P.; Hulsman, R.L.; Pieterse, A.H.; Street, R.; Tschoetschel, R.; van Weert, J. Effective health communication—A key factor in fighting the COVID-19 pandemic. Patient Educ. Couns. 2020, 103, 873–876. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Gallinoro, V.; Guida, A.; Morittu, C.; Ferro Allodola, V.; Lastrucci, V.; Zanobini, P.; Okan, O.; Dadaczynski, K.; Lorini, C. Digital Health Literacy and Information-Seeking in the Era of COVID-19: Gender Differences Emerged from a Florentine University Experience. Int. J. Environ. Res. Public Health 2023, 20, 2611. [Google Scholar] [CrossRef]

{kind=link}
| Survey 1 (April 2020) | Survey 2 (April 2021) | ||||||
|---|---|---|---|---|---|---|---|
| Total N = 3558 | Male n = 1670 * | Female n = 1886 * | Total N = 3179 | Male n = 1505 ** | Female n = 1674 ** | ||
| Participants | Patient | 57% a | 48.7% d | 64.4% d | 66.2% a | 60.7% d | 71.3% d |
| Relative | 43% a | 51.3% d | 35.6% d | 33.8% a | 39.3% d | 28.7% d | |
| Patient age in years (mean ± SD) | 23.7 ± 15.4 a | 22.4 ± 16 d | 24.7 ± 14.9 d | 26 ± 16.1 a | 25.6 ± 16.9 | 26.4 ± 15.3 | |
| Federal state | Old federal states | 69.6% | 70.6% | 68.7% | 68.0% | 68.1% | 68.0% |
| New federal states | 28.9% | 28.1% | 29.6% | 30.9% | 30.8% | 30.9% | |
| Unknown/Foreign country | 1.5% | 1.3% | 1.7% | 1.1% | 1.1% | 1.1% | |
| Residence size | 5000 inhabitants or less | 31.1% a | 31.3% | 31.2% | 22.1% a | 21.5% | 22.5% |
| 5001–20,000 inhabitants | 21.4% a | 21.3% | 21.4% | 25.8% a | 26.4% | 25.3% | |
| 20,001–100,000 inhabitants | 18.8% a | 18.4% | 19.2% | 21.2% a | 20.8% | 21.6% | |
| More than 100,000 inhabitants | 28.4% a | 28.8% | 28.0% | 30.9% a | 31.3% | 30.6% | |
| I do not know | 0.2% a | 0.2% | 0.2% | - | - | - | |
| Highest educational qualification | I don’t go to school yet | 14.8% a | 17.2% d | 12.7% d | 11.0% a | 12. 9% d | 9.3% d |
| Finished school without a degree | 2.0% a | 2.2% d | 1.9% d | 1.8% a | 2.0% d | 1.6% d | |
| Still go to school | 23.9% a | 28.4% d | 20.0% d | 21.5% a | 23. 7% d | 19.6% d | |
| Secondary school certificate A | 3.0% a | 3.1% d | 2.9% d | 2.7% a | 2.9% d | 2.6% d | |
| Secondary school certificate B | 7.8% a | 6.8% d | 8.6% d | 8.6% a | 6.8% d | 10.2% d | |
| Completed apprenticeship | 11.2% a | 8.7% d | 13.4% d | 12.8% a | 12.0% d | 13.5% d | |
| Advanced technical college entrance qualification | 5.6% a | 5.1% d | 6.0% d | 6.4% a | 5.5% d | 7.2% d | |
| High school diploma | 11.0% a | 9.5% d | 12.5% d | 11.7% a | 11.3% d | 12.1% d | |
| Technical/university degree | 17.0% a | 16.2% d | 17.8% d | 18.8% a | 18.1% d | 19.4% d | |
| Another degree | 3.6% a | 2.8% d | 4.2% d | 4.7% a | 4.9% d | 4.6% d | |
| Occupation | I don’t go to school yet | 13.4% | 15.8% | 11.2% | 9.2% | 10.2% | 8.3% |
| Still go to school | 28.0% | 32.6% | 23.9% | 26.0% | 28.6% | 23.6% | |
| I am a trainee | 4.8% | 4.0% | 5.5% | 5.4% | 4.4% | 6.3% | |
| I am a student | 8.2% | 6.9% | 9.4% | 8.6% | 8.0% | 9.1% | |
| I am employed part-time | 8.4% | 2.9% | 13.4% | 8.4% | 3.5% | 12.8% | |
| I am employed full-time | 24.9% | 28.3% | 22.0% | 27.1% | 31.2% | 23.4% | |
| I am looking for work | 1.6% | 1.3% | 2.0% | 2.2% | 2.1% | 2.3% | |
| I am self-employed | 1.5% | 1.4% | 1.6% | 1.9% | 1.6% | 2.1% | |
| I am a pensioner | 4.0% | 3.5% | 4.5% | 5.8% | 6.1% | 5.4% | |
| Other | 5.0% | 3.4% | 6.5% | 5.5% | 4.1% | 6.7% | |
| Survey 1 (April 2020) | Survey 2 (April 2021) | ||||||
|---|---|---|---|---|---|---|---|
| Total N = 3558 | Male n = 1670 * | Female n = 1886 * | Total N = 3179 | Male n = 1505 ** | Female n = 1674 ** | ||
| Severity of the congenital heart defect | |||||||
| Simple CHD | 25.8% a | 20.4% d | 30.6% d | 14.2% a | 10.6% d | 17.5% d | |
| Moderate CHD | 36.3% a | 37.7% d | 35.1% d | 39.1% a | 37.6% d | 40.5% d | |
| Complex CHD | 30.5% a | 34.3% d | 27.1% d | 37.7% a | 43.5% d | 32.5% d | |
| Unclassified/unknown CHD | 7.4% a | 7.6% d | 7.2% d | 8.9% a | 8.3% d | 9.5% d | |
| Have you been to the doctor since the start of the COVID-19 pandemic? MA | |||||||
| Cardiologists/pediatric cardiologists (practice) | 24.4% a | 27.2% d | 21.8% d | 39.8% a | 42.6% e | 37.2% e | |
| Cardiologists/pediatric cardiologists (clinic/heart center) | 23.1% a | 24.5% | 21.9% | 46.6% a | 47% | 46.2% | |
| Yes, with another doctor | 54.8% a | 52.6% f | 56.7% f | 65.8% a | 63.6% f | 67.8% f | |
| No | 22.7% a | 22.8% | 22.6% | 6.9% a | 6.7% | 7% | |
| Already hospitalized for AHF since the beginning of the pandemic (cardiac catheterization/surgery) | 5% a | 5.3% | 4.7% | 14.3% a | 16.1% e | 12.7% e | |
| Doctor’s appointment/check-up with pediatric cardiologist, cardiologist, heart clinic or hospital itself cancelled due to COVID-19 | 8.0% c | 7.9% | 8.1% | 9.6% c | 8.7% | 10.3% | |
| Cardiac catheter treatment cancelled even due to COVID-19 | 0.4% c | 0.5% | 0.2% | 0.2% c | 1.1% | 0.6% | |
| Operation itself cancelled due to COVID-19 | 0.6% | 1.0% f | 0.3% f | 0.9% | 1.0% | 0.9% | |
| Doctor’s appointment/check-up with pediatric cardiologist, cardiologist, heart clinic or hospital cancelled by doctor due to COVID-19 | 9.7% | 9.9% | 9.5% | 9.9% | 9.3% | 10.5% | |
| Cardiac catheter treatment cancelled by doctor due to COVID-19 | 0.7% | 0.7% | 0.7% | 1.0% | 1.3% | 0.8% | |
| Surgery cancelled by doctor due to COVID-19 | 1.2% | 1.3% | 1.1% | 1.6% | 1.7% | 1.6% | |
| If you have seen a doctor since the start of the COVID-19 pandemic, did the doctor talk to you/your parents about COVID-19 on their own initiative or did you or your parents ask about it? | |||||||
| Not been to the doctor since the start of the pandemic | 22.7% a | 22.8% | 22.6% | 6.9% a | 6.7% f | 7.0% f | |
| Approached (without asking) | 7.8% a | 7.5% | 8.1% | 17.8% a | 18.3% f | 17.3% f | |
| Received information material (without asking) | 0.8% a | 0.7% | 0.8% | 1.7% a | 2.1% f | 1.3% f | |
| Approached + information material (without asking) | 1.5% a | 1.7% | 1.4% | 3.4% a | 3.7% f | 3.2% f | |
| Conversation (upon request) | 15.5% a | 16.8% | 14.4% | 27.6% a | 28.8% f | 26.5% f | |
| Information material (upon request) | 0.6% a | 0.5% | 0.6% | 1.2% a | 1.5% f | 1.0% f | |
| Conversation + information material (upon request) | 0.8% a | 0.9% | 0.6% | 2.5% a | 1.9% f | 3.0% f | |
| No | 50.4% a | 49.1% | 51.4% | 39.0% a | 37.0% f | 40.7% f | |
| Did you or your parents call your doctor because you or your parents wanted to know something about COVID-19 and your heart defect? | 21.6% a | 21.8% | 21.3% | 30.0% a | 29. 7% | 30.3% | |
| Was your doctor able to answer the questions about COVID-19 and your heart defect? | |||||||
| Yes | 25.2% a | 25.6% | 24.8% | 46.3% a | 49.6% e | 43.4% e | |
| No | 8.9% a | 9.1% | 8.7% | 8.5% a | 7.7% e | 9.1% e | |
| Not yet spoken to the doctor about COVID-19 | 65.9% a | 65.3% | 66.5% | 45.2% a | 42.7% e | 47.5% e | |
| Have you ever called a hotline/health authority about COVID-19? | |||||||
| Yes, I called and got through to someone | 6.4% a | 6.8% | 6.0% | 21.1% a | 21.1% | 21.1% | |
| Yes. I called but never reached anyone | 2.0% a | 1.6% | 2.3% | 3.7% a | 3.7% | 3.8% | |
| No. I did not call | 91.6% a | 91.6% | 91.6% | 75.1% a | 75.3% | 75.0% | |
| Have you been vaccinated against the flu? | |||||||
| Yes | 50.9% a | 52.9% e | 49.2% e | 58.5% a | 61.1% e | 56.2% e | |
| No | 46.7% a | 44.0% e | 49.0% e | 39.4% a | 36.4% e | 42.2% e | |
| I do not know | 2.4% a | 3.1% e | 1.9% e | 2.0% a | 2.5% e | 1.7% e | |
| Have you been vaccinated against pneumococcus? | |||||||
| Yes | 53.7% c | 54.9% | 52.6% | 54.3% c | 55.4% | 53.3% | |
| No | 28.7% c | 27.1% | 30.0% | 25.9% c | 24.9% | 26.8% | |
| I do not know | 17.7% c | 18.0% | 17.4% | 19.8% c | 19.7% | 19.8% | |
| Was COVID-19 the reason for the flu/pneumococcal vaccination/s? | |||||||
| Yes, COVID-19 was the reason | 4.9% a | 4.7% f | 5.0% f | 9.7% a | 7.7% d | 11.5% d | |
| No, COVID-19 was not the reason | 62.5% a | 64.2% f | 61.0% f | 61.4% a | 64.8% d | 58.4% d | |
| No, I was not vaccinated | 28.6% a | 26.5% f | 30.4% f | 23.2% a | 21.8% d | 24.6% d | |
| I do not know | 4.0% a | 4.6% f | 3.6% f | 5.6% a | 5.7% d | 5.6% d | |
| Were there COVID-19 cases with family/acquaintances | 12.3% a | 11.8% | 12.7% | 63.5% a | 60.9% e | 65.9% e | |
| I was infected with COVID-19 at least once | 0.4% a | 0.5% | 0.3% | 4.2% a | 3.9% | 4.4% | |
| Survey 1 (April 2020) | Survey 2 (April 2021) | ||||||
|---|---|---|---|---|---|---|---|
| Total N = 3558 | Patients n = 2029 | Relatives n = 1529 | Total N = 3179 | Patients n = 2106 | Relatives n = 1073 | ||
| I know what coronavirus is. | 6.4 ± 1.0 a | 6.5 ± 0.8 d | 6.3 ± 1.2 d | 6.3 ± 0.9 a | 6.3 ± 0.9 | 6.3 ± 1.0 | |
| I am well informed about coronavirus. | 6.2 ± 1.0 a | 6.2 ± 0.9 | 6.1 ± 1.1 | 5.9 ± 1.0 a | 5.9 ± 1.1 d | 6.0 ± 1.0 d | |
| I understand the media coverage (internet/TV/radio/newspaper) about coronavirus. | 6.1 ± 1.2 a | 6.4 ± 0.9 d | 6.0 ± 1.4 d | 5.8 ± 1.3 a | 5.8 ± 1.3 | 5.8 ± 1.3 | |
| I trust the official information from the federal government, the federal authorities and the state authorities about coronavirus. | 5.5 ± 1.4 a | 5.6 ± 1.4 d | 5.4 ± 1.5 d | 4.9 ± 1.7 a | 5.0 ± 1.7 f | 4.8 ± 1.7 f | |
| I also find out about coronavirus by sharing information on social networks (Facebook, YouTube, Instagram, WhatsApp, etc.). | 3.9 ± 2.1 a | 3.4 ± 2.1 f | 3.8 ± 2.2 f | 3.3 ± 2.1 a | 3.4 ± 2.1 e | 3.1 ± 2.1 e | |
| I can tell which statements come from trustworthy sources and which are misinformation or “fake news”. | 5.6 ± 1.5 a | 5.8 ± 1.2 d | 5.3 ± 1.7 d | 5.4 ± 1.5 a | 5.6 ± 1.5 d | 5.2 ± 1.7 d | |
| I talk to other people about coronavirus every day. | 5.4 ± 1.7 a | 5.4 ± 1.7 e | 5.3 ± 1.8 e | 5.1 ± 1.7 a | 5.0 ± 1.8 | 5.1 ± 1.9 | |
| I follow the media coverage (internet/TV/radio/newspapers) about coronavirus every day. | 5.6 ± 1.7 a | 5.7 ± 1.6 e | 5.5 ± 1.8 e | 5.0 ± 1.9 a | 4.9 ± 1.9 e | 5.1 ± 1.9 e | |
| I have changed my habits and everyday behavior because of coronavirus. | 5.9 ± 1.4 a | 5.8 ± 1.4 d | 6.0 ± 1.3 d | 5.7 ± 1.5 a | 5.7 ± 1.5 | 5.7 ± 1.5 | |
| I feel restricted in my everyday life by the changes due to coronavirus. | 5.5 ± 1.5 a | 5.4 ± 1.5 d | 5.7 ± 1.4 d | 5.3 ± 1.7 a | 5.2 ± 1.8 | 5.3 ± 1.6 | |
| Coronavirus hasn’t changed my life. | 3.0 ± 2.0 b | 3.01 ± 2.0 | 3.0 ± 2.1 | 2.9 ± 2.0 b | 2.8 ± 2.0 | 2.9 ± 2.1 | |
| I’m worried about coronavirus. | 4.9 ± 1.6 c | 4.8 ± 1.6 d | 5.1 ± 1.6 d | 5.0 ± 1.6 c | 4.9 ± 1.6 d | 5.2 ± 1.6 d | |
| I generally feel well informed about the heart defect by my doctor/my child’s doctor. | 5.4 ± 1.8 c | 5.3 ± 1.8 e | 5.5 ± 1.8 e | 5.3 ± 1.7 c | 5.1 ± 1.8 d | 5.7 ± 1.5 d | |
| I understand what my doctor/my child’s doctor explains to me. | 6.0 ± 1.4 a | 5.9 ± 1.4 d | 6.2 ± 1.3 d | 5.9 ± 1.4 a | 5.7 ± 1.5 d | 6.2 ± 1.1 d | |
| I trust my doctor/my child’s doctor. | 6.2 ± 1.1 a | 6.2 ± 1.2 d | 6.3 ± 1.0 d | 6.0 ± 1.3 a | 5.9 ± 1.4 d | 6.3 ± 1.0 d | |
| I feel uncomfortable when I have to go to the doctor/when my child has to go to the doctor. | 3.4 ± 2.1 a | 3.2 ± 2.1 d | 3.6 ± 2.1 d | 3.0 ± 2.0 a | 3.0 ± 2.0 f | 3.1 ± 2.0 f | |
| I try (with my child) to go to the doctor as rarely as possible. | 4.5 ± 2.1 a | 4.4 ± 2.1 f | 4.6 ± 2.1 f | 3.7 ± 2.2 a | 3.7 ± 2.2 | 3.8 ± 2.2 | |
| I think it is important to be informed about coronavirus by my doctor/my child’s doctor. | 5.1 ± 1.9 b | 5.0 ± 1.9 d | 5.3 ± 1.8 d | 5.2 ± 1.7 b | 5.1 ± 1.8 d | 5.5 ± 1.7 d | |
| If I don’t understand something about the heart defect and/or coronavirus or want to know something, I ask my doctor/my child’s doctor about it. | 5.2 ± 2.0 a | 4.8 ± 2.0 d | 5.7 ± 1.7 d | 5.5 ± 1.8 a | 5.3 ± 1.8 d | 6.0 ± 1.5 d | |
| I feel well informed about coronavirus by my doctor/my child’s doctor. | 4.3 ± 2.1 a | 4.2 ± 2.0 d | 4.5 ± 2.1 d | 4.9 ± 1.8 a | 4.8 ± 1.8 d | 5.3 ± 1.7 d | |
| I’m worried that I’m getting infected with coronavirus. | 4.6 ± 1.8 c | 4.4 ± 1.8 d | 4.7 ± 1.8 d | 4.5 ± 1.8 c | 4.4 ± 1.8 | 4.5 ± 1.9 | |
| I will be infected with coronavirus in the next four weeks. | 2.8 ± 1.4 a | 2.8 ± 1.4 f | 2.7 ± 1.4 f | 2.3 ± 1.3 a | 2.3 ± 1.3 | 2.3 ± 1.3 | |
| I know how I can protect myself from coronavirus infection. | 6.1 ± 1.3 | 6.0 ± 1.3 e | 6.1 ± 1.2 e | 6.1 ± 1.2 | 6.1 ± 1.3 f | 6.2 ± 1.2 f | |
| I understand how coronavirus is spreading. | 6.4 ± 0.9 a | 6.4 ± 0.9 | 6.4 ± 1.0 | 6.3 ± 0.9 a | 6.3 ± 1.0 e | 6.4 ± 0.8 e | |
| I know the symptoms of coronavirus. | 6.3 ± 1.0 a | 6.2 ± 0.9 f | 6.3 ± 1.0 f | 6.2 ± 1.0 a | 6.1 ± 1.0 f | 6.2 ± 0.9 f | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schütte, E.; Nasri, S.O.; Ehmann, A.-L.; Semmler, J.; Berger, F.; Bauer, U.M.M.; Schmitt, K.; Tremblay, C.; Remmele, J.; Orwat, S.; et al. Impact of the COVID-19 Pandemic on the Everyday Life and Healthcare of Patients with Congenital Heart Defects: Insights from Pandemic Onset to One Year Later. J. Clin. Med. 2025, 14, 3462. https://doi.org/10.3390/jcm14103462
Schütte E, Nasri SO, Ehmann A-L, Semmler J, Berger F, Bauer UMM, Schmitt K, Tremblay C, Remmele J, Orwat S, et al. Impact of the COVID-19 Pandemic on the Everyday Life and Healthcare of Patients with Congenital Heart Defects: Insights from Pandemic Onset to One Year Later. Journal of Clinical Medicine. 2025; 14(10):3462. https://doi.org/10.3390/jcm14103462
Chicago/Turabian StyleSchütte, Emily, Saskia Olivia Nasri, Anna-Lena Ehmann, Janina Semmler, Felix Berger, Ulrike M. M. Bauer, Katharina Schmitt, Cornelia Tremblay, Julia Remmele, Stefan Orwat, and et al. 2025. "Impact of the COVID-19 Pandemic on the Everyday Life and Healthcare of Patients with Congenital Heart Defects: Insights from Pandemic Onset to One Year Later" Journal of Clinical Medicine 14, no. 10: 3462. https://doi.org/10.3390/jcm14103462
APA StyleSchütte, E., Nasri, S. O., Ehmann, A.-L., Semmler, J., Berger, F., Bauer, U. M. M., Schmitt, K., Tremblay, C., Remmele, J., Orwat, S., Diller, G.-P., Pfitzer, C., & Helm, P. C. (2025). Impact of the COVID-19 Pandemic on the Everyday Life and Healthcare of Patients with Congenital Heart Defects: Insights from Pandemic Onset to One Year Later. Journal of Clinical Medicine, 14(10), 3462. https://doi.org/10.3390/jcm14103462