
The Daily and Two-Day Usage of Low-Dose Atropine on Myopic Control in a Low-Myopia Population
 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Ophthalmic Examination
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATR | atropine |
| AXL | axial length |
| CI | confidence interval |
| D | diopter |
| N | number |
| OR | odds ratio |
| SER | spherical equivalent refraction |
References
- Huang, J.; Wen, D.; Wang, Q.; McAlinden, C.; Flitcroft, I.; Chen, H.; Saw, S.M.; Chen, H.; Bao, F.; Zhao, Y.; et al. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmology 2016, 123, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Foreman, J.; Salim, A.T.; Praveen, A.; Fonseka, D.; Ting, D.S.W.; Guang He, M.; Bourne, R.R.A.; Crowston, J.; Wong, T.Y.; Dirani, M. Association between digital smart device use and myopia: A systematic review and meta-analysis. Lancet Digit. Health 2021, 3, e806–e818. [Google Scholar] [CrossRef] [PubMed]
- Ha, A.; Lee, Y.J.; Lee, M.; Shim, S.R.; Kim, Y.K. Digital Screen Time and Myopia: A Systematic Review and Dose-Response Meta-Analysis. JAMA Netw. Open 2025, 8, e2460026. [Google Scholar] [CrossRef]
- Chamberlain, P.; Lazon de la Jara, P.; Arumugam, B.; Bullimore, M.A. Axial length targets for myopia control. Ophthalmic Physiol. Opt. 2021, 41, 523–531. [Google Scholar] [CrossRef]
- Yang, Y.; Li, C.; Gao, Y. Prevalence of reduced visual acuity among adolescents in Jiaocheng County, Shanxi Province. BMC Ophthalmol. 2022, 22, 344. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef]
- Walline, J.J. Myopia Control: A Review. Eye Contact Lens 2016, 42, 3–8. [Google Scholar] [CrossRef]
- Chierigo, A.; Ferro Desideri, L.; Traverso, C.E.; Vagge, A. The Role of Atropine in Preventing Myopia Progression: An Update. Pharmaceutics 2022, 14, 900. [Google Scholar] [CrossRef]
- Brar, V.S. 2021–2022 Basic and Clinical Science Course, Section 02: Fundamentals and Principles of Ophthalmology; American Academy of Ophthalmology: San Francisco, CA, USA, 2021. [Google Scholar]
- Leo, S.W. Current approaches to myopia control. Curr. Opin. Ophthalmol. 2017, 28, 267–275. [Google Scholar] [CrossRef]
- Sankaridurg, P. Contact lenses to slow progression of myopia. Clin. Exp. Optom. 2017, 100, 432–437. [Google Scholar] [CrossRef]
- Remón, L.; Pérez-Merino, P.; Macedo-de-Araújo, R.J.; Amorim-de-Sousa, A.I.; González-Méijome, J.M. Bifocal and Multifocal Contact Lenses for Presbyopia and Myopia Control. J. Ophthalmol. 2020, 2020, 8067657. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.; Tang, W.C.; Lee, P.H.; Zhang, H.Y.; Qi, H.; Hasegawa, K.; To, C.H. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: Results of a 3-year follow-up study. Br. J. Ophthalmol. 2022, 106, 1110–1114. [Google Scholar] [CrossRef]
- Tsai, H.R.; Wang, J.H.; Huang, H.K.; Chen, T.L.; Chen, P.W.; Chiu, C.J. Efficacy of atropine, orthokeratology, and combined atropine with orthokeratology for childhood myopia: A systematic review and network meta-analysis. J. Formos. Med. Assoc. 2022, 121, 2490–2500. [Google Scholar] [CrossRef]
- Wu, P.C.; Chuang, M.N.; Choi, J.; Chen, H.; Wu, G.; Ohno-Matsui, K.; Jonas, J.B.; Cheung, C.M.G. Update in myopia and treatment strategy of atropine use in myopia control. Eye 2019, 33, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Shi, M.H.; Li, X. Efficacy and safety of atropine in myopic children: A meta-analysis of randomized controlled trials. J. Fr. Ophtalmol. 2023, 46, 929–940. [Google Scholar] [CrossRef]
- Min, J.S.; Min, B.M. The Effect of Alternating Monocular Instillation of 0.125% Atropine in Korean Children with Progressive Myopia. J. Clin. Med. 2024, 13, 5003. [Google Scholar] [CrossRef] [PubMed]
- Loughman, J.; Kobia-Acquah, E.; Lingham, G.; Butler, J.; Loskutova, E.; Mackey, D.A.; Lee, S.S.Y.; Flitcroft, D.I. Myopia outcome study of atropine in children: Two-year result of daily 0.01% atropine in a European population. Acta Ophthalmol. 2024, 102, e245–e256. [Google Scholar] [CrossRef]
- Repka, M.X.; Weise, K.K.; Chandler, D.L.; Wu, R.; Melia, B.M.; Manny, R.E.; Kehler, L.A.F.; Jordan, C.O.; Raghuram, A.; Summers, A.I.; et al. Low-Dose 0.01% Atropine Eye Drops vs Placebo for Myopia Control: A Randomized Clinical Trial. JAMA Ophthalmol. 2023, 141, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Nilagiri, V.K.; Lingham, G.; Blaszkowska, M.; Sanfilippo, P.G.; Franchina, M.; Clark, A.; Mackey, D.A. Myopia progression following 0.01% atropine cessation in Australian children: Findings from the Western Australia—Atropine for the Treatment of Myopia (WA-ATOM) study. Clin. Exp. Ophthalmol. 2024, 52, 507–515. [Google Scholar] [CrossRef]
- Zadnik, K.; Schulman, E.; Flitcroft, I.; Fogt, J.S.; Blumenfeld, L.C.; Fong, T.M.; Lang, E.; Hemmati, H.D.; Chandler, S.P. Efficacy and Safety of 0.01% and 0.02% Atropine for the Treatment of Pediatric Myopia Progression Over 3 Years: A Randomized Clinical Trial. JAMA Ophthalmol. 2023, 141, 990–999. [Google Scholar] [CrossRef]
- Chia, A.; Lu, Q.S.; Tan, D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016, 123, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Ang, M.; Cho, P.; Guggenheim, J.A.; He, M.G.; Jong, M.; Logan, N.S.; Liu, M.; Morgan, I.; Ohno-Matsui, K.; et al. IMI Prevention of Myopia and Its Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 6. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Jiang, L.; Chen, M. Effect of atropine 0.01% on myopia control in children aged 6–13 years during the 2022 lockdown in Shanghai. Front. Public Health 2023, 11, 1074272. [Google Scholar] [CrossRef]
- Upadhyay, A.; Beuerman, R.W. Biological Mechanisms of Atropine Control of Myopia. Eye Contact Lens 2020, 46, 129–135. [Google Scholar] [CrossRef]
- Austermann, H.; Schaeffel, F.; Mathis, U.; Hund, V.; Mußhoff, F.; Ziemssen, F.; Schnichels, S. Corneal Penetration of Low-Dose Atropine Eye Drops. J. Clin. Med. 2021, 10, 588. [Google Scholar] [CrossRef]
- Simonaviciute, D.; Grzybowski, A.; Lanca, C.; Pang, C.P.; Gelzinis, A.; Zemaitiene, R. The Effectiveness and Tolerability of Atropine Eye Drops for Myopia Control in Non-Asian Regions. J. Clin. Med. 2023, 12, 2314. [Google Scholar] [CrossRef]
- Kuo, H.Y.; Ke, C.H.; Chen, S.T.; Sun, H.Y. The Impact of Clinical Atropine Use in Taiwanese Schoolchildren: Changes in Physiological Characteristics and Visual Functions. Children 2021, 8, 1054. [Google Scholar] [CrossRef]
- Ho, C.L. Context of Atropine Adherence in Preschool Children with Early-Onset Myopia: A Qualitative Study. Children 2024, 11, 1087. [Google Scholar] [CrossRef]
- Mutti, D.O. Hereditary and environmental contributions to emmetropization and myopia. Optom. Vis. Sci. 2010, 87, 255–259. [Google Scholar] [CrossRef]
- Whitmore, W.G. Congenital and developmental myopia. Eye 1992, 6 Pt 4, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.R.; Chen, S.C.; Wan, T.Y.; Chuang, L.H.; Chen, H.C.; Yeh, L.K.; Kuo, Y.K.; Wu, P.C.; Chen, Y.W.; Lai, I.C.; et al. Treatment of Myopia with Atropine 0.125% Once Every Night Compared with Atropine 0.125% Every Other Night: A Pilot Study. J. Clin. Med. 2023, 12, 5220. [Google Scholar] [CrossRef]
- Chamberlain, P.; Peixoto-de-Matos, S.C.; Logan, N.S.; Ngo, C.; Jones, D.; Young, G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom. Vis. Sci. 2019, 96, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ding, X.; Xiong, R.; Zhang, J.; Song, F.; Zhao, Z.; Lai, M.; Zeng, Y.; He, M. Physiological growth of ocular axial length among Chinese children and teenagers: A 6-year cohort study. PLoS ONE 2025, 20, e0317756. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef]
- Cooper, J.; Tkatchenko, A.V. A Review of Current Concepts of the Etiology and Treatment of Myopia. Eye Contact Lens 2018, 44, 231–247. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, F.; Yu, S.; Ma, N.; Huang, C.; Wang, M.; Wei, L.; Zhang, J.; Fu, A. Prevention of myopia shift and myopia onset using 0.01% atropine in premyopic children—A prospective, randomized, double-masked, and crossover trial. Eur. J. Pediatr. 2023, 182, 2597–2606. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characters | Daily Group (N = 32) | Two-Day Group (N = 26) | p |
|---|---|---|---|
| Age | 7.72 ± 1.22 | 7.50 ± 1.32 | 0.519 |
| Sex (male/female) | 18:14 | 15:11 | 0.562 |
| BCVA (LogMAR) | 0.00 ± 0.01 | 0.00 ± 0.01 | 0.999 |
| Sphere power | −0.67 ± 0.13 | −0.60 ± 0.15 | 0.082 |
| Cylinder power | −0.25 ± 0.08 | −0.28 ± 0.10 | 0.249 |
| SER | −0.80 ± 0.11 | −0.74 ± 0.14 | 0.082 |
| Simulated keratometry | 43.24 ± 1.78 | 43.52 ± 1.91 | 0.656 |
| Corneal astigmatism | 0.44 ± 0.16 | 0.52 ± 0.17 | 0.087 |
| AXL | 22.92 ± 0.29 | 22.87 ± 0.24 | 0.525 |
| Characters | Daily Group | Two-Day Group | p |
|---|---|---|---|
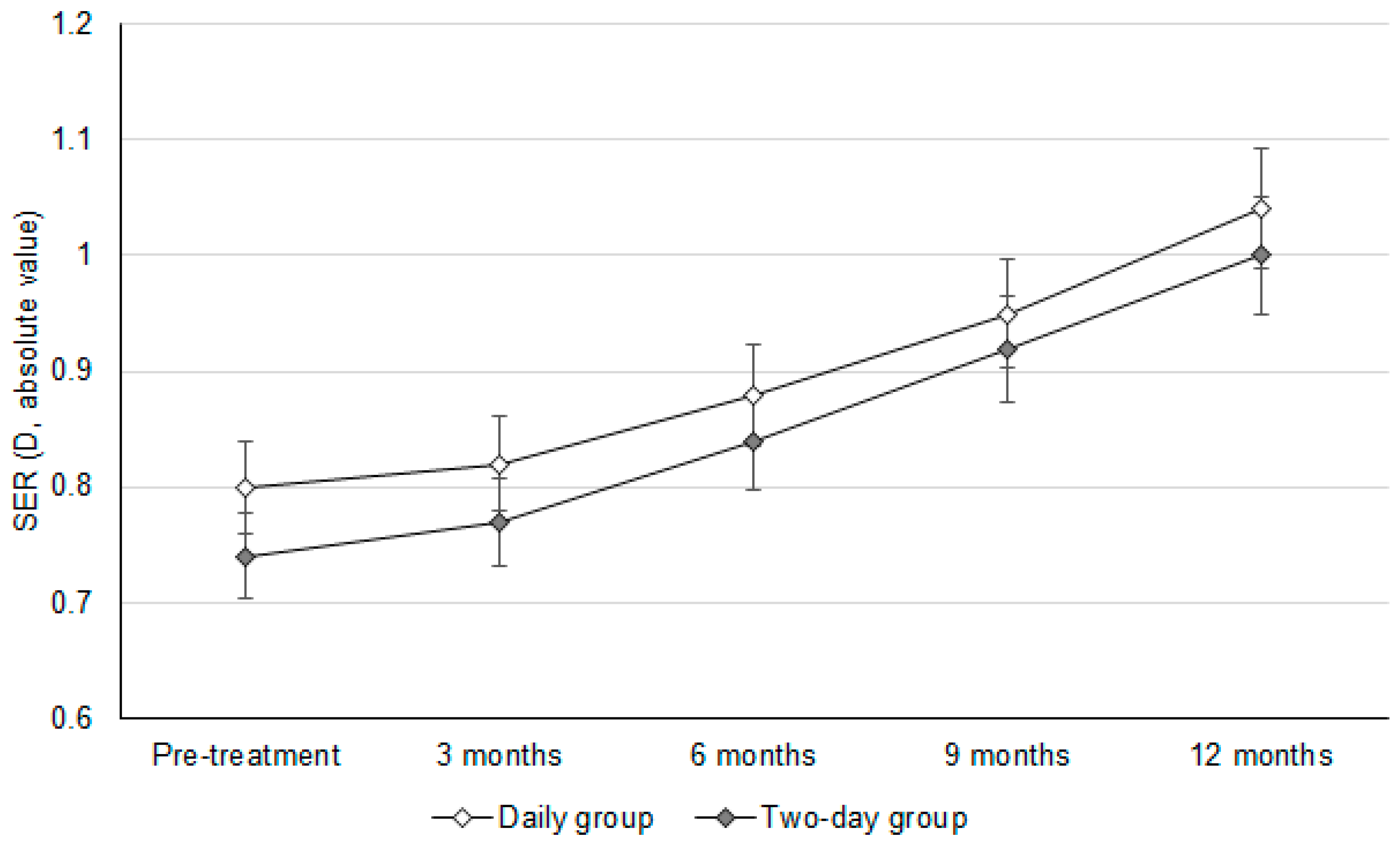
| SER | |||
| Pre-treatment | −0.80 ± 0.11 | −0.74 ± 0.14 | 0.082 |
| Post-treatment | −1.04 ± 0.12 | −1.00 ± 0.14 | 0.307 |
| Change | −0.24 ± 0.09 | −0.26 ± 0.08 | 0.393 |
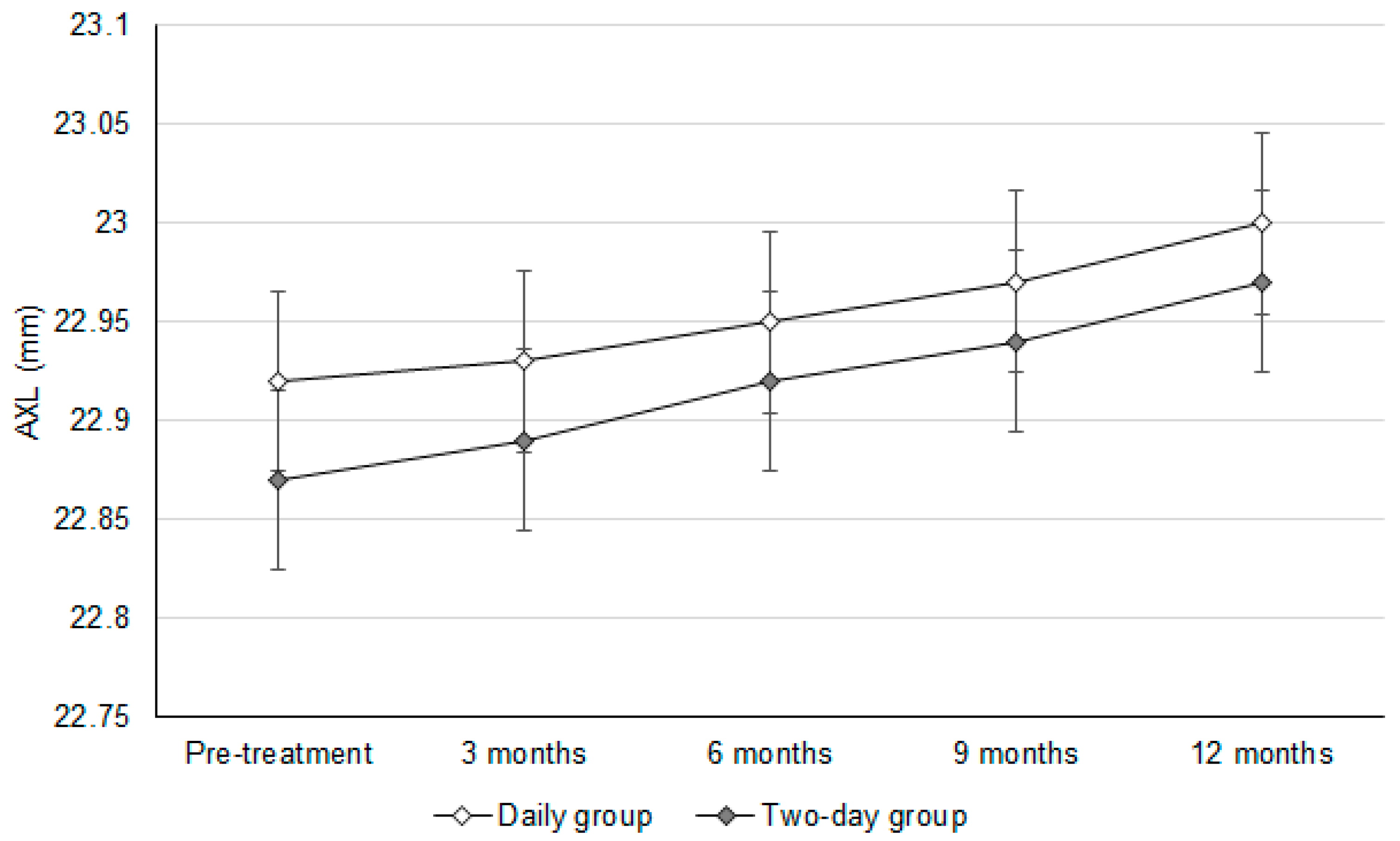
| AXL | |||
| Pre-treatment | 22.92 ± 0.29 | 22.87 ± 0.24 | 0.525 |
| Post-treatment | 23.00 ± 0.23 | 22.97 ± 0.21 | 0.689 |
| Change | 0.09 ± 0.07 | 0.10 ± 0.09 | 0.655 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Yang, S.-F.; Huang, J.-Y.; Lian, I.-B.; Chang, C.-K. The Daily and Two-Day Usage of Low-Dose Atropine on Myopic Control in a Low-Myopia Population. J. Clin. Med. 2025, 14, 3458. https://doi.org/10.3390/jcm14103458
Lee C-Y, Yang S-F, Huang J-Y, Lian I-B, Chang C-K. The Daily and Two-Day Usage of Low-Dose Atropine on Myopic Control in a Low-Myopia Population. Journal of Clinical Medicine. 2025; 14(10):3458. https://doi.org/10.3390/jcm14103458
Chicago/Turabian StyleLee, Chia-Yi, Shun-Fa Yang, Jing-Yang Huang, Ie-Bin Lian, and Chao-Kai Chang. 2025. "The Daily and Two-Day Usage of Low-Dose Atropine on Myopic Control in a Low-Myopia Population" Journal of Clinical Medicine 14, no. 10: 3458. https://doi.org/10.3390/jcm14103458
APA StyleLee, C.-Y., Yang, S.-F., Huang, J.-Y., Lian, I.-B., & Chang, C.-K. (2025). The Daily and Two-Day Usage of Low-Dose Atropine on Myopic Control in a Low-Myopia Population. Journal of Clinical Medicine, 14(10), 3458. https://doi.org/10.3390/jcm14103458