
Early Evaluation of Myeloperoxidase and Delta Neutrophil Indices Is Similar to 48 h Sequential Organ Failure Assessment Score for Predicting Multiple Organ Failure After Trauma
 , , , ,
, , , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
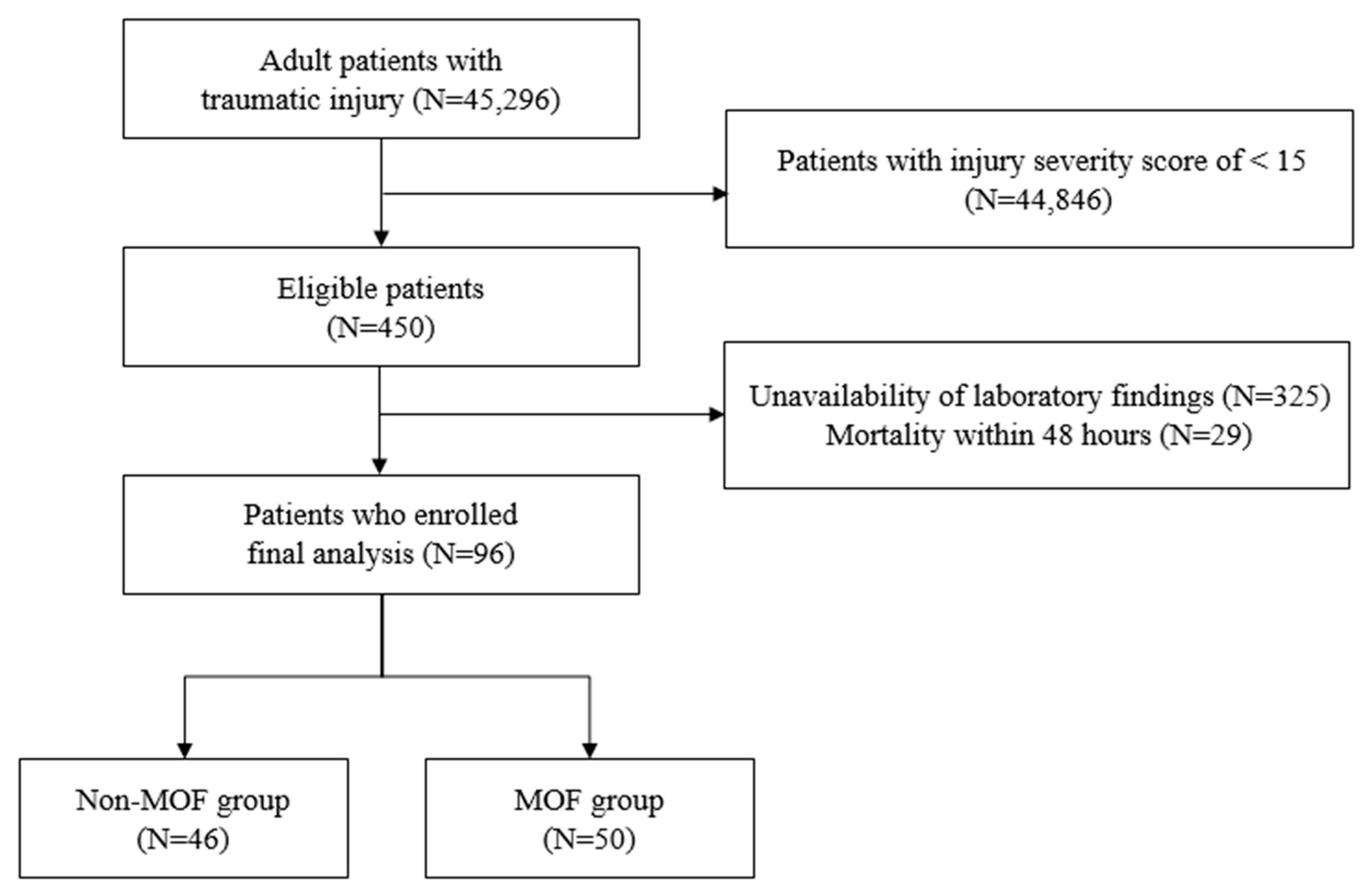
2.1. Study Setting and Enrolled Patients
2.2. Measurement of Variables
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
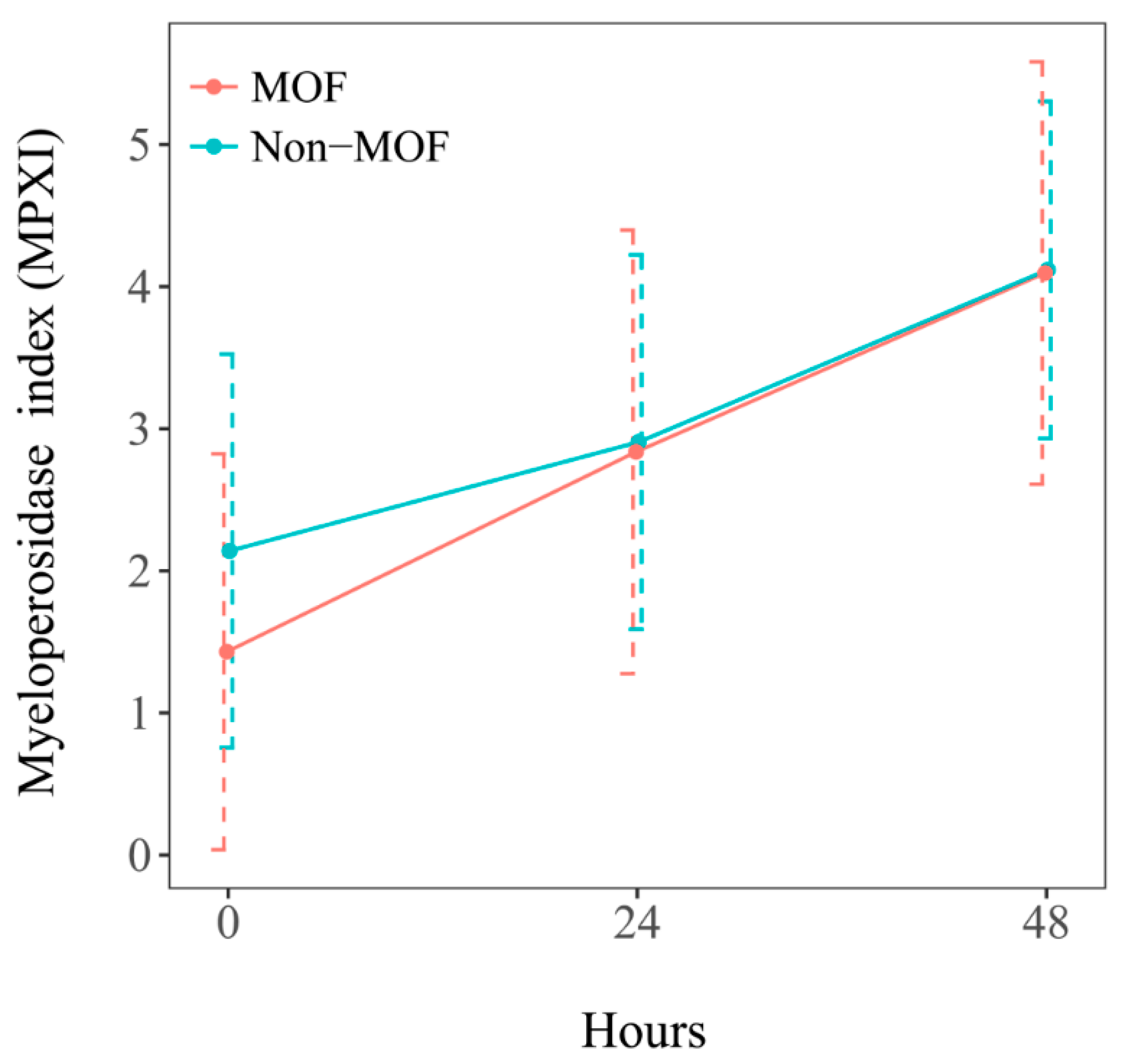
3.2. Myeloperoxidase and Delta Neutrophil Indices
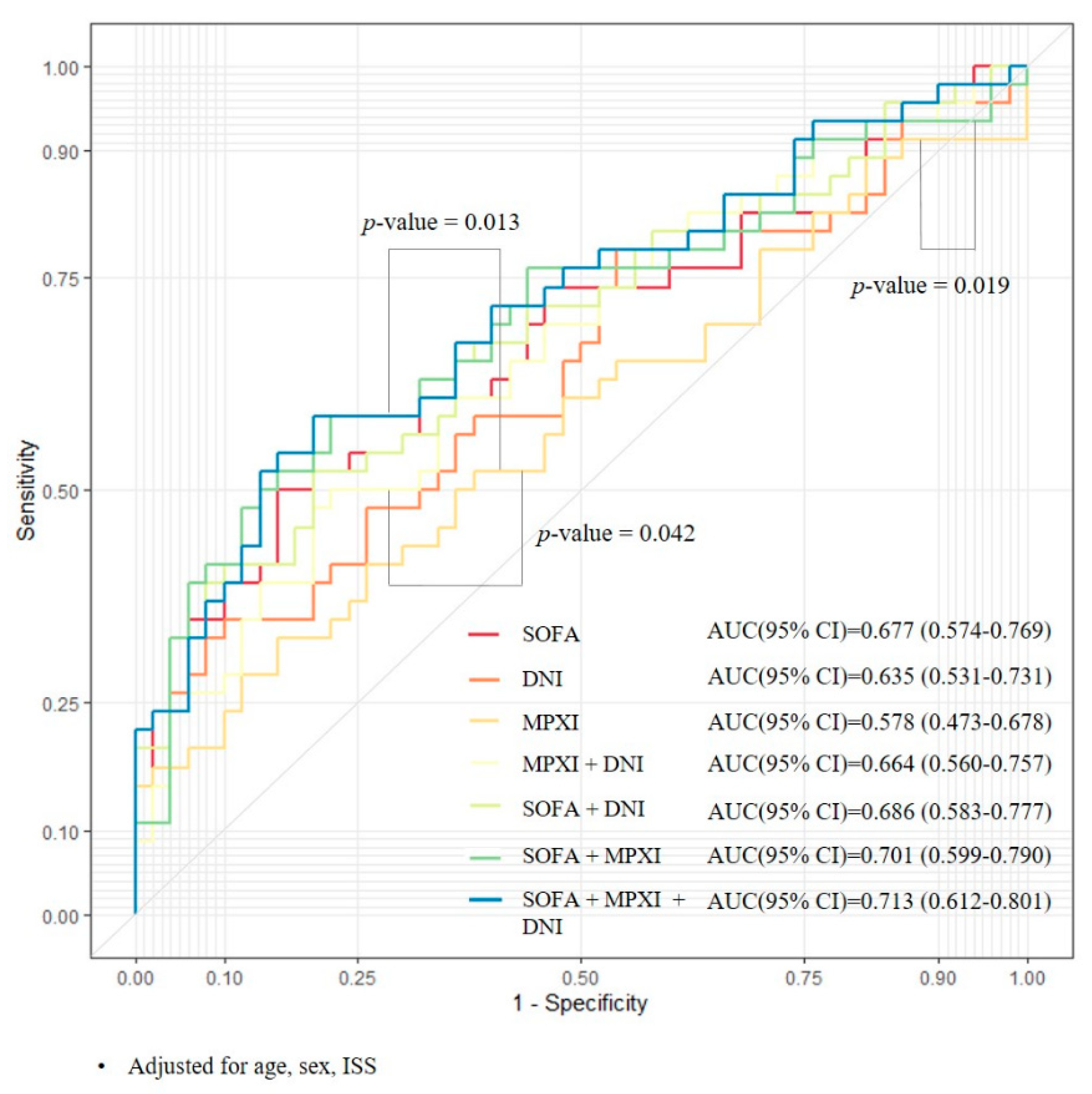
3.3. Comparative Analysis of Predictive Factors Related to Multiple Organ Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MOF | Multiple organ failure |
| ICU | Intensive care unit |
| SIRS | Systemic inflammatory response syndrome |
| SOFA | Sequential organ failure assessment |
| MPXI | Myeloperoxidase index |
| DNI | Delta neutrophil index |
| MPO | Myeloperoxidase |
| MAP | Mean arterial pressure |
References
- Nast-Kolb, D.; Aufmkolk, M.; Rucholtz, S.; Obertacke, U.; Waydhas, C. Multiple organ failure still a major cause of morbidity but not mortality in blunt multiple trauma. J. Trauma. 2001, 51, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Dewar, D.; Moore, F.A.; Moore, E.E.; Balogh, Z. Postinjury multiple organ failure. Injury 2009, 40, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Sauaia, A.; Moore, F.A.; Moore, E.E.; Moser, K.S.; Brennan, R.; Read, R.A.; Pons, P.T. Epidemiology of trauma deaths: A reassessment. J. Trauma. 1995, 38, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Ciesla, D.J.; Moore, E.E.; Johnson, J.L.; Burch, J.M.; Cothren, C.C.; Sauaia, A. A 12-year prospective study of postinjury multiple organ failure: Has anything changed? Arch. Surg. 2005, 140, 432–440. [Google Scholar] [CrossRef]
- Keel, M.; Trentz, O. Pathophysiology of polytrauma. Injury 2005, 36, 691–709. [Google Scholar] [CrossRef]
- Muckart, D.J.; Bhagwanjee, S. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference definitions of the systemic inflammatory response syndrome and allied disorders in relation to critically injured patients. Crit. Care Med. 1997, 25, 1789–1795. [Google Scholar] [CrossRef]
- Maier, B.; Lefering, R.; Lehnert, M.; Laurer, H.L.; Steudel, W.I.; Neugebauer, E.A.; Marzi, I. Early versus late onset of multiple organ failure is associated with differing patterns of plasma cytokine biomarker expression and outcome after severe trauma. Shock 2007, 28, 668–674. [Google Scholar] [CrossRef]
- Damsgaard, C.T.; Lauritzen, L.; Calder, P.C.; Kjaer, T.M.; Frokiaer, H. Whole-blood culture is a valid low-cost method to measure monocytic cytokines—A comparison of cytokine production in cultures of human whole-blood, mononuclear cells and monocytes. J. Immunol. Methods 2009, 340, 95–101. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Seok, Y.; Choi, J.R.; Kim, J.; Kim, Y.K.; Lee, J.; Song, J.; Kim, S.J.; Lee, K.A. Delta neutrophil index: A promising diagnostic and prognostic marker for sepsis. Shock 2012, 37, 242–246. [Google Scholar] [CrossRef]
- Ahn, C.; Kim, W.; Lim, T.H.; Cho, Y.; Choi, K.S.; Jang, B.H. The delta neutrophil index (DNI) as a prognostic marker for mortality in adults with sepsis: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 6621. [Google Scholar] [CrossRef] [PubMed]
- Yonezawa, K.; Horie, O.; Yoshioka, A.; Matsuki, S.; Tenjin, T.; Tsukamura, Y.; Yoneda, M.; Shibata, K.; Koike, Y.; Nomura, T.; et al. Association between the neutrophil myeloperoxidase index and subsets of bacterial infections. Int. J. Lab. Hematol. 2010, 32, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.S.; Yoon, J.M.; Jung, W.J.; Kim, Y.W.; Kim, T.H.; Kim, O.H.; Cha, K.C.; Kim, H.; Hwang, S.O.; Lee, K.H. Evaluation of usefulness of myeloperoxidase index (MPXI) for differential diagnosis of systemic inflammatory response syndrome (SIRS) in the emergency department. Emerg. Med. J. 2015, 32, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Badwey, J.A.; Karnovsky, M.L. Active oxygen species and the functions of phagocytic leukocytes. Annu. Rev. Biochem. 1980, 49, 695–726. [Google Scholar] [CrossRef]
- Aratani, Y.; Koyama, H.; Nyui, S.; Suzuki, K.; Kura, F.; Maeda, N. Severe impairment in early host defense against Candida albicans in mice deficient in myeloperoxidase. Infect. Immun. 1999, 67, 1828–1836. [Google Scholar] [CrossRef]
- Kong, T.; In, S.; Park, Y.S.; Lee, H.S.; Lee, J.W.; You, J.S.; Chung, H.S.; Park, I.; Chung, S.P. Usefulness of the delta neutrophil index to predict 30-day mortality in patients with upper gastrointestinal bleeding. Shock 2017, 48, 427–435. [Google Scholar] [CrossRef]
- Kong, T.; Park, Y.S.; Lee, H.S.; Kim, S.; Lee, J.W.; You, J.S.; Chung, H.S.; Park, I.; Chung, S.P. The delta neutrophil index predicts development of multiple organ dysfunction syndrome and 30-day mortality in trauma patients admitted to an intensive care unit: A retrospective analysis. Sci. Rep. 2018, 8, 17515. [Google Scholar] [CrossRef]
- Cole, E.; Davenport, R.; Willett, K.; Brohi, K. The burden of infection in severely injured trauma patients and the relationship with admission shock severity. J. Trauma. Acute Care Surg. 2014, 76, 730–735. [Google Scholar] [CrossRef]
- Peres Bota, D.; Melot, C.; Lopes Ferreira, F.; Nguyen Ba, V.; Vincent, J.L. The Multiple Organ Dysfunction Score (MODS) versus the Sequential Organ Failure Assessment (SOFA) score in outcome prediction. Intensive Care Med. 2002, 28, 1619–1624. [Google Scholar] [CrossRef]
- Maas, A.I.; Hukkelhoven, C.W.; Marshall, L.F.; Steyerberg, E.W. Prediction of outcome in traumatic brain injury with computed tomographic characteristics: A comparison between the computed tomographic classification and combinations of computed tomographic predictors. Neurosurgery 2005, 57, 1173–1182. [Google Scholar] [CrossRef]
- Dewar, D.C.; White, A.; Attia, J.; Tarrant, S.M.; King, K.L.; Balogh, Z.J. Comparison of postinjury multiple-organ failure scoring systems: Denver versus Sequential Organ Failure Assessment. J. Trauma. Acute Care Surg. 2014, 77, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.; Kunicka, J.; Kratz, A. The ADVIA 2120 hematology system: Flow cytometry-based analysis of blood and body fluids in the routine hematology laboratory. Lab. Hematol. 2005, 11, 47–61. [Google Scholar] [CrossRef]
- Nahm, C.H.; Choi, J.W.; Lee, J. Delta neutrophil index in automated immature granulocyte counts for assessing disease severity of patients with sepsis. Ann. Clin. Lab. Sci. 2008, 38, 241–246. [Google Scholar]
- Kim, O.H.; Cha, Y.S.; Hwang, S.O.; Jang, J.Y.; Choi, E.H.; Kim, H.I.; Cha, K.; Kim, H.; Lee, K.H. The Use of Delta Neutrophil Index and Myeloperoxidase Index for Predicting Acute Complicated Appendicitis in Children. PLoS ONE 2016, 11, e0148799. [Google Scholar] [CrossRef] [PubMed]
- Llompart-Pou, J.A.; Talayero, M.; Homar, J.; Royo, C.; Neurointens, G.T.T. Multiorgan failure in the serious trauma patient. Med. Intensiv. 2014, 38, 455–462. [Google Scholar] [CrossRef]
- Rangel-Frausto, M.S.; Pittet, D.; Costigan, M.; Hwang, T.; Davis, C.S.; Wenzel, R.P. The natural history of the systemic inflammatory response syndrome (SIRS). A prospective study. JAMA 1995, 273, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, L.; Watkinson, P.; Young, J.D.; Willett, K. Defining multiple organ failure after major trauma: A comparison of the Denver, Sequential Organ Failure Assessment, and Marshall scoring systems. J. Trauma. Acute Care Surg. 2017, 82, 534–541. [Google Scholar] [CrossRef]
- Hazeldine, J.; Hampson, P.; Lord, J.M. The diagnostic and prognostic value of systems biology research in major traumatic and thermal injury: A review. Burns Trauma. 2016, 4, 33. [Google Scholar] [CrossRef]
- Nydam, T.L.; Kashuk, J.L.; Moore, E.E.; Johnson, J.L.; Burlew, C.C.; Biffl, W.L.; Barnett, C.C., Jr.; Sauaia, A. Refractory postinjury thrombocytopenia is associated with multiple organ failure and adverse outcomes. J. Trauma. 2011, 70, 401–407. [Google Scholar] [CrossRef]
- Huber-Lang, M.; Lambris, J.D.; Ward, P.A. Innate immune responses to trauma. Nat. Immunol. 2018, 19, 327–341. [Google Scholar] [CrossRef]
- Wrba, L.; Halbgebauer, R.; Roos, J.; Huber-Lang, M.; Fischer-Posovszky, P. Adipose tissue: A neglected organ in the response to severe trauma? Cell Mol. Life Sci. 2022, 79, 207. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SOFA | |||||
|---|---|---|---|---|---|
| Variables | 0 | 1 | 2 | 3 | 4 |
| Respiration PaO2/FiO2 | >400 | ≤400 | ≤300 | ≤200 with respiratory support | ≤100 with respiratory support |
| Coagulation Platelet (×109/L) | >150 | ≤150 | ≤100 | ≤50 | ≤20 |
| Liver Total bilirubin (mg/dL) | <1.2 | 1.2–1.9 | 2.0–5.9 | 6.0–11.9 | ≥12.0 |
| Cardiovascular Hypotension | No Hypotension | MAP < 70 mmHg | Dopamine ≤ 5 or dobutamine (any dose) | Dopamine > 5 or epinephrine ≤ 0.1 or norepinephrine ≤ 0.1 | Dopamine > 15 or epinephrine > 0.1 or norepinephrine > 0.1 |
| Central Nervous System Glasgow coma scale | 15 | 13–14 | 10–12 | 6–9 | <6 |
| Renal Creatinine (mg/dL) | <1.2 | 1.2–1.9 | 2.0–3.4 | 3.5–4.9 | ≥5.0 |
| Total (n = 96) | Non-MOF Group (n = 50) | MOF Group (n = 46) | p Value | |
|---|---|---|---|---|
| Male (sex) | 74 (77.1%) | 39 (78.0%) | 35 (76.0%) | 1.000 |
| Age (years) | 52.0 (35.0–69.5) | 48.5 (37.5–63.7) | 55.5 (27.0–73.2) | 0.538 |
| Systolic blood pressure (mmHg) | 126 (95–146) | 120 (74–142) | 96 (77–131) | 0.072 |
| Diastolic blood pressure (mmHg) | 72 (60–89) | 64 (45–80) | 61 (46–77) | 0.139 |
| Pulse rate (beats/minute) | 96 (75–112) | 97 (82–111) | 101 (74–119) | 0.887 |
| Body temperature (°C) | 36.0 (35.6–36.4) | 36.0 (35.6–36.4) | 36.0 (35.1–36.2) | 0.221 |
| Glasgow coma scale | 11.6 ± 3.8 | 12.0 ± 3.7 | 11.2 ± 3.9 | 0.306 |
| ISS | 24.5 ± 8.8 | 22.9 ± 5.9 | 26.3 ± 10.9 | 0.065 |
| AIS1 | 3 (1–4) | 3 (0–4) | 3 (2–4) | 0.342 |
| AIS2 | 0 (0–1) | 0 (0–1) | 0 (0–2) | 0.112 |
| AIS3 | 3 (0–3) | 3 (0–3) | 3 (1–3) | 0.620 |
| AIS4 | 2 (0–2) | 1 (0–2) | 2 (0–3) | 0.466 |
| AIS5 | 0 (0–2) | 2 (0–2) | 0 (0–2) | 0.316 |
| AIS6 | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.330 |
| SOFA * | 5.7 ± 3.5 | 4.7 ± 2.7 | 6.8 ± 3.9 | 0.004 |
| Denver MOF score | 1 (0–1) | 1 (0–1) | 1.5 (0–4) | <0.001 |
| Rotterdam CT score | 2.9 ± 1.2 | 2.8 ± 1.2 | 2.9 ± 1.1 | 0.637 |
| Injury mechanism | 0.374 | |||
| Motor vehicle accident | 61 (63.5%) | 33 (66.0%) | 28 (60.8%) | |
| Falls | 21 (21.9%) | 10 (20.0%) | 11 (23.9%) | |
| Slip down | 6 (6.3%) | 3 (6.0%) | 3 (6.5%) | |
| Blunt injury | 4 (4.2%) | 3 (6.0%) | 1 (2.2%) | |
| Penetrating injury | 1 (1.0%) | 0 (0%) | 1 (2.2%) | |
| Others | 3 (3.1%) | 1 (2.0%) | 2 (4.4%) | |
| Laboratory findings | ||||
| Hemoglobin | 12.8 (10.4–14.2) | 13.3 (10.4–14.6) | 12.7 (10.4–13.5) | 0.364 |
| Platelets | 229 (170–283) | 235 (167–295) | 228 (170–270) | 0.697 |
| PT INR † | 1.08 ± 0.25 | 1.0 ± 0.2 | 1.1 ± 0.2 | 0.463 |
| C-reactive protein | 0.46 (0.29–1.08) | 0.71 (0.39–1.48) | 0.35 (0.06–0.63) | 0.056 |
| Worst lactate, 0–12 h | 2.57 (1.79–3.44) | 2.68 (1.72–3.61) | 2.48 (1.94–3.35) | 0.659 |
| Worst lactate, 12–24 h | 2.57 (1.70–3.44) | 2.68 (1.72–3.59) | 2.48 (1.70–3.35) | 0.575 |
| Worst base excess 0–12 h | −7.8 (−10.6–−5.1) | −7.7 (−10.6–−4.3) | −8.2 (−10.6–−5.6) | 0.358 |
| Worst base excess 12–24 h | −7.9 (−10.8–−5.1) | −7.7 (−10.9–−4.9) | −8.3 (−10.6–−6.5) | 0.423 |
| Transfusion (mL) | ||||
| Packed red blood cells | 1145 ± 931 | 1040 ± 917 | 1224 ± 951 | 0.499 |
| Fresh frozen plasma | 688 (352–1162) | 381 (332–747) | 925 (526–1264) | 0.006 |
| Length of ICU stay (days) | 23 (16–36) | 20 (15–29) | 32 (18–40) | 0.007 |
| Length of hospital stay (days) | 46(31–95) | 44(31–94) | 53(28–95) | 0.982 |
| Occurrence of MOF (day) | - | - | 5.3 ± 4.0 | - |
| Mechanical ventilation | 81 (84.4%) | 38 (76.0%) | 43 (93.5%) | 0.024 |
| Vasopressor use | 33 (34.4%) | 9 (18.0%) | 24 (52.2%) | <0.001 |
| Mortality | 14 (14.6%) | 1 (2.0%) | 13 (28.2%) | <0.001 |
| Total (n = 96) | Non-MOF Group (n = 50) | MOF Group (n = 46) | p Value | |
|---|---|---|---|---|
| Exploratory laparotomy * | 16 (16.6%) | 8 (16.0%) | 8 (17.4%) | 1.000 |
| Interventional angiography † | 2 (2.0%) | 0 (0%) | 2 (4.3%) | 0.227 |
| Exploratory thoracotomy and lung repair | 3 (3.1%) | 0 (0%) | 3 (6.5%) | 0.106 |
| Closed thoracostomy | 15 (15.6%) | 11 (22.0%) | 4 (8.6%) | 0.094 |
| Decompressive craniectomy and hematoma evacuation | 20 (20.8%) | 10 (20.0%) | 10 (21.7%) | 1.000 |
| Drainage catheter insertion for intracranial hemorrhage | 4 (4.1%) | 2 (4.0%) | 2 (4.3%) | 1.000 |
| Open reduction and internal fixation (injured extremity) | 5 (5.2%) | 4 (8.0%) | 1 (2.1%) | 0.364 |
| Limb amputation | 1 (1.0%) | 0 (0%) | 1 (2.1%) | 0.479 |
| Conservative management | 33 (34.4%) | 16 (32.0%) | 17 (36.9%) | 0.670 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, W.J.; Kim, H.S.; Cha, K.C.; Roh, Y.-I.; An, G.J.; Cha, Y.S.; Kim, H.; Lee, K.H.; Hwang, S.O.; Kim, O.H. Early Evaluation of Myeloperoxidase and Delta Neutrophil Indices Is Similar to 48 h Sequential Organ Failure Assessment Score for Predicting Multiple Organ Failure After Trauma. J. Clin. Med. 2025, 14, 3447. https://doi.org/10.3390/jcm14103447
Jung WJ, Kim HS, Cha KC, Roh Y-I, An GJ, Cha YS, Kim H, Lee KH, Hwang SO, Kim OH. Early Evaluation of Myeloperoxidase and Delta Neutrophil Indices Is Similar to 48 h Sequential Organ Failure Assessment Score for Predicting Multiple Organ Failure After Trauma. Journal of Clinical Medicine. 2025; 14(10):3447. https://doi.org/10.3390/jcm14103447
Chicago/Turabian StyleJung, Woo Jin, Hye Sim Kim, Kyoung Chul Cha, Young-Il Roh, Gyo Jin An, Yong Sung Cha, Hyun Kim, Kang Hyun Lee, Sung Oh Hwang, and Oh Hyun Kim. 2025. "Early Evaluation of Myeloperoxidase and Delta Neutrophil Indices Is Similar to 48 h Sequential Organ Failure Assessment Score for Predicting Multiple Organ Failure After Trauma" Journal of Clinical Medicine 14, no. 10: 3447. https://doi.org/10.3390/jcm14103447
APA StyleJung, W. J., Kim, H. S., Cha, K. C., Roh, Y.-I., An, G. J., Cha, Y. S., Kim, H., Lee, K. H., Hwang, S. O., & Kim, O. H. (2025). Early Evaluation of Myeloperoxidase and Delta Neutrophil Indices Is Similar to 48 h Sequential Organ Failure Assessment Score for Predicting Multiple Organ Failure After Trauma. Journal of Clinical Medicine, 14(10), 3447. https://doi.org/10.3390/jcm14103447