

Aligners as a Therapeutic Approach in Impacted Canine Treatment: A Systematic Review

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Focus Question and Eligibility Criteria
2.3. Search Strategy, Information Sources, and Study Selection
2.4. Data Collection Process and Data Items
2.5. Risk of Bias and Quality Assessment
2.6. Quality Assessment
3. Results
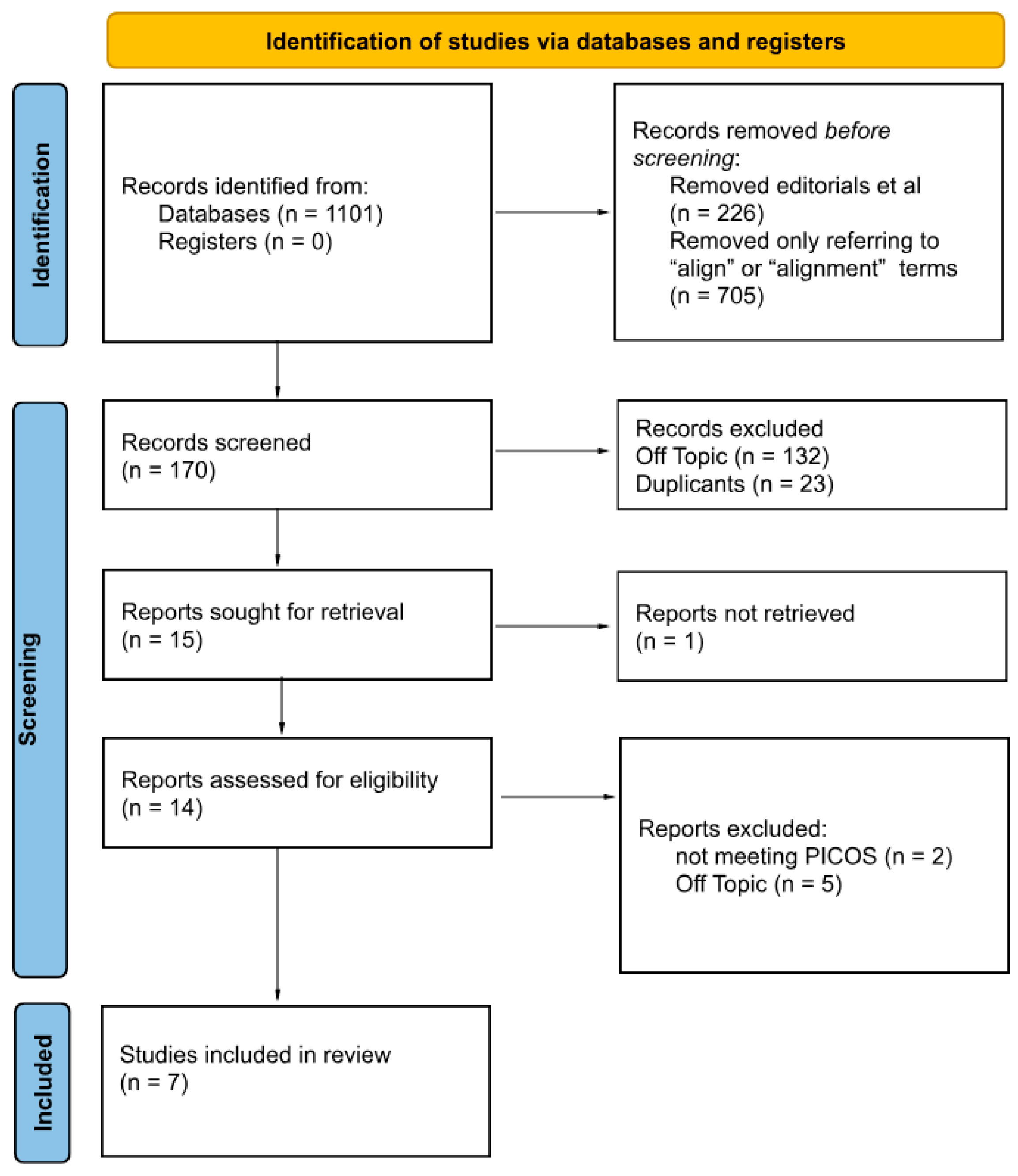
3.1. Literature Search Results and Study Selection
3.2. Study Characteristics
3.3. Main Study Outcomes
3.4. Quality Assessment of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vlaskalic, V.; Boyd, R. Orthodontic Treatment of a Mildly Crowded Malocclusion Using the Invisalign System. Aust. Orthod. J. 2001, 17, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Schupp, W.; Haubrich, J.; Neumann, I. Treatment of anterior open bite with the Invisalign system. J. Clin. Orthod. 2010, 44, 501–507. [Google Scholar] [PubMed]
- Celikoglu, M.; Kamak, H.; Oktay, H. Investigation of Transmigrated and Impacted Maxillary and Mandibular Canine Teeth in an Orthodontic Patient Population. J. Oral. Maxillofac. Surg. 2010, 68, 1001–1006. [Google Scholar] [CrossRef]
- Grover, P.; Lorton, L. The Incidence of Unerupted Permanent Teeth and Related Clinical Cases. Oral Surg. Oral Med. Oral Pathol. 1985, 59, 420–425. [Google Scholar] [CrossRef]
- Jacobs, S.G. Localization of the Unerupted Maxillary Canine: How to and when to. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 314–322. [Google Scholar] [CrossRef]
- Ericson, S.; Kurol, P.J. Resorption of Incisors after Ectopic Eruption of Maxillary Canines: A CT Study. Angle Orthod. 2000, 70, 415–423. [Google Scholar]
- Kettle, M.A. Treatment of the Unerupted Maxillary Canine. Trans. Br. Soc. Orthod. 1957, 18, 74–84. [Google Scholar]
- Ericson, S.; Kurol, J. Resorption of Maxillary Lateral Incisors Caused by Ectopic Eruption of the Canines. A Clinical and Radiographic Analysis of Predisposing Factors. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 503–513. [Google Scholar] [CrossRef]
- Alqerban, A.; Jacobs, R.; Fieuws, S.; Willems, G. Root Resorption of the Maxillary Lateral Incisor Caused by Impacted Canine: A Literature Review. Clin. Oral Investig. 2009, 13, 247–255. [Google Scholar] [CrossRef]
- Iancu Potrubacz, M.; Chimenti, C.; Marchione, L.; Tepedino, M. Retrospective Evaluation of Treatment Time and Efficiency of a Predictable Cantilever System for Orthodontic Extrusion of Impacted Maxillary Canines. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 55–64. [Google Scholar] [CrossRef]
- Chapokas, A.R.; Almas, K.; Schincaglia, G.P. The Impacted Maxillary Canine: A Proposed Classification for Surgical Exposure. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Sezici, Y.L.; Gediz, M.; Akış, A.A.; Sarı, G.; Duran, G.S.; Dindaroğlu, F. Displacement and Stress Distribution of Kilroy Spring and Nickel-Titanium Closed-Coil Spring during Traction of Palatally Impacted Canine: A 3-Dimensional Finite Element Analysis. Orthod. Craniofac. Res. 2020, 23, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Kommer, D.D.; McNeil, M.H.; Montagano, L.N.; Oesterle, L.J.; Youngquist, H.W. Management of Impacted Canines. Am. J. Orthod. 1976, 69, 371–387. [Google Scholar] [CrossRef] [PubMed]
- Bocchino, T.; Leone, C.; Moretti, R.; Rongo, R. “Canine First Technique”, An Innovative Approach in Maxillary Impacted Canines: A Case Report. Open Dent. J. 2022, 16, 1–7. [Google Scholar] [CrossRef]
- Leung, M.T.C.; Lee, T.C.; Rabie, A.B.M. Use of Miniscrews and Miniplates in Orthodontics. J. Oral Maxillofac. Surg. 2008, 66, 1461–1466. [Google Scholar] [CrossRef]
- Galluccio, G.; Impellizzeri, A.; Pietrantoni, A.; De Stefano, A.; La Monaca, G.; Pippi, R. The VISTA Approach in Canine Disimpaction. Methods Protoc. 2021, 4, 57. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) Design as a Framework to Formulate Eligibility Criteria in Systematic Reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Watson, P.F.; Petrie, A. Method Agreement Analysis: A Review of Correct Methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Critical Appraisal Tools for Use in JBI Systematic Reviews. Available online: https://jbi.global/critical-appraisal-tools (accessed on 14 December 2024).
- Giancotti, A.; Conigliaro, A.; Mampieri, G. Aligner Treatment of Transposed Maxillary Canines and Lateral Incisors. J. Clin. Orthod. 2021, 55, 34–43. [Google Scholar] [PubMed]
- Greco, M.; Machoy, M. Impacted Canine Management Using Aligners Supported by Orthodontic Temporary Anchorage Devices. Int. J. Environ. Res. Public Health 2022, 20, 131. [Google Scholar] [CrossRef] [PubMed]
- Mampieri, G.; Castroflorio, T.; Conigliaro, A.; Giancotti, A. Treatment of Impacted Canines with Aligners: An Alternative and Viable Option. Clin. Case Rep. 2021, 9, e04856. [Google Scholar] [CrossRef] [PubMed]
- Capuozzo, R.; Caruso, S.; Caruso, S.; De Felice, M.E.; Gatto, R. Canine Impaction: Digital Orthodontic Planning in Conjunction with TADs (Temporary Anchorage Devices) and Aligners. Appl. Sci. 2023, 13, 6914. [Google Scholar] [CrossRef]
- Memè, L.; Quinzi, V.; Coli, G.; Caciari, E.; Sampalmieri, F.; Gallusi, G. Unconventional Use of Invisalign® in the Treatment of Ectopic Palatal Maxillary Canines. Eur. J. Paediatr. Dent. 2024, 25, 61–68. [Google Scholar] [CrossRef]
- Bocchino, T.; Martina, S.; Sangiuolo, C.; Galdi, M.; Valletta, A.; D’Antò, V. Maxillary Impacted Canine and Upper Lateral Incisor Agenesis Treatment with “Canine First Technique” and Clear Aligners: A Case Report. Healthcare 2023, 11, 2345. [Google Scholar] [CrossRef]
- Xia, Q.; He, Y.; Jia, L.; Wang, C.; Wang, W.; Wang, C.; Song, J.; Fan, Y. Assessment of Labially Impacted Canines Traction Mode with Clear Aligners vs. Fixed Appliance: A Comparative Study Based on 3D Finite Element Analysis. Front. Bioeng. Biotechnol. 2022, 10, 1004223. [Google Scholar] [CrossRef]
- Palone, M.; Baciliero, M.; Cervinara, F.; Maino, G.B.; Paoletto, E.; Cremonini, F.; Lombardo, L. Class II Treatment of Transverse Maxillary Deficiency with a Single Bone-Borne Appliance and Hybrid Clear Aligner Approach in an Adult Patient: A Case Report. J. World Fed. Orthod. 2022, 11, 80–94. [Google Scholar] [CrossRef]
- Al-Motareb, F.; Al-Labani, M.; Al-Zubair, N.; Dhaifullah, E. Prevalence of Impacted Canine among Yemen Population in Sana’a City. Int. J. Dent. Res. 2017, 5, 148. [Google Scholar] [CrossRef]
- Rouzi, M.; Zhang, X.; Jiang, Q.; Long, H.; Lai, W.; Li, X. Impact of Clear Aligners on Oral Health and Oral Microbiome During Orthodontic Treatment. Int. Dent. J. 2023, 73, 603–611. [Google Scholar] [CrossRef]
- Elhaddaoui, R.; Qoraich, H.S.; Bahije, L.; Zaoui, F. Orthodontic Aligners and Root Resorption: A Systematic Review. Int. Orthod. 2017, 15, 1–12. [Google Scholar] [CrossRef]
- Castroflorio, T.; Sedran, A.; Parrini, S.; Garino, F.; Reverdito, M.; Capuozzo, R.; Mutinelli, S.; Grybauskas, S.; Vaitiekūnas, M.; Deregibus, A. Predictability of Orthodontic Tooth Movement with Aligners: Effect of Treatment Design. Prog. Orthod. 2023, 24, 2. [Google Scholar] [CrossRef]
- Kau, C.H.; Soh, J.; Christou, T.; Mangal, A. Orthodontic Aligners: Current Perspectives for the Modern Orthodontic Office. Medicina 2023, 59, 1773. [Google Scholar] [CrossRef] [PubMed]
- Kaklamanos, E.G.; Makrygiannakis, M.A.; Athanasiou, A.E. Oral Health-Related Quality of Life Throughout Treatment with Clear Aligners in Comparison to Conventional Metal Fixed Orthodontic Appliances: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3537. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, M.A.; Schroeder, D.K.; Capelli Júnior, J.; Santos, D.J.D.S. Orthodontic Traction of Impacted Maxillary Canines Using Segmented Arch Mechanics. Dent. Press J. Orthod. 2019, 24, 79–89. [Google Scholar] [CrossRef]
- Umalkar, S.S.; Jadhav, V.V.; Paul, P.; Reche, A. Modern Anchorage Systems in Orthodontics. Cureus 2022, 14, e31476. [Google Scholar] [CrossRef]
- Naoumova, J.; Kürol, J.; Kjellberg, H. Extraction of the Deciduous Canine as an Interceptive Treatment in Children with Palatally Displaced Canines—Part II: Possible Predictors of Success and Cut-Off Points for a Spontaneous Eruption. Eur. J. Orthod. 2015, 37, 219–229. [Google Scholar] [CrossRef]
- Koutzoglou, S.I.; Kostaki, A. Effect of Surgical Exposure Technique, Age, and Grade of Impaction on Ankylosis of an Impacted Canine, and the Effect of Rapid Palatal Expansion on Eruption: A Prospective Clinical Study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 342–352. [Google Scholar] [CrossRef]
- Sigler, L.M.; Baccetti, T.; McNamara, J.A., Jr. Effect of Rapid Maxillary Expansion and Transpalatal Arch Treatment Associated with Deciduous Canine Extraction on the Eruption of Palatally Displaced Canines: A 2-Center Prospective Study. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e235–e244. [Google Scholar] [CrossRef]
- Aragon, M.L.S.C.; Mendes Ribeiro, S.M.; Fernandes Fagundes, N.C.; Normando, D. Effectiveness of Dental Arch Expansion in the Orthodontic Treatment with Clear Aligners: A Scoping Review. Eur. J. Orthod. 2024, 46, cjae059. [Google Scholar] [CrossRef]
- Upadhyay, M.; Arqub, S.A. Biomechanics of clear aligners: Hidden truths & first principles. J. World Fed. Orthod. 2022, 11, 12–21. [Google Scholar] [CrossRef]
- Bilello, G.; Fazio, M.; Amato, E.; Crivello, L.; Galvano, A.; Currò, G. Accuracy evaluation of orthodontic movements with aligners: A prospective observational study. Prog. Orthod. 2022, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, R.; Liu, L.; Zhang, X.; Jiang, Q.; Fan, Q.; Zhang, H.; Long, H.; Lai, W. The effects of aligner anchorage preparation on mandibular first molars during premolar-extraction space closure with clear aligners: A finite element study. Am. J. Orthod. Dentofac. Orthop. 2023, 164, 226–238. [Google Scholar] [CrossRef]
- Becker, A.; Chaushu, G.; Chaushu, S. Analysis of failure in the treatment of impacted maxillary canines. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 743–754. [Google Scholar] [CrossRef]
- Lopatiene, K.; Dumbravaite, A. Risk factors of root resorption after orthodontic treatment. Stomatologija 2008, 10, 89–94. [Google Scholar]
- Smale, I.; Årtun, J.; Behbehani, F.; Doppel, D.; Hof, M.V.; Kuijpers-Jagtman, A.M. Apical root resorption 6 months after initiation of fixed orthodontic appliance therapy. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 57–67. [Google Scholar] [CrossRef]
- Li, Y.; Deng, S.; Mei, L.; Li, Z.; Zhang, X.; Yang, C.; Li, Y. Prevalence and severity of apical root resorption during orthodontic treatment with clear aligners and fixed appliances: A cone beam computed tomography study. Prog. Orthod. 2020, 21, 1–8. [Google Scholar] [CrossRef]
- Sawant, H.R.; Gangurde, P.V.; Shetty, N.S.; Sachdev, S.S.; Gaikwad, S.S.; Jadhav, S.M. Use of orthodontic mini-implants in conjunction with elastics for extrusion of impacted canines and correction of bimaxillary protrusion. J. Pharm. Bioallied Sci. 2024, 16, S2864–S2867. [Google Scholar] [CrossRef]
- Izadikhah, I.; Cao, D.; Zhao, Z.; Yan, B. Different management approaches in impacted maxillary canines: An overview on current trends and literature. J. Contemp. Dent. Pract. 2020, 21, 326–336. [Google Scholar] [CrossRef]
- Chaushu, S.; Chaushu, G.; Becker, A. Skeletal implant anchorage in the treatment of impacted teeth: A review of the state of the art. Semin. Orthod. 2010, 16, 234–241. [Google Scholar] [CrossRef]
- Maltha, J.C.; van Leeuwen, E.J.; Dijkman, G.E.; Kuijpers-Jagtman, A.M. Incidence and severity of root resorption in orthodontically moved premolars in dogs. Orthod. Craniofac. Res. 2004, 7, 115–121. [Google Scholar] [CrossRef]
- Giancotti, A.; Mampieri, G. Unilateral canine crossbite correction in adults using the Invisalign method. Orthodontics 2012, 13, 122–127. [Google Scholar] [PubMed]
- Cruz, R.M. Orthodontic traction of impacted canines: Concepts and clinical application. Dental Press J. Orthod. 2019, 24, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, M.; Cevidanes, L.; Sinfonico, G.; Drago, S.; Dalessandri, D.; Isola, G.; Biavati, A.S. Three dimensional movement analysis of maxillary impacted canine using TADs: A pilot study. Head Face Med. 2021, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alhamwi, A.M.; Burhan, A.S.; Idris, M.I.; Nawaya, F.R. Duration of orthodontic treatment with clear aligners versus fixed appliances in crowding cases: A systematic review. Clin. Oral Investig. 2024, 28, 249. [Google Scholar] [CrossRef]
- Flores-Mir, C. In mild to moderate crowded cases, is there a difference in orthodontic treatment duration between clear aligners and fixed appliances? Evid. Based Dent. 2024, 25, 136–137. [Google Scholar] [CrossRef]
- Zheng, M.; Liu, R.; Ni, Z.; Yu, Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2017, 20, 127–133. [Google Scholar] [CrossRef]
- Borda, A.F.; Garfinkle, J.S.; Covell, D.A.; Wang, M.; Doyle, L.; Sedgley, C.M. Outcome assessment of orthodontic clear aligner vs. fixed appliance treatment in a teenage population with mild malocclusions. Angle Orthod. 2020, 90, 485–490. [Google Scholar] [CrossRef]
- Shrivastava, A.; Mohanty, P.; Dash, B.P.; Jena, S.; Sahoo, N. Proficiency of clear aligner therapy: A systematic review and meta-analysis. Cureus 2023, 15, e45072. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Patients with impacted or significantly ectopic canines | - |
| Intervention | Orthodontic treatment carried out using aligner orthodontic therapy | Orthodontic treatment carried out without orthodontic aligners |
| Comparison | No comparison group was included | - |
| Outcomes | Any | Only tooth alignment after treatment |
| Study design | Any | Reviews, letters, editorials, commentaries, conference abstracts, books |
| Database | Search String |
|---|---|
| PubMed | (“Orthodontic aligner treatment” [All Fields] OR “Invisalign” [All Fields] OR “Clear aligner treatment”) AND (“Impacted Canine” [All Fields] OR “Impacted Tooth” [All Fields] OR “Ectopic Canine” [All Fields] OR “Ectopic Tooth” [All Fields]) |
| Google Scholar | “Orthodontic aligner treatment” OR “Invisalign” OR “ Clear aligner treatment” AND “Impacted Canine” OR “Impacted Tooth” OR “Ectopic Canine” OR “Ectopic Tooth” |
| EBSCO Complementary Index MEDLINE Ultimate Springer Nature Journals Oxford Medicine Online Academic Search Ultimate Dentistry and Oral Sciences Source Elsevier Web of Science | TS = (“Orthodontic aligner treatment” OR “Invisalign” OR “Clear aligner treatment”) AND TS = (“Impacted Canine” OR “Impacted Tooth” OR “Ectopic Canine” OR “Ectopic Tooth”) |
| Study | Group Size and Study Design | Patient Age | Patient Gender | Malposition of Canine | Period of Orthodontic Aligners Usage |
|---|---|---|---|---|---|
| Aldo Giancotti et al. 2021 [21] | 1; case study | 13 | Female | High vestibular ectopic transposition with lateral displacement and low exposition | Whole treatment |
| Qijan Xia et al. 2022 [27] | 1; 1 model was made into 4 3D finite models for 2 scenarios, 3D finite element analysis (FEA) | 23 | Male | Impacted in vestibular position, above premolar (scenario A) or above lateral incisor (scenario B) | Whole treatment |
| Mario Greco et al. 2022 [22] | 2; different cases with different sequences of the treatment | 16 and 43 | Male and female | Impacted palatally | In cases 1 and 2, whole treatment except for hybrid treatment during canine traction with TAD |
| Gianluca Mampieri et al. 2021 [23] | 1; case report | 17 | Female | Two slightly impacted in the alveolar crest | Whole treatment |
| Capuozzo R et al. 2023 [24] | 2; case 1 had palatally displaced canine and case 2 had buccally displaced canine | 17 and 18 | Female | Case 1: impacted palatally Case 2: highly vestibular | After short period of traction with TAD |
| Memè L et al. 2024 [25] | 1; case study | 13 | Female | Ectopic palatal with very low exposition | Whole treatment |
| Bocchino T et al. 2023 [26] | 1; case report | 19 | Male | Impacted palatally | 2nd phase of the treatment |
| Study | Treatment Protocol | TAD Use During Treatment | Usage of Fixed Orthodontic Appliance | Elastics Used | Aligner/Treatment Time |
|---|---|---|---|---|---|
| Aldo Giancotti et al. 2021 [21] | Resolve malocclusion and traction of ectopic canine into the arch, with the extraction of deciduous canine and two supernumeraries. Phase 1: Four months to create space for canines, with aligner changes every 2 weeks, then 5 months of canine traction with elastics. Phase 2: Residual canine extrusion and torque control, leveling the gingival anterior contour, with aligner changes every week. Phase 3: Class II correction with elastics and finishing. | No | No | Light auxiliary elastic stretched over the aligner between the palatal and buccal surfaces of the canine, then class II elastics to correct class II malocclusion and canine position. | 24 months of treatment: Phase 1: 40 aligners, 9 months; Phase 2: 27 aligners, 3 months; Phase 3: 8 aligners, 12 months; Total: 67 aligners. |
| Qijan Xia et al. 2022 [27] | Finite element models were created from a male model, including the maxillary dentition with maxilla, periodontal ligaments, clear aligners, traction attachments, and right labial canine. Two scenarios were investigated: impacted canine above the premolar vestibular (A) and impacted canine impacted above the lateral incisor vestibular (B). Three traction models with clear aligners and one fixed appliance model were created for every scenario. Traction was performed with 0.6N elastics from the canine to the attached auxiliary (7 mm power arm, 3D attachment, or Angel Button on aligners and hook on fixed appliance). ABAQUS software (version 6.14; SIMULIA, Aix-en-Provence, France) was used for nonlinear iterative calculations. | No | Control scenario: 0.018 × 0.025 stiff wire. | Straight to the auxiliary (power arm, button, or 3D-printed “hook like” attachment). | Due to the characteristics of the FEA study, neither the treatment time nor number of aligners were the subject of the calculations. |
| Mario Greco et al. 2022 [22] | Case 1: Phase 1: Correcting malocclusion and recreating space for the impacted canine with aligners. Phase 2: Surgical exposure and canine disimpaction and traction using TADs and sectional wires. Phase 3: Refinement of canine position and finishing. Case 2: Phase 1: Canine-first technique with surgical exposure, disimpaction of canine with TADs and sectional wires, and displacement of the TAD during treatment. Phase 2: Final correction of canine position and torque with aligners, and finalization of wire extrusion. | Case 1: Palatally between premolars and the premolar and molar. Case 2: Mesially from 1st molar in the palate later in the vestibule between canine and 1st premolar. | Case 1: During canine traction, a sectional 0.18SS Australian wire was used from the canines to the TADs. Then, to not reposition them, a 0.17 × 0.25 TMA was used from the 2.5 to the canine labially. Case 2: During canine traction, a 150 g closed coil spring with a metal ligature was used from the canine to the TAD. For finishing, a sectional 0.016 × 0.022 CuNiTi wire from the lateral to the 1st premolar was used. | Triangular criss-cross. | Case 1: 18 months of treatment: Phase 1: 25 aligners; Phase 2: TAD and sectional wire; Phase 3: 18 aligners; Total: 43 aligners. Case 2: Approximately 24 months of treatment: Phase 1: TAD + sectional wire; Phase 2: 38 aligners + sectional wire; Total: 38 aligners. |
| Gianluca Mampieri et al. 2021 [23] | Phase 1 was aimed at recovering space in the arch for canines, expansion, and the correction of incisor inclination. Phase 2 included deciduous canine removal, surgical exposure of both canines, and cuspid traction with elastic forces from the canines to the aligner and eruption guides. Phase 3 included residual positioning of canines and finishing for better esthetic and occlusal outcomes. | No | No | Intra-arch 6 mm/180 g elastics from canine hooks to buttons hidden inside pontics over the aligners, then replaced with buttons on canines, dovetail hook on aligners and 4 mm/180 g elastics. | 18 months of treatment: Phase 1: 21 aligners; Phase 2: 17 aligners; Phase 3: 13 aligners; Total: 61 aligners. |
| Capuozzo R et al. 2023 [24] | Case 1: Phase 1: Surgical exposure of canines, traction of impacted canines using TAD and sectional wire in cantilever spring (canine-first technique), and then extraction of the deciduous one. Phase 2: Use of aligners with bite ramps for leveling and alignment of both arches, and traction of canines with elastics. Phase 3: Residual canine traction and torque, followed by finishing. Case 2: Phase 1: Surgical exposure of canines, extraction of deciduous canines, and traction using TAD with cantilever spring (canine-first technique). Phase 2: Aligners used for space creation with eruption compensator, alignment, and leveling of both arches; class II elastics used to improve occlusion and canine traction. Phase 3: Aligners used for expansion to resolve crowding and transverse discrepancy, followed by torquing and final positioning of the canine. | Case 1: Palatally between 1.5 and 1.6. Case 2: Between 2.5 and 2.6 buccally. | Case 1: A 0.017 x 0.025 TMA 50 g cantilever spring was used from the canine to the TAD. Case 2: A 0.018 × 0.025 TMA 50 g cantilever spring from the TAD to the canine was used. | Case 1: Elastic ligature from the canine to the eruption compensator. Case 2: From the canine to 3.6, class II elastics and later, wrap around aligner elastics to a buccal button on the canine. | Case 1: 20 months of treatment: Phase 1: TAD + sectional wire; Phases 2 and 3: Approx 52 aligners (14 months). Case 2: 18 months of treatment: Phase 1: TAD + sectional wire; Phases 2 and 3: Approx 48 aligners (12 months). |
| Memè L et al. 2024 [25] | Phase 1: Upper arch expansion to make space for canines with pontics. Phase 2: Increase in posterior vertical dimension through fake build-ups implemented in aligners, followed by canine traction. Phase 3: Occlusion refinement, short class II for better canine position, and mesial derotation of molars. | No | No | Class II elastics with a size of 3/16” and 4.5 ounces were used from the canines to the lower premolars. | 21 months of treatment: Phase 1: 7 aligners; Phase 2: 31 aligners; Phase 3: 26 aligners; Total: 64 aligners. |
| Bocchino T et al. 2023 [26] | Phase 1: Canine-first approach; this procedure included surgical disimpaction of the canine, moving the crown away from the roots of the adjacent incisors with a cantilever and a skeletal anchorage (TAD). Phase 2: Canine traction with Alastik to 5.3 and composite ramping. Phase 3: Extraction of 5.3, sectional brackets on 1.6 and 1.3 with a cantilever for canine traction and torque. Phase 4: Alignment and mesialization of posterior segments and the canine into absent lateral incisor with aligners, followed by class III elastics to promote desired movements. | Between 2nd premolar and 1st molar palatally. | A 0.019 x 0.025 TMA 100 g cantilever spring from the TAD to the canine was used, with a bracket on 1.6 with the TAD for additional anchorage. A 0.019 × 0.025 TMA cantilever was used on the canine vestibular, followed by a bracket on the canine. | Alastik from 53 to 13 during the second course of traction, followed by class III on the canines during aligner treatment. | 14 months + phase 3 treatment time; Phase 1: TAD + sectional wire (3 months); Phase 2: Alastik from 53 to 13 (4 months); Phase 3: Sectional wire bonded on 16 and 13 + TAD; Phase 4: 24 aligners (7 months). |
| Checklist Question | Aldo Giancotti et al. [21] | Mario Greco et al. [22] | Gianluca Mampieri et al. [23] | Capuozzo R et al. [24] | Memè L et al. [25] | Bocchino T et al. [26] |
|---|---|---|---|---|---|---|
| Were the patient’s demographic characteristics clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the patient’s history clearly described and presented as a timeline? | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the current clinical condition of the patient upon presentation clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
| Were diagnostic tests or assessment methods and the results clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the intervention(s) or treatment procedure(s) clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the post-intervention clinical condition clearly described? | Yes | Yes | Yes | Yes | Yes | Yes |
| Were adverse events (harms) or unanticipated events identified and described? | No | No | No | No | No | No |
| Does the case report provide takeaway lessons? | Yes | Yes | Yes | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolny, M.; Sikora, A.; Olszewska, A.; Matys, J.; Czajka-Jakubowska, A. Aligners as a Therapeutic Approach in Impacted Canine Treatment: A Systematic Review. J. Clin. Med. 2025, 14, 3421. https://doi.org/10.3390/jcm14103421
Wolny M, Sikora A, Olszewska A, Matys J, Czajka-Jakubowska A. Aligners as a Therapeutic Approach in Impacted Canine Treatment: A Systematic Review. Journal of Clinical Medicine. 2025; 14(10):3421. https://doi.org/10.3390/jcm14103421
Chicago/Turabian StyleWolny, Mateusz, Agata Sikora, Aneta Olszewska, Jacek Matys, and Agata Czajka-Jakubowska. 2025. "Aligners as a Therapeutic Approach in Impacted Canine Treatment: A Systematic Review" Journal of Clinical Medicine 14, no. 10: 3421. https://doi.org/10.3390/jcm14103421
APA StyleWolny, M., Sikora, A., Olszewska, A., Matys, J., & Czajka-Jakubowska, A. (2025). Aligners as a Therapeutic Approach in Impacted Canine Treatment: A Systematic Review. Journal of Clinical Medicine, 14(10), 3421. https://doi.org/10.3390/jcm14103421