
Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Incomplete Detailed Fetal Anatomy Exams


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Extraction and Inclusion and Exclusion Criteria
2.3. Definitions of Inadequate Views and Incomplete Examination
- Normal if the item was entered as normal or previously documented, seen or visualized;
- Abnormal if it was entered as abnormal, a soft marker was seen or details were provided;
- Inadequate if it was entered as suboptimal, not seen or not examined, or if left blank.
2.4. Statistical Analyses
3. Results
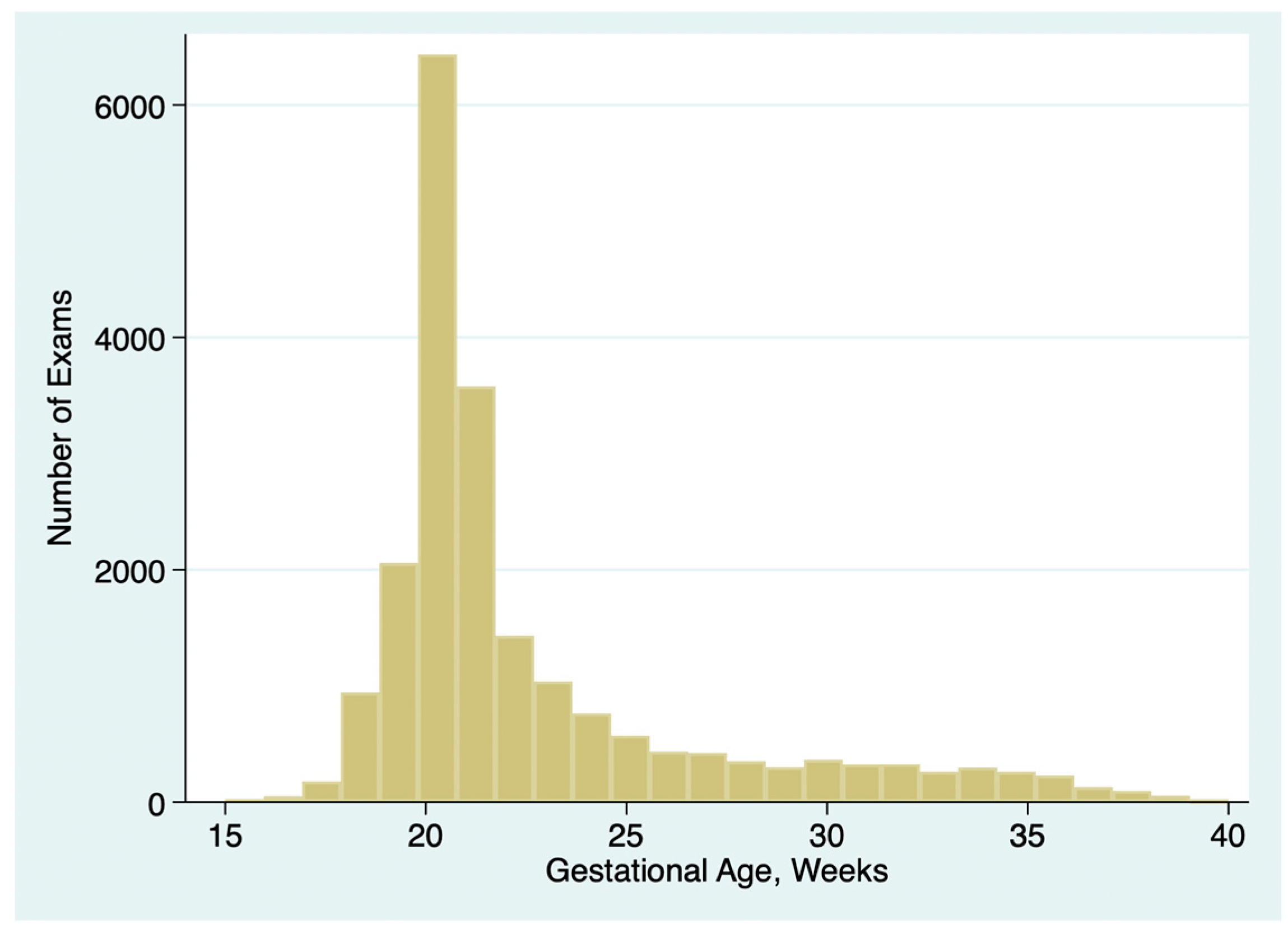
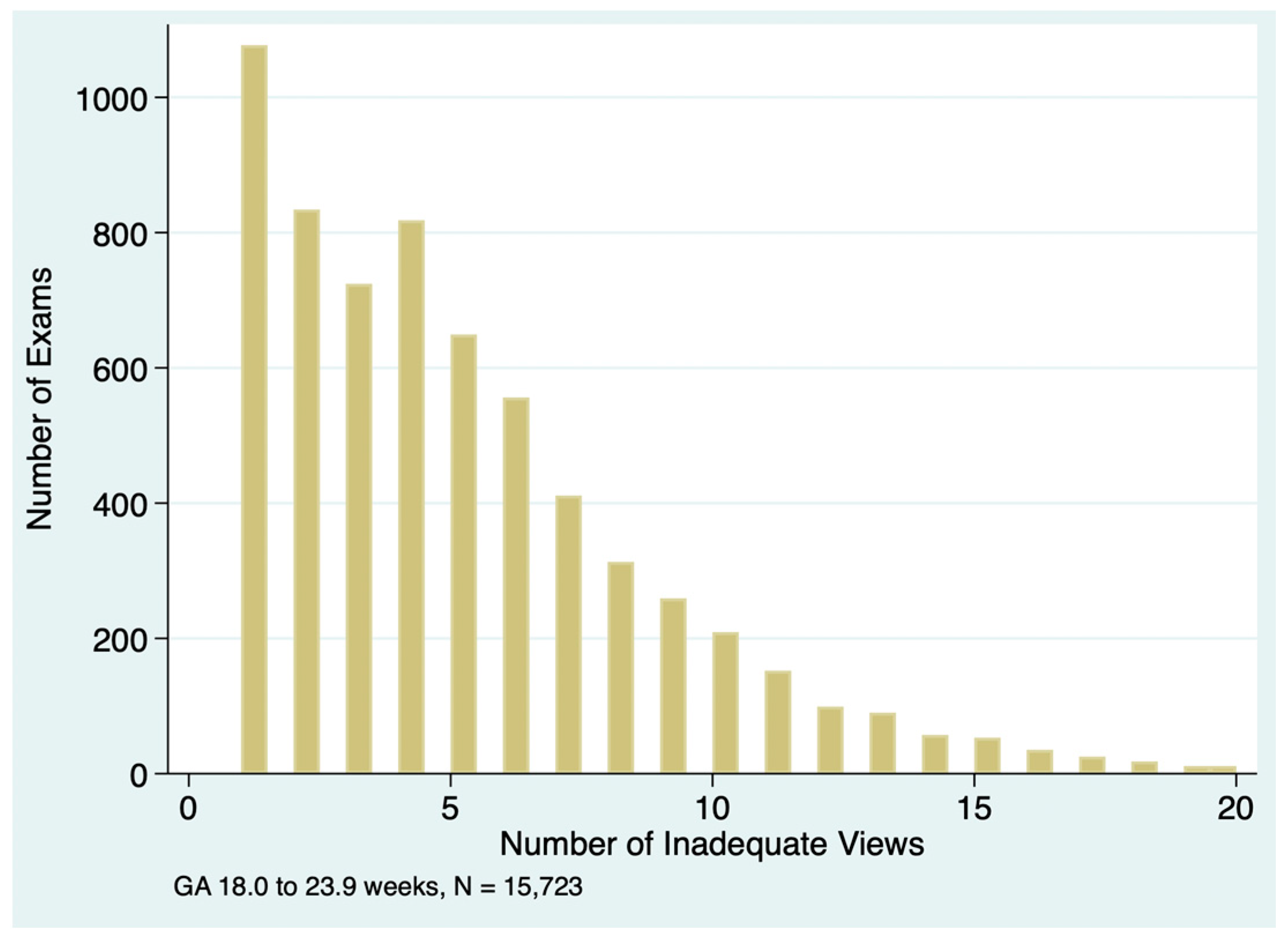
3.1. Included Exams and Gestational Age Considerations
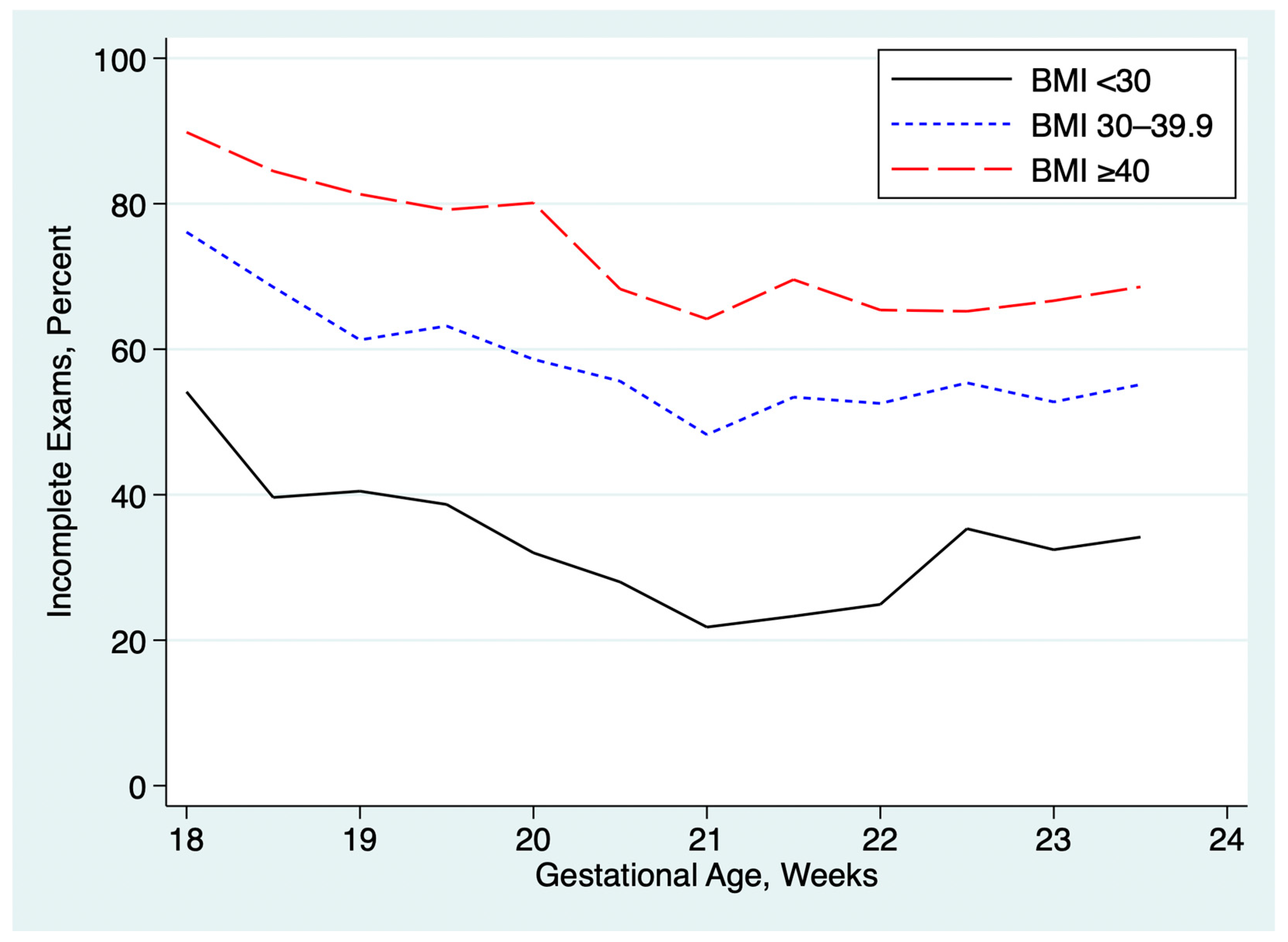
3.2. Clinical Factors Associated with Incomplete Exams
3.3. Practice-Level Variation in Exam Completeness
3.4. Sonographer-Level Variation in Exam Completeness
3.5. Physicain-Level Variation in Exam Completeness
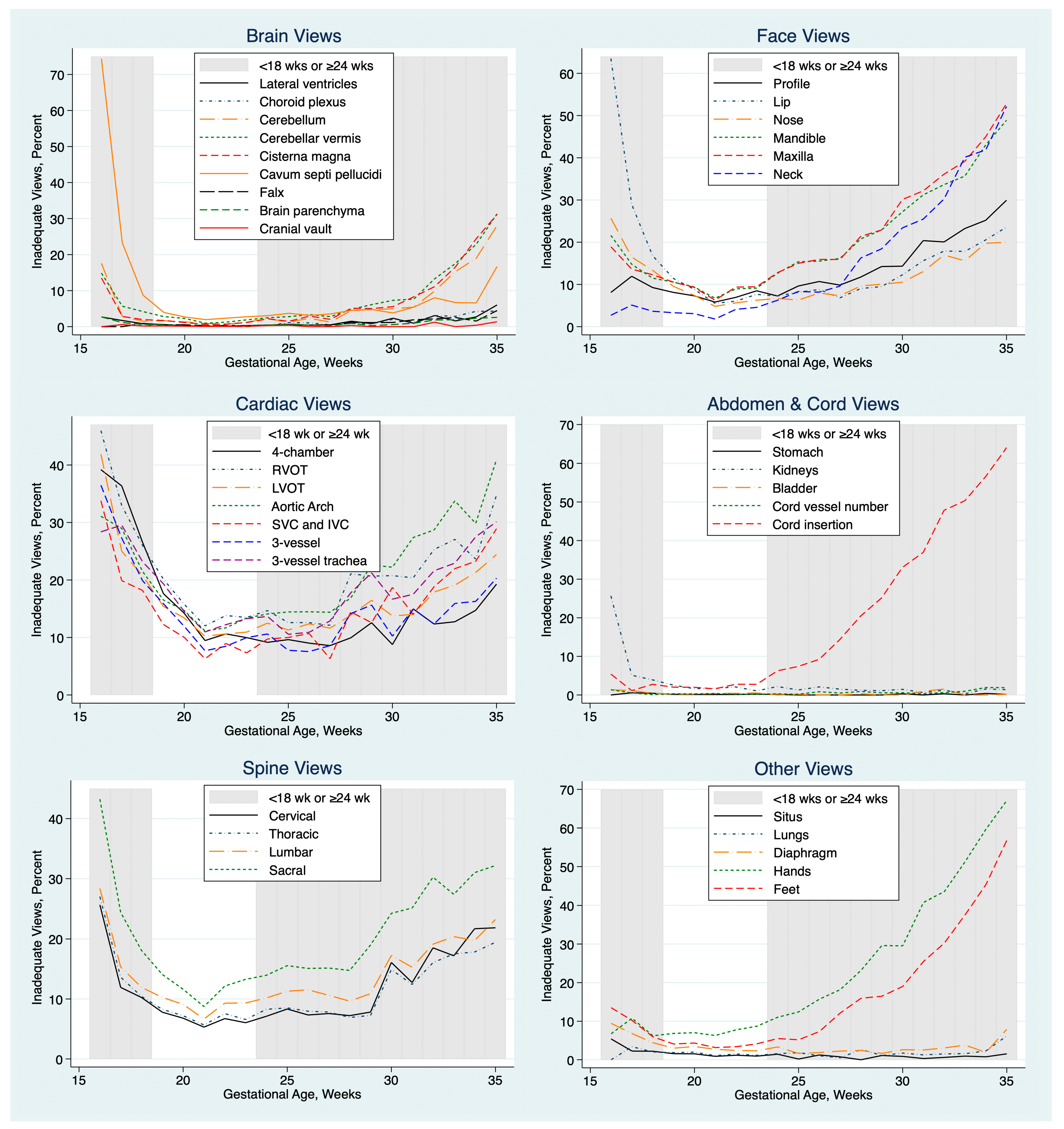
3.6. Focused Review of Inadequate Elements by Selected Examiners
4. Discussion
4.1. Principal Findings
4.2. Clinical Consequences of Incomplete Exams
4.3. Ideal Rate of Incomplete Exams
4.4. Possible Strategies to Reduce the Rate of Incomplete Exams
4.5. Evaluation of Individual-Level Variance
4.6. Strengths and Limitations
4.7. Future Directions—Software Enhancements
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AC | Abdominal circumference (fetal) |
| AIUM | American Institute of Ultrasound in Medicine |
| BMI | Body mass index |
| BPD | Biparietal diameter (fetal) |
| DOB | Date of birth (maternal) |
| EDD | Estimated date of delivery (date when gestational age = 40 weeks) |
| FL | Femur length (fetal) |
| GA | Gestational age |
| HC | Head circumference (fetal) |
| IQR | Interquartile range |
| SD | Standard deviation |
References
- AIUM. Practice parameter for the performance of standard diagnostic obstetric ultrasound. J. Ultrasound Med. 2024, 43, E20–E32. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1002/jum.16406 (accessed on 2 May 2025).
- American Institute of Ultrasound in Medicine. Case Study Submission Requirements: Detailed 2nd Trimester OB (Includes OB Standard), Updated 7/24/24. Available online: https://www.aium.org/docs/default-source/accreditation/case-study-requirements/76811.pdf (accessed on 2 May 2025).
- Lantz, M.E.; Chisholm, C.A. The Preferred Timing of Second-Trimester Obstetric Sonography Based on Maternal Body Mass Index. J. Ultrasound Med. 2004, 23, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Thornburg, L.L.; Miles, K.; Ho, M.; Pressman, E.K. Fetal anatomic evaluation in the overweight and obese gravida. Ultrasound Obstet. Gynecol. 2009, 33, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Padula, F.; Gulino, F.A.; Capriglione, S.; Giorlandino, M.; Cignini, P.; Mastrandrea, M.L.; Laura, D.; Giorlandino, C. What is the rate of incomplete fetal anatomic surveys during a second-trimester scan? Retrospective observational study of 4000 noonobese pregnant women. J. Ultrasound Med. 2014, 34, 2187–2191. [Google Scholar] [CrossRef]
- Pasko, D.N.; Wood, S.L.; Jenkins, S.M.; Owen, J.; Harper, L.M. Completion and Sensitivity of the Second-Trimester Fetal Anatomic Survey in Obese Gravidas. J. Ultrasound Med. 2016, 35, 2449–2457. [Google Scholar] [CrossRef]
- Silvestri, M.T.; Pettker, C.M.; Raney, J.H.; Xu, X.; Ross, J.S. Frequency and Importance of Incomplete Screening Fetal Anatomic Sonography in Pregnancy. J. Ultrasound Med. 2016, 35, 2665–2673. [Google Scholar] [CrossRef]
- O’Brien, K.; Shainker, S.A.; Modest, A.M.; Spiel, M.H.; Resetkova, N.; Shah, N.; Hacker, M.R. Cost Analysis of Following Up Incomplete Low-Risk Fetal Anatomy Ultrasounds. Birth 2016, 44, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.L.; Owen, J.; Jenkins, S.M.; Harper, L.M. The Utility of Repeat Midtrimester Anatomy Ultrasound for Anomaly Detection. Am. J. Perinatol. 2018, 35, 1346–1351. [Google Scholar] [CrossRef]
- Simmons, P.M.; Wendel, M.P.; Whittington, J.R.; San Miguel, K.; Ounpraseuth, S.T.; Magann, E.F. Accuracy and completion rate of the fetal anatomic survey in the super obese parturient. J. Ultrasound Med. 2021, 40, 2047–2051. [Google Scholar] [CrossRef]
- Gross, M.S.; Ju, H.; Osborne, L.M.; Jelin, E.B.; Sekar, P.; Jelin, A.C. Indeterminate Prenatal Ultrasounds and Maternal Anxiety: A Prospective Cohort Study. Matern. Child Health J. 2021, 25, 802–812. [Google Scholar] [CrossRef]
- Waller, S.A.; O’connell, K.; Carter, A.; Gravett, M.G.; Dighe, M.; Richardson, M.L.; Dubinsky, T.J. Incidence of Fetal Anomalies After Incomplete Anatomic Surveys Between 16 and 22 Weeks. Ultrasound Q. 2013, 29, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Adekola, H.; Soto, E.; Dai, J.; Lam-Rachlin, J.; Gill, N.; Leon-Peters, J.; Puder, K.; Abramowicz, J.S. Optimal visualization of the fetal four-chamber and outflow tract views with transabdominal ultrasound in the morbidly obese: Are we there yet? J. Clin. Ultrasound. 2015, 43, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, K.-A.; Daly, C.; Hunter, A.; McCance, D.; Young, I.; Holmes, V. The impact of maternal obesity on completion of fetal anomaly screening. J. Perinat. Med. 2017, 45, 1061–1067. [Google Scholar] [CrossRef]
- Lendrum, T.L.; Shaffer, R.K.; Heyborne, K.D. Repeat anatomic surveys performed for an initial incomplete study: The sonographer and physician factors. Am. J. Obstet. Gynecol. MFM 2022, 4, 100567. [Google Scholar] [CrossRef]
- Buskmiller, C.; Huntley, E.; Blackburn, B.; Sanchez, D.; Hernandez-Andrade, E. Completion of fetal anaomy evaluations in women with doy mass index ≥50 kg/m2. J. Ultrasound Med. 2023, 42, 2839–2844. [Google Scholar] [CrossRef]
- Ashimi Balogun, O.; Behnia, F.; Chelliah, A.; Luo, J.; Chauhan, S.P.; Samuel, A. 381 Comprehensive Detailed Anatomic Ultrasound: Allotted Time of 30- vs 45-Minutes. Am. J. Obstet. Gynecol. 2024, 230, S212–S213. [Google Scholar] [CrossRef]
- Benacerraf, B.R.; Minton, K.K.; Benson, C.B.; Bromley, B.S.; Coley, B.D.; Doubilet, P.M.; Lee, W.; Maslak, S.H.; Pellerito, J.S.; Perez, J.J.; et al. Proceedings: Beyond Ultrasound First Forum on improving the quality of ultrasound imaging in obstetrics and gynecology. Am. J. Obstet. Gynecol. 2018, 218, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine (SMFM); Stone, J.; Bromley, B.; Norton, M.E.; Feltovich, H.; Platt, L.D.; Copel, J.A.; Abu-Rustum, R.S.; Perez, M.; Connolly, K.; et al. Developing an optimal maternal-fetal medicine ultrasound practice: A report and recommendations of the workshop of the Society for Maternal-Fetal Medicine. Pregnancy 2025, 1. [Google Scholar] [CrossRef]
- American Institute of Ultrasound in Medicine. Standards and Guidelines for the Accreditation of Ultrasound Practices. Available online: https://www.aium.org/resources/official-statements/view/standards-and-guidelines-for-the-accreditation-of-ultrasound-practices (accessed on 2 May 2025).
- American College of Radiology. Physician QA Requirements: CT, MRI, Nuclear Medicine/PET, Ultrasound (Revised 3-4-2025). Available online: https://accreditationsupport.acr.org/support/solutions/articles/11000068451-physician-qa-requirements-ct-mri-nuclear-medicine-pet-ultrasound-revised-9-7-2021- (accessed on 2 May 2025).
- Combs, C.A.; Amara, S.; Kline, C.; Ashimi Balogun, O.; Bowman, Z.S. Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Fetal Biometry. J. Clin. Med. 2024, 13, 4860. [Google Scholar] [CrossRef]
- Combs, C.A.; Lee, R.C.; Lee, S.Y.; Amara, S.; Ashimi Balogun, O. Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Estimated Fetal Weight and Fetal Sex. J. Clin. Med. 2024, 13, 6895. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologist; American Institute of Ultrasound in Medicine; Society for Maternal-Fetal Medicine. Methods for Estimating the due date. Committee Opinion number 700. American College of Obstetricians and Gynecologists. Obs. Gynecol. 2017, 129, e150–e154. [Google Scholar] [CrossRef]
- NHS England. Public Health Functions to Be Exercised by NHS England. Available online: https://assets.publishing.service.gov.uk/media/5a759b7be5274a545822cd2e/17_nhs_fetal_anomaly.pdf (accessed on 2 May 2025).
- Reddy, U.M.; Abuhamad, A.Z.; Levine, D.; Saade, G.R. Fetal imaging: Executive summary of a joint Eunice Kennedy Shriver National Intitue of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Institute of Ultrasound in Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of Radiologists in Ultrasound Fetal Imaging Workshop. Am. J. Obs. Gynecol. 2014, 210, 387–397. [Google Scholar]
- Cargill, Y.; Morin, L. No. 223–Content of a complete routine second trimester obstetrical ultrasound examination and report. J. Obs. Gynecol. Can. 2017, 39, e144–e149. [Google Scholar] [CrossRef]
- Salomon, L.J.; Alfirevic, Z.; Berghella, V.; Bilardo, C.M.; Chalouhi, G.E.; Da Silva Costa, F.; Hernandez-Andrade, E.; Malinger, G.; Munoz, H.; Paladini, D.; et al. ISUOG Practice Guidelines (updated): Performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obs. Gynecol. 2022, 59, 840–856. [Google Scholar]
- Hendler, I.; Blackwell, S.C.; Bujold, E.; Treadwell, M.C.; Mittal, P.; Sokol, R.J.; Sorokin, Y. Suboptimal Second-Trimester Ultrasonographic Visualization of the Fetal Heart in Obese Women. J. Ultrasound Med. 2005, 24, 1205–1209. [Google Scholar] [CrossRef]
- Byrne, J.J.; Morgan, J.L.; Twickler, D.M.; McIntire, D.D.; Dashe, J.S. Utility of follow-up standard sonography for fetal anomaly detection. Am. J. Obstet. Gynecol. 2020, 222, 615.e1–615.e9. [Google Scholar] [CrossRef]
- Song, Y.; Skinner, J.; Bynum, J.; Sutherland, J.; Wennberg, J.E.; Fisher, E.S. Regional Variations in Diagnostic Practices. N. Engl. J. Med. 2010, 363, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Agathathakleous, M.; Chaveeva, P.; Poon, L.C.Y.; Kosinski, P.; Nicolaides, K.H. Meta-analysis of second-trimester markers for trisomy 21. Ultrasound Obs. Gynecol. 2013, 41, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Kataguiri, M.R.; Júnior, E.A.; Bussamra, L.C.S.; Nardozza, L.M.M.; Moron, A.F. Influence of Second-Trimester Ultrasound Markers for Down Syndrome in Pregnant Women of Advanced Maternal Age. J. Pregnancy 2014, 2014, 785730. [Google Scholar] [CrossRef] [PubMed]
- Benacerraf, B.R.; A Laboda, L.; Frigoletto, F.D. Thickened nuchal fold in fetuses not at risk for aneuploidy. Radiology 1992, 184, 239–242. [Google Scholar] [CrossRef]
- Li, L.; Fu, F.; Li, R.; Liu, Z.; Liao, C. Prenatal diagnosis and pregnancy outcome analysis of thickened nuchal fold in the second trimester. Medicine 2018, 97, e13334. [Google Scholar] [CrossRef]
- Kievskaya, J.K.; Shilova, N.V.; Kaniets, I.V.; Kudryavtseva, E.V.; Pyankov, D.V.; Korostelev, S.A. SNP-based chromosomal microarray analysis for detecting DNA copy number variations in fetuses with a thickened nuchal fold. Sovrem. Tehnol. V Med. 2021, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Wu, J.; Liang, D.; Yuan, J.; Wang, J.; Shen, Y.; Lu, J.; Xia, A.; Li, J.; Wu, L. Association analysis between chromosomal abnormalities and fetal ultrasonographic soft markers based on 15,263 fetuses. Am. J. Obstet. Gynecol. MFM 2023, 5, 101072. [Google Scholar] [CrossRef] [PubMed]
- Moczulska, H.; Serafin, M.; Wojda, K.; Borowiec, M.; Sieroszewski, P. Fetal Nasal Bone Hypoplasia in the Second Trimester as a Marker of Multiple Genetic Syndromes. J. Clin. Med. 2022, 11, 1513. [Google Scholar] [CrossRef] [PubMed]
- Cusick, W.; Provenzano, J.; Sullivan, C.A.; Gallousis, F.M.; Rodis, J.F. Fetal Nasal Bone Length in Euploid and Aneuploid Fetuses Between 11 and 20 Weeks' Gestation. J. Ultrasound Med. 2004, 23, 1327–1333. [Google Scholar] [CrossRef]
- Buijtendijk, M.F.; Bet, B.B.; Leeflang, M.M.; Shah, H.; Reuvekamp, T.; Goring, T.; Docter, D.; Timmerman, M.G.; Dawood, Y.; A Lugthart, M.; et al. Diagnostic accuracy of ultrasound screening for fetal structural abnormalities during the first and second trimester of pregnancy in low-risk and unselected populations. Cochrane Database Syst. Rev. 2024, CD014715. [Google Scholar] [CrossRef]
- Yehudit, Z.; Rachel, M.-C.; Ari, W.; Ori, S.; Eyal, M.; Yitzhak, S.H. Detection Rate of Fetal Anomalies in Early Mid-Trimester Compared to Late Mid-Trimester Detailed Scans: Possible Implications for First-Trimester Sonography. J. Clin. Med. 2024, 13, 5750. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | AIUM Item Number | Normal % | Abnormal n (%) | Inadequate % |
|---|---|---|---|---|
| Situs | 6 | 98.6% | 6 (0.04%) | 1.4% |
| Lateral cerebral ventricles | 8 | 99.2% | 71 (0.45%) | 0.3% |
| Choroid plexus | 9 | 99.2% | 91 (0.58%) | 0.3% |
| Midline falx | 10 | 99.5% | 12 (0.08%) | 0.45% |
| Brain parenchyma | 11 | 99.7% | 14 (0.09%) | 0.2% |
| Cerebellum | 15 | 98.5% | 39 (0.25%) | 1.2% |
| Cerebellar vermis including 4th ventricle | 16 | 97.8% | 22 (0.14%) | 2.1% |
| Cisterna magna | 17 | 98.7% | 19 (0.12%) | 1.2% |
| Cavum septi pellucidi | 18 | 96.7% | 25 (0.16%) | 3.1% |
| Cranial vault, integrity and shape | 19 | 99.7% | 26 (0.17%) | 0.1% |
| Profile (mid-sagittal) | 20 | 92.3% | 55 (0.35%) | 7.3% |
| Upper lip (coronal view) | 21 | 91.0% | 27 (0.17%) | 8.8% |
| Nose (coronal view) | 22 | 92.4% | 38 (0.24%) | 7.4% |
| Maxilla (axial view) | 24 | 90.8% | 8 (0.05%) | 9.1% |
| Mandible (axial view) | 25 | 90.8% | 3 (0.02%) | 9.1% |
| Neck | 26 | 96.8% | 3 (0.02%) | 3.1% |
| Lungs | 28 | 98.2% | 16 (0.10%) | 1.7% |
| Diaphragm | 29 | 96.8% | 13 (0.08%) | 3.1% |
| Hands | 31 | 92.9% | 21 (0.13%) | 7.0% |
| Feet | 32 | 95.6% | 57 (0.36%) | 4.1% |
| Stomach | 33 | 99.7% | 25 (0.16%) | 0.2% |
| Kidneys | 34 | 95.5% | 401 (2.6%) | 1.8% |
| Urinary bladder | 35 | 99.6% | 8 (0.05%) | 0.3% |
| Umbilical cord, number of vessels | 36 | 98.7% | 159 (1.01%) | 0.3% |
| Umbilical cord, insertion into abdomen | 37 | 97.8% | 12 (0.08%) | 2.1% |
| 4-chamber view of heart | 39 | 84.8% | 177 (1.13%) | 14.1% |
| Right outflow tract | 40 | 83.7% | 34 (0.22%) | 16.1% |
| Left outflow tract | 41 | 86.1% | 64 (0.41%) | 13.2% |
| Aortic arch (sagittal view) | 42 | 85.4% | 32 (0.20%) | 14.4% |
| Superior and inferior vena cavae | 43 | 90.0% | 19 (0.12%) | 9.9% |
| 3-vessel view | 44 | 87.8% | 57 (0.36%) | 11.8% |
| 3-vessel trachea view | 45 | 84.8% | 56 (0.36%) | 14.9% |
| Cervical spine | 47 | 93.1% | 5 (0.03%) | 6.8% |
| Thoracic spine | 48 | 92.5% | 8 (0.05%) | 7.3% |
| Lumbar spine | 49 | 90.8% | 18 (0.11%) | 9.0% |
| Sacral spine | 50 | 87.9% | 16 (0.10%) | 12.0% |
| Characteristic | Incomplete Exams, n/N (%) | Univariable Odds Ratio (95% Confidence Interval) | Multivariable Odds Ratio (95% Confidence Interval) |
|---|---|---|---|
| Maternal obesity § | |||
| BMI < 30 kg/m2 | 3424/10,918 (31.2%) | Referent | -- |
| BMI ≥ 30 kg/m2 | 2992/4805 (62.3%) | 3.61 (3.36–3.88) | 3.56 (3.32–3.83) |
| Gestational age § | |||
| 18.0–18.9 weeks | 640/1122 (57.0%) | 2.03 (1.79–2.29) | 2.11 (1.86–2.40) |
| 19.0–23.9 weeks | 5776/14,601 (39.6%) | Referent | -- |
| Prior cesarean § | |||
| Yes | 1231/2616 (47.1%) | 1.36 (1.25–1.48) | 1.22 (1.11–1.33) |
| No | 5285/13,107 (39.6%) | Referent | -- |
| Maternal age § | |||
| <35 years | 4443/10,561 (42.2%) | Referent | -- |
| ≥35 years | 1973/5182 (38.1%) | 0.84 (0.79–0.90) | 0.89 (0.83–0.95) |
| Practice 1 | Practice 2 | Practice 3 | Practice 4 | Practice 5 | Practice 6 | Practice 7 | Total | |
|---|---|---|---|---|---|---|---|---|
| Exams at GA 18.0 to 23.9 weeks | ||||||||
| Number of anatomy exams | 235 | 8303 | 1396 | 513 | 724 | 1534 | 3018 | 15,723 |
| Incomplete exams, % | 1.3% † | 52.7% † | 37.0% † | 37.2% † | 30.5% † | 49.7% † | 11.4% † | 41% |
| Number of inadequate views | ||||||||
| in incomplete exams, | 2 (1–5) | 4 (2–7) | 3 (2–5) | 4 (2–6) | 3 (1–5) | 5 (2–8) | 4 (2–6) | 4 (2–7) |
| median (interquartile range) § | ||||||||
| Exams with ≥1 abnormal | 1.7% | 7.2% | 10.0% | 9.8% | 5.5% | 7.0% | 5.2% | 7.0% |
| anatomy view, % ‡ | ||||||||
| Exams at GA ≤ 20.0 weeks | ||||||||
| Number of exams | 64 | 2969 | 493 | 244 | 433 | 698 | 268 | 5169 |
| Nuchal fold not measured, % ‡ | 9.4% | 3.3% | 5.7% | 1.6% | 0.7% | 0.6% | 0 | 2.8% |
| Exams at GA ≤ 22.0 weeks | ||||||||
| Number of exams | 204 | 7023 | 1077 | 406 | 646 | 1433 | 2860 | 13,649 |
| Nasal bone not measured, % ‡ | 100% | 19.2% | 40.7% | 9.9% | 91.5% | 56.1% | 63.7% | 38.4% |
| Sonographer | Incomplete Anatomy Exams, n/N (%) | Number of Inadequate Views If Anatomy Incomplete, Median (IQR) † | Nuchal Fold Not Measured at 18.0–20.0 Weeks, n/N (%) | Nasal Bone Not Measured at 18.0–22.0 Weeks, n/N (%) |
|---|---|---|---|---|
| Sonographer 1 | 44/317 (13.8%) ‡ | 2 (1–5) | 0/92 (0%) | 13/265 (4.9%) § |
| Sonographer 2 | 70/348 (20.1%) ‡ | 2 (1–4) | 1/105 (1%) | 16/284 (5.6%) § |
| Sonographer 3 | 106/256 (41.4.6%) ‡ | 3 (2–5) | 2/70 (3%) | 44/223 (19.7%) |
| Sonographer 4 | 127/269 (47.2%) | 5 (3–7) | 2/84 (2%) | 20/219 (9.1%) § |
| Sonographer 5 | 76/156 (48.7%) | 2 (1–6) | 3/58 (5%) | 76/132 (57.6%) § |
| Sonographer 6 | 184/300 (61.3%) ‡ | 5 (3–7) | 11/113 (10%) § | 48/257 (28.7%) |
| Sonographer 7 | 104/157 (66.2%) ‡ | 4 (2–7) | 9/56 (16%) § | 32/133 (24.1%) |
| Sonographer 8 | 209/275 (76.0%) ‡ | 5 (3–7) | 0/104 (0%) § | 28/246 (11.4%) § |
| Sonographer 9 | 248/310 (80.0%) ‡ | 6 (3–8) | 3/97 (3%) | 259/261 (99.2%) § |
| Sonographer 10 | 267/321 (83.2%) ‡ | 4 (2–7) | 0/83 (0%) | 136/264 (51.3%) § |
| Practice Total | 4379/8303 (52.7%) | 4 (2–7) | 99/2969 (3.3%) | 1346/7023 (19.2%) |
| Physicians | Incomplete Exams, n/N (%) | Number of Inadequate Views If Anatomy Incomplete, Median (IQR) † | Nuchal Fold Not Measured At 18.0–20.0 Weeks, n/N (%) ‡ | Nasal Bone Not Measured At 18.0–22.0 Weeks, n/N (%) ‡ |
|---|---|---|---|---|
| Physician 1 | 248/678 (36.6%) § | 4 (2–5) | 8/206 (3.9%) | 78/572 (13.6%) ‡ |
| Physician 2 | 416/983 (42.3%) § | 5 (2–8) | 9/322 (2.8%) | 239/803 (29.4%) ‡ |
| Physician 3 | 298/604 (48.0%) § | 4 (2–5) | 1/193 (0.5%) ‡ | 73/529 (14.1%) ‡ |
| Physician 4 | 361/711 (50.8%) | 5 (3–8) | 8/272 (2.9%) | 92/591 (15.6%) ‡ |
| Physician 5 | 162/278 (58.3%) § | 5 (3–8) | 0/75 (0%) | 30/238 (12.6%) ‡ |
| Physician 6 | 413/567 (72.8%) § | 6 (3–9) | 5/172 (2.9%) | 82/501 (16.4%) |
| Physician 7 | 382/511 (74.8%) § | 3 (1–5) | 4/154 (2.6%) | 211/426 (49.5%) ‡ |
| Practice Total | 4359/8303 (52.5%) | 4 (2–7) | 99/2969 (3.3%) | 1345/7023 (19.2%) |
| Structure | Sonographer 10 (321 Exams) Inadequate Views, n (%) | Physician 7 (511 Exams) Inadequate Views, n (%) | Sonographer 9 (310 Exams) Inadequate Views, n (%) | Physician 2, (983 Exams) Inadequate Views, n (%) |
|---|---|---|---|---|
| Situs | 3 (0.9%) | 1 (0.2%) | 7 (2.3%) | 18 (1.6%) |
| Lateral cerebral ventricles | 1 (0.3%) | 2 (0.4%) | 1 (0.3%) | 10 (1.0%) |
| Choroid plexus | 1 (0.3%) | 2 (0.4%) | 4 (1.3%) | 6 (0.6%) |
| Midline falx | 0 | 1 (0.2%) | 0 | 8 (0.8%) |
| Brain parenchyma | 8 (2.4%) | 10 (2.0%) | 0 | 0 |
| Cerebellum | 8 (2.4%) | 10 (2.0%) | 1 (0.3%) | 10 (1.0%) |
| Cerebellar vermis including 4th ventricle | 12 (3.7%) | 17 (3.3%) | 1 (0.3%) | 14 (1.4%) |
| Cisterna magna | 4 (1.3%) | 6 (1.2%) | 0 | 10 (1.0%) |
| Cavum septi pellucidi | 24 (7.5%) | 28 (5.5%) | 4 (1.3%) | 25 (2.5%) |
| Cranial vault, integrity and shape | 0 | 0 | 0 | 2 (2.0%) |
| Profile (mid-sagittal) | 53 (16.5%) | 67 (13.1%) | 27 (8.7%) | 59 (6.0%) |
| Upper lip (coronal view) | 50 (15.6%) | 59 (11.6%) | 50 (16.1%) | 87 (8.9%) |
| Nose (coronal view) | 41 (12.8%) | 54 (10.6%) | 40 (12.9%) | 77 (7.8%) |
| Maxilla (axial view) | 82 (25.6%) | 118 (23.9%) | 148 (47.7%) | 157 (16.0%) |
| Mandible (axial view) | 77 (24.0%) | 115 (22.5%) | 150 (48.4%) | 169 (17.2%) |
| Neck | 23 (7.2%) | 23 (4.5%) | 127 (41.0%) | 102 (10.4%) |
| Lungs | 0 | 1 (0.2%) | 68 (21%) | 65 (6.6%) |
| Diaphragm | 7 (2.2%) | 6 (1.2%) | 12 (3.9%) | 41 (4.1%) |
| Hands | 213 (66.4%) | 320 (62.6%) | 15 (4.8%) | 21 (2.1%) |
| Feet | 35 (10.9%) | 42 (8.2%) | 9 (2.9%) | 24 (2.4%) |
| Stomach | 0 | 0 | 1 (0.3%) | 1 (0.1%) |
| Kidneys | 8 (2.5%) | 11 (2.2%) | 11 (3.6%) | 20 (2.0%) |
| Urinary bladder | 1 (0.3%) | 0 | 3 (1.0%) | 4 (0.4%) |
| Umbilical cord, number of vessels | 0 | 0 | 0 | 1 (0.1%) |
| Umbilical cord, insertion into abdomen | 7 (2.1%) | 8 (1.6%) | 8 (2.6%) | 14 (1.4%) |
| 4-chamber view of heart | 95 (29.6%) | 110 (23.1%) | 41 (13.2%) | 108 (11.0%) |
| Right outflow tract | 25 (7.8%) | 21 (4.1%) | 91 (29.4%) | 146 (14.9%) |
| Left outflow tract | 28 (8.7%) | 26 (5.1%) | 69 (22.3%) | 135 (13.7%) |
| Aortic arch (sagittal view) | 100 (31.2%) | 123 (24.1%) | 108 (34.8%) | 160 (16.2%) |
| Superior and inferior vena cavae | 22 (6.9%) | 6 (1.2%) | 49 (15.8%) | 81 (8.2%) |
| 3-vessel view | 18 (5.6%) | 30 (5.9%) | 56 (18.1%) | 125 (12.7%) |
| 3-vessel trachea view | 51 (15.9%) | 69 (13.5%) | 86 (27.4%) | 152 (15.5%) |
| Cervical spine | 20 (6.2%) | 23 (4.5%) | 71 (22.9%) | 100 (10.2%) |
| Thoracic spine | 11 (3.4%) | 12 (2.4%) | 71 (22.9%) | 100 (10.2%) |
| Lumbar spine | 25 (7.8%) | 30 (5.9%) | 76 (24.5%) | 111 (11.3%) |
| Sacral spine | 57 (17.8%) | 67 (13.1%) | 87 (28.1%) | 126 (12.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Combs, C.A.; Ashimi Balogun, O.; Vanderhoeven, J.; Amara, S. Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Incomplete Detailed Fetal Anatomy Exams. J. Clin. Med. 2025, 14, 3356. https://doi.org/10.3390/jcm14103356
Combs CA, Ashimi Balogun O, Vanderhoeven J, Amara S. Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Incomplete Detailed Fetal Anatomy Exams. Journal of Clinical Medicine. 2025; 14(10):3356. https://doi.org/10.3390/jcm14103356
Chicago/Turabian StyleCombs, C. Andrew, Olaide Ashimi Balogun, Jeroen Vanderhoeven, and Sushma Amara. 2025. "Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Incomplete Detailed Fetal Anatomy Exams" Journal of Clinical Medicine 14, no. 10: 3356. https://doi.org/10.3390/jcm14103356
APA StyleCombs, C. A., Ashimi Balogun, O., Vanderhoeven, J., & Amara, S. (2025). Quantitative Approach to Quality Review of Prenatal Ultrasound Examinations: Incomplete Detailed Fetal Anatomy Exams. Journal of Clinical Medicine, 14(10), 3356. https://doi.org/10.3390/jcm14103356