1. Introduction
The World Health Organization (WHO) defines overweight in children between 5–19 years old as a z-score greater than 1 standard deviation (SD) and obesity as a z-score greater than 2 SD for body mass index (BMI) [
1]. Overweight and obesity in children is a worldwide health concern, with a high prevalence and an increasing trend in recent years. According to WHO data, prevalence tends to be higher in high-income countries (e.g., the USA and the UK), but increasing trends have also been observed in low- and middle-income countries (LMICs), including regions in Southeast Asia and Latin America [
2,
3,
4]. The overall prevalence of overweight is estimated at around 14.8%, and the prevalence of obesity at around 8.5%, meaning that around 23.3% of children are either living with overweight or obesity, i.e., 1 in 4 children [
2].
Overweight and obesity result from an imbalance between the intake and the expenditure of calories [
5]. The intake of calories/day required for children varies with age and sex, ranging from 100 cal/kg/day in infants to 1800–2200 kcal/day for 12-year-olds [
6]. Factors that contribute to achieving this status include genetic susceptibility, environmental factors, and behavioral factors. Genetic obesity occurs in less than 5% of cases in the pediatric population, but genetic susceptibility may play a role in all cases of children living with obesity, along with many other factors, such as the diet of the child in early life; therefore, the genetic factor is not the cause of the increased rate of childhood overweight and obesity. The factors that play a more significant role in the dramatic increase in childhood overweight and obesity in recent decades could be fast-food and sugary beverage consumption, large portion sizes of the meals, sedentary lifestyle, extensive usage of electronic devices, and family habits [
7,
8,
9,
10]. An important aspect that contributes to the high consumption of fast-food and sugary beverages is the natural preference for sweet and salty tastes in children [
11,
12]. A new factor (and it should not be neglected) contributing to childhood weight gain over the last few years is the COVID 19 pandemic [
13,
14,
15].
In the long-term, obesity has the potential to affect all body systems. Hypertension is strongly associated with childhood obesity, being estimated be present in about ¼ of children with obesity. Type 2 diabetes mellitus (DM) is also closely linked with childhood obesity; around 85% of the children with type 2 DM are living with overweight or obesity. Dyslipidemia is also a common complication of pediatric obesity. The complications of obesity are increased risks for the development of cardiovascular disease (CVD), strokes, and kidney failure [
16,
17,
18,
19]. Other complications include pulmonary-related issues (asthma and sleep apnea) or mineral deficiencies [
20,
21]. The psychosocial impact of obesity, e.g., body dissatisfaction, depressive disorder, anxiety disorder, and even suicidal thoughts, must not be overlooked [
22,
23].
The reported prevalence of overweight and obesity in the adult population of Romania is very high, with around 30% of the adult population being overweight and 21–26% living with obesity [
24,
25,
26,
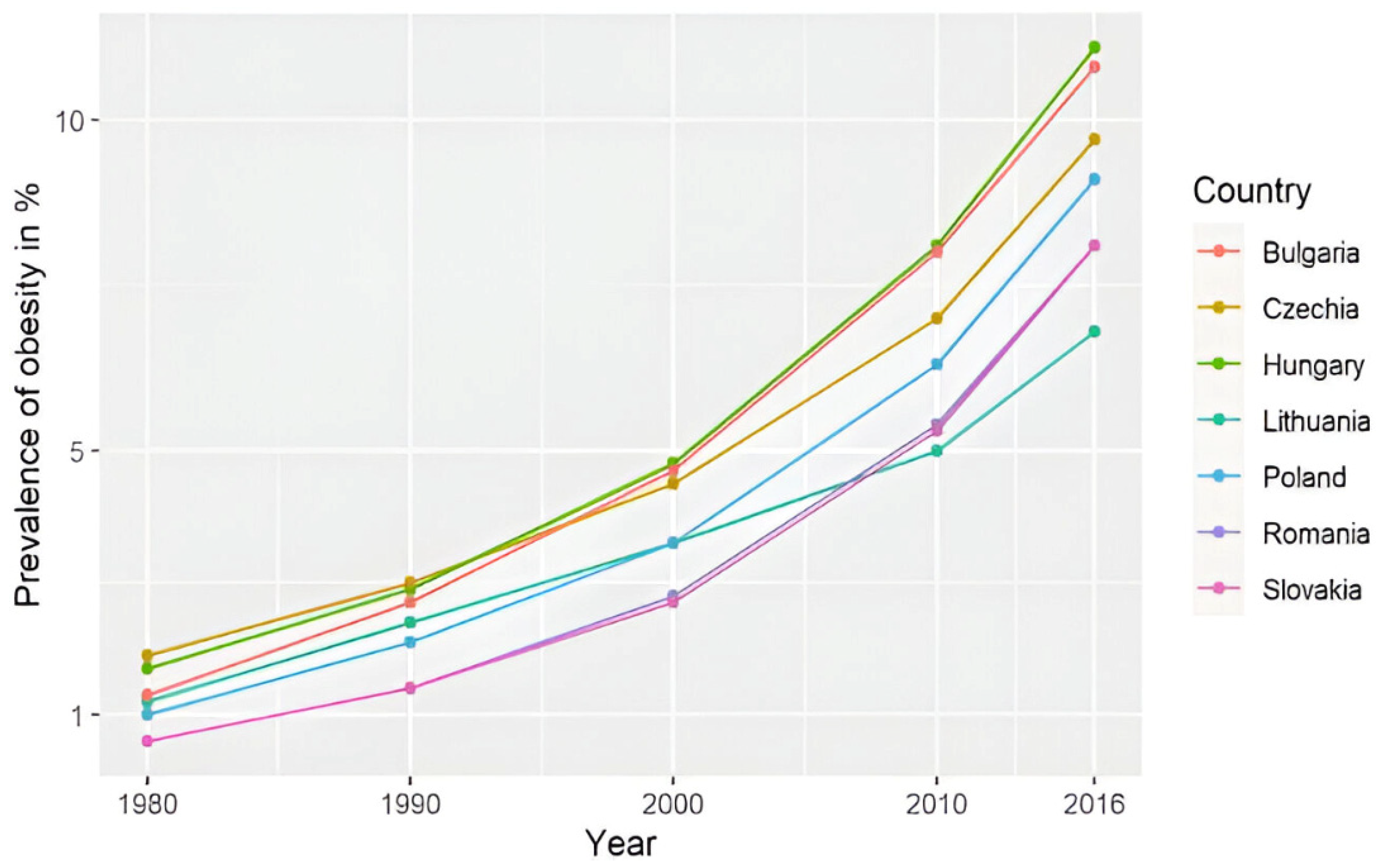
27]. The prevalence of pediatric overweight and obesity in Romania is unclear; some studies estimate the overweight rate at 15–20% and the obesity rate at 8.7–10.7%, with a constantly increasing prevalence from 1980 to 2016 (
Figure 1) [
28,
29,
30,
31]. The WHO Childhood Obesity Surveillance Initiative (COSI), round 6 (2022–2024), estimates that 28% of 7–9 years old children from Romania are living with weight excess (overweight and obesity), and 12% of these children live with obesity. Between round 5 (2020–2022) and round 6, the prevalence was decreasing in girls of this age (−0.7%), but what is more alarming is the increase of 2.9% in boys, with Romania, in this report, being the second country (after Austria-3%) in terms of the rate of increase in this prevalence in boys in this age group (Brief review of results from round 6 of COSI [
32].
The objective of this study is to measure the current prevalence of overweight and obesity of children in Romania, their prevalence by the country regions, and to study the factors that may positively/negatively influence the weight of children in this country.
2. Materials and Methods
This is a repeated cross-sectional study performed by a team of pediatricians across 2 years, in the summers of 2023 and 2024, over a period of 5 days each summer in health centers in Romanian holiday resorts during the holiday period, including respondents from all over the country.
The children, aged 5–17 years old, participated voluntary in the study. All the parents signed an informed consent form, approving the inclusion of their child in the study.
Anamnestic data were collected from the child’s parent, and some medical and anthropometric parameters (weight and height) were measured by the doctors for each child. The BMI and z-scores were calculated using the WHO charts, using standard deviations (SD). The anamnesis consisted of demographics questions, i.e., sex, age, and provenance, family data; the International Standard Classification of Education (ISCED) of the parents and the existence of a parent/sibling with excess weight; and the child’s lifestyle (the existence of a meal schedule, how many times a week the child consumed fast food, how many hours a week the child practiced sports, and how many hours a day the child sat in front of electronic screens).
The margin of error for a confidence interval (CI) of 95% was 3%, calculated by the following formula: ε = z × σ/√n.
ε = margin of error;
z = z-score; 1.96 for a CI of 95%;
σ = population standard deviation; 4 million children;
n = sample size; 1231 respondents.
The z-score of BMI was calculated using the Ped(z) pediatric calculator and was interpreted using WHO references (
Table 1) [
1].
In the text, excess weight was defined as overweight or children living with obesity.
The International Standard Classification of Education (ISCED), adapted to our country, was used to classify the education of the parents (
Table 2). We noted the highest education level in the family (father or mother) [
33].
The numbers of respondents were counted for each county of Romania, i.e., 41 counties and the capital city of Bucharest. In addition, the individuals were according to one of the eight development regions of Romania:
North-East: Bacău, Botoșani, Iași, Neamț, Suceava, and Vaslui.
South-East: Brăila, Buzău, Constanța, Galați, Tulcea, and Vrancea.
South-Muntenia: Argeș, Călărași, Dâmbovița, Giurgiu, Ialomița, Prahova, and Teleorman.
South-West Oltenia: Dolj, Gorj, Mehedinți, Olt, and Vâlcea.
West: Arad, Caraș-Severin, Hunedoara, and Timiș.
North-West: Bihor, Bistrița-Năsăud, Cluj, Maramureș, Satu Mare, and Sălaj.
Center: Alba, Brașov, Covasna, Harghita, Mureș, and Sibiu.
Bucharest–Ilfov: Bucharest and Ilfov [
34].
The data were analyzed using IBM SPSS Statistics, version 25, and illustrated using Microsoft Office Excel/Word 2013. Quantitative variables were tested for normal distribution using the Shapiro–Wilk test and were used as medians with interquartile ranges (IQR). Quantitative variables were tested between two independent groups using Mann–Whitney U tests. The Kruskal–Wallis test was used to determine significant differences between three or more groups of independent variables. Fisher’s exact test was used to determine the nonrandom associations between categorical variables, with the Bonferroni method used for correction. Fisher’s exact test was used independently to assess the association between child overweight/obesity and several categorical risk factors, including parental weight status, sibling weight status, and the presence of a meal schedule. Although each test was performed separately, they addressed related hypotheses concerning predictors of excess weight. Therefore, Bonferroni correction was applied for multiple comparisons (n = 3), setting the adjusted significance level at α = 0.017. Fisher’s exact test was used to assess the association between nutritional status categories (severe thinness, thinness, normal weight, overweight, and obesity) and categorical variables such as regular fast-food consumption and area of provenance. A statistically significant association was found between regular fast-food consumption and nutritional status (p < 0.001), with a higher proportion of excess weight observed among children who reported regular fast-food intake. In contrast, no significant association was observed between area of provenance and nutritional status (p = 0.987). As these comparisons were conducted independently and addressed distinct hypotheses, correction for multiple testing was not applied in this context. Logistic regression models were verified for goodness-of-fit and used for estimating the prediction value of fast-food consumption, parents’ education, physical activity, screen time, regular meal schedule, and the presence of a parent/sibling with obesity in case of increased children weight (in univariate and multivariate models). The regression used continuous variables, i.e., fast-food consumption (how many times per week), physical activity (hours/week), parents’ education (ISCED score), and screen time (hours/day), and categorical variables that were defined as yes/no, i.e., excess weight in parents/siblings (BMI over 25 kg/m2) and meal schedule (the child had the practice of eating at designated times throughout the day more than 5 days/week).
In our logistic regression analysis, the model fit was evaluated using the Hosmer–Lemeshow test, which indicated that the model sufficiently fit the data (p = 0.44). For multicollinearity testing, variance inflation factor (VIF) and tolerance were measured, and both were close to one for each variable; therefore, multicollinearity does not exist in the regression model.
3. Results
In the period of the study, 1439 voluntary respondents under 18 years old were included. A total of 1231 children were included in the cohort (194 children did not meet the age criteria as aged 5–17 years, and there were missing data for another 14 children). A total of 621 (50.4%) were female, and 610 (49.6%) were male (
Table 3).
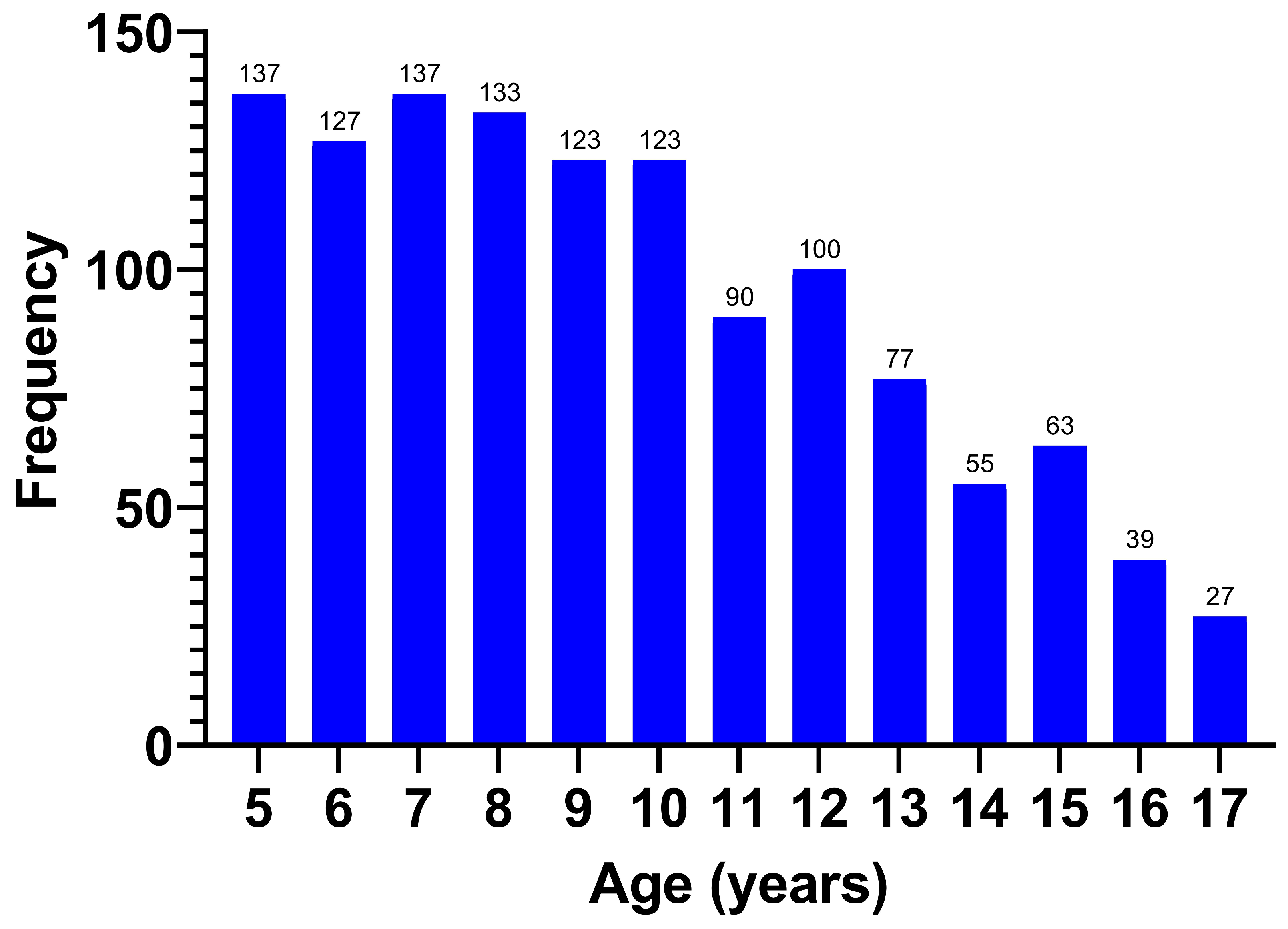
The age of the respondents displayed a non-normal distribution (
p < 0.001), with a median of 9.25 (7–12) years (
Figure 2).
The respondents were classified by age group (
Table 3), with the majority coming from the 5–7 years age group (32.6%).
After calculating and interpreting the BMI and the z-scores, we classified the weight of the children (
Table 3). The BMI z-score showed a normal distribution (
p = 0.062), with an average of +0.11 ± 1.29 SD
A total of 364 (29.6%) children were not classified as normal weight for their age, with most of them being overweight. Almost a quarter of all the participants, 310 (25.1%) children, were either living with overweight or with obesity, and 54 (4.5%) were classified as exhibiting thinness or severe thinness. The rate of obesity was 7.6%, and of that of overweight was 17.5%. The mean z-score of the overweight children was +1.44 ± 0.27 SD.
Weight excess affected 24.5% of females and 25.9% of males, with similar obesity rates (7.4% vs. 7.9%) and no significant gender difference (p = 0.584).
We found no correlation between age and the weight class (p = 0.59) or the age group and the weight class (p = 0.296).
The majority came from urban areas, 937 (76.1%). We found no association between area of provenance and the weight class (p = 0.987). This can be explained by the fact that the rural/urban division no longer respects the degree of development, as there are rural environments, such as those around the capital city or other large cities, which are more developed than some urban environments in the country.
The study included respondents from 40 of the 41 counties of Romania and the capital city of Bucharest; most of them, 255 (20.7%), were from Bucharest, (
Figure 3). Dividing the respondents by region, the highest prevalence of excess weight was found in the South-West Oltenia region (37.3%) and the lowest in the North-East region (19.6%), but it should be noted that the number of respondents by region was not equally distributed (
Table 4).
Most of the children came from a high education background, 763 (62%), followed by medium education, 418 (34%), and the fewest came from a low education background, 50 (4%). The rate of excess weight was higher in those with a medium education background than in those with parents of high education (30.9% vs. 21.5%) (p = 0.001), and the ISCED was higher in the group with no excess weight (6 (3–6) vs. 5 (3–6); p < 0.001).
The majority families, 815 (66.2%), responded that they ate fast food. Of those responders who ate fast food, more than a half of the children, 510 (66.2%), confirmed that they consumed this type of food only once a week (
Figure 4).
The rate of fast-food consumption was higher in the children with excess weight than in normal the weight/thinness group (77.4% vs. 57.5%)
(p < 0.001). The fast-food consumption rate by individual groups was 75.5% reporting regular consumption in the obesity group and 78.2% reporting regular consumption in the overweight group (
p < 0.001;
Table 5), and the group with excess weight consumed fast food more frequently (1 (0–1) vs. 1 (1–2) days/week;
p < 0.001).
A total of 795 (64.6%) children responded that they engaged in physical activity, with a median of 4 (2–6) hours/week. The rate of excess weight was higher in those who did not report engaging in physical activity (29.4%) than in those without regular physical activity (22.9%) (p = 0.013). The number of hours/week of physical activity was lower in the excess weight group, 2 (0–4) hours, compared with that reported by the other group, 2 (0–5) hours (p = 0.02).
A total of 400 (32.5%) had at least one parent with excess weight, 309 (25.1%) had one excess weight parent, and 91 (7.4%) possessed both parents with excess weight.
The proportion of children with excess weight is significantly higher in the group with at least one parent with excess weight (34.3%) than in the group with neither parent with excess weight (20.8%) (p < 0.001).
A total of 893 (72.5%) of the children included in the study had siblings; 92 (7.2%) of those had at least a sibling with excess weight, and the rate of excess weight was higher in those with an excess weight sibling (38% vs. 22.7%) (p = 0.004).
The majority, 908 (73.8%), of families responded that they had a meal schedule. The children with a meal schedule had a lower excess weight rate (22.2%) than those without a definite meal schedule (33.4%) (p < 0.001).
They were asked how much screen time the children were allowed in 1 day, with answers ranging from 1 to 8 h. Almost half of them (42.9%) responded that they watched electronic devices for a maximum of 2 h/day. The average screen time was 3.25 ± 1.85 h/day. Children with excess weight had significantly higher screen time (median: 5 vs. 4 h/day; p = 0.001).
Significant associations were observed between excess weight and the following variables: fast-food consumption, ISCED of the parents, the presence of at least one parent with excess weight, siblings with excess weight, physical activity, and a meal schedule, variables that were further used in the regression (summary in
Table 6).
Data from
Table 7 represents logistic regression models for the overweight/obesity status of the children. In univariate models, all included variables significantly predicted the weight of the children.
A multivariate regression model was created using the variables included in the univariate models, i.e., the days of fast-food consumption, parents’ ISCED, parents with excess weight, siblings with excess weight, hours of physical activity/week, the existence of a meal schedule, and screen time/day as prediction variables. In this model, fast-food consumption, parents’ ISCED, the existence of an excess weight parent, and physical activity had a significant effect (p < 0.005).
The fact that meal schedule did not have a significant effect in the multivariable regression can be explained by the fact that the existence of a regular/irregular meal schedule is predictable according to the frequency of days of fast-food consumption (0.75; 95% CI; 0.68–0.83; p < 0.001), the predictive effect of the meal schedule decreasing in the multivariable logistic regression.
The information that the existence of siblings with excess weight did not have a significant effect in the multivariable regression can be explained by the fact that the existence of a sibling with excess weight is predictable according to the existence of a parent with obesity (3.63; 95% CI; 2.3–5.73; p < 0.001) and the ISCED of the parents (0.78; 95% CI; 0.68–0.9; p = 0.001), the predictive effect of the siblings decreasing in the multivariable logistic regression.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}