1. Introduction
The COVID-19 pandemic has recently been associated with a significant increase in heart failure (HF)-related mortality in a large US nationwide data analysis [
1]. It is known that SARS-CoV-2 infection can exacerbate myocardial injury in patients with chronic HF by generating a high inflammatory status, endotelitis, and myocarditis-like cardiac damage [
2]. Severe COVID-19 can trigger a pro-coagulative state, characterized by high D-dimer, thrombin, von Willebrand factor, and lupus anticoagulant levels, leading to a higher risk of thrombotic events, a need for mechanical ventilation, and adverse outcomes [
3]. Moreover, the cytokine storm in response to SARS-CoV-2 infection can increase platelet production and function, which can predispose to disseminated microthrombosis in different organs and diffuse myocardial injury [
3].
In parallel, the COVID-19 pandemic generated the need for an important reassessment of healthcare resources and policies, with significant consequences in limiting and/or delaying the patient’s access to hospital care [
4,
5,
6,
7]. In particular, a decreasing trend in HF hospitalizations during the first waves of the COVID-19 pandemic was reported, together with changes in interventional and surgical practice [
4,
8]. The STS-INTERMACS registry documented a 17% and 23.5% decline in durable LVAD implantations in 2020 and 2021, respectively, compared to 2019 [
9]. Conversely, heart transplantation (HTX) trends in the pre-pandemic and pandemic eras varied significantly across centers [
10,
11,
12,
13]. While some institutions reported unchanged rates of HTX procedures across the different pandemic waves, other large multicenter registries observed a deflection in HTX activity, especially in extreme ages [
10,
11,
12,
13]. However, the role of modifying patients’ access to HF care in exacerbating HF-related excess mortality during the COVID-19 pandemic is unclear.
In the present study, we aimed to assess how the COVID-19 pandemic affected the therapeutic management of HF in the Lombardy Region using a large multicenter database and evaluate the impact of the pandemic on the prognosis of patients with newly-diagnosed HF. In particular, we explored how the utilization of index therapies for HF (medical, interventional, and surgical) and the survival of HF patients changed from the pre-pandemic era to the pandemic era.
2. Materials and Methods
We conducted a retrospective observational study using the healthcare utilization databases of all residents of Lombardy, an Italian region that accounts for almost 16% of national population (~10 million residents), which is entirely covered by the National Health Service (NHS). These databases provide precise information on all reimbursable health services such as outpatient drug prescriptions, inpatient and outpatient surgical interventions, primary and secondary diagnoses of hospitalizations, and death and are linked by a single individual identification code, which allows one to trace the healthcare pathway of NHS beneficiaries. The study was conducted according to the Declaration of Helsinki. Given the retrospective nature of the study, without direct contact with patients, approval from an ethics review board is not needed (according to the rules from the Italian Medicines Agency, available at:
http://www.agenziafarmaco.gov.it/sites/default/files/det_20marzo2008.pdf; accessed on 30 January 2024).
All Lombardy residents aged ≥18 years and with the first hospital diagnosis of HF from January 2018 to December 2021 were identified and followed up from the date of the first hospitalization until death, emigration, or 31 December 2021. Patients were classified into a pre-pandemic or pandemic group, i.e., diagnosed before and after 1 March 2020, respectively. High-dimensional propensity score (HDPS) [
14] was applied to account for possible differences between groups. Briefly, the propensity to be diagnosed during the pandemic was estimated through a logistic regression model, which included the 200 most predictive covariates among all drugs dispensed and hospital diagnoses experienced in the three years before the HF hospitalization.
Primary outcomes were the utilization of index HF therapies: prescription of Sacubitril/Valsartan (medical management); implantation of cardiac resynchronization therapy (CRT) and/or implantable cardioverter-defibrillator (ICD) (interventional management); mechanical circulatory support (MCS) and heart transplantation (HTX) (surgical management).
Cox regression models were fitted to estimate the hazard ratios (HR) and 95% confidence intervals (CI) for primary outcomes associated with the COVID-19 pandemic, included as a time-dependent variable. Models were adjusted for several demographic and clinical covariates (see
Table 1) and HDPS.
To evaluate the differences in mortality rates between the two time periods, two analyses were performed: (i) Cox regression models and (ii) cumulative incidence function (CIF). Among patients enrolled during the COVID-19 pandemic, overall mortality was depurated from SARS-CoV-2 mortality, defined as at least a sign of infection in the month preceding death. Thus, two Cox regression models were fitted to estimate the HR and 95% CI of, respectively, overall mortality and non-COVID-19-related mortality (COVID-19-related mortality was considered as a competing event for this latter). To calculate CIF, patients enrolled during the pandemic were matched for HDPS to patients enrolled in the pre-pandemic period, whose follow-up was censored to 1 March 2020. Cox models were adjusted for all the covariates, including HDPS.
3. Results
In the pre-pandemic and pandemic era, 36,130 and 17,263 patients, respectively, with newly-diagnosed HF were identified. Demographic characteristics and the burden of concomitant medications and comorbidities are summarized in
Table 1.
Sacubitril/Valsartan was prescribed to 3.5% and 3.8% of patients before and during the pandemic, respectively. CRT/ICD was implanted in 4.1% and 2.7% of patients, MCS was used in 0.4% and 0.3%, and HTX was performed in 0.6% and 0.3% in the pre-pandemic and pandemic eras, respectively (
Table 2).
According to the Cox model, the COVID-19 pandemic was associated with a significant reduction in the utilization of Sacubitril/Valsartan (HR = 0.77, 95% CI: 0.65–0.91, model adjusted also for calendar time, given that Sacubitril/Valsartan prescriptions showed a clear trend during the study period) and implantations of CRT/ICD (HR = 0.85, 95% CI: 0.78–0.92), but it had no significant effect on the probability of receiving an MCS (HR = 1.11, 95% CI: 0.86–1.43) or undergoing a HTX (HR = 0.88, 95% CI: 0.70–1.09).
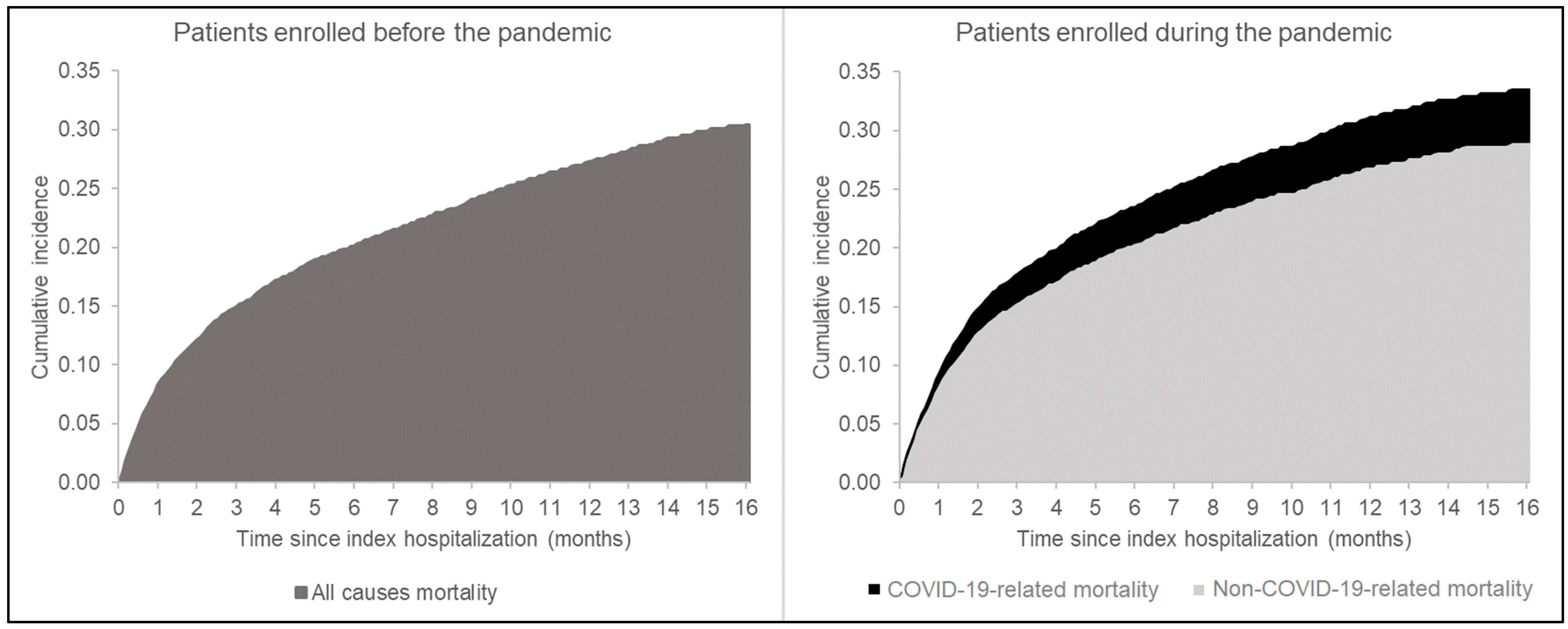
The COVID-19 pandemic was associated with a 19% increased mortality risk (95% CI: 15%–23%). A total of 11,954 individuals from the pandemic era were then matched with as many patients enrolled before the pandemic. The overall cumulative incidence of death was higher in the pandemic matched-cohort compared with the pre-pandemic one (
Figure 1). An overall 4% excess mortality during the pandemic era (at 12 months) was attributable to SARS-CoV2 infection. Patients implanted with MCS displayed a higher cumulative incidence of death, especially during the pandemic era (40% vs. 34% in the pandemic and pre-pandemic era at 12 months, respectively,
p = 0.307) (
Table 2). According to the Cox model, non-COVID-19-related mortality risk during the pandemic was similar to the pre-pandemic mortality risk (HR = 1.01, 95% CI: 0.97–1.04).
4. Discussion
Our work highlights the changes in HF management across the COVID-19 pandemic eras for newly-diagnosed HF patients. Using a large electronic health record database covering a population of ~10 million residents, we identified a significant impact of the COVID-19 pandemic in reducing the utilization of medical (−23%) and interventional therapeutic strategies (−15%) for HF. To assess these modifications, we analyzed the changes in the prescription of index medications for advanced HF (Sacubitril/Valsartan), as well as the implantation of CRT/ICD, MCS, and HTX procedures.
Our data align with the lower access of patients to health system resources [
6,
7,
15] and electrophysiology procedures [
8] recorded during the pandemic. Boriani and colleagues observed a 40% reduction of elective pacemaker, ICD, and CRT implantations during the first pandemic wave (compared to 2019), with a return to pre-pandemic activity intensity only during the third and fourth waves [
8]. In a similar real-world healthcare utilization-based study in Germany, Kerwagen et al. documented a significant decrease in the quarterly growth rate of Sacubitril/Valsartan prescriptions in concomitance with the COVID-19 pandemic [
16]. Interestingly, the treatment initiation remained compromised for 1 year [
16], revealing a potential persistent therapeutic inertia, which mirrors our present findings.
Conversely, our analysis revealed that surgical strategies for end-stage HF (namely short- and long-term MCS and HTX) were not significantly influenced by the pandemic. These data suggest an acceptable preservation of the referral and treatment of most severe HF cases in Lombardy during the pandemic. In fact, important updates and adjustments in HT donor selection, as well as HT recipient monitoring and surveillance, were introduced in Italy at the beginning of the COVID-19 pandemic [
12]. Similarly, ad hoc novel guidelines for cardiac surgical patient screening at admission and during hospitalization, isolation measures, and intraoperative safety measures for patients and healthcare personnel were produced by the Italian Society of Cardiac Surgery in response to the COVID-19 outbreak [
6,
7]. However, the under-treatment of less severe patients might have led to an increase in candidates for advanced therapies, possibly mitigating the difference between the two eras.
As previously reported [
1], our analysis confirms an increased (+19%,
p < 0.001) excess risk of mortality for HF patients during the COVID-19 pandemic (
Figure 1). These data parallel the results of Zuin and colleagues, who observed an increase in HF-related mortality in 2020 of 13.2% and 25.9% compared to 2019 and 2018, respectively [
1]. In our work, after HDPS matching, the pandemic era was confirmed to be associated with a higher overall cumulative incidence of death in the HF population compared to the pre-pandemic period (31% vs. 27% at 12 months, respectively,
p < 0.001). Interestingly, the 4% excess mortality during the pandemic was attributable to SARS-CoV2 infection, while non-COVID-19-related mortality risk in the pandemic era was similar to the pre-pandemic mortality risk. Although the identification of COVID-19 related mortality events presents inner limitations, our data support the deleterious effects of SARS-CoV2 infection itself in the fragile population of patients suffering from HF [
2,
3]. Additional investigations are necessary to better extrapolate the very direct and long-term consequences of the healthcare system reassessment on the prognosis of HF patients.
5. Limitations
Our work presents several limitations. The analysis of healthcare databases allows proper tracking of the utilization of healthcare resources (medications, interventions, surgeries, and hospitalizations) by a large number of patients over a long period of time. However, our databases lack additional clinical variables, such as the New York Heart Association functional class, the echocardiographic metrics of ventricular function, and other less frequent comorbidities, which may act as confounding variables. Although adjusting for HDPS should minimize potential biases, the severity of the disease may differ between patients admitted before and during the pandemic, and results may suffer from residual confounding. Therefore, we cannot make any argumentations about the relationship between the observed (slight) therapeutic management modifications and the increased risk of mortality during the pandemic. Moreover, we were not able to analyze the causes of death in our databases, which may give additional information to clarify the relationship between SARS-CoV-2 infection and the observed excess mortality in HF patients. Future studies should address also the quality of healthcare delivery during pandemics, as well as the patient’s perception and reaction to changes in healthcare policies, to further understand how healthcare reorganization during pandemic periods can actually impact the prognosis of patients.
6. Conclusions
Our work further corroborates (i) the indirect consequences of the COVID-19 pandemic on the reorganization of health care systems, organ availability, and the diagnostic-therapeutic management of HF and (ii) the detrimental association of SARS-CoV2 infection/inflammatory status and pre-existent cardiovascular diseases leading to HF, whose understanding is mandatory to implement pandemic preparedness and preventive strategies in extremely delicate populations. Further longitudinal studies are awaited to determine the very long-term effects of the COVID-19 pandemic on HF management strategies and their impact on patient outcomes. Moreover, the quality of healthcare delivery as perceived by patients and healthcare providers should be explored to optimize hospital policies during pandemic emergencies.
Author Contributions
M.P., G.M., F.R. and A.C. conceived and wrote the paper. G.M., F.R. and A.C. provided statistical expertise. M.P., F.R., G.C., G.G. and A.C. supervised the work. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by grants from the Italian Ministry of the Education, University and Research (‘Fondo d’Ateneo per la Ricerca’ portion, year 2020), and from the Italian Ministry of Health [‘Ricerca Finalizzata 2016′, NET-2016-02363853]. The funding sources had no role in the design of the study, in the collection, analysis, and interpretation of the data, or in the decision to approve publication of the finished manuscript.
Institutional Review Board Statement
The study was conducted according to the Declaration of Helsinki. Given the retrospective nature of the study, without direct contact with patients, approval from an ethics review board is not needed (according to the rules from the Italian Medicines Agency, available at:
http://www.agenziafarmaco.gov.it/sites/default/files/det_20marzo2008.pdf, accessed on 30 January 2024).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study, without direct contact with patients.
Data Availability Statement
The data that support the findings of this study are available from the Lombardy Region, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. Data are, however, available from the corresponding author upon reasonable request and with permission of the Lombardy Region.
Conflicts of Interest
Giovanni Corrao received research support from the European Community (EC), the Italian Medicines Agency (AIFA), Italian Ministry of Health, and the Italian Ministry of Education, University and Research (MIUR). He took part in a variety of projects that were funded by pharmaceutical companies (i.e., Novartis, GSK, Roche, AMGEN, BMS, and Servier). He also received honoraria from Roche as a member of its Advisory Board. All other authors have no disclosures.
References
- Zuin, M.; Rigatelli, G.; Bilato, C. Excess of heart failure-related deaths during the 2020 COVID-19 pandemic in Unites States. Hear. Lung 2023, 58, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System. JAMA Cardiol. 2020, 5, 831. [Google Scholar] [CrossRef] [PubMed]
- Reboiro, M.L.L.; Fuentetaja, R.S.; López, R.G.; Castro-Conde, B.A.; González, C.S.; Menéndez, I.N.; Barrionuevo, M.F.P.; Pérez, M.T.A.; Castro, J.L. Role of lupus anticoagulant and von Willebrand factor in chronic reactive endotheliitis in COVID-19. J. Infect. 2021, 82, e27–e28. [Google Scholar] [CrossRef] [PubMed]
- Bollmann, A.; Hohenstein, S.; König, S.; Meier-Hellmann, A.; Kuhlen, R.; Hindricks, G. In-hospital mortality in heart failure in Germany during the COVID-19 pandemic. ESC Hear. Fail. 2020, 7, 4416–4419. [Google Scholar] [CrossRef] [PubMed]
- Ruzzenenti, G.; Maloberti, A.; Giani, V.; Biolcati, M.; Leidi, F.; Monticelli, M.; Grasso, E.; Cartella, I.; Palazzini, M.; Garatti, L.; et al. Covid and Cardiovascular Diseases: Direct and Indirect Damages and Future Perspective. High Blood Press. Cardiovasc. Prev. 2021, 28, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Bonalumi, G.; Di Mauro, M.; Garatti, A.; Barili, F.; Parolari, A.; Gerosa, G. COVID-19 outbreak and Cardiac Surgery: Position paper from the COVID-SICCH Task Force of the Italian Society for Cardiac Surgery. G. Ital. Cardiol. 2020, 21, 396–400. [Google Scholar]
- Bonalumi, G.; Giambuzzi, I.; Buratto, B.; Barili, F.; Garatti, A.; Casado, A.P.; Di Mauro, M.; Parolari, A. The day after tomorrow: Cardiac surgery and coronavirus disease-2019. J. Cardiovasc. Med. 2022, 23, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Guerra, F.; De Ponti, R.; D’onofrio, A.; Accogli, M.; Bertini, M.; Bisignani, G.; Forleo, G.B.; Landolina, M.; Lavalle, C.; et al. Five waves of COVID-19 pandemic in Italy: Results of a national survey evaluating the impact on activities related to arrhythmias, pacing, and electrophysiology promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing). Intern. Emerg. Med. 2023, 18, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Yuzefpolskaya, M.; Schroeder, S.E.; Houston, B.A.; Robinson, M.R.; Gosev, I.; Reyentovich, A.; Koehl, D.; Cantor, R.; Jorde, U.P.; Kirklin, J.K.; et al. The Society of Thoracic Surgeons Intermacs 2022 Annual Report: Focus on 2018 Heart Transplant Allocation System. Ann. Thorac. Surg. 2022, 115, 311–327. [Google Scholar] [CrossRef] [PubMed]
- Balsara, K.R.; Rahaman, Z.; Sandhaus, E.; Hoffman, J.; Zalawadiya, S.; McMaster, W.; Lindenfeld, J.; Wigger, M.; Absi, T.; Brinkley, D.M.; et al. Prioritizing heart transplantation during the COVID-19 pandemic. J. Card. Surg. 2021, 36, 3217–3221. [Google Scholar] [CrossRef] [PubMed]
- Scientific Registry of Transplant Recipients. COVID-19 Changes to January 2022 PSRs/OSRs. Available online: https://www.srtr.org (accessed on 30 January 2024).
- Fiocco, A.; Ponzoni, M.; Caraffa, R.; Carrozzini, M.; Bagozzi, L.; Nadali, M.; Bifulco, O.; Toscano, G.; Fraiese, A.P.; Bottio, T.; et al. Heart transplantation management in northern Italy during COVID-19 pandemic: Single-centre experience. ESC Heart Fail. 2020, 7, 2003–2006. [Google Scholar] [CrossRef]
- Caraffa, R.; Bagozzi, L.; Fiocco, A.; Bifulco, O.; Nadali, M.; Ponzoni, M.; Carrozzini, M.; Toscano, G.; Fraiese, A.P.; Metra, M.; et al. Coronavirus disease 2019 (COVID-19) in the heart transplant population: A single-centre experience. Eur. J. Cardio-Thorac. Surg. 2020, 58, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S.; Rassen, J.A.; Glynn, R.J.; Avorn, J.; Mogun, H.; Brookhart, M.A. High-dimensional Propensity Score Adjustment in Studies of Treatment Effects Using Health Care Claims Data. Epidemiology 2009, 20, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Bellicini, M.G.; D’altilia, F.P.; Gussago, C.; Adamo, M.; Lombardi, C.M.; Tomasoni, D.; Inciardi, R.M.; Metra, M.; Pagnesi, M. Telemedicine for the treatment of heart failure: New opportunities after COVID-19. J. Cardiovasc. Med. 2023, 24, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Kerwagen, F.; Riemer, U.; Wachter, R.; von Haehling, S.; Abdin, A.; Böhm, M.; Schulz, M.; Störk, S. Impact of the COVID-19 pandemic on implementation of novel guideline-directed medical therapies for heart failure in Germany: A nationwide retrospective analysis. Lancet Reg. Health Eur. 2023, 35, 100778. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 


{kind=link}