

Effect of Antiresorptive Drugs on Osseointegrated Dental Implants: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Focused Questions
2.3. Search Strategy
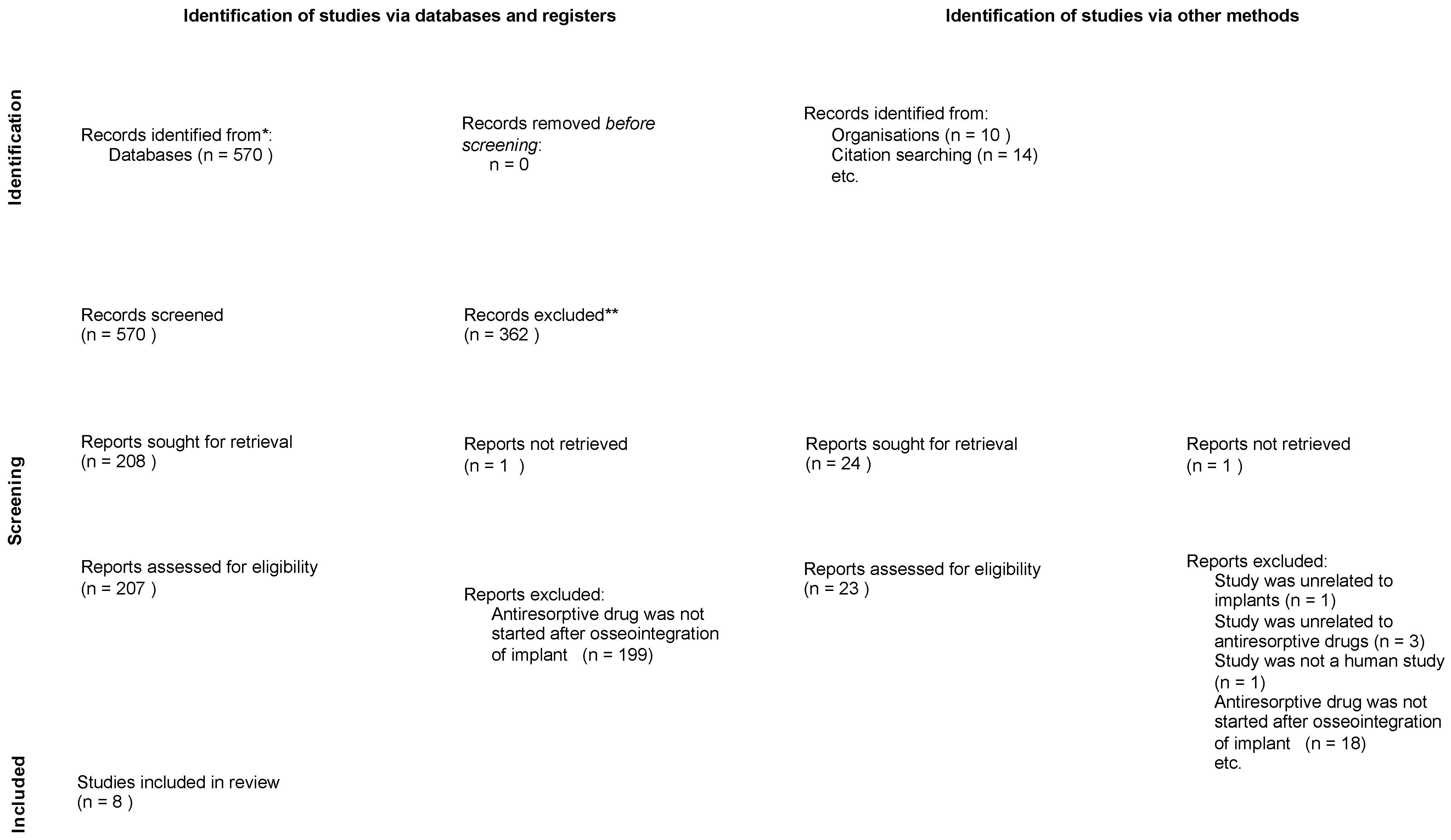
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis and Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Risk of Bias in Studies
3.3. Result of Syntheses
3.3.1. Demographics (Table 2)
3.3.2. Average Time from Initiation of Antiresorptive Drug to MRONJ (Table 2)
3.3.3. Antiresorptive Drug (Table 4)

{kind=link}
| Study | Patients | Mean Age (Years) | Gender | Diagnosis | Type of ARD | Route of Administration | Follow-Up Period | Number of Implants | Survival | Failure | Failure Reason |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pichardo 2020 [13] | 1–14 | NS | NS | NS | NS | 6 O 5 IV 3 S | ≥3 months postoperatively after MRONJ treatment; median 12.5 (3–36) months | 34 | 8 | 26 | 26 MRONJ |
| Holzinger 2014 [14] | 15–17 | NS | 3 F | NS | All BPs 3 Z/I | 3 IV | Retrospective study, studies from 2004 to 2012 | 8 | 0 | 8 | 8 MRONJ |
| Goss 2010 [15] | 18–21 | 70 (66–75) | 2 M, 2 F | All OS | All BPs 3 A 1 A then R | 4 O | Up to 3 years post surgery | 12 | 6 | 6 | 4 MRONJ 2 Fell out |
| Massaad 2022 [16] | 22–27 | 66 (50–83) | 2 M, 4 F | 4 OS 2 C | 3 D 2 Z 1 A/Z | 1 O, IV 2 IV 3 S | Minimum twice/month until improvement of symptoms/healing; 4 stable, 7 healed | 11 | 0 | 11 | 11 MRONJ |
| Kwon 2014 [17] | 28–30 | 70 (67–73) | 3 F | All OS | All BPs 2 A 1 R | 3 O | Until lesion completely/mostly covered by mucosa | 5 | 0 | 5 | 5 MRONJ |
| Pogrel 2018 [18] | 31–41 | NS | 11 F | NS | D/BP 8 A 1 Z 2 D | 8 O 1 IV 2 S | ≥2 years | 11 | 0 | 11 | 11 MRONJ |
| Shabestari 2010 [19] | 42–55 | 53 (42–79) | 14 F | All OS | All BPs | 14 O | Up to 4 years | 20 | 20 | 0 | NA |
| Kim 2020 [20] | 56–135 | 67.7 | 30 M, 314 F (in terms of implant number) | NS | 12 Z 18 A/R 4 D/I | 18 O 12 IV 4 S | ≥1 year | 344 | 310 | 34 | 11 MRONJ 14 Peri-implantitis |
| Total | 135 | 65 (42–83) | 9% M 34/385 91% F 351/385 | 93% OS 25/27 7% C 2/27 | 88% BPs (66/75) 12% D (9/75) | 61% O (54/89) 39% IV/S 35/89 | ≥1 year | 445 | 77% 344/445 | 23% 101/445 | 83% MRONJ 76/92 17% Peri-implantitis 16/92 |
3.3.4. Location of MRONJ (Table 5)
| Study | Implants w/MRONJ | ARD-MRONJ Mean Time (Months) | Reasons | Level of MRONJ | Site of MRONJ | Site of Survived Implants |
|---|---|---|---|---|---|---|
| Pichardo 2020 [13] | 1–26 | median 24 (7–120) | 26 MRONJ | NS | NS | |
| Holzinger 2014 [14] | 27–34 | 18 (14–23) | 8 MRONJ | NS | NS | |
| Goss 2010 [15] | 35–38 | 34 (3–61) | 4 MRONJ | 2—Extensive ONJ 2—Localized ONJ | 3 posterior mand 1 anterior mand | 6 max |
| Massaad 2022 [16] | 39–49 | 51 (24–192) | 11 MRONJ | 10—Stage 2 1—Stage 3 | 3 posterior max 2 anterior max 6 posterior mand | |
| Kwon 2014 [17] | 50–54 | 19 (13–27) | 5 MRONJ | NS | 4 posterior max 1 posterior mand | |
| Pogrel 2018 [18] | 55–65 | 58 (24–156) | 11 MRONJ | NS | 2 max 9 mand | |
| Shabestari 2010 [19] | NA | NA | NA | NA | not applicable | 3 posterior max 5 anterior max 5 posterior mand 7 anterior mand |
| Kim 2020 [20] | 66–76 | 11—≤12 months 10—13–35 months 13—≥36 months | 11 MRONJ | NS | 34 MRONJ/Peri-implantitis 44% max (15/34) 56% mand (19/34) 3% anterior (1/34) 38% premolar (13/34) 59% molar (20/34) | |
| Total | 76 | range 3–192 | MRONJ (76/92) |
3.3.5. Severity of MRONJ (Table 5)
3.3.6. Treatment Modalities of MRONJ (Table 6)
| Study | Implants w/MRONJ | Treatments | Outcome of Treatment |
|---|---|---|---|
| Pichardo 2020 [13] | 1–26 | Mostly treated with sequestrectomy and antibiotics | A total of 94% had closed and healed mucosa and were free of complaints. A total of 36% of the implants could be preserved. |
| Holzinger 2014 [14] | 27–34 | Implant removed during ostectomy for osteonecrosis | A total of 36% of the implants could be preserved. |
| Goss 2010 [15] | 35–38 | 2 attempted surgeries with antibiotics 1 surgical salvation 1 removed 1 nil | A total of 75% healed over 3 months; only one case had pain for 3 years, which was then resolved. |
| Massaad 2022 [16] | 39–49 | Local (CHX, H2O2 mouthwash) Antibiotics (Amoxicillin, Clavulanic acid) Surgical procedures (explantation, curettage, and sequestrectomy) | A total of 17% of the implants could be preserved. A total of 64% of the MRONJ locations were healed, and 46% were stable. |
| Kwon 2014 [17] | 50–54 | Sequestrectomy, removed implant, curettage | A total of 20% of the implants could be preserved. A total of 40% of the MRONJ sites were completely covered by mucosa, and 60% were mostly covered by mucosa. |
| Pogrel 2018 [18] | 55–65 | Antibiotics to all, 8 implants removed, curettage | All cases had satisfactory healing following implant removal and debridement. |
| Shabestari 2010 [19] | NA | No treatment needed | No treatment needed. |
| Kim 2020 [20] | 66–76 | Removed simultaneously during removal of sequestrum in MRONJ | Not specified. |
| Total | A total of 27% of the implants could be preserved. A total of 75% of the MRONJ sites were completely healed. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Berenson, J.R.; Stopeck, A.T. Risks of Therapy with Bone Antiresorptive Agents in Patients with Advanced Malignancy. Available online: https://www.uptodate.com/contents/risks-of-therapy-with-bone-antiresorptive-agents-in-patients-with-advanced-malignancy (accessed on 18 February 2024).
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- Kunihara, T.; Tohmori, H.; Tsukamoto, M.; Kobayashi, M.; Okumura, T.; Teramoto, H.; Hamasaki, T.; Yamasaki, T.; Nakagawa, T.; Okimoto, N.; et al. Incidence and trend of antiresorptive agent-related osteonecrosis of the jaw from 2016 to 2020 in Kure, Japan. Osteoporos. Int. 2023, 34, 1101–1109. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, C.A. Bisphosphanates and oral cavity avascular bone necrosis. J. Clin. Oncol. 2003, 21, 4253–4254. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxillofac. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Silva, W.; Montezuma, M.A.; Benites, B.M.; Bruno, J.S.; Fonseca, F.P.; Fregnani, E.R. Current knowledge regarding medication-related osteonecrosis of the jaw among different health professionals. Support Care Cancer 2020, 28, 5397–5404. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohaya, M.A.; Al-Khashan, H.I.; Mishriky, A.M.; Al-Otaibi, L.M. Physicians’ awareness of bisphosphonates-related osteonecrosis of the jaw. Saudi Med. J. 2011, 32, 830–835. [Google Scholar]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Diabetes and Oral Implant Failure:A Systematic Review. J. Dent. Res. 2014, 93, 859–867. [Google Scholar] [CrossRef]
- Veitz-Keenan, A.; Keenan, J.R. Implant outcomes poorer in patients with history of periodontal disease. Evid.-Based Dent. 2017, 18, 5. [Google Scholar] [CrossRef]
- Alqutaibi, A.Y.; Radi, I.A.-E. No Clear Evidence Regarding the Effect of Osteoporosis on Dental Implant Failure. J. Evid. Based Dent. Pract. 2016, 16, 124–126. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Pichardo, S.E.C.; van der Hee, J.G.; Fiocco, M.; Appelman-Dijkstra, N.M.; van Merkesteyn, J.P.R. Dental implants as risk factors for patients with medication-related osteonecrosis of the jaws (MRONJ). Br. J. Oral Maxillofac. Surg. 2020, 58, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Seemann, R.; Matoni, N.; Ewers, R.; Millesi, W.; Wutzl, A. Effect of Dental Implants on Bisphosphonate-Related Osteonecrosis of the Jaws. J. Oral Maxillofac. Surg. 2014, 72, 1937.e1–1937.e8. [Google Scholar] [CrossRef] [PubMed]
- Goss, A.D.F.; Bartold, M.D.F.; Sambrook, P.M.B.B.S.F.; Hawker, P.B.D.S.M.S. The Nature and Frequency of Bisphosphonate-Associated Osteonecrosis of the Jaws in Dental Implant Patients: A South Australian Case Series. J. Oral Maxillofac. Surg. 2010, 68, 337–343. [Google Scholar] [CrossRef]
- Massaad, J.; Magremanne, M. Is medication related osteonecrosis of the jaw around implants a rare entity? A case series with a focus on etiopathophysiology. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e743–e748. [Google Scholar] [CrossRef]
- Kwon, T.-G.; Lee, C.-O.; Park, J.-W.; Choi, S.-Y.; Rijal, G.; Shin, H.-I. Osteonecrosis associated with dental implants in patients undergoing bisphosphonate treatment. Clin. Oral Implant. Res. 2014, 25, 632–640. [Google Scholar] [CrossRef]
- Pogrel, M.A.; Ruggiero, S.L. Previously successful dental implants can fail when patients commence anti-resorptive therapy—A case series. Int. J. Oral Maxillofac. Surg. 2018, 47, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Shabestari, G.O.; Shayesteh, Y.S.; Khojasteh, A.; Alikhasi, M.; Moslemi, N.; Aminian, A.; Masaeli, R.; Eslami, B.; Treister, N.S. Implant Placement in Patients with Oral Bisphosphonate Therapy: A Case Series. Clin. Implant Dent. Relat. Res. 2010, 12, 175–180. [Google Scholar] [CrossRef]
- Kim, J.Y.; Choi, H.; Park, J.H.; Jung, H.D.; Jung, Y.S. Effects of anti-resorptive drugs on implant survival and peri-implantitis in patients with existing osseointegrated dental implants: A retrospective cohort study. Osteoporos. Int. 2020, 31, 1749–1758. [Google Scholar] [CrossRef]
- European Federation of Periodontology Home Page. Available online: https://www.efp.org/faqs/#:~:text=Implants%20are%20also%20not%20suitable,tissue)%20develops%20suddenly%20and%20quickly (accessed on 24 January 2024).
- Guidance on the Standards of Care for NHS-Funded Dental Implant Treatment 2019; Royal College of Surgeons of England Faculty of Dentistry: London, UK, 2019.
- Jacobsen, C.; Metzler, P.; Rössle, M.; Obwegeser, J.; Zemann, W.; Grätz, K.-W. Osteopathology induced by bisphosphonates and dental implants: Clinical observations. Clin. Oral Investig. 2013, 17, 167–175. [Google Scholar] [CrossRef]
- Lazarovici, T.S.; Yahalom, R.; Taicher, S.; Schwartz-Arad, D.; Peleg, O.; Yarom, N. Bisphosphonate-Related Osteonecrosis of the Jaw Associated With Dental Implants. J. Oral Maxillofac. Surg. 2010, 68, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Madrid, C.; Bagan, J. Dental Endosseous Implants in Patients on Bisphosphonate Therapy. Implant Dent. 2006, 15, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Minguez Serra, M.P.; Salort Llorca, C.; Silvestre Donat, F.J. Oral implants in patients receiving bisphosphonates: A review and update. Med. Oral Patol. Oral Cirugía Bucal 2008, 13, E755–E760. [Google Scholar]
- Seki, K.; Namaki, S.; Kamimoto, A.; Hagiwara, Y. Medication-Related Osteonecrosis of the Jaw Subsequent to Peri-Implantitis: A Case Report and Literature Review. J. Oral Implantol. 2021, 47, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Tempesta, A.; Capodiferro, S.; Mauceri, R.; Lauritano, D.; Maiorano, E.; Favia, G.; Limongelli, L. Peri-implantitis-like medication-related osteonecrosis of the jaw: Clinical considerations and histological evaluation with confocal laser scanning microscope. Oral Dis. 2022, 28, 1603–1609. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Cagna, D.; Stähler, P.; Probst, F.; Kaeppler, G.; Troeltzsch, M.; Ehrenfeld, M.; Otto, S. Clinical features of peri-implant medication-related osteonecrosis of the jaw: Is there an association to peri-implantitis? J. Cranio-Maxillofac. Surg. 2016, 44, 1945–1951. [Google Scholar] [CrossRef]
| P | I | C | O |
|---|---|---|---|
| Patients | Intervention | Control | Outcome |
| Patients with dental implants | Initiation of antiresorptive drug therapy after osseointegration of implant | Patients who did not receive antiresorptive drugs | Incidence of medication-related osteonecrosis of the jaw (MRONJ) |
| Author and Year | Study Type | Patients | Dental Implants | Primary Disease in ARD Patients (n) | Mean Time between Initiation of ARD and MRONJ |
|---|---|---|---|---|---|
| Pichardo et al. (2020) [13] | case series | 14 | 34 implants | Did not specify | Median 24 months (range 7–20) |
| Holzinger et al. (2014) [14] | case series | 3 | 8 implants | Did not specify | 18 months (range 14–23) |
| Goss et al. (2010) [15] | case series | 4 | 12 implants | All osteoporosis | 34 months (range 3–61) |
| Massaad et al. (2022) [16] | case series | 6 | 11 implants | 4 osteoporosis 2 cancer | 51 months (range 24–192) |
| Kwon et al. (2014) [17] | case series | 3 | 5 implants | All osteoporosis | 19 months (range 13–27) |
| Pogrel et al. (2018) [18] | case series | 11 | 11 implants | Did not specify | 58 months (range 24–156) |
| Shabestari et al. (2010) [19] | case series | 14 | 20 implants | All osteoporosis | No MRONJ |
| Kim et al. (2020) [20] | retrospective cohort | 80 | 344 implants | Did not specify | 11 patients—≤12 months 10 patients—13–35 months 13 patients—≥36 months |
| Study Design | Patient Selection | Data Collection Method | Outcome Assessment | Statistical Analysis | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Presence of Control Group | Blinding | Sample Size | Representative Sample | Standardized Data Collection | Complete Data Reporting | Objective Outcome Measures | Consistent Outcome Assessment | Appropriate Statistical Tests | Complete Reporting of Results | |
| Pichardo 2020 [13] | + | - | + | ? | + | + | + | + | - | ? |
| Holzinger 2014 [14] | + | - | - | ? | + | ? | + | + | ? | ? |
| Goss 2010 [15] | - | - | + | + | ? | + | + | ? | - | + |
| Massaad 2022 [16] | - | - | - | ? | + | ? | + | + | - | + |
| Kwon 2014 [17] | + | - | - | ? | + | + | + | + | - | + |
| Pogrel 2018 [18] | - | - | - | ? | + | ? | + | + | - | ? |
| Shabestari 2010 [19] | + | - | - | ? | + | + | + | + | - | ? |
| Kim 2020 [20] | + | - | + | + | + | + | + | + | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.T.W.; Leung, Y.Y. Effect of Antiresorptive Drugs on Osseointegrated Dental Implants: A Systematic Review. J. Clin. Med. 2024, 13, 2091. https://doi.org/10.3390/jcm13072091
Li JTW, Leung YY. Effect of Antiresorptive Drugs on Osseointegrated Dental Implants: A Systematic Review. Journal of Clinical Medicine. 2024; 13(7):2091. https://doi.org/10.3390/jcm13072091
Chicago/Turabian StyleLi, Joyce Tin Wing, and Yiu Yan Leung. 2024. "Effect of Antiresorptive Drugs on Osseointegrated Dental Implants: A Systematic Review" Journal of Clinical Medicine 13, no. 7: 2091. https://doi.org/10.3390/jcm13072091
APA StyleLi, J. T. W., & Leung, Y. Y. (2024). Effect of Antiresorptive Drugs on Osseointegrated Dental Implants: A Systematic Review. Journal of Clinical Medicine, 13(7), 2091. https://doi.org/10.3390/jcm13072091