

A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents—A Case Series with 3-Month Follow-Up


Abstract
1. Introduction
1.1. Clinical Presentation and Types of RAS
1.2. Environmental and Systematic Factors Contributing to RAS Aetiology
1.3. RAS Pathogenesis
1.4. Current Treatment Modalities
1.4.1. Pharmacotherapy
1.4.2. High-Level Laser Therapy (Surgical Laser)
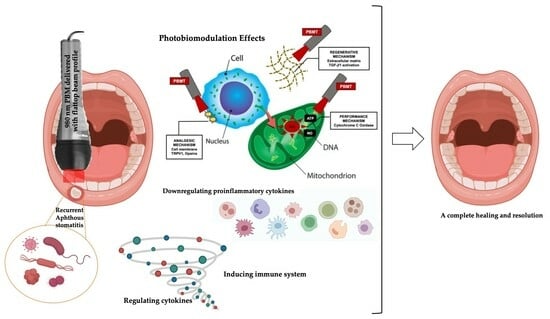
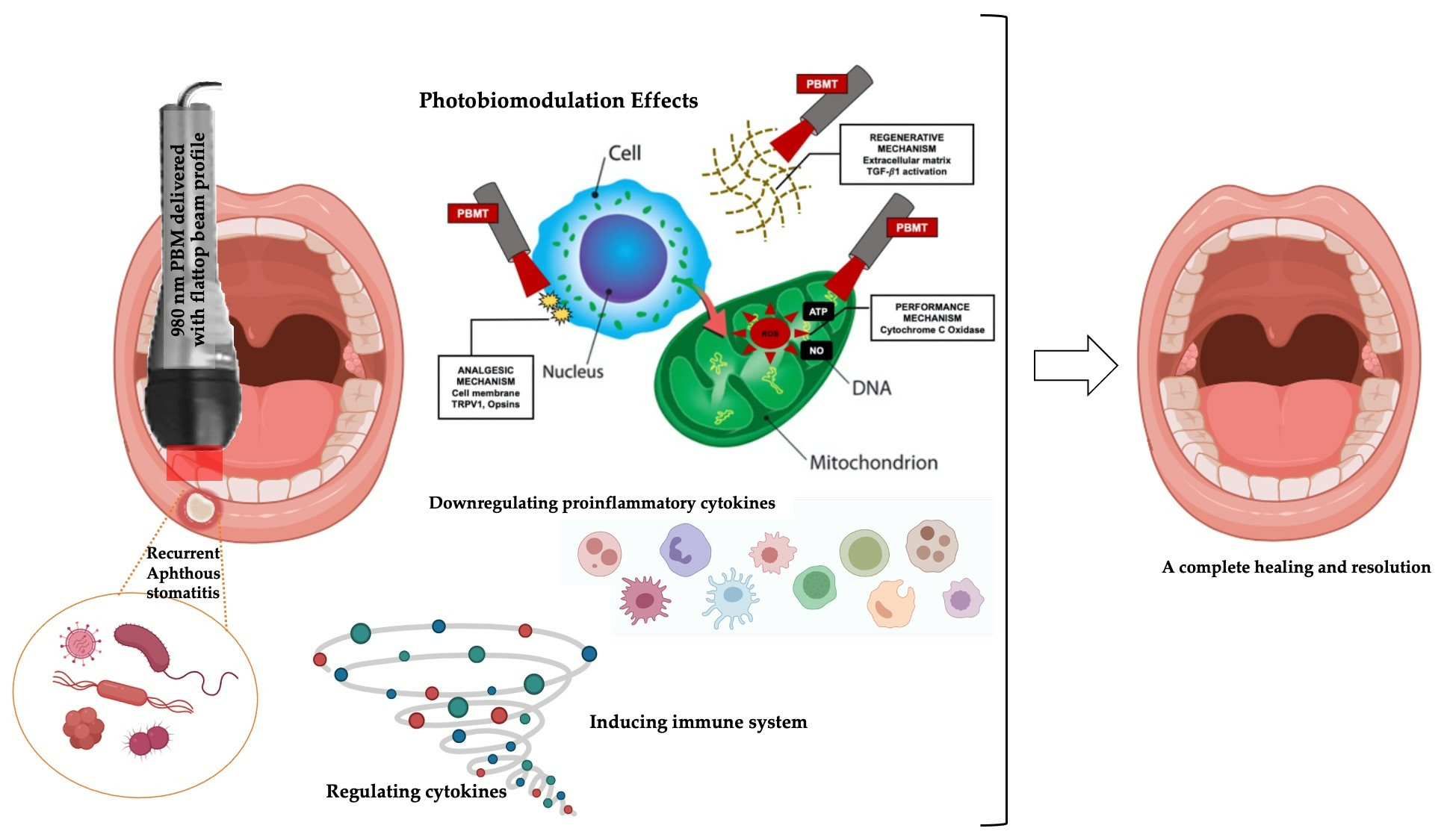
1.4.3. Photobiomodulation Therapy
1.5. Rationale in Conducting the Present Study
2. Materials and Methods
2.1. Study Design
2.2. Interventional Group
2.3. Study’s Focused Question and PICO
- P: Subjects who were <18 years old, presented with any subtype of oral RAU, which occurred no more than 48 h prior to their first PBM session, and diagnosed, with a detailed clinical history and examination of the ulcers and systemic tests [53].
- I: λ 980 nm laser PBM irradiation
- C: Not applicable.
- O: Pain intensity (at rest and during functional activities), wound healing rate, complete lesion resolution, evidence of lesion recurrence, patient treatment satisfaction and parent’s positive experience. All these outcomes were based on qualitative and quantitative measures.
2.4. Therapeutic Photobiomodulation Protocol
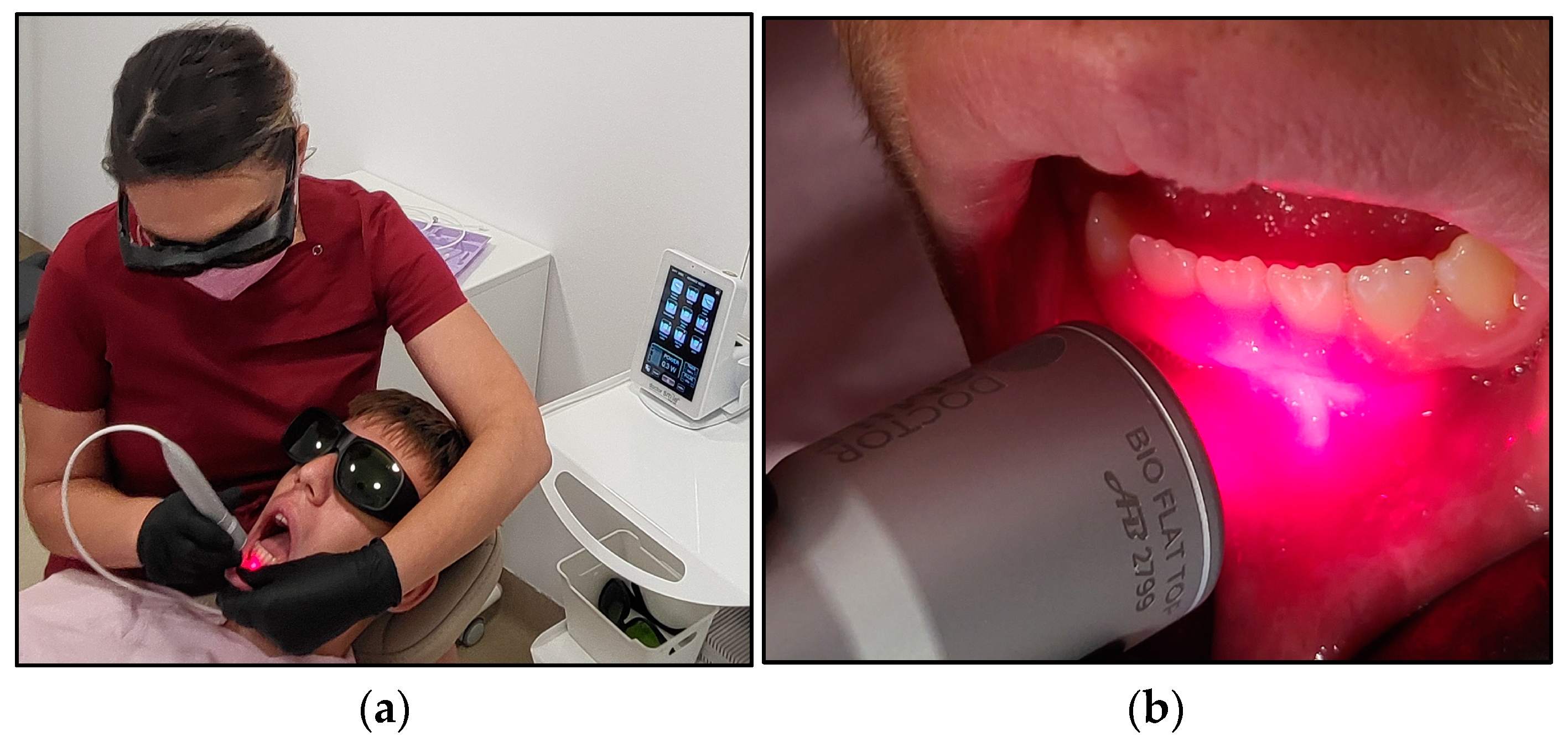
2.5. Description of λ 980 nm Irradiation with Flattop Beam Profile Application
2.6. Study’s Outcomes
2.7. Outcome Assessment Measures
2.7.1. Visual Analogue Scale
2.7.2. Clinician Erythema Assessment (CEA) Visual Assessment Scale
2.7.3. Ruler Method for Wound Surface Area Measurement
2.7.4. Wound Healing Grading Tool
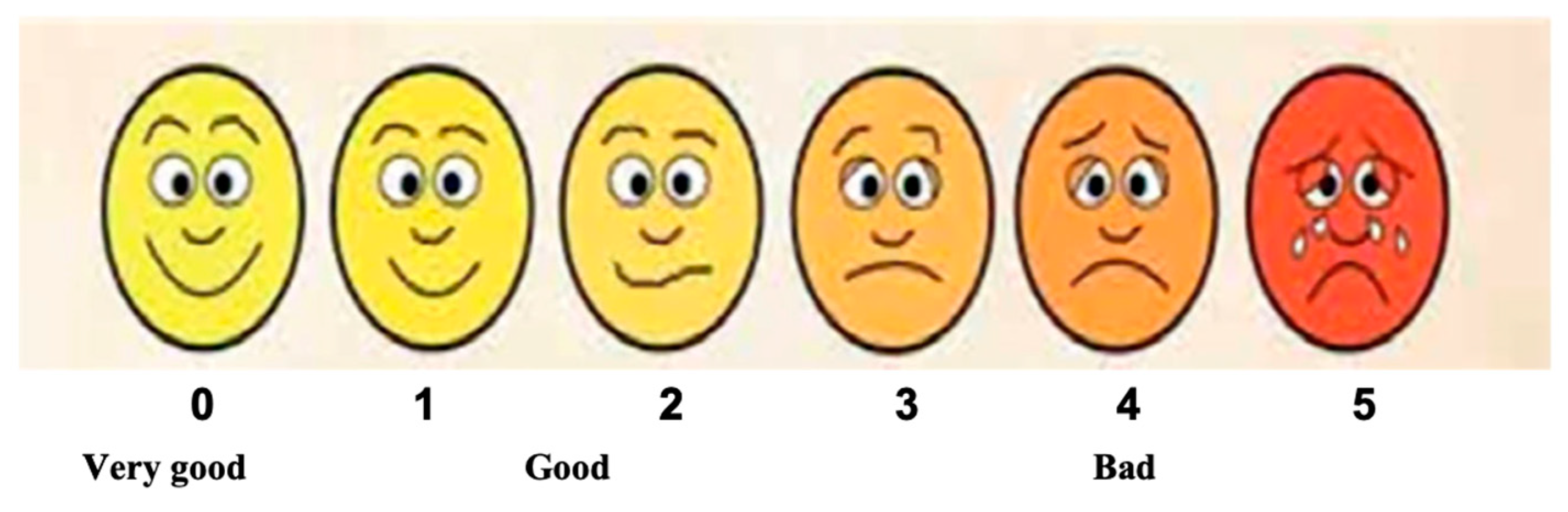
2.7.5. Patient Cooperation Assessment
2.7.6. Patient Treatment Satisfaction
2.8. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Lesion Description
3.2. Primary Endpoints
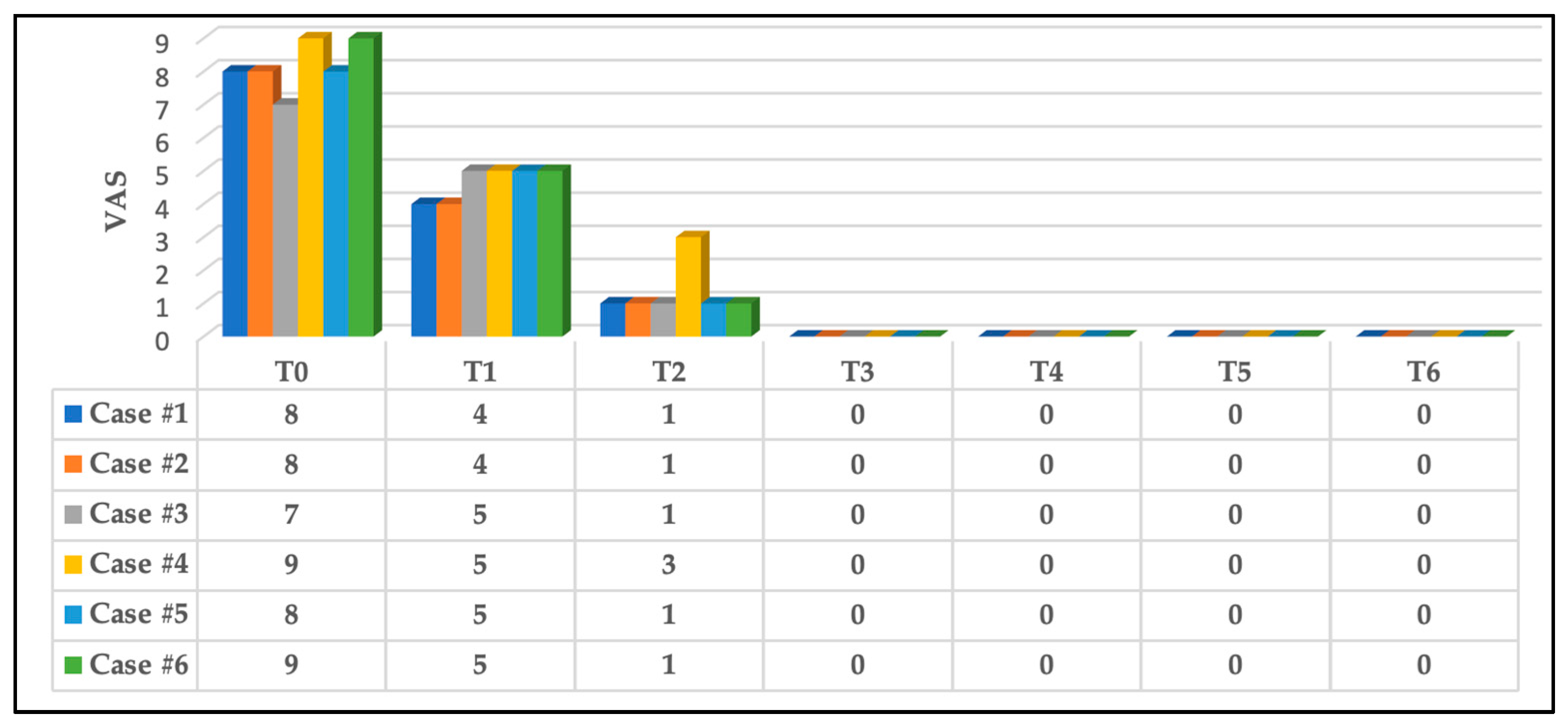
3.2.1. Pain Intensity Scoring at Rest
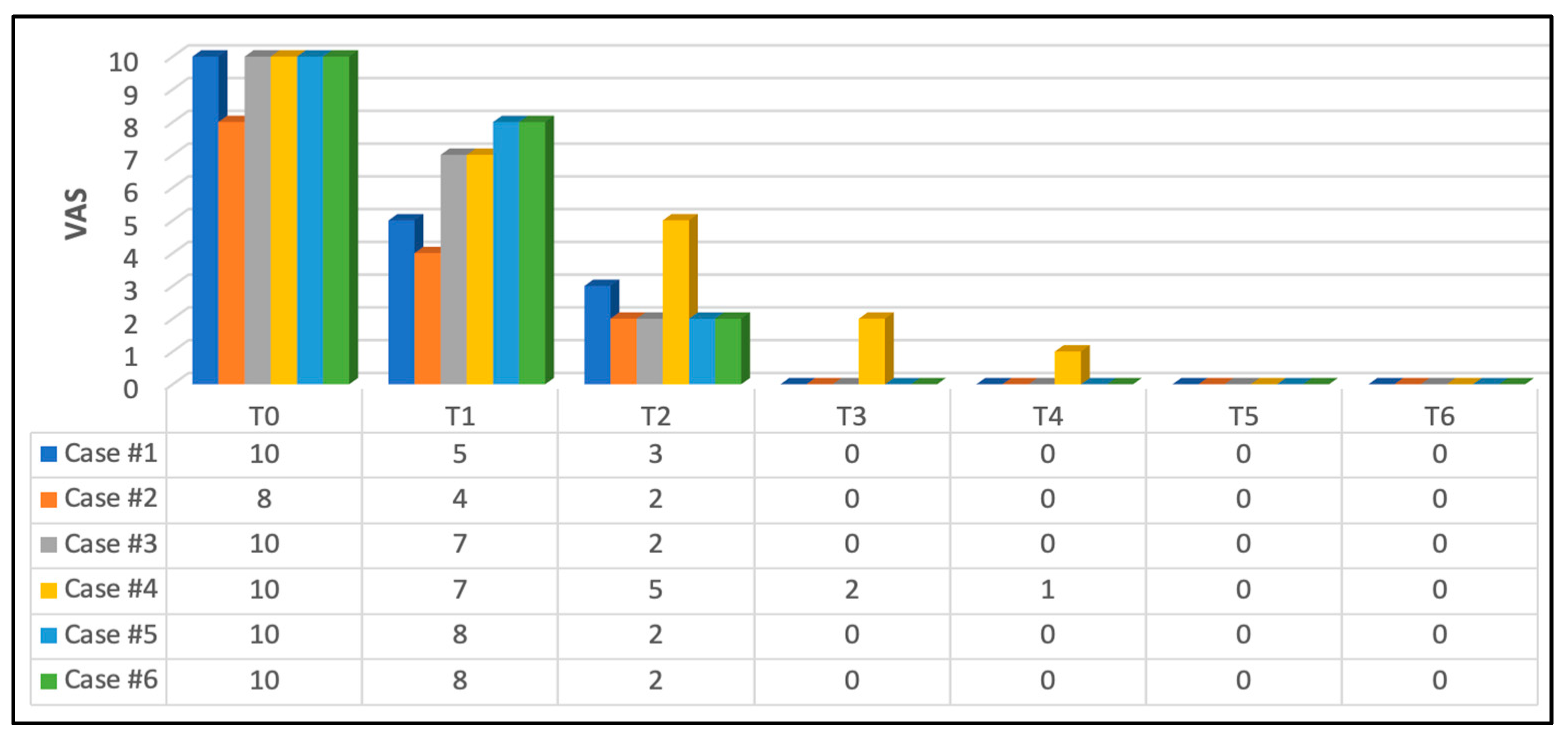
3.2.2. Pain Intensity Scoring at Functional Activities
3.3. Secondary Endpoints
3.3.1. Effects on Erythema
3.3.2. Wound Healing Rate
3.3.3. Patient’s Cooperation
3.3.4. Patient’s Treatment Satisfaction and Parent’s Positive Experience
4. Discussion
4.1. Evaluation Pain Alleviation
4.1.1. Evaluation of Pain Alleviation at Rest
4.1.2. Assessment of Pain Alleviation at Functional Activities
4.2. Appraisal of Wound Healing Rate
4.3. Patient’ Compliance and Cooperation
4.4. PBM Feasibility, Safety and Patient Satisfaction
4.5. PBM Dosimetry and Treatment Protocol Evaluation
4.6. Study’s Limitation and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Preeti, L.; Magesh, K.; Rajkumar, K.; Karthik, R. Recurrent aphthous stomatitis. J. Oral Maxillofac. Pathol. 2011, 3, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, S.O.; Greenberg, M.S. Recurrent aphthous stomatitis. Dent. Clin. N. Am. 2014, 58, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Koberová, R.; Merglová, V.; Radochová, V. Recurrent Aphthous Stomatitis in Children: A Practical Guideline for Paediatric Practitioners. Acta Med. 2020, 63, 145–149. [Google Scholar] [CrossRef]
- Belenguer-Guallar, I.; Jiménez-Soriano, Y.; Claramunt-Lozano, A. Treatment of recurrent aphthous stomatitis. A literature review. J. Clin. Exp. Dent. 2014, 6, e168–e174. [Google Scholar] [CrossRef] [PubMed]
- Huling, L.B.; Baccaglini, L.; Choquette, L.; Feinn, R.S.; Lalla, R.V. Effect of stressful life events on the onset and duration of recurrent aphthous stomatitis. J. Oral Pathol. Med. 2012, 41, 149–152. [Google Scholar] [CrossRef]
- Gasmi Benahmed, A.; Noor, S.; Menzel, A.; Gasmi, A. Oral Aphthous: Pathophysiology, Clinical Aspects and Medical Treatment. Arch. Razi Inst. 2021, 76, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Chavan, M.; Jain, H.; Diwan, N.; Khedkar, S.; Shete, A.; Durkar, S. Recurrent aphthous stomatitis: A review. J. Oral Pathol. Med. 2012, 41, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Vaillant, L.; Samimi, M. Aphthous ulcers and oral ulcerations. Presse Med. 2016, 45, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Jurge, S.; Kuffer, R.; Scully, C.; Porter, S.R. Mucosal disease series. Number VI. Recurrent aphthous stomatitis. Oral Dis. 2006, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Oner, U.; Oner, F.; Kurt, O.; Ozdemir, S. The role of hematologic parameters in recurrent aphthous stomatitis. Ann. Med. Res. 2021, 28, 231–453. [Google Scholar] [CrossRef]
- Baccaglini, L.; Lalla, R.V.; Bruce, A.J.; Sartori-Valinotti, J.C.; Latortue, M.C.; Carrozzo, M.; Rogers, R.S. Recurrent aphthous stomatitis. Oral Dis. 2011, 17, 755–770. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Chen, H.M.; Cheng, S.J.; Wang, Y.P.; Chang, J.Y.; Wu, Y.C. Significant association of deficiencies of hemoglobin, iron, vitamin B12, and folic acid and high homocysteine level with recurrent aphthous stomatitis. J. Oral Pathol. Med. 2015, 44, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Choi, Y.S.; Baek, K.J.; Yoon, S.-H.; Park, H.K.; Choi, Y. Mucosal and salivary microbiota associated with recurrent aphthous stomatitis. BMC Microbiol. 2016, 16, 57. [Google Scholar] [CrossRef]
- Al-Samadi, A.; Salem, A.; Ainola, M.; Hietanen, J.; Häyrinen-Immonen, R.; Konttinen, Y.T. Increased beta 2 defensin in recurrent aphthous ulcer. Oral Dis. 2015, 21, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Slebioda, Z.; Szponar, E.; Kowalska, A. Etiopathogenesis of recurrent aphthous stomatitis and the role of immunologic aspects: Literature review. Arch. Immunol. Ther. Exp. 2014, 62, 205–215. [Google Scholar] [CrossRef]
- Yılmaz, S.; Tuna Kırsaçlıoğlu, C.; Şaylı, T.R. Celiac disease and hematological abnormalities in children with recurrent aphthous stomatitis. Pediatr. Int. 2020, 62, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Boulinguez, S.; Cornée-Leplat, I.; Bouyssou-Gauthier, M.L.; Bedane, C.; Bonnetblanc, J.M. Analysis of the literature about drug-induced aphthous ulcers. Ann. Dermatol. Venereol. 2000, 127, 155–158. [Google Scholar]
- Keenan, A.V.; Spivakovksy, S. Stress associated with onset of recurrent aphthous stomatitis. Evid. Based Dent. 2013, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Conejero Del Mazo, R.; García Forcén, L.; Navarro Aguilar, M.E. Recurrent aphthous stomatitis. Med. Clin. 2023, 161, 251–259. [Google Scholar] [CrossRef]
- Ghasemi, S.; Farokhpour, F.; Mortezagholi, B.; Movahed, E.; Ghaedi, A.; Gargari, M.K.; Khanzadeh, M.; Bazrgar, A.; Khanzadeh, S. Systematic review and meta-analysis of oxidative stress and antioxidant markers in recurrent aphthous stomatitis. BMC Oral Health 2023, 23, 960. [Google Scholar] [CrossRef]
- Saikaly, S.K.; Saikaly, T.S.; Saikaly, L.E. Recurrent aphthous ulceration: A review of potential causes and novel treatments. J. Dermatolog. Treat. 2018, 29, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Tugrul, S.; Koçyiğit, A.; Doğan, R.; Eren, S.B.; Senturk, E.; Ozturan, O.; Ozar, O.F. Total antioxidant status and oxidative stress in recurrent aphthous stomatitis. Int. J. Dermatol. 2016, 55, e130–e135. [Google Scholar] [CrossRef] [PubMed]
- Najafi, S.; Mohammadzadeh, M.; Rajabi, F.; Zare Bidoki, A.; Yousefi, H.; Farhadi, E.; Rezaei, N. Interleukin-4 and Interleukin-4 Receptor Alpha Gene Polymorphisms in Recurrent Aphthous Stomatitis. Immunol. Investig. 2018, 47, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Deng, Y.; Wang, Y.; Yao, H.; Du, G.; Tang, G. Dynamic salivary cytokine profile of recurrent aphthous stomatitis patients in thalidomide maintenance treatment. Clin Oral Investig. 2024, 28, 140. [Google Scholar] [CrossRef] [PubMed]
- Ziaudeen, S.; Ravindran, R. Assessment of Oxidant-Antioxidant status and stress factor in recurrent aphthous stomatitis patients: Case-control study. J. Clin. Diagn. Res. 2017, 11, ZC01–ZC04. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S. Assessment of plasma and salivary antioxidant status in patients with recurrent aphthous stomatitis. RDBO 2011, 8, 261–265. [Google Scholar]
- Zhang, Z.; Li, S.; Fang, H. Enzymatic antioxidants status in patients with recurrent aphthous stomatitis. J. Oral Pathol. Med. 2017, 46, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, H.; Pal Singh, M.; Nahar, P.; Mathur, H.; Sowmya, G.V. Efficacy of low-level laser therapy in treatment of recurrent aphthous ulcers—A sham controlled, split mouth follow up study. J. Clin. Diagn. Res. 2014, 8, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Annamaraju, P.; Baradhi, K.M. Pentpxifyline; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Brocklehurst, P.; Tickle, M.; Glenny, A.-M.; Lewis, M.A.; Pemberton, M.N.; Taylor, J.; Walsh, T.; Riley, P.; Yates, J.M. Systemic interventions for recurrent aphthous stomatitis (mouth ulcers). Cochrane Database Syst. Rev. 2012, 9, CD005411. [Google Scholar] [CrossRef]
- Tarakji, B.; Gazal, G.; Al-Maweri, S.A.; Azzeghaiby, S.N.; Al Aizari, N.A. Guideline for the diagnosis and treatment of recurrent aphthous stomatitis for dental practitioners. J. Int. Oral Health 2015, 7, 74–80. [Google Scholar]
- Hanna, R.; Benedicenti, S. 10,600 nm High Level-Laser Therapy Dosimetry in Management of Unresponsive Persistent Peripheral Giant Cell Granuloma to Standard Surgical Approach: A Case Report with 6-Month Follow-Up. J. Pers. Med. 2024, 14, 26. [Google Scholar] [CrossRef]
- Hanna, R.; Miron, C.M.; Benedicenti, S. Feasibility and Safety of Adopting a New Approach in Delivering a 450 nm Blue Laser with a Flattop Beam Profile in Vital Tooth Whitening. A Clinical Case Series with an 8-Month Follow-Up. J. Clin. Med. 2024, 13, 491. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.; Amaroli, A.; Signore, A.; Benedicenti, S. Utilization of carbon dioxide laser therapy in the management of denture induced hyperplasia and vestibuloplasty in a medically compromised patient: A case report. Int. J. Prosthodont. 2019, 32, 211–213. [Google Scholar] [CrossRef]
- Suter, V.G.A.; Sjölund, S.; Bornstein, M.M. Effect of laser on pain relief and wound healing of recurrent aphthous stomatitis: A systematic review. Lasers Med. Sci. 2017, 32, 953–963. [Google Scholar] [CrossRef]
- Prasad, R.S.; Pai, A. Assessment of immediate pain relief with laser treatment in recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 189–193. [Google Scholar] [CrossRef]
- Tezel, A.; Kara, C.; Balkaya, V.; Orbak, R. An evaluation of different treatments for recurrent aphthous stomatitis and patient perceptions: Nd:YAG laser versus medication. Photomed. Laser Surg. 2009, 27, 101–106. [Google Scholar] [CrossRef]
- Zand, N.; Fateh, M.; Ataie-Fashtami, L.; Djavid, G.E.; Fatemi, S.M.; Shirkavand, A. Promoting wound healing in minor recurrent aphthous stomatitis by non-thermal, non-ablative CO2 laser therapy: A pilot study. Photomed. Laser Surg. 2012, 30, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Zand, N.; Ataie-Fashtami, L.; Djavid, G.E.; Fateh, M.; Alinaghizadeh, M.R.; Fatemi, S.M.; Arbabi-Kalati, F. Relieving pain in minor aphthous stomatitis by a single session of non-thermal carbon dioxide laser irradiation. Lasers Med. Sci. 2009, 24, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Mohsina, S.; Gurushankari, B.; Niranjan, R.; Sureshkumar, S.; Sreenath, G.S.; Kate, V. Assessment of the quality of randomized controlled trials in surgery using Jadad score: Where do we stand? J. Postgrad. Med. 2022, 68, 207–212. [Google Scholar] [CrossRef]
- Hanna, R.; Bensadoun, R.J.; Beken, S.V.; Burton, P.; Carroll, J.; Benedicenti, S. Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial. Antioxidants 2022, 11, 533. [Google Scholar] [CrossRef]
- Hanna, R.; Dalvi, S.; Bensadoun, R.J.; Benedicenti, S. Role of Photobiomodulation Therapy in Modulating Oxidative Stress in Temporomandibular Disorders. A Systematic Review and Meta-Analysis of Human Randomised Controlled Trials. Antioxidants 2021, 10, 1028. [Google Scholar] [CrossRef]
- Hanna, R.; Dalvi, S.; Tomov, G.; Hopper, C.; Rebaudi, F.; Rebaudi, A.L.; Bensadoun, R.J. Emerging potential of phototherapy in management of symptomatic oral lichen planus: A systematic review of randomised controlled clinical trials. J. Biophotonics 2023, 16, e202300046. [Google Scholar] [CrossRef] [PubMed]
- Basso, F.G.; Soares, D.G.; Pansani, T.N.; Cardoso, L.M.; Scheffel, D.L.; de Souza Costa, C.A. Proliferation, migration, and expression of oral-mucosal-healing-related genes by oral fibroblasts receiving low-level laser therapy after inflammatory cytokines challenge. ASLMS 2016, 48, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top Quantum. Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, Y.; Yamaguchi, M.; Abiko, Y. Inhibitory effect of low-level laser irradiation on LPS-stimulated prostaglandin E2 production and cyclooxygenase-2 in human gingival fibroblasts. Eur. J. Oral Sci. 2000, 108, 29–34. [Google Scholar] [CrossRef]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.; Carroll, J.; Hamblin, M.R. The Nuts and Bolts of Low-level Laser (Light) Therapy. Ann. Biomed. Eng. 2011, 40, 516–533. [Google Scholar] [CrossRef]
- Hanna, R.; Dalvi, S.; Bensadoun, R.J.; Raber-Durlacher, J.E.; Benedicenti, S. Role of Photobiomodulation Therapy in Neurological Primary Burning Mouth Syndrome. A Systematic Review and Meta-Analysis of Human Randomised Controlled Clinical Trials. Pharmaceutics 2021, 13, 1838. [Google Scholar] [CrossRef]
- Xiao, X.; Deng, Y.; Long, Y.; Liu, W.; Shi, H. Evaluation of cytokines as diagnostic and therapeutic indicators for recurrent aphthous stomatitis: A statistical study. J. Dent. Sci. 2023, 18, 883–888. [Google Scholar] [CrossRef]
- Khaleel, A.M.; Jafer, M.; Nayeem, M.; Hussain, M.I.; Quadri, M.F.A.; Gopalaiah, H.; Quadri, A.M.F. Low-Level Laser Therapy and Topical Medications for Treating Aphthous Ulcers: A Systematic Review. J. Multidiscip. Healthc. 2020, 13, 1595–1605. [Google Scholar] [CrossRef]
- Amorim Dos Santos, J.; Normando, A.G.C.; de Toledo, I.P.; Melo, G.; De Luca Canto, G.; Santos-Silva, A.R.; Guerra, E.N.S. Laser therapy for recurrent aphthous stomatitis: An overview. Clin. Oral Investig. 2020, 24, 37–45. [Google Scholar] [CrossRef]
- Bardellini, E.; Veneri, F.; Amadori, F.; Conti, G.; Majorana, A. Photobiomodulation therapy for the management of recurrent aphthous stomatitis in children: Clinical effectiveness and parental satisfaction. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e549–e553. [Google Scholar] [CrossRef]
- Milia, E.; Sotgiu, M.A.; Spano, G.; Filigheddu, E.; Gallusi, G.; Campanella, V. Recurrent aphthous stomatitis (RAS): Guideline for differential diagnosis and management. Eur. J. Paediatr. Dent. 2022, 23, 73–78. [Google Scholar] [CrossRef]
- Hudson, D.E.; Hudson, D.O.; Wininger, J.M.; Richardson, B.D. Penetration of Laser Light at 808 and 980 nm in Bovine Tissue Samples. Photomed. Laser Surg. 2013, 31, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.; Agas, D.; Benedicenti, S.; Laus, F.; Cuteri, V.; Sabbieti, M.G.; Amaroli, A. A comparative study between the effectiveness of 980 nm photobiomodulation, delivered by Gaussian versus flattop profiles on osteoblasts maturation Frontier in Endocrinology. Bone Res. 2019, 10, 92. [Google Scholar] [CrossRef]
- Selting, W. Atlas of Laser Therapy: State of the Art, 4th ed.; Teamwork Media Srl: Villa Carcina, Italy, 2016; pp. 225–236. [Google Scholar]
- Laser Institute of America. American National Standard for Safe Use of Lasers. ANSI Z 136.1. 2014. Available online: https://www.lia.org/store/product/ansi-z1361-1014-safe-use-lasers-electronic-version (accessed on 25 February 2024).
- DeLoach, L.J.; Higgins, M.S.; Caplan, A.B.; Stiff, J.L. The Visual Analog Scale in the Immediate Postoperative Period. Anesth. Analg. 1998, 86, 102–106. [Google Scholar] [CrossRef]
- Madooei, A.; Abdlaty, R.M.; Doerwald-Munoz, L.; Hayward, J.; Drew, M.S.; Fang, Q.; Zerubia, J. Hyperspectral image processing for detection and grading of skin Erythema. In Proceedings of the SPIE Medical Imaging Conference, Orlando, FL, USA, 24 February 2017. [Google Scholar] [CrossRef]
- Majeske, C. Reliability of wound surface area measurements. Phys. Ther. 1992, 72, 138–141. [Google Scholar] [CrossRef]
- Langemo, D.; Anderson, J.; Hanson, D.; Hunter, S.; Thompson, P. Measuring wound length, width, and area: Which technique? Adv. Skin Wound Care 2008, 21, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Ibraheem, W.I.; Bhati, A.K.; Hakami, N.A.; Alshehri, A.D.; Wadani, M.H.M.; Ageeli, F.M.E. Comparison of Digital Planimetry and Ruler Methods for the Measurement of Extraction Socket Wounds. Medicina 2023, 59, 135. [Google Scholar] [CrossRef]
- Grey, J.E.; Enoch, S.; Harding, K.G. Wound assessment. BMJ 2006, 332, 285–288. [Google Scholar] [CrossRef]
- Tan, K.-Y.; Zin, T.; Sim, H.L.; Poon, P.L.; Cheng, A.; Mak, K. Randomized clinical trial comparing LigaSure haemorrhoidectomy with open diathermy haemorrhoidectomy. Tech. Coloproctol. 2008, 12, 93–97. [Google Scholar] [CrossRef][Green Version]
- Al Homoud, R.A.; Alshellatie, A.K.; Alzumaie, A.S.; Al-Bayati, S.A. Behavior and anxiety levels in pediatric patient: The behavioral changes and anxiety of pediatric patient in dental clinic. Clin. Exp. Dent. Res. 2023, 9, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Légeret, C.; Furlano, R. Oral ulcers in children-a clinical narrative overview. Ital. J. Pediatr. 2021, 47, 144. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.B.; Smith, G.P. Recurrent aphthous stomatitis: A comprehensive review and recommendations on therapeutic options. Dermatol Ther. 2022, 35, e15500. [Google Scholar] [CrossRef] [PubMed]
- Polonowita, A.; Guan, G. Aphthae and Recurrent Aphthous Stomatitis. In Oral Medicine—A Clinical Guide; Balasubramaniam, R., Yeoh, S.C., Yap, T., Prabhu, S., Eds.; Springer: Cham, Switzerland, 2023; pp. 213–215. [Google Scholar] [CrossRef]
- Sattayut, S.; Trivibulwanich, J.; Pipithirunkarn, N.; Danvirutai, N. A clinical efficacy of using CO2 laser irradiating to transparent gel on aphthous stomatitis patients. Laser Ther. 2013, 22, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Enwemeka, C.S.; Parker, C.J.; Dowdy, D.S.; Harkness, E.E.; Sanford, L.E.; Woodruff, L.D. The efficacy of low-power lasers in tissue repair and pain control: A meta-analysis study. Photomed. Laser Surg. 2004, 22, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Hussein, H.; Zaky, A.A.; Nadim, M.K.; Elbarbary, A. Low-Level Diode Laser Therapy (LLLT) versus Topical Corticosteroids in the Management of Recurrent Aphthous Stomatitis Patients: A Randomized Controlled Trial. Adv. Dent. J. 2021, 3, 200–210. [Google Scholar] [CrossRef]
- Farist, S.; Kalakonda, B.; Farista, S.; Ahmed, A.S. Effectiveness of 980 nm Diode Laser on Recurrent Aphthous Stomatitis. Int. J. Laser Dent. 2014, 4, 83–86. [Google Scholar] [CrossRef]
- Dhopte, A.; Bagde, H. Comparative Evaluation of Low-Level Laser Therapy and Topical Triamcinolone Acetonide 0.1% in Recurrent Aphthous Stomatitis Subjects. Cureus 2022, 14, e25564. [Google Scholar] [CrossRef] [PubMed]
- Millet, D.; Welbury, R. Clinical Problem Solving in Orthodontics and Paediatric Dentistry; Churchill Livingstone: Edinburgh, Scotland, 2004; pp. 143–144. [Google Scholar]
- Sánchez-Bernal, J.; Conejero, C.; Conejero, R. Recurrent Aphthous Stomatitis. Actas Dermosifiliogr. (Engl. Ed.) 2020, 111, 471–480. [Google Scholar] [CrossRef]
- Rigante, D.; Vitale, A.; Natale, M.F.; Lopalco, G.; Andreozzi, L.; Frediani, B.; D’Errico, F.; Iannone, F.; Cantarini, L. A comprehensive comparison between pediatric and adult patients with periodic fever, aphthous stomatitis, pharyngitis, and cervical adenopathy (PFAPA) syndrome. Clin. Rheumatol. 2017, 36, 463–468. [Google Scholar] [CrossRef]
- Albrektson, M.L.; Hedström, L.; Bergh, H. Recurrent aphthous stomatitis and pain management with low-level laser therapy: A randomized controlled trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Khurshid, Z.; Zafar, M.S.; Ajlal, S. Applications of light amplification by stimulated emission of radiation (lasers) for restorative dentistry. Med. Princ. Pract. 2016, 25, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, V.; Rao, S.B.; Chandra, S.; Kumar, P.; Rao, L.; Guddattu, V.; Satyamoorthy, K.; Mahato, K.K. Spectroscopic and histological evaluation of wound healing progression following Low Level Laser Therapy (LLLT). J. Biophotonics 2012, 5, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Lalabonova, H.; Daskalov, H. Clinical assessment of the therapeutic effect of low-level laser therapy on chronic recurrent aphthous stomatitis. Biotechnol. Biotechnol. Equip. 2014, 28, 929–933. [Google Scholar] [CrossRef]
- Marya, C.M.; Mehlawat, J.; Nagpal, R.; Kataria, S.; Taneja, P. Comparative assessment of low-level laser therapy (LLLT) vs. topical application of amlexanox + lidocaine to treat recurrent aphthous ulcers (RAUs): A randomized controlled trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2021, 15, 11–15. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device specifications | Manufacturer | Doctor Smile, Lambda, Italy |
| Model identifier | Wiser 2 | |
| Emitters type | Diode laser | |
| Medical/laser class | IV | |
| Beam delivery system | Fibre | |
| Probe design | Single | |
| Beam profile | Flattop | |
| Beam divergence | 0° | |
| Irradiation parameters | Wavelength (nm) | 980 |
| Therapeutic power output (W) | 0.3 | |
| Emission mode | CW | |
| Beam spot size at target (cm2) | 1 | |
| Irradiance at target (W/cm2) | 0.3 | |
| Energy per spot (J) | 18 | |
| Fluence (J/cm2) per point | 18 | |
| Irradiation time (s) per point | 60 | |
| Treatment protocol | Number of irradiated point per case | 1 |
| Laser–tissue distance (mm) | 2 (non-contact) | |
| Application technique | Static | |
| Total treatment sessions per week | 2 | |
| Frequency of session/week | Twice a week | |
| Time interval | 3 days (72 h) |
| Grade | Description of the Erythema |
|---|---|
| 0 | Clear; no sign of erythema |
| 1 | Almost clear; slight redness |
| 2 | Mild erythema; definite redness |
| 3 | Moderate erythema; marked redness |
| 4 | Severe erythema; fiery redness |
| Case # | Gender | Age (yrs) | Lesion Onset (h) | RAS Type | Lesion Site | No. of Lesions |
|---|---|---|---|---|---|---|
| 1 | M | 11 | ~6 | Major: 1 Herpetiform: 7 | Keratinised and non-keratinised buccal mucosa of UR3 and UR4, extending to buccal vestibule | 8 |
| 2 | M | 13 | ~10 | Minor | Keratinised labial mucosa of LL1 | 1 |
| 3 | F | 12 | ~10 | Minor | Non-keratinised buccal mucosa of inner cheek, opposite to LR4 | 1 |
| 4 | F | 6 | ~12 | Major/Minor | Keratinised and non-keratinised buccal mucosa of URc, extending to the buccal sulcus | 2 |
| 5 | M | 7 | ~10 | Minor | Keratinised buccal mucosa of URc | 1 |
| 6 | F | 7 | ~24 | Major | Non-keratinised labial mucosa of LR1, extending to the labial sulcus and lower midline frenum | 1 |
| Case # | RAS Type | No. Lesion | Wound Surface Area Progression Measured in mm2; CC and NR | ||||
|---|---|---|---|---|---|---|---|
| T0 | T3 | T4 | T5 | T6 | |||
| 1 | MaRAS | 1 | 5.6 | 2 | CC | CC | NR |
| herpetiform | 7 | 0.6–3.3 | 6 lesions = 0; 1 lesion = 0.5 | NR | |||
| 2 | MiRAS | 1 | 2.8 | 2.5 | CC | CC | NR |
| 3 | MiRAS | 1 | 3.4 | 1.5 | CC | CC | NR |
| 4 | MiRAS | 1 | 4.5 | 1 | CC | CC | NR |
| MaRAS | 1 | 8 | 2 | 0.5 | |||
| 5 | MiRAS | 1 | 4.5 | 2 | CC | CC | NR |
| 6 | MaRAS | 1 | 15 | CC | CC | CC | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanna, R.; Miron, I.C.; Benedicenti, S. A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents—A Case Series with 3-Month Follow-Up. J. Clin. Med. 2024, 13, 2007. https://doi.org/10.3390/jcm13072007
Hanna R, Miron IC, Benedicenti S. A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents—A Case Series with 3-Month Follow-Up. Journal of Clinical Medicine. 2024; 13(7):2007. https://doi.org/10.3390/jcm13072007
Chicago/Turabian StyleHanna, Reem, Ioana Cristina Miron, and Stefano Benedicenti. 2024. "A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents—A Case Series with 3-Month Follow-Up" Journal of Clinical Medicine 13, no. 7: 2007. https://doi.org/10.3390/jcm13072007
APA StyleHanna, R., Miron, I. C., & Benedicenti, S. (2024). A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents—A Case Series with 3-Month Follow-Up. Journal of Clinical Medicine, 13(7), 2007. https://doi.org/10.3390/jcm13072007