
Different Therapeutic Response to Anti-TNF Drugs in Patients with Axial Spondyloarthritis Depending on Their Clinical Profile: An Unsupervised Cluster Analysis

 , , , and
, , , and 
Abstract
1. Introduction
2. Methods
2.1. Design and Patients
2.2. Collected Variables
- -
- Sociodemographic data: sex, age, smoking status, and body mass index (BMI).
- -
- Clinical characteristics and SpA features: age of onset of axSpA, the initial symptom of low back pain, disease duration (years between symptom onset and the study visit of anti-TNF initiation), diagnostic delay (years between symptom onset and axSpA diagnosis), family history of SpA, and HLA-B27 antigen status. Peripheral (i.e., arthritis, enthesitis, dactylitis) and EMMs (i.e., uveitis, psoriasis, IBD) at any time during the course of the disease were collected.
- -
- Patient-reported outcomes (PROs): To measure disease activity indices and determine if the patient was a responder or not, the following data were collected at baseline (i.e., the day of the anti-TNF initiation) and at the 6-month follow-up visit: the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) [13], the patient’s global visual analog scale (global VAS), the patient’s medical visual analog scale (medical VAS) the patient’s total visual analog scale (total VAS), and the Ankylosing Spondylitis Disease Activity Score (ASDAS) [14] were collected for all patients to assess disease activity. The Bath Ankylosing Spondylitis Functional Index (BASFI) was used to evaluate function in these patients [15]. Finally, the C-reactive protein (CRP, mg/dL) and the erythrocyte sedimentation rate (ESR) were collected.Based on these data, at the 6-month follow-up, patients were classified into a new dichotomous variable (responders and non-responders) according to the decrease in disease activity indices following the ASAS/EULAR 2022 recommendations (considering an improvement ≥1.1 for the ASDAS index or ≥2.0 for the BASDAI index as a responder) [6].
- -
- Past and current treatment: Data on previous or concomitant treatments were collected, including nonsteroidal anti-inflammatory drugs (NSAIDs) and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) such as sulfasalazine, methotrexate, leflunomide, or corticosteroids.
2.3. Statistical Analysis
3. Results
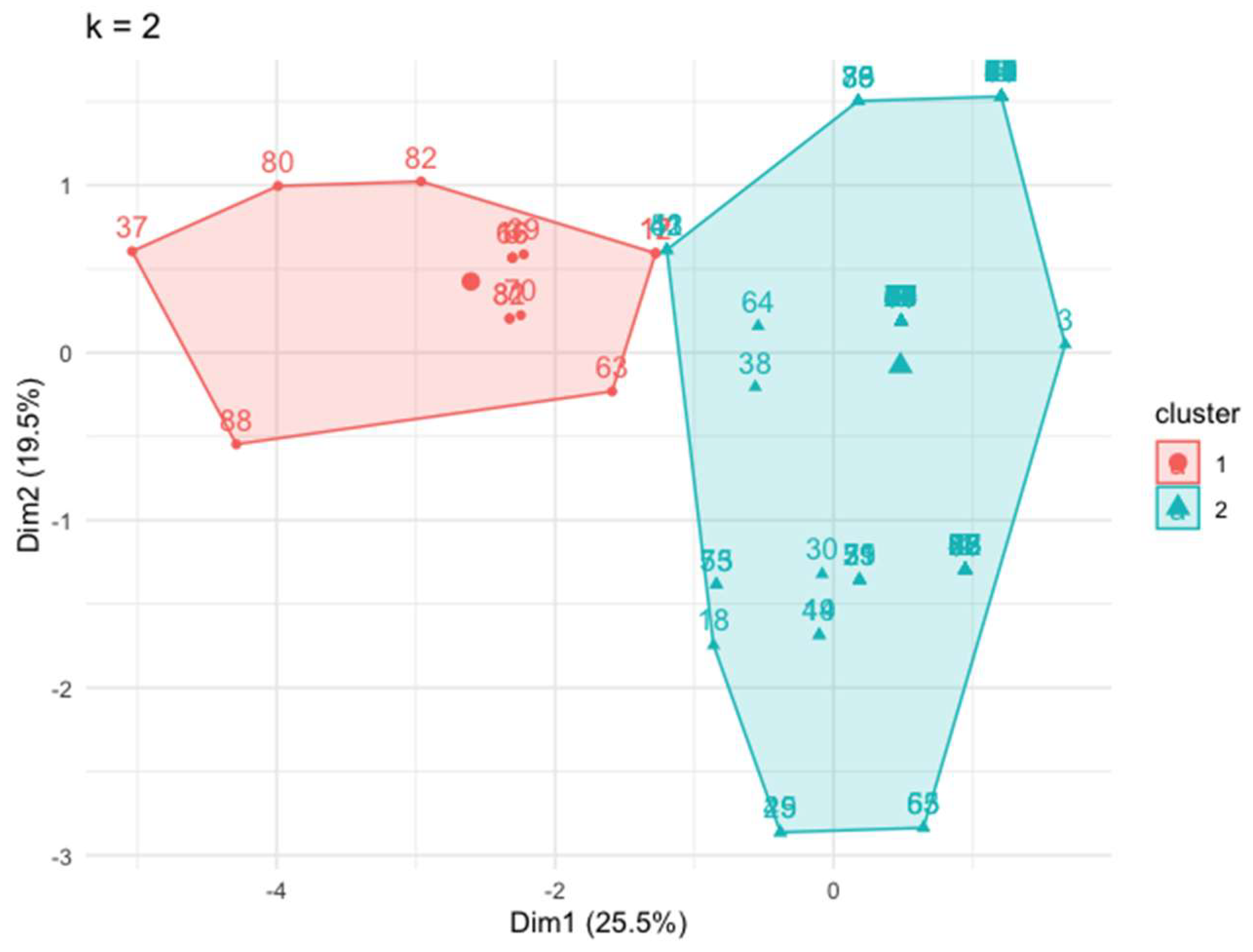
3.1. Cluster Identification according to the Peripheral and Extra-Musculoskeletal Manifestations
3.2. Comparison of the Clusters
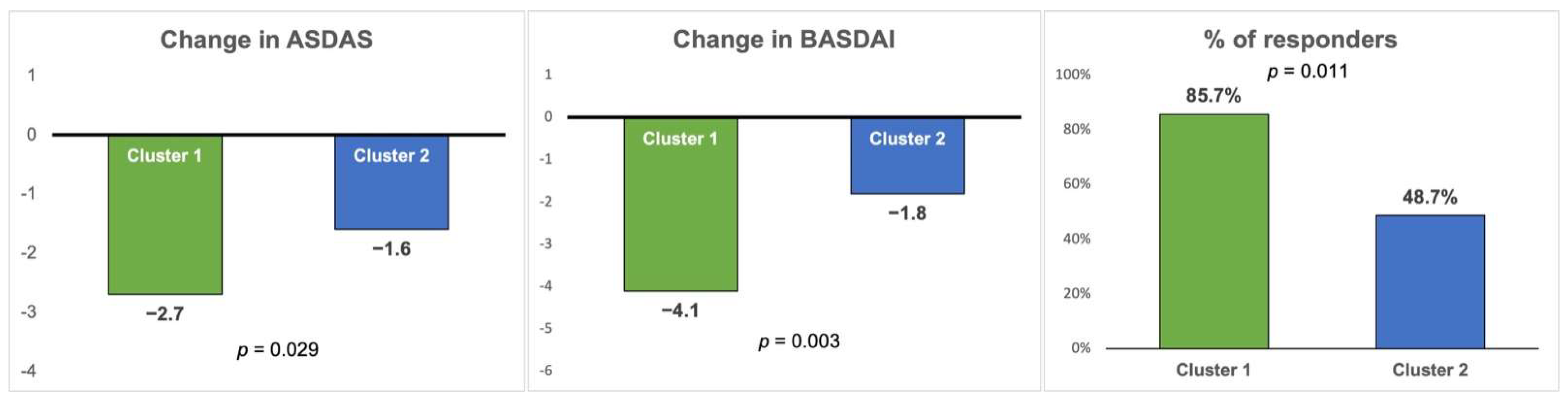
3.3. Comparison of Anti-TNF Effectiveness between the Two Clusters after 6 Months of Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dougados, M.; Baeten, D. Spondyloarthritis. Lancet 2011, 377, 2127–2137. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Poddubnyy, D. Axial Spondyloarthritis. Lancet 2017, 390, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.V.; van der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The Assessment of Spondylo Arthritis international Society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann. Rheum. Dis. 2011, 70, 25–31. [Google Scholar] [CrossRef]
- de Winter, J.J.; van Mens, L.J.; van der Heijde, D.; Landewé, R.; Baeten, D.L. Prevalence of peripheral and extra-articular disease in ankylosing spondylitis versus non-radiographic axial spondyloarthritis: A meta-analysis. Arthritis Res. Ther. 2016, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Puche-Larrubia, M.Á.; Ladehesa-Pineda, L.; Vázquez-Mellado, J.; Escudero-Contreras, A.; Gratacós, J.; Juanola, X.; Collantes-Estévez, E.; Font-Ugalde, P.; López-Medina, C. Identification of the first signs or symptoms in different spondyloarthritis subtypes and their association with HLA-B27: Data from REGISPONSER and RESPONDIA registries. RMD Open 2023, 9, e003235. [Google Scholar] [CrossRef] [PubMed]
- Ramiro, S.; Nikiphorou, E.; Sepriano, A.; Ortolan, A.; Webers, C.; Baraliakos, X.; Landewé, R.B.; Van den Bosch, F.E.; Boteva, B.; Bremander, A.; et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann. Rheum. Dis. 2023, 82, 19–34. [Google Scholar] [CrossRef]
- Maxwell, L.J.; Zochling, J.; Boonen, A.; Singh, J.A.; Veras, M.M.; Ghogomu, E.T.; Jandu, M.B.; Tugwell, P.; Wells, G.A. TNF-alpha inhibitors for ankylosing spondylitis. Cochrane Database Syst. Rev. 2015, 4, CD005468. [Google Scholar] [CrossRef]
- Juanola, X.; Ramos, M.J.; Belzunegui, J.M.; Fernández-Carballido, C.; Gratacós, J. Treatment Failure in Axial Spondyloarthritis: Insights for a Standardized Definition. Adv. Ther. 2022, 39, 1490–1501. [Google Scholar] [CrossRef]
- Lord, P.A.; Farragher, T.M.; Lunt, M.; Watson, K.D.; Symmons, D.P.; Hyrich, K.L.; BSR Biologics Register. Predictors of response to anti-TNF therapy in ankylosing spondylitis: Results from the British Society for Rheumatology Biologics Register. Rheumatology 2010, 49, 563–570. [Google Scholar] [CrossRef]
- Maneiro, J.R.; Souto, A.; Salgado, E.; Mera, A.; Gomez-Reino, J.J. Predictors of response to TNF antagonists in patients with ankylosing spondylitis and psoriatic arthritis: Systematic review and meta-analysis. RMD Open 2015, 1, e000017. [Google Scholar] [CrossRef]
- Puche-Larrubia, M.Á.; Ladehesa-Pineda, L.; Gómez-García, I.; Font-Ugalde, P.; Escudero-Contreras, A.; Collantes-Estévez, E.; López-Medina, C.; REGISPONSER Study Group. Impact of the number of comorbidities on the outcome measures and on the retention rate of the first anti-TNF in patients with Ankylosing Spondylitis. Two-year follow-up in REGISPONSER-AS. Semin. Arthritis. Rheum. 2022, 52, 151938. [Google Scholar] [CrossRef] [PubMed]
- De Craemer, A.S.; Renson, T.; Deroo, L.; Van Praet, L.; Cypers, H.; Varkas, G.; Joos, R.; Devinck, M.; Gyselbrecht, L.; Peene, I.; et al. Peripheral manifestations are major determinants of disease phenotype and outcome in new onset spondyloarthritis. Rheumatology 2022, 61, 3279–3288. [Google Scholar] [CrossRef]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in ankylosing spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar]
- Lukas, C.; Landewé, R.; Sieper, J.; Dougados, M.; Davis, J.; Braun, J.; Van der Linden, S.; Van der Heijde, D.; Assessment of SpondyloArthritis international Society. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2009, 68, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Calin, A.; Garrett, S.; Whitelock, H.; Kennedy, L.G.; O’hea, J.; Mallorie, P.; Jenkinson, T. A new approach to defining functional ability in ankylosing spondylitis: The development of the Bath Ankylosing Spondylitis Functional Index. J. Rheumatol. 1994, 21, 2281–2285. [Google Scholar]
- Charrad, M.; Ghazzali, N.; Boiteau, V.; Niknafs, A. NbClust: An R Package for Determining the Relevant Number of Clusters in a Data Set. J. Stat. Softw. 2014, 61, 1–36. [Google Scholar] [CrossRef]
- de Winter, J.J.; Paramarta, J.E.; de Jong, H.M.; van de Sande, M.G.; Baeten, D.L. Peripheral disease contributes significantly to the level of disease activity in axial spondyloarthritis. RMD Open 2019, 5, e000802. [Google Scholar] [CrossRef] [PubMed]
- Salaet, M.A.; López-Medina, C.; Moreno, M.; Navarro-Compan, V.; Fontova, J.C.; Llop, M.; Dougados, M.; Gratacós, J. Association between HLA-B27 and peripheral spondyloarthritis phenotype: Results from the ASAS perSpA study. RMD Open 2022, 8, e002696. [Google Scholar] [CrossRef]
- Rudwaleit, M.; Claudepierre, P.; Wordsworth, P.; Cortina, E.L.; Sieper, J.; Kron, M.; Carcereri-De-Prati, R.; Kupper, H.; Kary, S. Effectiveness, Safety, and Predictors of Good Clinical Response in 1250 Patients Treated with Adalimumab for Active Ankylosing Spondylitis. J. Rheumatol. 2009, 36, 801–808. [Google Scholar] [CrossRef]
- Davis, J.C. Understanding the role of tumor necrosis factor inhibition in ankylosing spondylitis. Semin. Arthritis Rheum. 2005, 34, 668–677. [Google Scholar] [CrossRef]
- Chen, J.; Lin, S.; Liu, C. Sulfasalazine for ankylosing spondylitis. Cochrane Database Syst. Rev. 2014, 11, CD004800. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total n = 90 n (%) | Cluster 1 n = 14 n (%) | Cluster 2 n = 76 n (%) | p-Value | |
|---|---|---|---|---|
| HLA-B27-positive | 71 (78.9%) | 14 (100%) | 57 (75.0%) | 0.035 |
| Arthritis | 18 (20%) | 8 (57.1%) | 10 (13.2%) | <0.001 |
| Enthesitis | 11 (12.2%) | 11 (78.6%) | 0 (0.0%) | <0.001 |
| Dactylitis | 9 (10.0%) | 6 (42.9%) | 3 (3.9%) | <0.001 |
| Uveitis | 19 (21.1%) | 0 (0.0%) | 19 (25.5%) | 0.035 |
| Psoriasis | 12 (13.3%) | 1 (7.1%) | 11 (14.5%) | 0.683 |
| IBD | 9 (10.0%) | 5 (35.7%) | 4 (5.3%) | <0.001 |
| Total n = 90 n (%) | Cluster 1 n = 14 n (%) | Cluster 2 n = 76 n (%) | p-Value | |
|---|---|---|---|---|
| Sex (male) | 59 (65.6%) | 10 (71.4%) | 49 (64.5%) | 0.764 |
| Age, mean (SD) | 42.5 (11.8) | 38.0 (14.8) | 43.4 (11.1) | 0.058 |
| Smoking | 36 (48.6%) | 1 (8.3%) | 35 (56.5%) | 0.002 |
| BMI, mean (SD) | 26.8 (5.3) | 25.0 (5.2) | 27.1 (5.3) | 0.345 |
| Obesity | 14 (15.6%) | 1 (7.1%) | 13 (17.1%) | 0.688 |
| Disease duration, mean (SD) | 11.9 (10.7) | 6.7 (11.2) | 12.9 (10.5) | 0.007 |
| Diagnosis delay, mean (SD) | 7.5 (9.2) | 3.7 (9.9) | 8.2 (9.0) | 0.003 |
| Back pain as initial symptom | 63 (79.7%) | 7 (58.3%) | 56 (83.6%) | 0.060 |
| Family history of SpA | 35 (46.7%) | 8 (72.7%) | 27 (42.2%) | 0.061 |
| NSAIDs ever | 84 (94.4%) | 13 (92.9%) | 71 (94.7%) | 0.584 |
| Sulfasalazine ever | 34 (38.2%) | 6 (42.9%) | 28 (37.3%) | 0.696 |
| Methotrexate ever | 14 (16.1%) | 7 (50.0%) | 7 (9.6%) | 0.001 |
| Leflunomide ever | 1 (1.1%) | 0 (0.0%) | 1 (1.4%) | 0.839 |
| Corticosteroids ever | 10 (11.2%) | 1 (7.1%) | 9 (12.0%) | 0.509 |
| Diabetes medication | 3 (3.4%) | 0 (0.0%) | 3 (4.0%) | 0.595 |
| Hypertension medication | 23 (25.8%) | 2 (14.3%) | 21 (28.0%) | 0.235 |
| Statins medication | 11 (12.4%) | 1 (7.1%) | 10 (13.3%) | 0.452 |
| Cluster 1 n = 14 Mean (SD) | Cluster 2 n = 76 Mean (SD) | p-Value | |
|---|---|---|---|
| BASDAI (0–10) | |||
| Baseline | 5.9 (2.0) | 5.6 (2.0) | |
| 6 months | 1.8 (1.4) | 3.7 (2.5) | |
| Mean change | −4.1 (0.6) | −1.8 (0.3) | 0.003 |
| BASDAI question 1 (0–10) | |||
| Baseline | 6.2 (1.8) | 6.3 (2.4) | |
| 6 months | 1.2 (1.1) | 3.5 (2.4) | |
| Mean change | −5.0 (2.0) | −2.8 (2.6) | 0.036 |
| BASDAI question 2 (0–10) | |||
| Baseline | 6.4 (0.5) | 7.1 (2.4) | |
| 6 months | 2.0 (2.9) | 3.8 (3.1) | |
| Mean change | −4.4 (2.6) | −3.3 (3.4) | 0.246 |
| BASDAI question 3 (0–10) | |||
| Baseline | 6.4 (1.9) | 4.0 (3.0) | |
| 6 months | 2.0 (2.9) | 3.0 (2.9) | |
| Mean change | −4.4 (3.5) | −1.0 (2.9) | 0.012 |
| BASDAI question 4 (0–10) | |||
| Baseline | 6.8 (1.1) | 5.2 (2.8) | |
| 6 months | 1.8 (2.5) | 3.4 (3.0) | |
| Mean change | −5.0 (2.9) | −1.8 (3.1) | 0.017 |
| BASDAI question 5 (0–10) | |||
| Baseline | 4.8 (3.9) | 6.1 (2.9) | |
| 6 months | 1.2 (1.8) | 3.4 (3.1) | |
| Mean change | −3.6 (5.3) | −2.7 (3.5) | 0.311 |
| BASDAI question 6 (0–10) | |||
| Baseline | 3.2 (4.3) | 5.3 (3.2) | |
| 6 months | 1.0 (1.4) | 2.5 (2.9) | |
| Mean change | −2.2 (5.3) | −2.8 (3.0) | 0.356 |
| ASDAS | |||
| Baseline | 4.2 (1.4) | 3.5 (1.0) | |
| 6 months | 1.5 (1.0) | 1.9 (1.1) | |
| Mean change | −2.7 (1.5) | −1.6 (1.2) | 0.029 |
| Global VAS (0–100) | |||
| Baseline | 43.7 (30.8) | 49.5 (31.1) | |
| 6 months | 13.5 (13.3) | 20.3 (21.7) | |
| Mean change | −30.2 (30.3) | −29.2 (34.2) | 0.887 |
| CRP mg/L | |||
| Baseline | 27.7 (40.0) | 11.2 (10.6) | |
| 6 months | 1.7 (2.2) | 3.1 (5.1) | |
| Mean change | −25.9 (38.9) | −8.1 (10.5) | 0.140 |
| Improvement ≥ 1.1 ASDAS, n (%) | 5 (35.7%) | 21 (27.6%) | 0.374 |
| Improvement ≥ 2.0 BASDAI, n (%) | 11 (78.6%) | 27 (35.5%) | 0.003 |
| Improvement ≥ 1.1 ASDAS or ≥ 2.0 BASDAI, n (%) | 12 (85.7%) | 37 (48.7%) | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priego-Pérez, C.; Puche-Larrubia, M.Á.; Ladehesa-Pineda, L.; Calvo-Guitérrez, J.; Ortega-Castro, R.; Escudero-Contreras, A.; Barbarroja, N.; Collantes-Estévez, E.; López-Medina, C. Different Therapeutic Response to Anti-TNF Drugs in Patients with Axial Spondyloarthritis Depending on Their Clinical Profile: An Unsupervised Cluster Analysis. J. Clin. Med. 2024, 13, 1855. https://doi.org/10.3390/jcm13071855
Priego-Pérez C, Puche-Larrubia MÁ, Ladehesa-Pineda L, Calvo-Guitérrez J, Ortega-Castro R, Escudero-Contreras A, Barbarroja N, Collantes-Estévez E, López-Medina C. Different Therapeutic Response to Anti-TNF Drugs in Patients with Axial Spondyloarthritis Depending on Their Clinical Profile: An Unsupervised Cluster Analysis. Journal of Clinical Medicine. 2024; 13(7):1855. https://doi.org/10.3390/jcm13071855
Chicago/Turabian StylePriego-Pérez, Carmen, María Ángeles Puche-Larrubia, Lourdes Ladehesa-Pineda, Jerusalem Calvo-Guitérrez, Rafaela Ortega-Castro, Alejandro Escudero-Contreras, Nuria Barbarroja, Eduardo Collantes-Estévez, and Clementina López-Medina. 2024. "Different Therapeutic Response to Anti-TNF Drugs in Patients with Axial Spondyloarthritis Depending on Their Clinical Profile: An Unsupervised Cluster Analysis" Journal of Clinical Medicine 13, no. 7: 1855. https://doi.org/10.3390/jcm13071855
APA StylePriego-Pérez, C., Puche-Larrubia, M. Á., Ladehesa-Pineda, L., Calvo-Guitérrez, J., Ortega-Castro, R., Escudero-Contreras, A., Barbarroja, N., Collantes-Estévez, E., & López-Medina, C. (2024). Different Therapeutic Response to Anti-TNF Drugs in Patients with Axial Spondyloarthritis Depending on Their Clinical Profile: An Unsupervised Cluster Analysis. Journal of Clinical Medicine, 13(7), 1855. https://doi.org/10.3390/jcm13071855