
Predicting the Length of Mechanical Ventilation in Acute Respiratory Disease Syndrome Using Machine Learning: The PIONEER Study

 ,
,  , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Methods
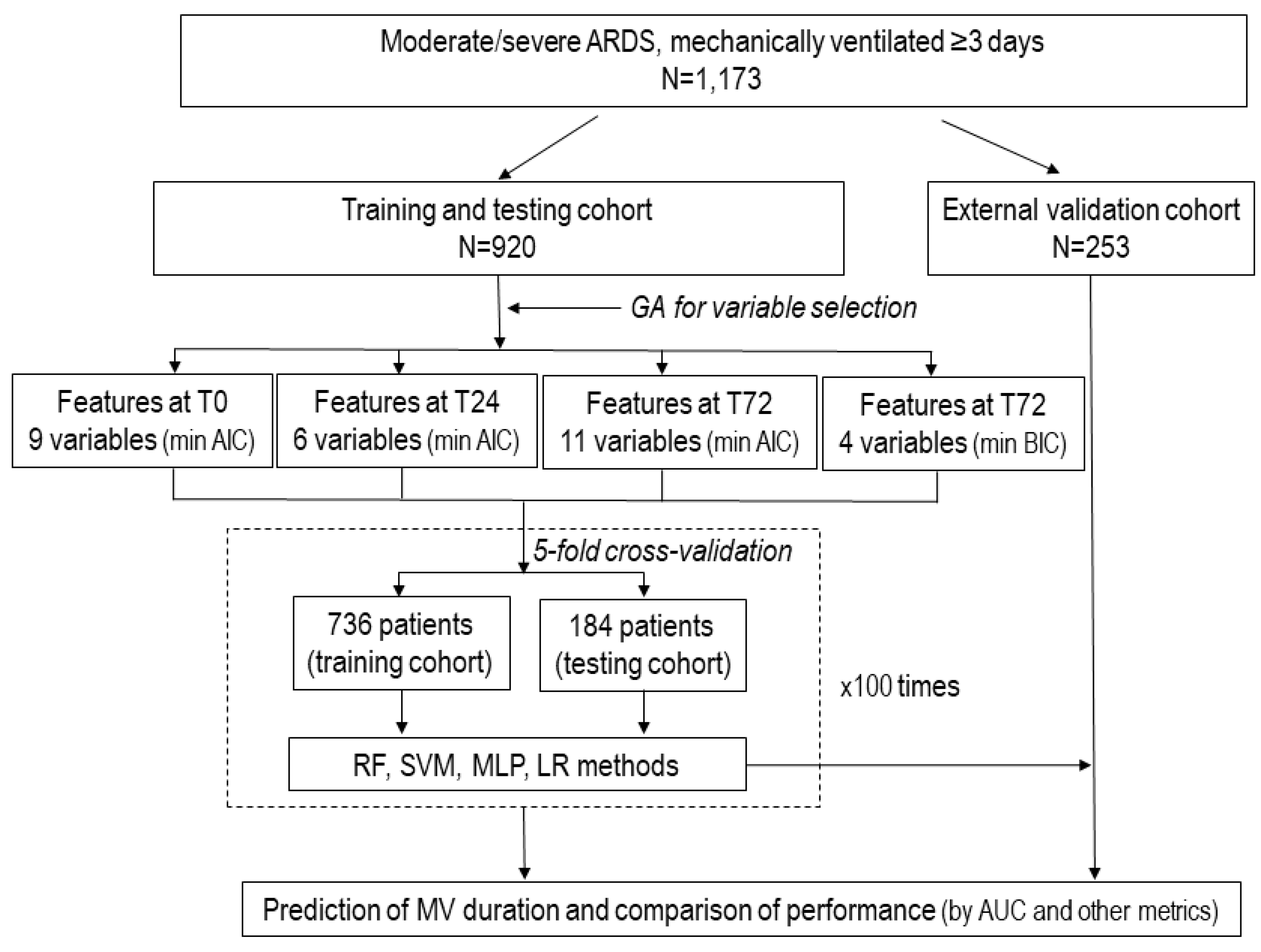
2.1. Patient Population and Study Design
2.2. Variables and Outcomes
2.3. Predefined Rules and Statistical Analysis
Feature Selection Method
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grasselli, G.; Calfee, C.S.; Camporota, L.; Poole, D.; Amato, M.B.; Antonelli, M.; Arabi, Y.M.; Baroncelli, F.; Beitler, J.R.; Bellani, G.; et al. ESICM guidelines on acute respiratory distress syndrome: Definition, phenotyping and respiratory support strategies. Intensive Care Med. 2023, 49, 727–759. [Google Scholar] [CrossRef]
- Maslove, D.M.; Tang, B.; Shankar-Hari, M.; Lawler, P.R.; Angus, D.C.; Baillie, J.K.; Baron, R.M.; Bauer, M.; Buchman, T.G.; Calfee, C.S.; et al. Redefining critical illness. Nature Med. 2022, 28, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 389, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Hybmayr, R.D.; Burchardi, H.; Elliot, M.; Fessler, H.; Georgopoulos, D.; Jubran, A.; Limper, A.; Pesenti, A.; Rubenfeld, G.; Stewart, T.; et al. Statement of the 4th International Conference in Critical Care on ICU-acquired pneumonia-Chicago, Illinois, May 2002. Intensive Care Med. 2002, 28, 1521–1536. [Google Scholar] [CrossRef]
- Dasta, J.F.; McLaughlin, T.P.; Mody, S.H.; Piech, C.T. Daily cost of an intensive care unit day: The contribution of mechanical ventilation. Crit. Care Med. 2005, 33, 1266–1271. [Google Scholar] [CrossRef]
- Figueroa-Casas, J.B.; Connery, S.M.; Montoya, R.; Dwivedi, A.K.; Lee, S. Accuracy of Early Prediction of Duration of Mechanical Ventilation by Intensivists. Ann. Am. Thorac. Soc. 2014, 11, 182–185. [Google Scholar] [CrossRef]
- Figueroa-Casas, J.B.; Dwivedi, A.K.; Connery, S.M.; Quansah, R.; Ellerbrook, L.; Galvis, J. Predictive models of prolonged mechanical ventilation yield moderate accuracy. J. Crit. Care 2015, 30, 502–505. [Google Scholar] [CrossRef]
- Raimondi, N.; Vial, M.R.; Calleja, J.; Quintero, A.; Cortés, A.; Celis, E.; Pacheco, C.; Ugarte, S.; Añón, J.M.; Hernández, G.; et al. Evidence-based guidelines for the use of tracheostomy in critically ill patients. J. Crit. Care 2016, 38, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Troché, G.; Moine, P. Is the duration of mechanical ventilation predictable? Chest 1997, 112, 745–751. [Google Scholar] [CrossRef]
- Añón, J.; Gómez-Tello, V.; González-Higueras, E.; Oñoro, J.; Córcoles, V.; Quintana, M.; López-Martínez, J.; Marina, L.; Choperena, G.; García-Fernández, A.; et al. Prolonged mechanical ventilation probability model. Med. Intensive 2012, 36, 488–495. [Google Scholar] [CrossRef]
- Sayed, M.; Riaño, D.; Villar, J. Predicting duration of mechanical ventilation using supervised machine learning. J. Clin. Med. 2021, 10, 3824. [Google Scholar] [CrossRef] [PubMed]
- Vali, M.; Paydar, S.; Self, M.; Sabetian, G.; Abujaber, A.; Ghaem, H. Prediction prolonged mechanical ventilation in trauma patients of the intensive care units according to initial medical factors: A machine learning approach. Sci. Rep. 2023, 13, 5925. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, G. Artificial Intelligence in the Intensive Care Unit. Crit. Care 2020, 24, 101. [Google Scholar] [CrossRef] [PubMed]
- Dam, T.A.; Roggeveen, L.F.; van Diggelen, F.; Fleuren, L.M.; Jagesar, A.R.; Otten, M.; de Vries, H.J.; Gommers, D.; Cremer, O.L.; Bosman, R.J.; et al. Predicting responders to prone positioning in mechanically ventilated patients with COVID-19 using machine learning. Ann. Intensive Care 2022, 12, 99. [Google Scholar] [CrossRef] [PubMed]
- Parreco, J.; Hidalgo, A.; Parks, J.J.; Kozol, R.; Rattan, R. Using artificial intelligence to predict prolonged mechanical ventilation and tracheostomy placement. J. Surg. Res. 2018, 228, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.F.; Li, J.B.; Liang, H.Y.; Wang, Z.Y.; Jiao, T.T.; Liu, Z.; Yi, L.; Bian, W.S.; Wang, S.P.; Zhu, X.; et al. Predictive model for acute respiratory distress syndrome events in ICU patients in China using machine learning algorithms: A secondary analysis of a cohort study. J. Trans. Med. 2019, 17, 326. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, L.; Huang, T.; Yang, R.; Cheng, H.; Wang, H.; Yin, H.; Lyu, J. Developing an explainable machine learning model to predict the mechanical ventilation duration of patients with ARDS in intensive care units. Hear. Lung 2023, 58, 74–81. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. J. Clin. Epidemiol. 2015, 68, 112–121. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; Blanco, J.; Añón, J.M.; Blanch, L.; Belda, J.; Santos-Bouza, A.; Fernández, R.L.; Kacmarek, R.M.; Spanish Initiative for Epidemiology, Stratification and Therapies for ARDS (SIESTA) network. A universal definition of ARDS: The PaO2/FiO2 under a standard ventilator setting—A prospective, multicenter, validation study. Intensive Care Med. 2013, 39, 583–592. [Google Scholar] [CrossRef]
- Villar, J.; Mora-Ordoñez, J.M.; Soler, J.A.; Mosteiro, F.; Vidal, A.; Ambrós, A.; Fernández, L.; Murcia, I.; Civantos, B.; Romera, M.A.; et al. The PANDORA Study: Prevalence and Outcome of Acute Hypoxemic Respiratory Failure in the Pre-COVID-19 Era. Crit. Care Explor. 2022, 4, e0684. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome. The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Vergouwe, Y.; Steyerberg, E.W.; Eijkemans, M.J.; Habbema, J.D.F. Substantial effective sample sizes were required for external validation studies of predictive logistic regression models. J. Clin. Epidemiol. 2005, 58, 475–483. [Google Scholar] [CrossRef]
- Leisman, D.E.B.; Harhay, M.O.; Lederer, D.J.; Abramson, M.M.; Adjei, A.A.; Bakker, J.M.; Ballas, Z.K.; Barreiro, E.; Bell, S.C.M.; Bellomo, R.; et al. Development and Reporting of Prediction Models: Guidance for Authors from Editors of Respiratory, Sleep, and Critical Care Journals. Crit. Care Med. 2020, 48, 623–633. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; López, J.; Belda, J.; Blanco, J.; Saralegui, I.; Suárez-Sipmann, F.; López, J.; Lubillo, S.; Kacmarek, R.M.; et al. An Early PEEP/FiO2 Trial Identifies Different Degrees of Lung Injury in Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2007, 176, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ambrós, A.; Mosteiro, F.; Martínez, D.; Fernández, L.; Ferrando, C.; Carriedo, D.; Soler, J.A.; Parrilla, D.; Hernández, M.; et al. A Prognostic Enrichment Strategy for Selection of Patients with Acute Respiratory Distress Syndrome in Clinical Trials. Crit. Care Med. 2019, 47, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.; Wang, S.; Liu, R.; Wang, H.; Zheng, J.; Yu, K. Risk factors for outcomes of acute respiratory distress syndrome patients: A retrospective study. J. Thorac. Dis. 2019, 11, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Le, S.; Pellegrini, E.; Green-Saxena, A.; Summers, C.; Hoffman, J.; Calvert, J.; Das, R. Supervised machine learning for the early prediction of acute respiratory distress syndrome (ARDS). J. Crit. Care 2020, 60, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; González-Martín, J.M.; Hernández-González, J.; Armengol, M.A.; Fernández, C.; Martín-Rodríguez, C.; Mosteiro, F.; Martínez, D.; Sánchez-Ballesteros, J.; Ferrando, C.; et al. Predicting ICU Mortality in Acute Respiratory Distress Syndrome Patients Using Machine Learning: The Predicting Outcome and STratifiCation of severity in ARDS (POSTCARDS) Study. Crit. Care Med. 2023, 51, 1638–1649. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; de Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Meng, L.; Zhang, J.; Zhao, Z.; Zou, L.; Jia, Z.; Han, X.; Zhao, L.; Song, M.; Zong, J.; et al. Identification of ferroptosis-related molecular clusters and genes for diabetic osteoporosis based on the machine learning. Front. Endocrinol. 2023, 14, 1189513. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Scrucca, L. GA: A Package for Genetic Algorithms in R. J. Stat. Softw. 2013, 53, 1–37. [Google Scholar] [CrossRef]
- Vrieze, S.I. Model selection and psychological theory: A discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol. Methods 2012, 17, 228–243. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. The Proposal to Lower P Value Thresholds to. 005. JAMA 2018, 319, 1429–1430. [Google Scholar] [CrossRef]
- Kim, J.H.; Kwon, Y.S.; Baek, M.S. Machine Learning Models to Predict 30-Day Mortality in Mechanically Ventilated Patients. J. Clin. Med. 2021, 10, 2172. [Google Scholar] [CrossRef]
- Rashid, M.; Ramakrishnan, M.; Chandran, V.P.; Nandish, S.; Nair, S.; Shanbhag, V.; Thunga, G. Artificial intelligence in acute respiratory distress syndrome: A systematic review. Artif. Intell. Med. 2022, 131, 102361. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Hear. J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef]
- Van Calster, B.; Nieboer, D.; Vergouwe, Y.; De Cock, B.; Pencina, M.J.; Steyerberg, E.W. A calibration hierarchy for risk models was defined: From utopia to empirical data. J. Clin. Epidemiol. 2016, 74, 167–176. [Google Scholar] [CrossRef]
- Schwager, E.; Liu, X.; Nabian, M.; Feng, T.; French, R.M.; Amelung, P.; Atallah, L.; Badawi, O. Machine learning prediction of the total duration of invasive and non-invasive ventilation During ICU Stay. PLoS Digit. Health 2023, 2, e0000289. [Google Scholar] [CrossRef]
- Smit, J.M.; Krijthe, J.H.; van Bommel, J.; van Genderen, M.; Labrecque, J.; Komorowski, M.; Gommers, D.; Reinders, M.J.T.; the Causal Inference for ICU Collaborators. The future of artificial intelligence in intensive care: Moving from predictive to actionable AI. Intensive Care Med. 2023, 49, 1114–1116. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.M.; van Klaveren, D.; Paulus, J.K.; D’Agostino, R.; Goodman, S.; Hayward, R.; Ioannidis, J.P.; Patrick-Lake, B.; Morton, S.; Pencina, M.; et al. The Predictive Approaches to Treatment effect Heterogeneity (PATH) Statement: Explanation and Elaboration. Ann. Intern. Med. 2020, 172, W1–W25. [Google Scholar] [CrossRef]
- Villar, J.; González-Martin, J.M.; Añón, J.M.; Ferrando, C.; Soler, J.A.; Mosteiro, F.; Mora-Ordoñez, J.M.; Ambrós, A.; Fernández, L.; Montiel, R.; et al. Clinical relevance of timing of assessment of ICU mortality in patients with moderate-to-severe Acute Respiratory Distress Syndrome. Sci. Rep. 2023, 13, 1543. [Google Scholar] [CrossRef]
- Marti, J.; Hall, P.; Hamilton, P.; Lamb, S.; McCabe, C.; Lall, R.; Darbyshire, J.; Young, D.; Hulme, C. One-year resource utilisation, costs and quality of life in patients with acute respiratory distress syndrome (ARDS): Secondary analysis of a randomised controlled trial. J. Intensive Care 2016, 4, 56. [Google Scholar] [CrossRef] [PubMed]
- Pirracchio, R.; Petersen, M.L.; Carone, M.; Rigon, M.R.; Chevret, S.; van der Laan, M.J. Mortality prediction in intensive care units with the Super ICU Learner Algorithm (SICULA): A population-based study. Lancet Respir. Med. 2015, 3, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.; McGinlay, M.; Amin, R.; Burns, K.E.; Connolly, B.; Hart, N.; Jouvet, P.; Katz, S.; Leasa, D.; Mawdsley, C.; et al. Variation in definition of prolonged mechanical ventilation. Respir. Care 2017, 62, 1324–1332. [Google Scholar] [CrossRef]
- Villar, J.; Fernández, C.; González-Martín, J.M.; Ferrando, C.; Añón, J.M.; del Saz-Ortíz, A.M.; Díaz-Lamas, A.; Bueno-González, A.; Fernández, L.; Domínguez-Berrot, A.M.; et al. Respiratory Subsets in Patients with Moderate to Severe Acute Respiratory Distress Syndrome for Early Prediction of Death. J. Clin. Med. 2022, 11, 5724. [Google Scholar] [CrossRef] [PubMed]
- Briel, M.; Meade, M.; Mercat, A.; Brower, R.G.; Talmor, D.; Walter, S.D.; Slutsky, A.S.; Pullenayegum, E.; Zhou, Q.; Cook, D.; et al. Higher versus lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: Systematic review and meta-analysis. JAMA 2010, 303, 865–873. [Google Scholar] [CrossRef]
- Shin, K.K.; Rosen, M.J. Is there a safe plateau pressure threshold for patients with acute lung injury and acute respiratory distress syndrome? Am. J. Respir. Crit. Care Med. 2006, 173, 686–687. [Google Scholar]
- Kallet, R.H.; Lipnick, M.S.; Zhuo, H.; Pangilinan, L.P.; Gomez, A. Characteristics of non-pulmonary organ dysfunction at onset of ARDS based on the Berlin definition. Respir. Care 2019, 64, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Jivraj, N.K.; Hill, A.D.; Shieh, M.-S.; Hua, M.; Gershengorn, H.B.; Ferrando-Vivas, P.; Harrison, D.; Rowan, K.; Lindenauer, P.K.; Wunsch, H. Use of Mechanical Ventilation Across 3 Countries. JAMA Intern. Med. 2023, 183, 824–831. [Google Scholar] [CrossRef]
- Neto, A.S.; Tomlinson, G.; Sahetya, S.K.; Ball, L.; Nichol, A.D.; Hodgson, C.; Cavalcanti, A.B.; Briel, M.; Gama de Abreu, M.; Pelosi, P.; et al. Higher PEEP for acute respiratory distress síndrome: A Bayesain meta-analysis of randomized clinical trials. Crit. Care Resusc. 2021, 23, 171–182. [Google Scholar]
- Brun-Buisson, C.; Minelli, C.; Bertolini, G.; Brazzi, L.; Pimentel, J.; Lewandowski, K.; Bion, J.; Romand, J.-A.; Villar, J.; Thorsteinsson, A.; et al. Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med. 2004, 30, 51–61. [Google Scholar] [CrossRef]
- Romano, T.G.; Correia, M.D.T.; Mendes, P.V.; Zampieri, F.G.; Maciel, A.T.; Park, M. Metabolic acid-base adaptation triggered by acute persistent hypercapnia in mechanically ventilated patients with acute respiratory distress syndrome. Rev. Bras. Ter. Intensive 2016, 28, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Gendreau, S.; Geri, G.; Pham, T.; Vieillard-Baron, A.; Dessap, A.M. The role of acute hypercapnia on mortality and short-term physiology in patients mechanically ventilated for ARDS: A systematic review and meta-analysis. Intensive Care Med. 2022, 48, 517–534. [Google Scholar] [CrossRef] [PubMed]
- Schwager, E.; Jansson, K.; Rahman, A.; Schiffer, S.; Chang, Y.; Boverman, G.; Gross, B.; Xu-Wilson, M.; Boehme, P.; Truebel, H.; et al. Utilizing machine learning to improve clinical trial design for acute respiratory distress syndrome. NPJ Digit. Med. 2021, 4, 133. [Google Scholar] [CrossRef] [PubMed]
- Nuckton, T.J.; Alonso, J.A.; Kallet, R.H.; Daniel, B.M.; Pittet, J.-F.; Eisner, M.D.; Matthay, M.A. Pulmonary Dead-Space Fraction as a Risk Factor for Death in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2002, 346, 1281–1286. [Google Scholar] [CrossRef]
- Pozzi, T.; Fratti, I.; Tomarchio, E.; Bruno, G.; Catozzi, G.; Monte, A.; Chiumello, D.; Coppola, S. Early time-course of respiratory mechanics, mechanical power and gas exchange in ARDS patients. J. Crit. Care 2024, 79, 154444. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for some traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Development Cohort | Testing Cohort | ||||
|---|---|---|---|---|---|---|
| T0 n = 920 | T24 n = 920 | T72 n = 920 | T0 n = 253 | T24 n = 253 | T72 n = 253 | |
| SOFA score | 8.9 ± 3.3 | 8.9 ± 3.5 | 7.9 ± 3.9 | 9.7 ± 3.5 | 9.4 ± 3.9 | 8.3 ± 4.4 |
| FiO2 | 0.79 ± 0.19 | 0.65 ± 0.17 | 0.63 ± 0.20 | 0.76 ± 0.20 | 0.62 ± 0.16 | 0.57 ± 0.19 |
| PaO2, mmHg | 85.9 ± 25.8 | 91.8 ± 26.8 | 108.1 ± 35.2 | 86.6 ± 25.3 | 98.3 ± 30.5 | 107.6 ± 32.9 |
| PaO2/FiO2, mmHg | 114.4 ± 37.5 | 150.2 ± 57.3 | 196.0 ± 81.7 | 120.8 ± 40.3 | 170.0 ± 65.9 | 221.5 ± 84.6 |
| PaCO2, mmHg | 49.1 ± 12.5 | 46.6 ± 10.1 | 48.1 ± 9.5 | 50.3 ± 13.7 | 47.1 ± 9.9 | 47.2 ± 9.2 |
| pH | 7.31 ± 0.11 | 7.35 ± 0.08 | 7.40 ± 0.08 | 7.30 ± 0.11 | 7.35 ± 0.08 | 7.40 ± 0.07 |
| VT, ml/kg/PBW | 6.9 ± 1.0 | 6.8 ± 0.9 | 6.9 ± 1.1 | 6.7 ± 1.1 | 6.5 ± 1.1 | 6.6 ± 1.2 |
| Respiratory rate | 21.4 ± 4.9 | 23.3 ± 5.0 | 24.7 ± 5.2 | 22.3 ± 4.4 | 23.4 ± 4.8 | 24.2 ± 4.9 |
| PEEP, cmH2O | 12.1 ± 3.3 | 12.5 ± 3.0 | 11.5 ± 3.3 | 11.1 ± 3.0 | 11.8 ± 2.8 | 10.7 ± 3.0 |
| Pplat, cmH2O | 26.4 ± 4.9 | 26.6 ± 4.6 | 24.5 ± 4.7 | 25.0 ± 4.9 | 24.7 ± 4.5 | 22.4 ± 4.4 |
| Driving pressure, cmH2O | 14.4 ± 4.9 | 14.2 ± 4.5 | 13.0 ± 4.4 | 14.0 ± 4.5 | 12.9 ± 4.2 | 11.6 ± 3.8 |
| No. extrapulmonary OF | 1.6 ± 1.1 | 1.7 ± 1.1 | 1.5 ± 1.2 | 1.9 ± 1.1 | 1.9 ± 1.2 | 1.6 ± 1.3 |
| Variable | MV 3–14 Days n = 479 | MV > 14 Days n = 441 | Mean Difference (95%CI) | p |
|---|---|---|---|---|
| Age, yr, mean ± SD | 56.0 ± 16.8 | 57.1 ± 15.0 | 1.1 (−1 to 3.2) | 0.292 * |
| Sex, n (%) | 0.050 ¶ | |||
| Male | 311 (64.9) | 313 (71.0) | 6.1 (0.1 to 12.0) | |
| Female | 168 (35.1) | 128 (29.0) | 6.1 (0.1 to 12.0) | |
| Etiology, n (%) | 0.124 ¶ | |||
| Pneumonia | 226 (47.2) | 232 (52.6) | 5.4 (−1.6 to 11.8) | |
| Sepsis | 142 (29.6) | 104 (23.6) | 6.0 (0.3 to 11.6) | |
| Aspiration | 51 (10.6) | 39 (8.8) | 1.8 (−2.1 to 5.6) | |
| Trauma | 37 (7.7) | 35 (7.9) | 0.2 (−3.3 to 3.8) | |
| Others | 23 (4.8) | 31 (7.0) | 2.2 (−0.9 to 5.4) | |
| Degree of severity, n (%) | 0.195 ¶ | |||
| Severe | 183 (38.2) | 187 (42.4) | 4.2 (−2.1 to 10.5) | |
| Moderate | 296 (61.8) | 254 (57.6) | 4.2 (−2.1 to 10.5) | |
| APACHE II score | 20.2 ± 6.6 | 20.6 ± 6.1 | 0.4 (−0.4 to 1.2) | 0.352 * |
| SOFA score | 8.7 ± 3.5 | 9.1 ± 3.1 | 0.4 (−0.01 to 0.8) | 0.055 * |
| FiO2 | 0.79 ± 0.19 | 0.79 ± 0.19 | 0 (0 to 0) | 1.0 * |
| PaO2, mmHg | 87.8 ± 26.8 | 83.7 ± 24.5 | −4.1 (−7.5 to −0.8) | 0.016 * |
| PaO2/FiO2, mmHg | 117.3 ± 38.4 | 111.4 ± 36.3 | −5.9 (−10.7 to −1.1) | 0.017 * |
| PaCO2, mmHg | 48.4 ± 12.5 | 49.8 ± 12.4 | 1.4 (−0.1 to 3.1) | 0.074 * |
| pH | 7.31 ± 0.11 | 7.31 ± 0.10 | 0.0 (−0.01 to 0.01) | 1.0 * |
| VT, ml/Kg PBW | 6.9 ± 1.0 | 6.9 ± 1.0 | 0.0 (−0.1 to 0.1) | 0.770 * |
| Respiratory rate, cycles/min | 21.1 ± 4.9 | 21.7 ± 4.9 | 0.6 (−0.1 to 1.2) | 0.093 * |
| PEEP, cmH2O | 11.8 ± 3.3 | 12.3 ± 3.4 | 0.5 (0.03 to 0.9) | 0.036 * |
| Plateau pressure, cmH2O | 26.2 ± 5.0 | 26.6 ± 4.7 | 0.4 (−0.1 to 1.1) | 0.119 * |
| Driving pressure, cmH2O | 14.4 ± 4.9 | 14.4 ± 4.9 | 0 (−1.0 to 1.0) | 0.852 * |
| No. extrapulmonary OF | 1.5 ± 1.1 | 1.7 ± 1.0 | 0.2 (0.01 to 0.29) | 0.030 * |
| All-cause ICU mortality, n (%) | 155 (32.4) | 152 (34.5) | 2.1 (−4.0 to 8.2) | 0.500 ¶ |
| Time | Methods | Model | AUC (95%CI) | Sensitivity | Specificity | Accuracy | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| T0 (minimizing AIC) | Multilayer Perceptron | 9-variable | 0.66 (0.60–0.72) | 0.60 | 0.63 | 0.62 | 0.60 | 0.63 |
| Random Forest | 9-variable | 0.54 (0.47–0.60) | 0.46 | 0.60 | 0.53 | 0.51 | 0.55 | |
| Support Vector Machine | 9-variable | 0.51 (0.43–0.59) | 0.37 | 0.66 | 0.52 | 0.50 | 0.53 | |
| Logistic regression | 9-variable | 0.58 (0.52–0.64) | 0.63 | 0.55 | 0.59 | 0.58 | 0.64 | |
| T24 (minimizing AIC) | Multilayer Perceptron | 6-variable | 0.63 (0.56–0.69) | 0.76 | 0.44 | 0.59 | 0.56 | 0.67 |
| Random Forest | 6-variable | 0.54 (0.47–0.61) | 0.47 | 0.59 | 0.53 | 0.51 | 0.55 | |
| Support Vector Machine | 6-variable | 0.51 (0.43–0.59) | 0.40 | 0.64 | 0.52 | 0.50 | 0.54 | |
| Logistic regression | 6-variable | 0.58 (0.52–0.64) | 0.66 | 0.52 | 0.59 | 0.57 | 0.64 | |
| T72 (minimizing AIC) | Multilayer Perceptron | 11-variable | 0.71 (0.65–0.76) | 0.53 | 0.74 | 0.64 | 0.65 | 0.63 |
| Random Forest | 11-variable | 0.61 (0.55–0.68) | 0.46 | 0.68 | 0.57 | 0.57 | 0.58 | |
| Support Vector Machine | 11-variable | 0.55 (0.40–0.65) | 0.24 | 0.84 | 0.55 | 0.60 | 0.55 | |
| Logistic regression | 11-variable | 0.63 (0.57–0.69) | 0.64 | 0.61 | 0.62 | 0.61 | 0.66 | |
| T72 (minimizing BIC) | Multilayer Perceptron | 4-variable | 0.63 (0.57–0.70) | 0.49 | 0.69 | 0.60 | 0.60 | 0.60 |
| Random Forest | 4-variable | 0.58 (0.50–0.65) | 0.48 | 0.62 | 0.55 | 0.54 | 0.57 | |
| Support Vector Machine | 4-variable | 0.53 (0.41–0.63) | 0.50 | 0.58 | 0.54 | 0.52 | 0.56 | |
| Logistic regression | 4-variable | 0.62 (0.56–0.68) | 0.65 | 0.58 | 0.61 | 0.60 | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villar, J.; González-Martín, J.M.; Fernández, C.; Soler, J.A.; Ambrós, A.; Pita-García, L.; Fernández, L.; Ferrando, C.; Arocas, B.; González-Vaquero, M.; et al. Predicting the Length of Mechanical Ventilation in Acute Respiratory Disease Syndrome Using Machine Learning: The PIONEER Study. J. Clin. Med. 2024, 13, 1811. https://doi.org/10.3390/jcm13061811
Villar J, González-Martín JM, Fernández C, Soler JA, Ambrós A, Pita-García L, Fernández L, Ferrando C, Arocas B, González-Vaquero M, et al. Predicting the Length of Mechanical Ventilation in Acute Respiratory Disease Syndrome Using Machine Learning: The PIONEER Study. Journal of Clinical Medicine. 2024; 13(6):1811. https://doi.org/10.3390/jcm13061811
Chicago/Turabian StyleVillar, Jesús, Jesús M. González-Martín, Cristina Fernández, Juan A. Soler, Alfonso Ambrós, Lidia Pita-García, Lorena Fernández, Carlos Ferrando, Blanca Arocas, Myriam González-Vaquero, and et al. 2024. "Predicting the Length of Mechanical Ventilation in Acute Respiratory Disease Syndrome Using Machine Learning: The PIONEER Study" Journal of Clinical Medicine 13, no. 6: 1811. https://doi.org/10.3390/jcm13061811
APA StyleVillar, J., González-Martín, J. M., Fernández, C., Soler, J. A., Ambrós, A., Pita-García, L., Fernández, L., Ferrando, C., Arocas, B., González-Vaquero, M., Añón, J. M., González-Higueras, E., Parrilla, D., Vidal, A., Fernández, M. M., Rodríguez-Suárez, P., Fernández, R. L., Gómez-Bentolila, E., Burns, K. E. A., ... the PredictION of Duration of mEchanical vEntilation in ARDS (PIONEER) Network. (2024). Predicting the Length of Mechanical Ventilation in Acute Respiratory Disease Syndrome Using Machine Learning: The PIONEER Study. Journal of Clinical Medicine, 13(6), 1811. https://doi.org/10.3390/jcm13061811