
Improved Oral Health Is Associated with a Lower Risk of Late Onset Ankylosing Spondylitis: A Nationwide Cohort Study

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
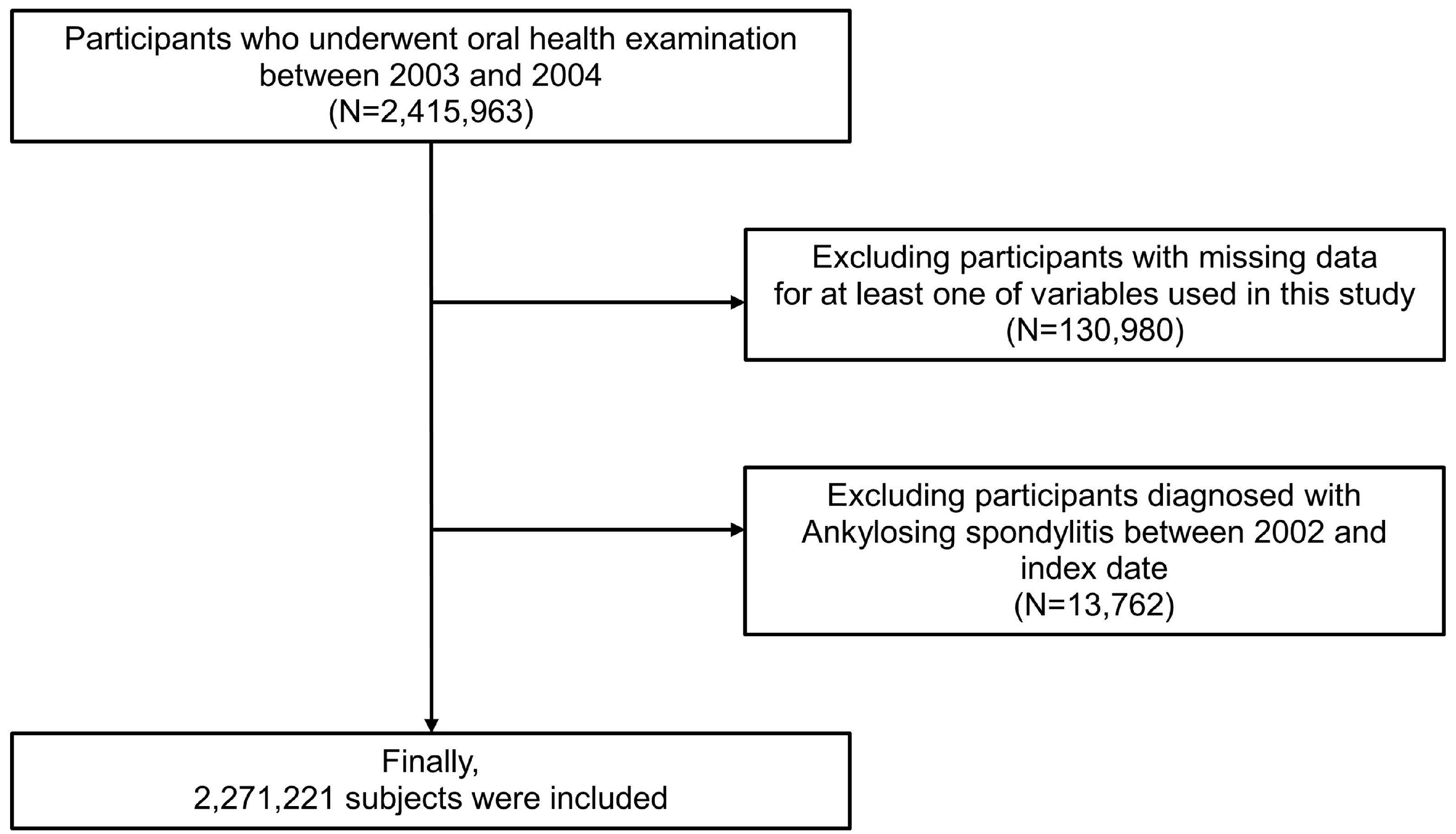
2.2. Study Population
2.3. Definition and Variables
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | Ankylosing spondylitis |
| ASAS | Assessment of SpondyloArthritis International Society |
| BASMI | Bath Ankylosing Spondylitis Metrology Index |
| BMI | Body mass index |
| BOP | Bleeding on probing |
| CAL | Clinical attachment loss |
| CI | Confidence interval |
| HEALS | Health screening |
| HLA-B27 | Human Leukocyte Antigen B27 |
| HR | Hazard ratio |
| IBD | Inflammatory bowel disease |
| ICBP | Individual copayment beneficiaries program |
| ICD | International classification of diseases |
| IL | Interleukin |
| MASES | Maastricht Ankylosing Spondylitis Enthesitis Score |
| NHIS | National Health Insurance Service |
| PAD | PeptidylArginine Deiminase |
| PSM | Propensity score matching |
| RA | Rheumatoid arthritis |
| RID | Rare and intractable diseases |
| SLE | Systemic lupus erythematosus |
| SMD | Standardized mean difference |
Appendix A
References
- Ranganathan, V.; Gracey, E.; Brown, M.A.; Inman, R.D.; Haroon, N. Pathogenesis of ankylosing spondylitis—Recent advances and future directions. Nat. Rev. Rheumatol. 2017, 13, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Dean, L.E.; Jones, G.T.; MacDonald, A.G.; Downham, C.; Sturrock, R.D.; Macfarlane, G.J. Global prevalence of ankylosing spondylitis. Rheumatology 2014, 53, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Toussirot, E. Late-onset ankylosing spondylitis and spondylarthritis: An update on clinical manifestations, differential diagnosis and pharmacological therapies. Drugs Aging 2010, 27, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The assessment of spondyloarthritis international society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann. Rheum. Dis. 2011, 70, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Ramadan, D.E.; Hariyani, N.; Indrawati, R.; Ridwan, R.D.; Diyatri, I. Cytokines and chemokines in periodontitis. Eur. J. Dent. 2020, 14, 483–495. [Google Scholar] [CrossRef]
- Ray, R.R. Periodontitis: An oral disease with severe consequences. Appl. Biochem. Biotechnol. 2023, 195, 17–32. [Google Scholar] [CrossRef]
- Cecoro, G.; Annunziata, M.; Iuorio, M.T.; Nastri, L.; Guida, L. Periodontitis, low-grade inflammation and systemic health: A scoping review. Medicina 2020, 56, 272. [Google Scholar] [CrossRef]
- Penoni, D.C.; Vettore, M.V.; Torres, S.R.; Farias, M.L.F.; Leão, A.T.T. An investigation of the bidirectional link between osteoporosis and periodontitis. Arch. Osteoporos. 2019, 14, 94. [Google Scholar] [CrossRef]
- Krutyhołowa, A.; Strzelec, K.; Dziedzic, A.; Bereta, G.P.; Łazarz-Bartyzel, K.; Potempa, J.; Gawron, K. Host and bacterial factors linking periodontitis and rheumatoid arthritis. Front. Immunol. 2022, 13, 980805. [Google Scholar] [CrossRef]
- Pessoa, L.; Aleti, G.; Choudhury, S.; Nguyen, D.; Yaskell, T.; Zhang, Y.; Li, W.; Nelson, K.E.; Neto, L.L.S.; Sant’Ana, A.C.P.; et al. Host-microbial interactions in systemic lupus erythematosus and periodontitis. Front. Immunol. 2019, 10, 2602. [Google Scholar] [CrossRef]
- Bunte, K.; Beikler, T. Th17 cells and the il-23/il-17 axis in the pathogenesis of periodontitis and immune-mediated inflammatory diseases. Int. J. Mol. Sci. 2019, 20, 3394. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Huang, N.; Chen, Y.M.; Chen, T.J.; Chou, P.; Lee, Y.L.; Chou, Y.J.; Lan, J.L.; Lai, K.L.; Lin, C.H.; et al. Association between a history of periodontitis and the risk of rheumatoid arthritis: A nationwide, population-based, case-control study. Ann. Rheum. Dis. 2013, 72, 1206–1211. [Google Scholar] [CrossRef] [PubMed]
- Arkema, E.V.; Karlson, E.W.; Costenbader, K.H. A prospective study of periodontal disease and risk of rheumatoid arthritis. J. Rheumatol. 2010, 37, 1800–1804. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Van Dyke, T.E. Periodontitis and atherosclerotic cardiovascular disease: Consensus report of the joint efp/aapworkshop on periodontitis and systemic diseases. J. Periodontol. 2013, 84 (Suppl. S4), S24–S29. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef]
- Pischon, N.; Pischon, T.; Gülmez, E.; Kröger, J.; Purucker, P.; Kleber, B.M.; Landau, H.; Jost-Brinkmann, P.G.; Schlattmann, P.; Zernicke, J.; et al. Periodontal disease in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2010, 69, 34–38. [Google Scholar] [CrossRef]
- Keller, J.J.; Kang, J.H.; Lin, H.C. Association between ankylosing spondylitis and chronic periodontitis: A population-based study. Arthritis Rheum. 2013, 65, 167–173. [Google Scholar] [CrossRef]
- Kang, E.H.; Lee, J.T.; Lee, H.J.; Lee, J.Y.; Chang, S.H.; Cho, H.J.; Choi, B.Y.; Ha, Y.J.; Park, K.U.; Song, Y.W.; et al. Chronic periodontitis is associated with spinal dysmobility in patients with ankylosing spondylitis. J. Periodontol. 2015, 86, 1303–1313. [Google Scholar] [CrossRef]
- Pandey, A.; Rajak, R.; Pandey, M. Periodontal diseases and its association with disease activity in ankylosing spondylitis/spa: A systematic review. Eur. J. Rheumatol. 2021, 8, 168–179. [Google Scholar] [CrossRef]
- Daltaban, Ö.; Enginar, A.; Üstün, K.; Hatipoğlu, M.; Kaçar, C.; Tuncer, T. Evaluating the relationship between ankylosing spondylitis and periodontal disease: A case-control study. Clin. Oral. Investig. 2023, 27, 411–420. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The national health insurance service-national health screening cohort (nhis-heals) in korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef]
- Park, M.S.; Jeon, J.; Song, T.J.; Kim, J. Association of periodontitis with microvascular complications of diabetes mellitus: A nationwide cohort study. J. Diabetes Complicat. 2022, 36, 108107. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, S.H.; Kim, S.J.; Kim, J.W. Recovery from chronic periodontal disease is associated with lower risk for incident diabetes. J. Clin. Periodontol. 2022, 49, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Woo, H.G.; Lee, J.S.; Song, T.J. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 2021, 92, 87–94. [Google Scholar] [CrossRef]
- Song, T.J.; Chang, Y.; Jeon, J.; Kim, J. Oral health and longitudinal changes in fasting glucose levels: A nationwide cohort study. PLoS ONE 2021, 16, e0253769. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the new york criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef]
- Sezer, U.; Erciyas, K.; Pehlivan, Y.; Ustün, K.; Tarakçioğlu, M.; Senyurt, S.Z.; Onat, A.M. Serum cytokine levels and periodontal parameters in ankylosing spondylitis. J. Periodontal Res. 2012, 47, 396–401. [Google Scholar] [CrossRef]
- Ziebolz, D.; Douglas, D.; Douglas, D.; Schmickler, J.; Patschan, D.; Müller, G.A.; Haak, R.; Schmidt, J.; Schmalz, G.; Patschan, S. Periodontal condition is associated with disease duration and motoric disabilities in patients with ankylosing spondylitis: Results of a cross-sectional study. Rheumatol. Int. 2018, 38, 855–863. [Google Scholar] [CrossRef]
- Ratz, T.; Dean, L.E.; Atzeni, F.; Reeks, C.; Macfarlane, G.J.; Macfarlane, T.V. A possible link between ankylosing spondylitis and periodontitis: A systematic review and meta-analysis. Rheumatology 2015, 54, 500–510. [Google Scholar] [CrossRef]
- Białowąs, K.; Radwan-Oczko, M.; Duś-Ilnicka, I.; Korman, L.; Świerkot, J. Periodontal disease and influence of periodontal treatment on disease activity in patients with rheumatoid arthritis and spondyloarthritis. Rheumatol. Int. 2020, 40, 455–463. [Google Scholar] [CrossRef]
- Montilla, C.; Del Pino-Montes, J.; Collantes-Estevez, E.; Font, P.; Zarco, P.; Mulero, J.; Gratacós, J.; Rodríguez, C.; Juanola, X.; Fernández-Sueiro, J.L.; et al. Clinical features of late-onset ankylosing spondylitis: Comparison with early-onset disease. J. Rheumatol. 2012, 39, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Karaarslan, A.; Yilmaz, H.; Aycan, H.; Orman, M.; Kobak, S. Demographic, clinical, and laboratory features of turkish patients with late onset ankylosing spondylitis. Bosn. J. Basic. Med. Sci. 2015, 15, 64–67. [Google Scholar] [CrossRef]
- Endo, Y.; Fujikawa, K.; Koga, T.; Mizokami, A.; Mine, M.; Tsukada, T.; Uetani, M.; Kawakami, A. Characteristics of late-onset spondyloarthritis in japan: A retrospective cohort study. Medicine 2019, 98, e14431. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Bartl, M.; Schmickler, J.; Patschan, S.; Patschan, D.; Ziebolz, D. Tooth loss is associated with disease-related parameters in patients with rheumatoid arthritis and ankylosing spondylitis-a cross-sectional study. J. Clin. Med. 2021, 10, 3052. [Google Scholar] [CrossRef] [PubMed]
- Abbood, H.M.; Pathan, E.; Cherukara, G.P. The link between ankylosing spondylitis and oral health conditions: Two nested case-control studies using data of the uk biobank. J. Appl. Oral. Sci. 2018, 27, e20180207. [Google Scholar] [CrossRef] [PubMed]
- Zelig, R.; Goldstein, S.; Touger-Decker, R.; Firestone, E.; Golden, A.; Johnson, Z.; Kaseta, A.; Sackey, J.; Tomesko, J.; Parrott, J.S. Tooth loss and nutritional status in older adults: A systematic review and meta-analysis. JDR Clin. Trans. Res. 2022, 7, 4–15. [Google Scholar] [CrossRef]
- Chawla, M.; Gupta, R.; Das, B. Gut microbiome dysbiosis in malnutrition. Prog. Mol. Biol. Transl. Sci. 2022, 192, 205–229. [Google Scholar]
- D’Aiuto, F.; Nibali, L.; Parkar, M.; Suvan, J.; Tonetti, M.S. Short-term effects of intensive periodontal therapy on serum inflammatory markers and cholesterol. J. Dent. Res. 2005, 84, 269–273. [Google Scholar] [CrossRef]
- Lee, K.; Lee, J.S.; Kim, J.; Lee, H.; Chang, Y.; Woo, H.G.; Kim, J.W.; Song, T.J. Oral health and gastrointestinal cancer: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 796–808. [Google Scholar] [CrossRef]
- Taurog, J.D.; Richardson, J.A.; Croft, J.T.; Simmons, W.A.; Zhou, M.; Fernández-Sueiro, J.L.; Balish, E.; Hammer, R.E. The germfree state prevents development of gut and joint inflammatory disease in hla-b27 transgenic rats. J. Exp. Med. 1994, 180, 2359–2364. [Google Scholar] [CrossRef] [PubMed]
- Rehaume, L.M.; Mondot, S.; Aguirre de Cárcer, D.; Velasco, J.; Benham, H.; Hasnain, S.Z.; Bowman, J.; Ruutu, M.; Hansbro, P.M.; McGuckin, M.A.; et al. Zap-70 genotype disrupts the relationship between microbiota and host, leading to spondyloarthritis and ileitis in skg mice. Arthritis Rheumatol. 2014, 66, 2780–2792. [Google Scholar] [CrossRef] [PubMed]
- Ogrendik, M. Periodontal pathogens are likely to be responsible for the development of ankylosing spondylitis. Curr. Rheumatol. Rev. 2015, 11, 47–49. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Total | Periodontitis (−) | Periodontitis (+) | p-Value |
|---|---|---|---|---|
| Number of participants (%) | 2,271,221 (100.0) | 2,153,217 | 118,004 | <0.0001 |
| Age, years | 42.14 ± 12.75 | 42.08 ± 12.72 | 43.29 ± 13.32 | <0.0001 |
| <65 | 2,136,898 (94.1) | 2,028,391 (94.2) | 108,507 (92.0) | |
| ≥65 | 134,323 (5.9) | 124,826 (5.7) | 9497 (8.0) | |
| Sex | <0.0001 | |||
| Male | 1,505,305 (66.3) | 1,422,811 (66.1) | 82,494 (69.9) | |
| Female | 765,916 (33.7) | 730,406 (33.9) | 35,510 (30.1) | |
| Body mass index (kg/m2) | 23.54 ± 14.22 | 23.53 ± 14.19 | 23.68 ± 14.75 | <0.0001 |
| Household income | <0.0001 | |||
| Q1, lowest | 590,312 (26.0) | 560,074 (26.0) | 30,238 (25.6) | |
| Q2 | 821,367 (36.2) | 778,034 (36.1) | 43,333 (36.7) | |
| Q3 | 597,235 (26.3) | 565,897 (26.3) | 31,338 (26.6) | |
| Q4, highest | 262,307 (11.6) | 249,212 (11.6) | 13,095 (11.1) | |
| Smoking status | <0.0001 | |||
| Never | 1,273,168 (56.1) | 1,208,682 (56.1) | 64,486 (54.6) | |
| Former | 244,362 (10.8) | 230,468 (10.7) | 13,894 (11.8) | |
| Current | 753,691 (33.2) | 714,067 (33.2) | 39,624 (33.6) | |
| Alcohol consumption (days/week) | <0.0001 | |||
| None | 1,518,140 (66.8) | 1,440,863 (66.9) | 77,277 (65.5) | |
| 1–4 | 694,720 (30.6) | 657,789 (30.6) | 36,931 (31.3) | |
| ≥5 | 58,361 (2.6) | 54,565 (2.5) | 3796 (3.2) | |
| Regular physical activity (days/week) | <0.0001 | |||
| None | 1,183,012 (52.1) | 1,121,610 (52.1) | 61,402 (52.0) | |
| 1–4 | 926,030 (40.8) | 878,599 (40.8) | 47,431 (40.2) | |
| ≥5 | 162,179 (7.1) | 153,008 (7.1) | 9171 (7.8) | |
| Comorbidities | ||||
| Hypertension | 656,672 (28.9) | 620,352 (28.8) | 36,320 (30.8) | <0.0001 |
| Diabetes mellitus | 156,574 (6.9) | 146,373 (6.8) | 10,201 (8.6) | <0.0001 |
| Dyslipidemia | 292,308 (12.9) | 276,226 (12.8) | 16,082 (13.6) | <0.0001 |
| Atrial fibrillation | 8513 (0.4) | 7816 (0.4) | 697 (0.6) | <0.0001 |
| Cancer | 21,733 (1.0) | 19,799 (0.9) | 1934 (1.6) | <0.0001 |
| Renal disease | 21,010 (0.9) | 19,443 (0.9) | 1567 (1.3) | <0.0001 |
| Rheumatoid arthritis | 7982 (0.4) | 7325 (0.3) | 657 (0.6) | <0.0001 |
| Systemic lupus erythematosus | 1415 (0.1) | 1312 (0.1) | 103 (0.1) | 0.001 |
| Oral hygiene behaviors | ||||
| Frequency of tooth brushing (times/day) | <0.0001 | |||
| 0–1 | 312,664 (13.8) | 295,522 (13.7) | 17,142 (14.5) | |
| 2 | 1,036,201 (45.6) | 981,304 (45.6) | 54,897 (46.5) | |
| ≥3 | 922,356 (40.6) | 876,391 (40.7) | 45,965 (39.0) | |
| Number of missing teeth | <0.0001 | |||
| 0 | 1,871,990 (82.4) | 1,776,314 (82.5) | 95,676 (81.1) | |
| 1–7 | 365,959 (16.1) | 345,952 (16.1) | 20,007 (17.0) | |
| 8–14 | 19,431 (0.9) | 18,037 (0.8) | 1394 (1.2) | |
| ≥15 | 13,841 (0.6) | 12,914 (0.6) | 927 (0.7) | |
| Dental visit for any reason | <0.0001 | |||
| No | 1,360,869 (59.9) | 1,292,701 (60.0) | 68,168 (57.8) | |
| Yes | 910,352 (40.1) | 860,516 (40.0) | 49,836 (42.2) | |
| Dental Scaling | <0.0001 | |||
| No | 1,748,018 (80.0) | 1,658,214 (77.0) | 89,804 (76.1) | |
| Yes | 523,203 (23.0) | 495,003 (23.0) | 28,200 (23.9) |
| Variable | Before PSM (n = 2,271,221) | After PSM (n = 590,014) | SMD | |||
|---|---|---|---|---|---|---|
| Periodontitis (−) | Periodontitis (+) | p-Value | Periodontitis (−) | Periodontitis (+) | ||
| Number of participants (%) | 2,153,217 | 118,004 | <0.0001 | 472,010 | 118,004 | |
| Age, years | 42.08 ± 12.72 | 43.29 ± 13.32 | <0.0001 | 43.12 ± 13.28 | 43.29 ± 13.32 | 0.001 |
| <65 | 2,028,391 (94.2) | 108,507 (92.0) | 433,836 (91.9) | 108,507 (92.0) | ||
| ≥65 | 124,826 (5.7) | 9497 (8.0) | 38,174 (80.1) | 9497 (8.1) | ||
| Sex | <0.0001 | −0.014 | ||||
| Male | 1,422,811 (66.1) | 82,494 (69.9) | 332,514 (70.5) | 82,494 (69.9) | ||
| Female | 730,406 (33.9) | 35,510 (30.1) | 139,496 (29.5) | 35,510 (30.1) | ||
| Body mass index (kg/m2) | 23.53 ± 14.19 | 23.68 ± 14.75 | <0.0001 | 23.6 ± 18.3 | 23.68 ± 14.75 | 0.003 |
| Household income | <0.0001 | 0.007 | ||||
| Q1, lowest | 560,074 (26.0) | 30,238 (25.6) | 122,565 (26.0) | 30,238 (25.6) | ||
| Q2 | 778,034 (36.1) | 43,333 (36.7) | 172,197 (36.5) | 43,333 (36.7) | ||
| Q3 | 565,897 (26.3) | 31,338 (26.6) | 125,149 (26.5) | 31,338 (26.6) | ||
| Q4, highest | 249,212 (11.6) | 13,095 (11.1) | 52,099 (11.0) | 13,095 (11.1) | ||
| Smoking status | <0.0001 | −0.002 | ||||
| Never | 1208,682 (56.1) | 64,486 (54.7) | 257,923 (54.6) | 64,486 (54.6) | ||
| Former | 230,468 (10.7) | 13,894 (11.8) | 52,614 (11.2) | 13,894 (11.8) | ||
| Current | 714,067 (33.2) | 39,624 (33.6) | 161,473 (34.2) | 39,624 (33.6) | ||
| Alcohol consumption (days/week) | <0.0001 | 0.003 | ||||
| None | 1,440,863 (66.9) | 77,277 (65.5) | 308,396 (65.3) | 77,277 (65.5) | ||
| 1–4 | 657,789 (30.6) | 36,931 (31.3) | 149,401 (31.7) | 36,931 (31.3) | ||
| ≥5 | 54,565 (2.5) | 3796 (3.2) | 14,213 (3.0) | 3796 (3.2) | ||
| Regular physical activity (days/week) | <0.0001 | 0.009 | ||||
| None | 1,121,610 (52.1) | 61,402 (52.0) | 245,126 (51.9) | 61,402 (52.0) | ||
| 1–4 | 878,599 (40.8) | 47,431 (40.2) | 193,179 (40.9) | 47,431 (40.2) | ||
| ≥5 | 153,008 (7.1) | 9171 (7.8) | 33,705 (7.1) | 9171 (7.8) | ||
| Comorbidities | ||||||
| Hypertension | 620,352 (28.8) | 36,320 (30.8) | <0.0001 | 140,890 (29.9) | 36,320 (30.8) | −0.014 |
| Diabetes mellitus | 146,373 (6.8) | 10,201 (8.6) | <0.0001 | 40,291 (8.5) | 10,201 (8.6) | −0.015 |
| Dyslipidemia | 276,226 (12.8) | 16,082 (13.6) | <0.0001 | 61,914 (13.1) | 16,082 (13.6) | −0.033 |
| Atrial fibrillation | 7816 (0.4) | 697 (0.6) | <0.0001 | 2788 (0.6) | 697 (0.6) | −0.004 |
| Cancer | 19,799 (0.9) | 1934 (1.6) | <0.0001 | 7827 (1.7) | 1934 (1.6) | 0.002 |
| Renal disease | 19,443 (0.9) | 1567 (1.3) | <0.0001 | 6239 (1.3) | 1567 (1.3) | −0.004 |
| Rheumatoid arthritis | 7325 (0.3) | 657 (0.6) | <0.0001 | 2699 (0.6) | 657 (0.6) | −0.001 |
| Systemic lupus erythematosus | 1312 (0.1) | 103 (0.1) | 0.001 | 413 (0.1) | 103 (0.1) | 0.001 |
| Oral hygiene behaviors | ||||||
| Frequency of tooth brushing (times/day) | <0.0001 | −0.010 | ||||
| 0–1 | 295,522 (13.7) | 17,142 (14.5) | 67,291 (14.3) | 17,142 (14.5) | ||
| 2 | 981,304 (45.6) | 54,897 (46.5) | 219,403 (46.5) | 54,897 (46.5) | ||
| ≥3 | 876,391 (40.7) | 45,965 (39.0) | 185,316 (39.3) | 45,965 (39.0) | ||
| Number of missing teeth | <0.0001 | 0.021 | ||||
| 0 | 1,776,314 (82.5) | 95,676 (81.1) | 385,229 (81.6) | 95,676 (81.1) | ||
| 1–7 | 345,952 (16.1) | 20,007 (17.0) | 78,160 (16.6) | 20,007 (16.9) | ||
| 8–14 | 18,037 (0.8) | 1394 (1.2) | 4787 (1.0) | 1394 (1.2) | ||
| ≥15 | 12,914 (0.6) | 927 (0.8) | 3834 (0.8) | 927 (0.8) | ||
| Dental visit for any reason | <0.0001 | 0.001 | ||||
| No | 1,292,701 (60.0) | 68,168 (57.8) | 274,845 (58.2) | 68,168 (57.8) | ||
| Yes | 860,516 (40.0) | 49,836 (42.2) | 197,165 (41.8) | 49,836 (42.2) | ||
| Dental Scaling | <0.0001 | −0.005 | ||||
| No | 1,658,214 (77.0) | 89,804 (76.1) | 360,699 (76.4) | 89,804 (76.1) | ||
| Yes | 495,003 (23.0) | 28,200 (23.9) | 111,311 (23.6) | 28,200 (23.9) | ||
| Number of Participants | Number of Events | Event Rate (%)(95% CI) | Person-Years | Incidence Rate(per 1000 Person-Years) | Adjusted HR(95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|
| Oral health status | |||||||
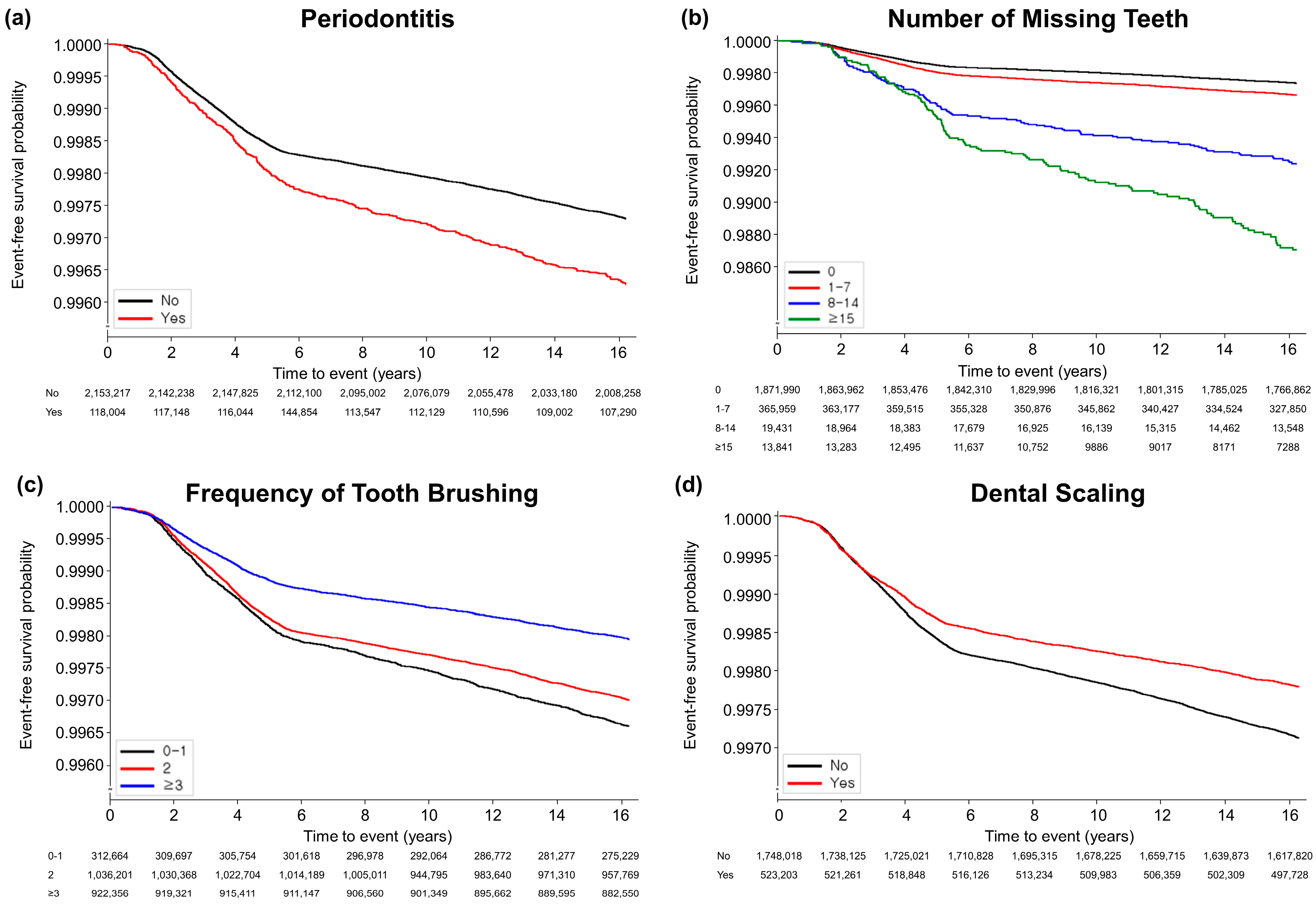
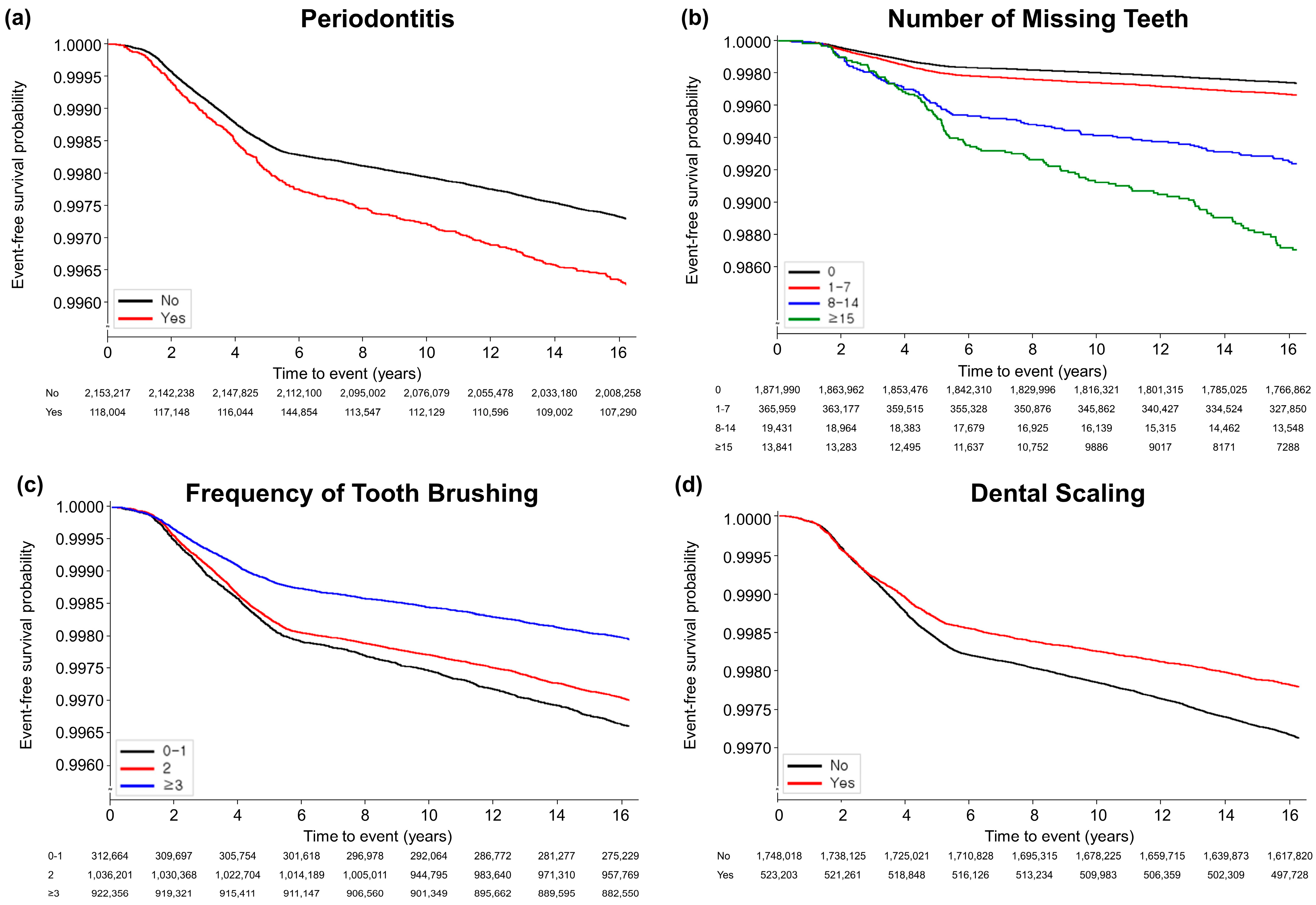
| Periodontitis | |||||||
| No | 2,153,217 | 5912 | 0.27 (0.27, 0.28) | 35,309,467.51 | 0.17 | 1 (reference) | |
| Yes | 118,004 | 454 | 0.38 (0.35, 0.42) | 1,898,712.29 | 0.24 | 1.33 (1.20, 1.46) | <0.0001 |
| Number of missing teeth | |||||||
| 0 | 1,871,990 | 4862 | 0.26 (0.25, 0.27) | 30,838,486.07 | 0.16 | 1 (reference) | |
| 1–7 | 365,959 | 1215 | 0.33 (0.31, 0.35) | 5,904,907.22 | 0.21 | 1.12 (1.05, 1.19) | 0.001 |
| 8–14 | 19,431 | 140 | 0.72 (0.60, 0.84) | 284,109.54 | 0.49 | 1.44 (1.22, 1.72) | <0.0001 |
| ≥15 | 13,841 | 149 | 1.08 (0.90, 1.25) | 180,676.98 | 0.82 | 1.68 (1.42, 1.99) | <0.0001 |
| Oral hygiene behaviors | |||||||
| Frequency of tooth brushing (times/day) | |||||||
| 0–1 | 312,664 | 1118 | 0.36 (0.34, 0.38) | 5,019,097.36 | 0.22 | 1 (reference) | |
| 2 | 1,036,201 | 3261 | 0.31 (0.30, 0.33) | 16,953,586.96 | 0.19 | 0.99 (0.92, 1.06) | 0.683 |
| ≥3 | 922,356 | 1987 | 0.22 (0.21, 0.22) | 15,235,495.48 | 0.13 | 0.77 (0.71, 0.83) | <0.0001 |
| Dental visit for any reason | |||||||
| No | 1,360,869 | 3977 | 0.29 (0.28, 0.30) | 22,237,856.02 | 0.18 | 1 (reference) | |
| Yes | 910,352 | 2389 | 0.26 (0.25, 0.27) | 14,970,323.78 | 0.16 | 0.98 (0.93, 1.04) | 0.485 |
| Dental scaling | |||||||
| No | 1,748,018 | 5183 | 0.30 (0.29, 0.30) | 28,562,069.05 | 0.18 | 1 (reference) | |
| Yes | 523,203 | 1183 | 0.23 (0.21, 0.24) | 8,646,110.75 | 0.14 | 0.88 (0.82, 0.95) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, M.K.; Chang, Y.; Park, J.-H.; Leem, G.H.; Song, T.-J. Improved Oral Health Is Associated with a Lower Risk of Late Onset Ankylosing Spondylitis: A Nationwide Cohort Study. J. Clin. Med. 2024, 13, 1606. https://doi.org/10.3390/jcm13061606
Chung MK, Chang Y, Park J-H, Leem GH, Song T-J. Improved Oral Health Is Associated with a Lower Risk of Late Onset Ankylosing Spondylitis: A Nationwide Cohort Study. Journal of Clinical Medicine. 2024; 13(6):1606. https://doi.org/10.3390/jcm13061606
Chicago/Turabian StyleChung, Min Kyung, Yoonkyung Chang, Jung-Hyun Park, Gwang Hyun Leem, and Tae-Jin Song. 2024. "Improved Oral Health Is Associated with a Lower Risk of Late Onset Ankylosing Spondylitis: A Nationwide Cohort Study" Journal of Clinical Medicine 13, no. 6: 1606. https://doi.org/10.3390/jcm13061606
APA StyleChung, M. K., Chang, Y., Park, J.-H., Leem, G. H., & Song, T.-J. (2024). Improved Oral Health Is Associated with a Lower Risk of Late Onset Ankylosing Spondylitis: A Nationwide Cohort Study. Journal of Clinical Medicine, 13(6), 1606. https://doi.org/10.3390/jcm13061606