
Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease
 ,
,
Abstract
1. Introduction
- -
- External compression of the main left coronary artery by the dilated PA;
- -
- PA dissection/rupture (with angina, hemoptysis, tamponade, or hemothorax—according to the site of rupture);
- -
- PA thrombosis (from asymptomatic to severe forms with hemoptysis);
- -
- Airway compression;
- -
- Recurrent laryngeal nerve compression.
2. The Aim of This Study
3. Patients and Methods
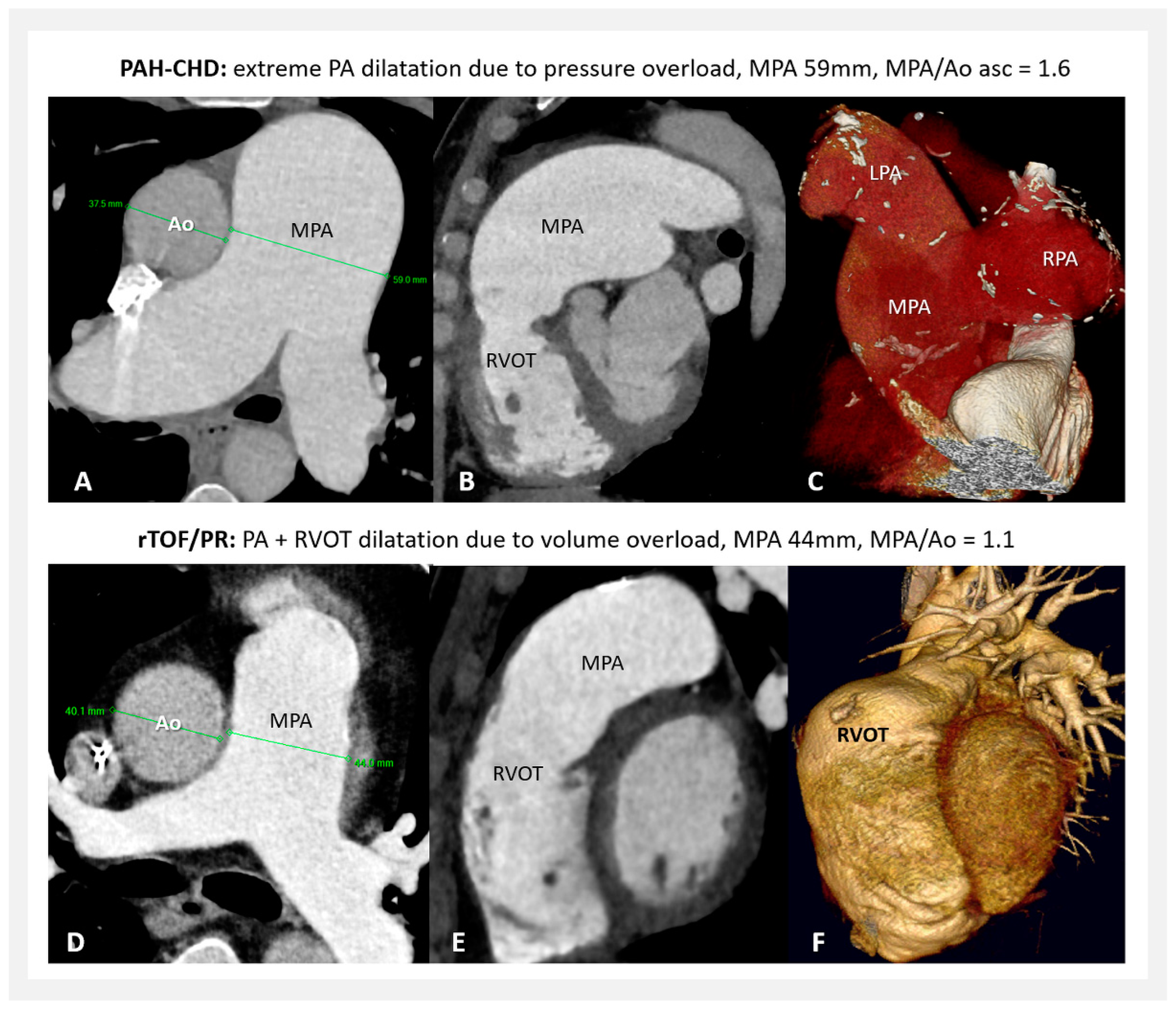
- Sixty patients with pulmonary arterial hypertension associated with congenital heart defect (PAH-CHD) (47 patients with unoperated shunt defects; 10 after surgical or interventional shunt closure, or with small defects; and 3 with congenital portopulmonary PH); all with the long-term (median 15 years) confirmed hemodynamics of severe pulmonary artery pressure overload (with mean pulmonary artery pressure 60 mmHg (median), and pulmonary vascular resistance 9.3 Wood units (median)).
- Sixty-four patients with a repaired Tetralogy of Fallot with isolated “free” pulmonary regurgitation (rTOF/PR) had the hemodynamics of pure proximal pulmonary artery volume overload. The median age at complete TOF repair was 5 years, and the median follow-up after repair was 22 years. The PA data analysis was performed at the time period before any reintervention due to pulmonary regurgitation was performed. In this study, patients with Tetralogy of Fallot with absent pulmonary valve syndrome, patients with pulmonary conduit or any other valve implantation during primary complete repair, or patients with any presence of significant (valvar, subvalvar, or supravalvar) pulmonary stenosis or significant pulmonary artery branch deformation during follow-up were not included.
- In this study, 80 age-matched healthy volunteers without any significant cardiac disease, with normal structural and functional findings, without systemic or pulmonary hypertension, without arrhythmia, or any known chronic diseases like diabetes or connective tissue disease (NORMAL) were included.
Statistical Analysis
4. Results
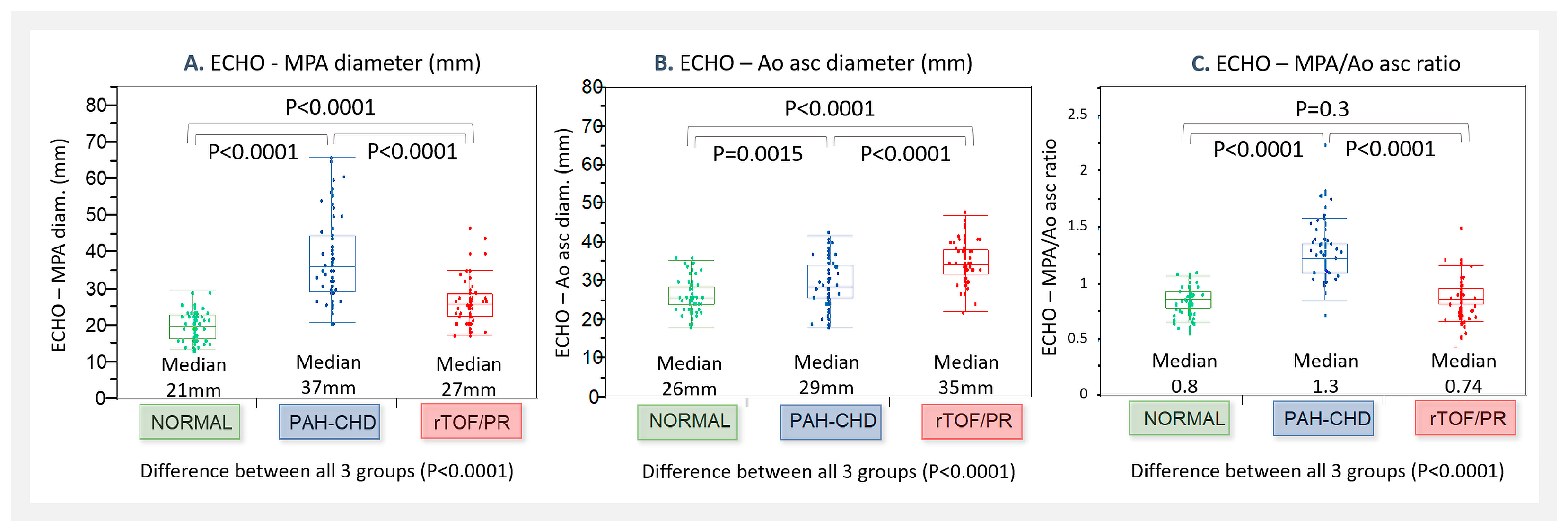
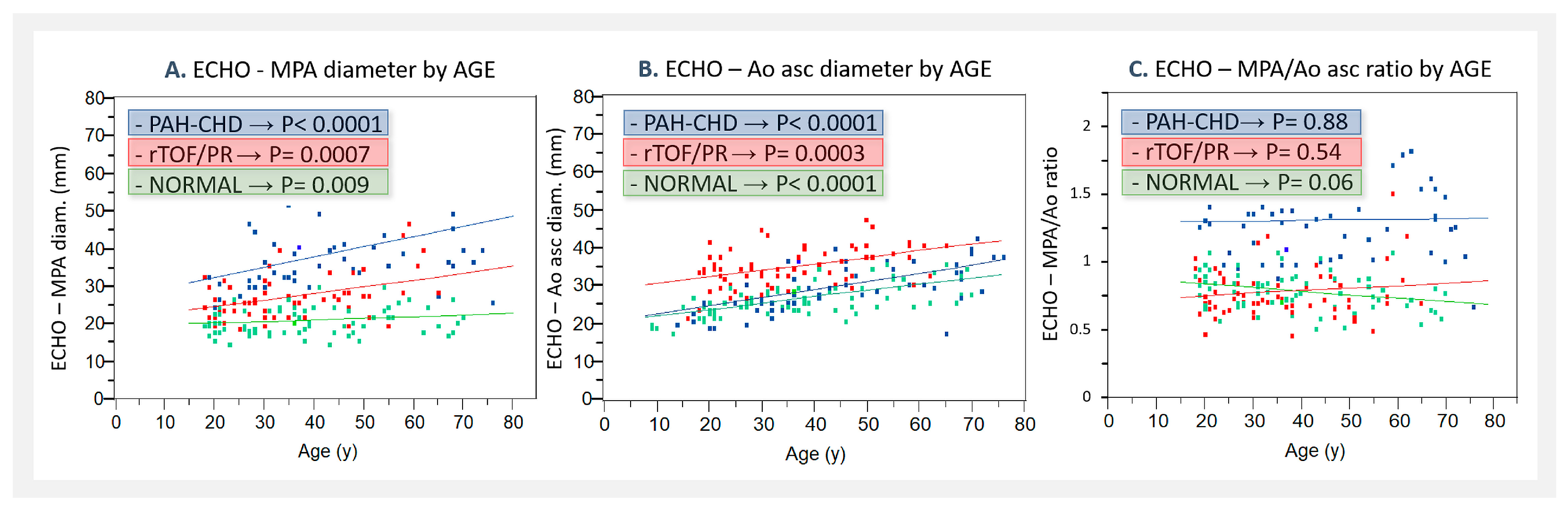
4.1. Echocardiographic Parameters
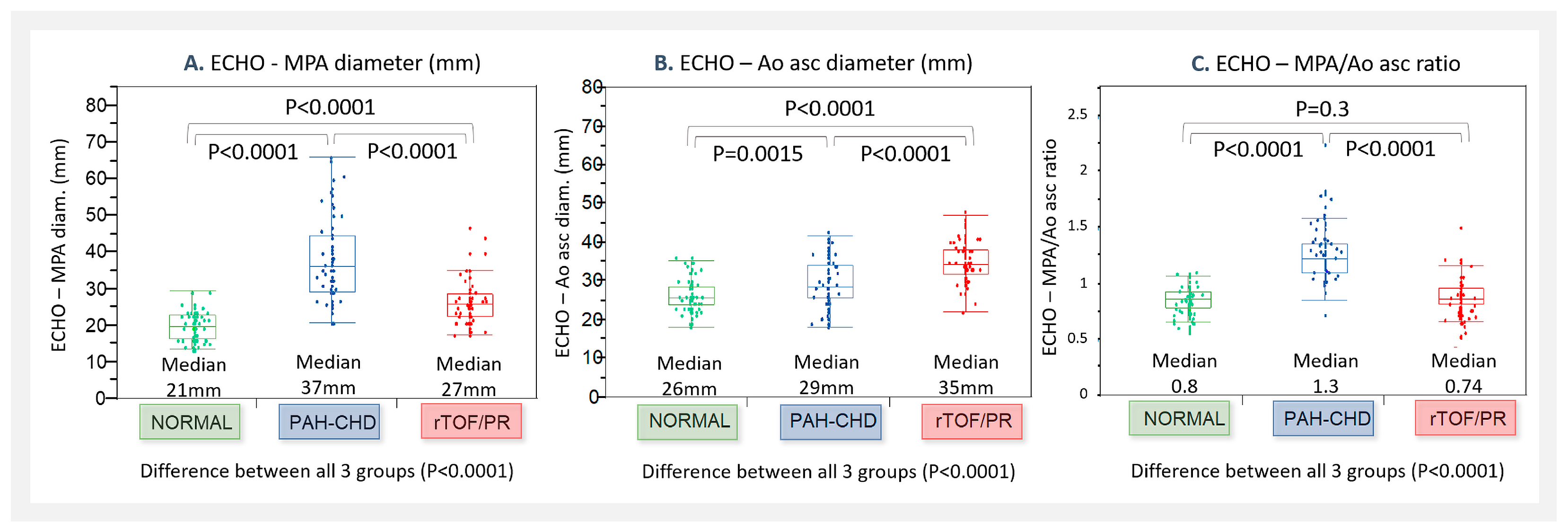
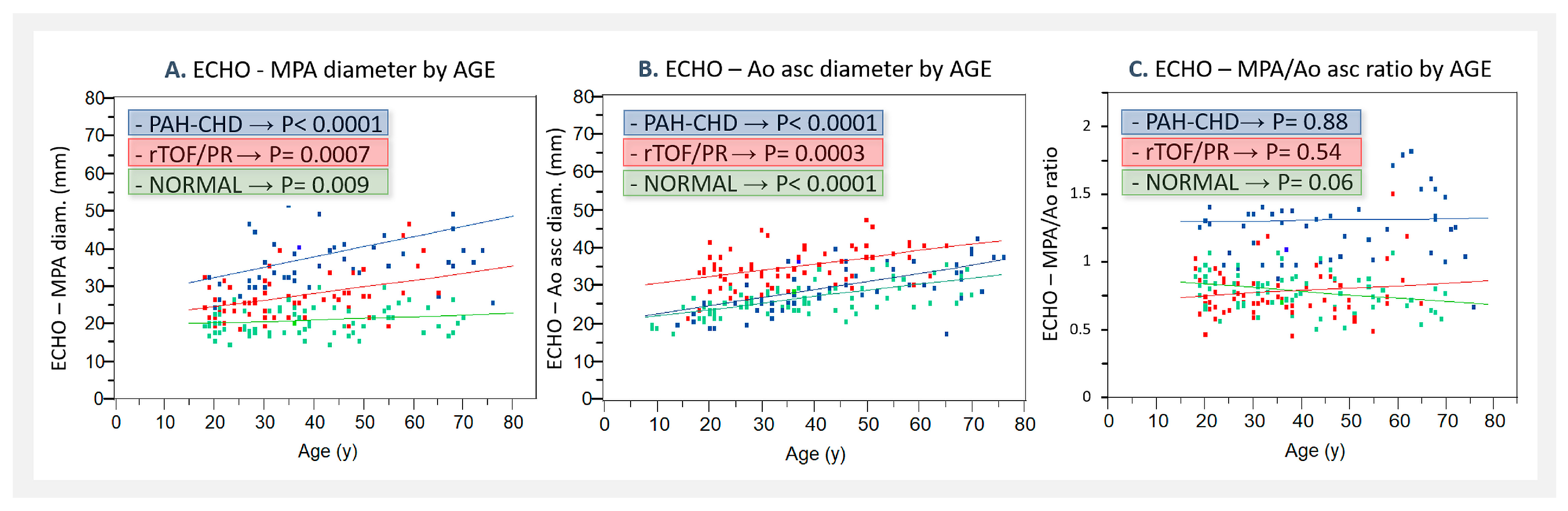
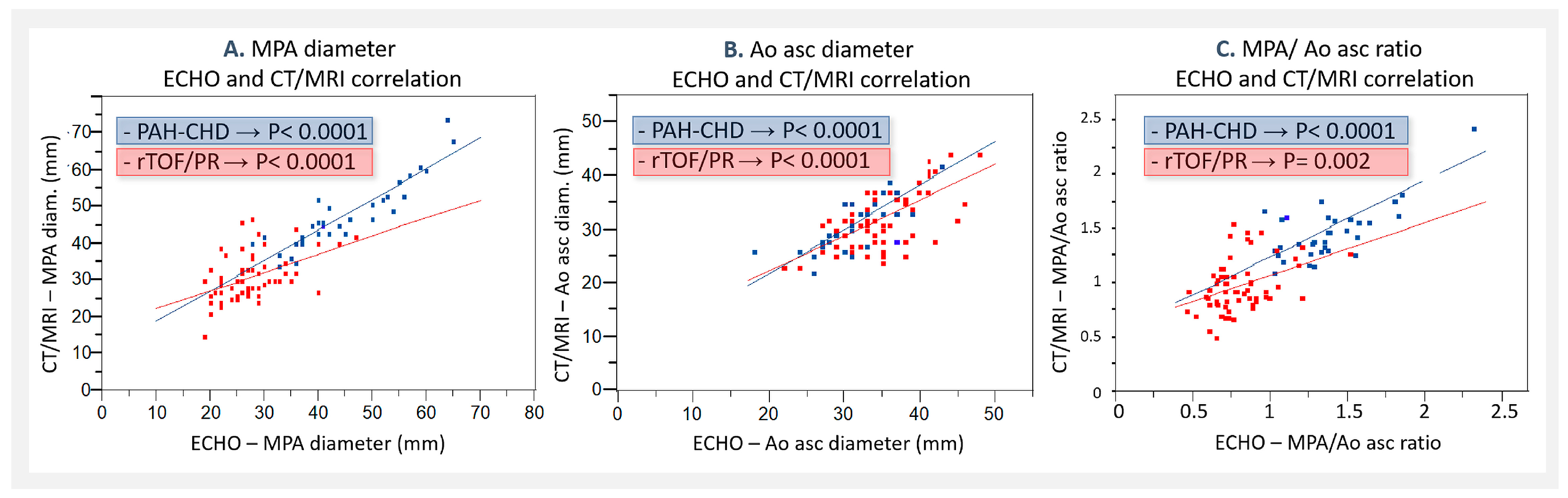
- The MPA/Ao asc diameter ratio was significantly greater in PAH-CHD (0.68–2.3, median 1.3), but not in rTOF/PR (0.46–1.52, median 0.74), compared to NORMAL (0.52–1.09, median 0.8)—Figure 2C. MPA/Ao asc ratio did not show statistically significant changes with age in all 3 patients’ groups, as shown in Figure 3C.
4.2. CT/MRI Measurements
4.3. ECHO and CT/MRI Measurement Comparison
4.4. MPA Dilatation—Severity
4.5. MPA/Ao Asc Ratio
5. Discussion
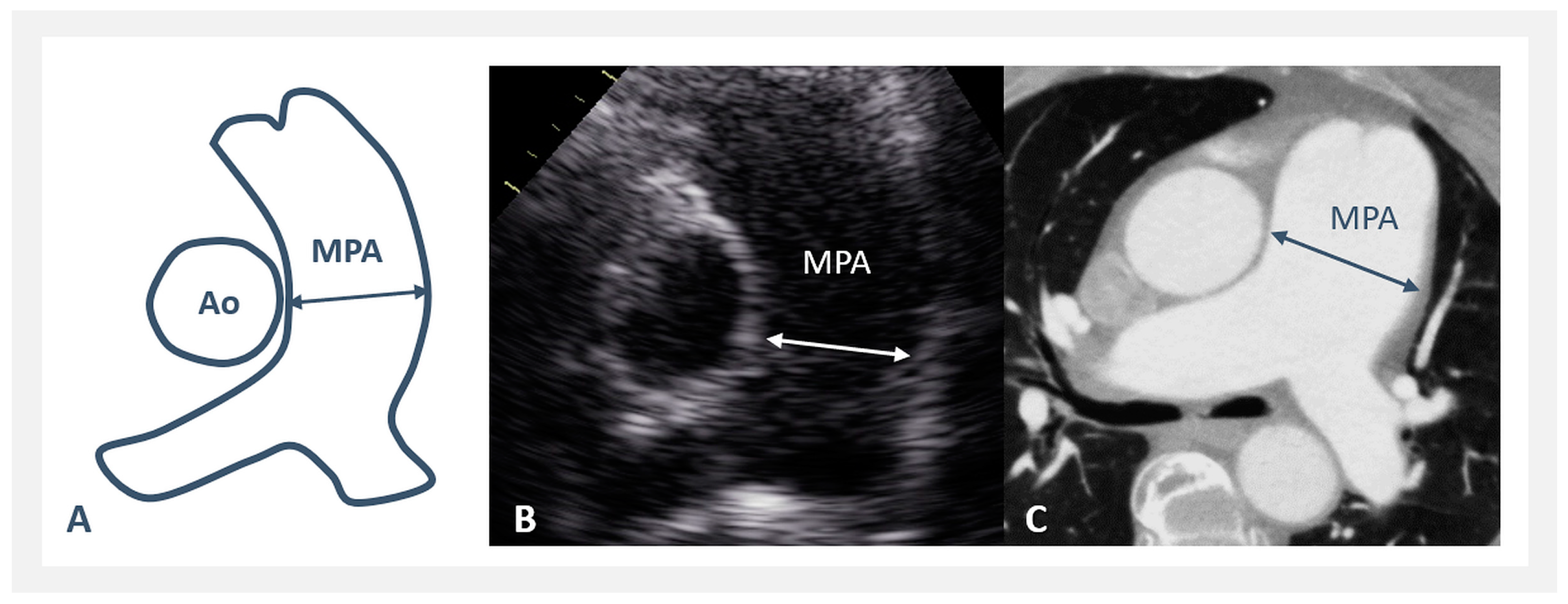
- What is a normal-sized MPA, and what is the optimal tool for MPA measurement?
- What are the factors influencing the normal MPA size?
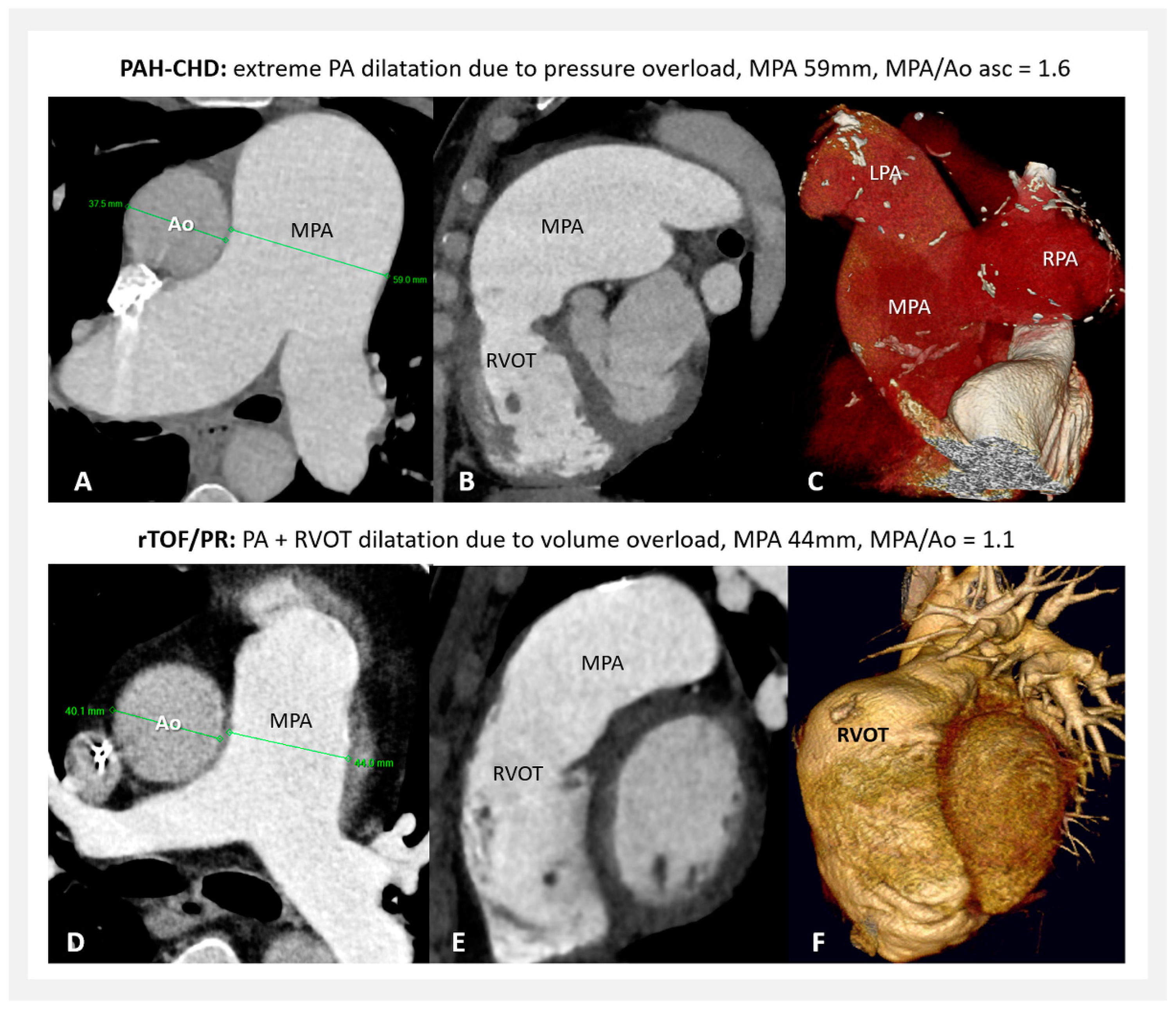
- MPA dilatation—what are the differences due to pressure overload (PAH-CHD) and volume overload (rTOF/PR)?
- MPA/Ao asc ratio—how relevant is it and when to use it?
- What degree of MPA dilatation may be considered high-risk for the development of severe complications?
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Truong, Q.A.; Massaro, J.M.; Rogers, I.S.; Mahabadi, A.A.; Kriegel, M.F.; Fox, C.S.; O′Donnell, C.J.; Hoffmann, U. Reference values for normal pulmonary artery dimensions by noncontrast cardiac computed tomography: The Framingham Heart Study. Circ. Cardiovasc. Imaging 2012, 5, 147–154. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.; Brida, M.; Carlsen, J.; Coats, A.J.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Weerakkody, Y.; Hacking, C.; Worsley, C.; Luong, D.; Botz, B.; Murphy, A. Pulmonary Trunk Dilatation. Reference Article. Available online: https://radiopaedia.org/articles/pulmonary-trunk-dilatation?lang=us (accessed on 22 January 2024).
- Raymond, T.E.; Khabbaza, J.E.; Yadav, R.; Tonelli, A.R. Significance of Main Pulmonary Artery Dilation on Imaging Studies. Ann. Am. Thorac. Soc. 2015, 11, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Raju, S.N.; Pandey, N.N.; Sharma, A.; Malhi, A.S.; Deepti, S.; Kumar, S. Pulmonary Arterial Dilatation: Imaging Evaluation Using Multidetector Computed Tomography. Indian J. Radiol. Imaging 2021, 31, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Daliento, L.; Somerville, J.; Presbitero, P.; Menti, L.; Brach-Prever, S.; Rizzoli, G.; Stone, S. Eisenmenger syndrome: Factors relating to deterioration and death. Eur. Heart J. 1998, 19, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Badagliacca, R.; Poscia, R.; Pezzuto, B.; Papa, S.; Nona, A.; Mancone, M.; Mezzapesa, M.; Nocioni, M.; Sciomer, S.; Valli, G.; et al. Pulmonary Arterial Dilatation in Pulmonary Hypertension: Prevalence and Prognostic Relevance. Cardiology 2012, 121, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Demerouti, E.A.; Manginas, A.N.; Athanassopoulos, G.D.; Karatasakis, G.T. Complications Leading to Sudden Cardiac Death in Pulmonary Arterial Hypertension. Respir. Care 2013, 58, 1246–1254. [Google Scholar] [CrossRef]
- Fernanado, D.M.G.; Thilakarathne, S.M.N.K.; Wickramasinghe, C.U. Pulmonary artery dissection—A review of 150 cases. Heart Lung 2019, 48, 428–435. [Google Scholar] [CrossRef]
- Akbal, O.Y.; Kaymaz, C.; Tanboga, I.H.; Hakgor, A.; Yilmaz, F.; Turkday, S.; Dogan, C.; Tanyeri, S.; Demir, D.; Bayram, Z.; et al. Extrinsic compression of left main coronary artery by aneurysmal pulmonary artery in severe pulmonary hypertension: Its correlates, clinical impact, and management strategies. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1302–1308. [Google Scholar] [CrossRef]
- Kaldarárová, M.; Šimková, I.; Valkovičová, T.; Remková, A.; Neuschl, V. Pulmonary thromboembolism in congenital heart defects with severe pulmonary arterial hypertension. Cor Vasa 2013, 55, E170–E175. [Google Scholar] [CrossRef]
- Klauco, F.; Kaldararova, M.; Valkovicova, T.; Bobocka, K.; Simkova, I. Rare complication in common condition: Dissection of dilated pulmonary artery. Lek. Obz. 2023, 72, 113–117. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Augustine, D.X.; Coates-Bradshaw, L.D.; Willis, J.; Harkness, A.; Ring, L.; Grapsa, J.; Coghlan, G.; Kaye, N.; Oxborough, D.; Robinson, S.; et al. Echocardiographic assessment of pulmonary hypertension: A guideline protocol from the British Society of Echocardiography. Echo Res. Pract. 2018, 5, G11–G24. [Google Scholar] [CrossRef]
- Edwards, P.D.; Bull, R.K.; Coulden, R. CT measurement of main pulmonary artery diameter. Br. J. Radiol. 1998, 71, 1018–1020. [Google Scholar] [CrossRef]
- Karazincir, S.; Balci, A.; Seyfeli, E.; Akoğlu, S.; Babayiğit, C.; Akgül, F.; Yalçin, F.; Eğilmez, E. CT assessment of main pulmonary artery diameter. Diagn. Interv. Radiol. 2008, 14, 72–74. [Google Scholar] [PubMed]
- Remy-Jardin, M.; Ryerson, C.J.; Schiebler, M.L.; Leung, A.N.; Wild, J.M.; Hoeper, M.M.; Alderson, P.O.; Goodman, L.R.; Mayo, J.; Haramati, L.B.; et al. Imaging of pulmonary hypertension in adults: A position paper from the Fleischner Society. Eur. Respir. J. 2021, 57, 2004455. [Google Scholar] [CrossRef]
- Bozlar, U.; Ors, F.; Deniz, O.; Uzun, M.; Gumus, S.; Ugurel, M.S.; Yazar, F.; Tayfun, C. Pulmonary artery diameters measured by multidetector-row computed tomography in healthy adults. Acta Radiol. 2007, 48, 1086–1091. [Google Scholar] [CrossRef] [PubMed]
- Kreibich, M.; Siepe, M.; Kroll, J.; Höhn, R.; Grohmann, J.; Beyersdorf, F. Aneurysms of the pulmonary artery. Circulation 2015, 131, 310–316. [Google Scholar] [CrossRef]
- Sheikhzadeh, S.; De Backer, J.; Gorgan, N.R.; Rybczynski, M.; Hillebrand, M.; Schüler, H.; Bernhardt, A.M.; Koschyk, D.; Bannas, P.; Keyser, B.; et al. The main pulmonary artery in adults: A controlled multicenter study with assessment of echocardiographic reference values, and the frequency of dilatation and aneurysm in Marfan syndrome. Orphanet J. Rare Dis. 2014, 9, 203–212. [Google Scholar] [CrossRef]
- Kauhanen, S.P.; Liimatainen, T.; Korhonen, M.; Parkkonen, J.; Vienonen, J.; Vanninen, R.; Hedman, M. Pulmonary Artery Dilatation Is a Common Finding in a Coronary Artery CT Angiography Population. In Vivo 2021, 35, 2177–2185. [Google Scholar] [CrossRef]
- Berger, T.; Siepe, M.; Simon, B.; Beyersdorf, F.; Chen, Z.; Kondov, S.; Schlett, C.L.; Bamberg, F.; Tarkhnishvili, A.; Chikvatia, S.; et al. Pulmonary artery diameter: Means and normal limits—Assessment by computed tomography angiography. Interact. Cardiovasc. Thorac. Surg. 2022, 34, 637–644. [Google Scholar] [CrossRef]
- Goerne, H.; Batra, K.; Rajjah, P. Imaging of pulmonary hypertension: An update. Cardiovasc. Diagn. Ther. 2018, 8, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Ran, H.; Pistritto, A.M.; Gerges, C.; Heidari, H.; Nitsche, C.; Gerges, M.; Hengstenberg, C.; Mascherbauer, J.; Binder, T.; et al. Pulmonary artery to ascending aorta ratio by echocardiography: A strong predictor for presence and severity of pulmonary hypertension. PLoS ONE 2020, 15, e0235716. [Google Scholar] [CrossRef] [PubMed]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults with Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e81–e192. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. The ESC clinical practice guidelines for the management of adult congenital Heart Disease 2020. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef] [PubMed]
- Ussavarungsi, K.; Whitlock, J.P.; Lundy, T.A.; Carabenciov, I.D.; Burger, C.D.; Lee, A.S. The Significance of Pulmonary Artery Size in Pulmonary Hypertension. Diseases 2014, 2, 243–259. [Google Scholar] [CrossRef]
- Xi, Q.; Liu, Z.; Xiong, C.; Luo, Q.; Zhao, Z.; Zhao, Q.; Yang, T.; Zeng, Q.; Li, P.; Qiu, L. Pulmonary artery dilatation in different causes of pulmonary hypertension. Pulm. Circ. 2023, 13, e12313. [Google Scholar] [CrossRef]
- Gallego, P.; Rodríguez-Puras, M.J.; Gotarredona, P.S.; Valverde, I.; Manso, B.; González-Calle, A.; Adsuar, A.; Cubero, J.M.; de la Llera, L.D.; Ordoñez, A.; et al. Prevalence and prognostic significance of pulmonary artery aneurysms in adults with congenital heart disease. Int. J. Cardiol. 2018, 270, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Kaldararova, M.; Simkova, I.; Pacak, J.; Tiitel, P.; Masura, J. Pulmonary artery dilatation in Eisenmenger syndrome, when and why? Eur. J. Echocardiogr. 2011, 12 (Suppl. S2), ii176–ii177. [Google Scholar]
- Hlavata, T.; Kaldararova, M.; Klauco, F.; Drangova, E.; Reptova, A.; Simkova, I. Congenital Absence of the Portal Vein as a Rare Cause of Portopulmonary Hypertension—A Case Study Series. Medicina 2022, 58, 1484. [Google Scholar] [CrossRef]
- Duijnhouwer, A.L.; Lemmers, J.; Smit, J.; van Haren-Willems, J.; Knaapen-Hans, H.; Cate, T.T.; Have, W.H.O.T.; de Boer, M.-J.; Roos-Hesselink, J.; Vonk, M.; et al. The outcome of pulmonary hypertension and its association with pulmonary artery dilatation. Neth. Heart J. 2020, 28, 645–655. [Google Scholar] [CrossRef]
- Hu, L.; Ouyang, R.; Sun, A.; Wang, Q.; Guo, C.; Peng, Y.; Qin, Y.; Zhang, Y.; Xiang, Y.; Zhong, Y. Pulmonary artery hemodynamic assessment of blood flow characteristics in repaired tetralogy of Fallot patients versus healthy child volunteers. Quant. Imaging Med. Surg. 2020, 10, 921–933. [Google Scholar] [CrossRef]
- Kaldararova, M.; Klauco, F.; Martanovicova, K.; Valkovicova, T.; Bobocka, K.; Drangova, E.; Simkova, I. Progressive pulmonary artery dilatation–important but frequently ignored parameter. Lek. Obz. 2023, 72, 106–112. [Google Scholar]
- Geva, T. Repaired tetralogy of Fallot: The roles of cardiovascular magnetic resonance in evaluating pathophysiology and for pulmonary valve replacement decision support. J. Cardiovasc. Magn. Reson. 2011, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Senthilnathan, S.; Dragulescu, A.; Mertens, L. Pulmonary Regurgitation after Tetralogy of Fallot Repair: A Diagnostic and Therapeutic Challenge. J. Cardiovasc. Echogr. 2013, 23, 1–9. [Google Scholar] [PubMed]
- Siripornpitak, S.; Lueangwattanapong, D.; Sriprachyakul, A.; Wanitkun, S.; Limsuwan, A. Branch Pulmonary Artery Regurgitation in Repaired Tetralogy of Fallot: Correlation with Pulmonary Artery Morphology, Distensibility, and Right Ventricular Function. Tomography 2021, 7, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Caro-Domínguez, P.; Compton, G.; Humpl, T.; Manson, D. Pulmonary Arterial Hypertension in Children: Diagnosis Using Ratio of Main Pulmonary Artery to Ascending Aorta Diameter as Determined by Multi-Detector Computed Tomography. Pediatr. Radiol. 2016, 46, 1378–1383. [Google Scholar] [CrossRef]
- Baldi, B.G.; Fernandes, C.J.C.d.S.; Heiden, G.I.; Freitas, C.S.G.; Sobral, J.B.; Kairalla, R.A.; Carvalho, C.R.R.; Souza, R. Association Between Pulmonary Artery to Aorta Diameter. Medicine 2021, 100, e26483. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Agrawal, A.; Iakovou, A.; Cohen, S.; Shah, R.; Talwar, A. Pulmonary artery aneurysm: A review. Pulm. Circ. 2020, 10, 2045894020908780. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.H.; Lamers, W.H.; Hikspoors, J.P.J.M.; Mohun, T.J.; Bamforth, S.D.; Chaudhry, B.; Eley, L.; Kerwin, J.; Crosier, M.; Henderson, D.J. Development of the arterial roots and ventricular outflow tracts. J. Anat. 2024, 244, 497–513. [Google Scholar] [CrossRef]
- Kutty, S.; Kuehne, T.; Gribben, P.; Reed, E.; Li, L.; Danford, D.A.; Beerbaum, P.B.; Sarikouch, S. Ascending Aortic and Main Pulmonary Artery Areas Derived From Cardiovascular Magnetic Resonance as Reference Values for Normal Subjects and Repaired Tetralogy of Fallot. Circ. Cardiovasc. Imaging 2012, 5, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.Y.; Geisinger, M.T.; Bhamare, T.; Wasserman, M.; Min, J.; Goldmuntz, E. Natural history of the aortic root in Tetralogy of Fallot after repair. Int. J. Cardiol. Congenit. Heart Dis. 2021, 3, 100092. [Google Scholar] [CrossRef]
- Sengupta, A.; Lee, J.M.; Gauvreau, K.; Colan, S.D.; del Nido, P.J.; Mayer, J.E.; Nathan, M. Natural history of aortic root dilatation and pathologic aortic regurgitation in tetralogy of Fallot and its morphological variants. J. Thorac. Cardiovasc. Surg. 2023, 166, 1718–1728. [Google Scholar] [CrossRef]
- Egbe, A.C.; Miranda, W.R.; Jain, C.C.; Anderson, J.H.; Stephens, E.H.; Andi, K.; Goda, A.; Abozied, O.; Ramachandran, D.; Crestanello, J.A.; et al. Risk of pulmonary artery dissection in adults with congenital heart disease. Int. J. Cardiol. 2023, 370, P186–P190. [Google Scholar] [CrossRef]
- Florczyk, M.; Wieteska, M.; Kurzyna, M.; Gościniak, P.; Pepke-Żaba, J.; Biederman, A.; Torbicki, A. Acute and chronic dissection of pulmonary artery: New challenges in pulmonary arterial hypertension? Pulm. Circ. 2018, 8, 2045893217749114. [Google Scholar] [CrossRef]
- Cool, C.J.; Fathini, F.; Adams, I.; Saboe, A.; Kusumawardhani, N.Y.; Astuti, A.; Yahya, A.F. Eisenmenger syndrome with left main compression syndrome: A case report. BMC Cardiovasc. Disord. 2022, 22, 89–99. [Google Scholar] [CrossRef]
- Duijnhouwer, A.L.; Navarese, E.P.; Van Dijk, A.P.; Loeys, B.; Roos-Hesselink, J.W.; De Boer, M.J. Aneurysm of the pulmonary artery, a systematic review and critical analysis of current literature. Congenit. Heart Dis. 2016, 11, 102–109. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | NORMAL (N = 80) | PAH-CHD (N = 60) | rTOF/PR (N = 64) |
|---|---|---|---|
| Gender: Male/Female | 31/50 | 15/45 | 27/36 |
| Age (years): median (min.–max.) | 34 (18–70) | 37.5 (18–76) | 32.5 (19–65) |
| Height (cm): median (min.–max.) | 172 (132–193) | 158.5 (139–195) | 170.5 (150–195) |
| Weight (kg): median (min.–max.) | 68 (32–101) | 57 (38–120) | 74 (40–108) |
| BSA (Dubois, m2): median (min.–max.) | 1.81 (1.1–2.29) | 1.57 (1.2–2.4) | 1.82 (1.3–2.34) |
| PAH–CHD: Defect Type | N = 60 | % |
|---|---|---|
| Unoperated defects/or with significant residual shunts | 47 | 78.3 |
| 1. Pre-tricuspid shunt: | 13 | 21.7 |
| 8 | 13.3 |
| 5 | 8.3 |
| 2. Post-tricuspid shunt: | 34 | 56.7 |
| 15 | 25 |
| 9 | 15 |
| 5 | 8.3 |
| 5 | 8.3 |
| After closure, without/or insignificant residual shunt | 10 | 16.7 |
| Other (congenital portopulmonary hypertension) | 3 | 5 |
| Associated Down’s syndrome | 15 | 25 |
| rTOF/PR: Patients’ Characteristics | N = 64 |
|---|---|
| Complete TOF repair—age (years): median (min.–max.) | 5 (0.25–21) |
| 51 (79.7) |
| 13 (20.3) |
| Previous shunt palliation: No. of patients (%) | 9 (14.1) |
| 5 (7.8) |
| 1 (1.6) |
| 3 (4.7) |
| Follow-up after complete repair (years): median (min.–max.) | 22 (17–53) |
| Overall | PAH-CHD | rTOF/PR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Analyzed Parameter | ECHO Median | CT/MRI Median | p-Value | ECHO Median | CT/MRI Median | p-Value | ECHO Median | CT/MRI Median | p-Value |
| MPA (mm) | 26 | 33 | <0.0001 | 37 | 46 | <0.0001 | 27 | 32 | <0.0001 |
| Ao asc (mm) | 30 | 33 | 0.01 | 29 | 31.5 | 0.01 | 32 | 35 | 0.002 |
| MPA/Ao asc ratio | 0.86 | 1.12 | <0.0001 | 1.3 | 1.5 | 0.002 | 0.74 | 0.94 | <0.0001 |
| ECHO | C T/MRI | |||||
|---|---|---|---|---|---|---|
| Severity of MPA Dilatation /% of Patients | PAH-CHD | rTOF/PR | p-Value | PAH-CHD | rTOF/PR | p-Value |
| 13.3% | 56.3% | <0.0001 | 0 | 31.3% | <0.0001 |
| 51.7% | 40.6% | 22.9% | 60.9% | ||
| 35% | 3.1% | 76.9% | 7.8% | ||
| 16.7% | 0 | 31.4% | 0 | ||
| MPA Dilatation | MPA/Ao asc > 1 | MPA/Ao asc > 1.5 | ||||
|---|---|---|---|---|---|---|
| Examination Technique /% of Patients | PAH-CHD | rTOF/PR | p-Value | PAH-CHD | rTOF/PR | p-Value |
| 88.1% | 10.9% | <0.0001 | 25.4% | 1.5% | <0.0001 |
| 100% | 34.5% | 45.7% | 1.6% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaldararova, M.; Bobocka, K.; Kantorova, A.; Drangova, E.; Polakova Mistinova, J.; Klauco, F.; Hlavata, T.; Reptova, A.; Valkovicova, T.; Simkova, I. Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease. J. Clin. Med. 2024, 13, 1567. https://doi.org/10.3390/jcm13061567
Kaldararova M, Bobocka K, Kantorova A, Drangova E, Polakova Mistinova J, Klauco F, Hlavata T, Reptova A, Valkovicova T, Simkova I. Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease. Journal of Clinical Medicine. 2024; 13(6):1567. https://doi.org/10.3390/jcm13061567
Chicago/Turabian StyleKaldararova, Monika, Katarina Bobocka, Andrea Kantorova, Erika Drangova, Jana Polakova Mistinova, Filip Klauco, Tereza Hlavata, Adriana Reptova, Tatiana Valkovicova, and Iveta Simkova. 2024. "Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease" Journal of Clinical Medicine 13, no. 6: 1567. https://doi.org/10.3390/jcm13061567
APA StyleKaldararova, M., Bobocka, K., Kantorova, A., Drangova, E., Polakova Mistinova, J., Klauco, F., Hlavata, T., Reptova, A., Valkovicova, T., & Simkova, I. (2024). Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease. Journal of Clinical Medicine, 13(6), 1567. https://doi.org/10.3390/jcm13061567