
Portal Vein Thrombosis: State-of-the-Art Review

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Literature Search Strategy
3. Classification of Portal Vein Thrombosis
4. Risk Factors for Portal Vein Thrombosis
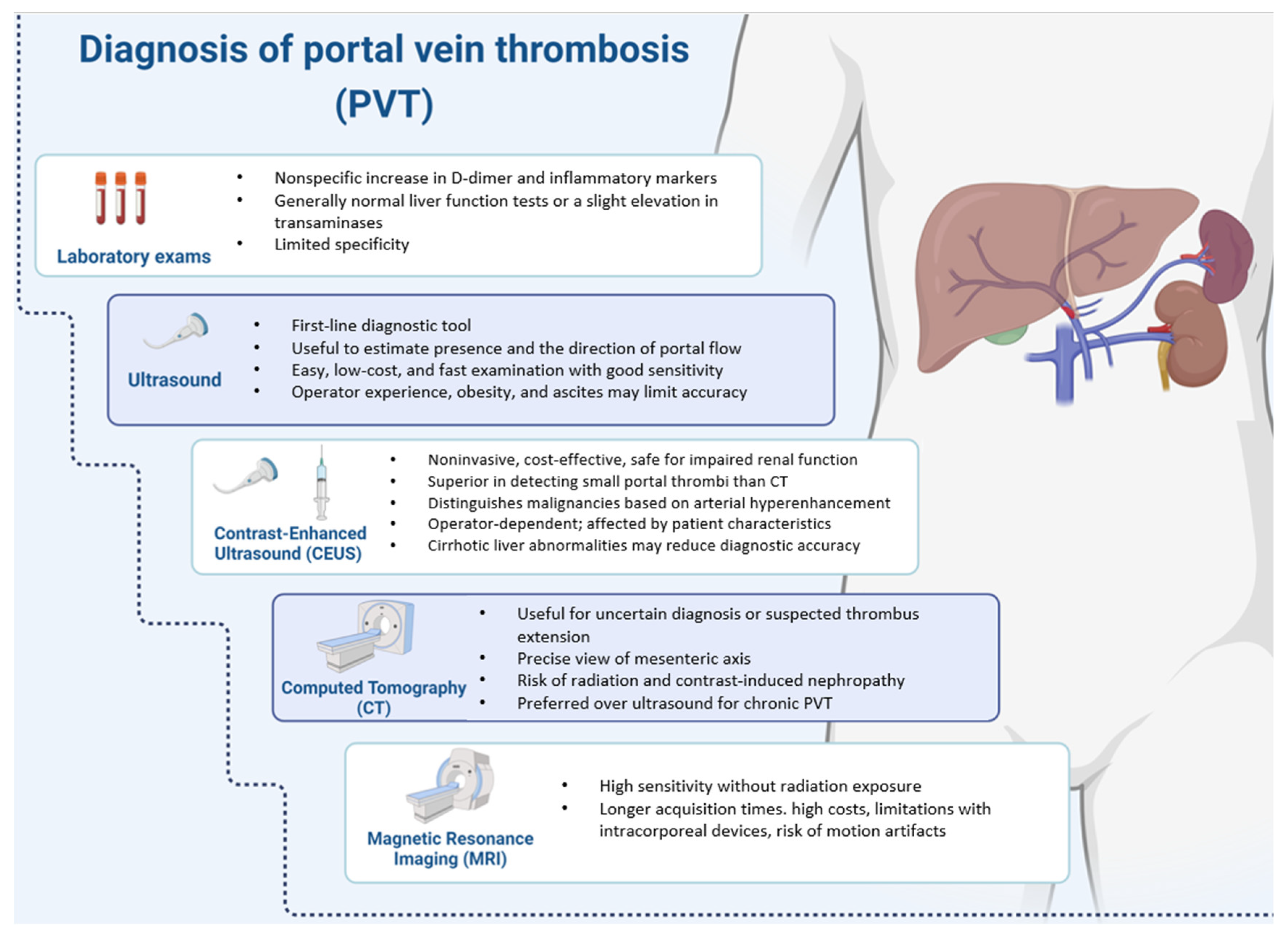
5. Diagnosis
5.1. Laboratory
5.2. Imaging
6. Differential Diagnosis
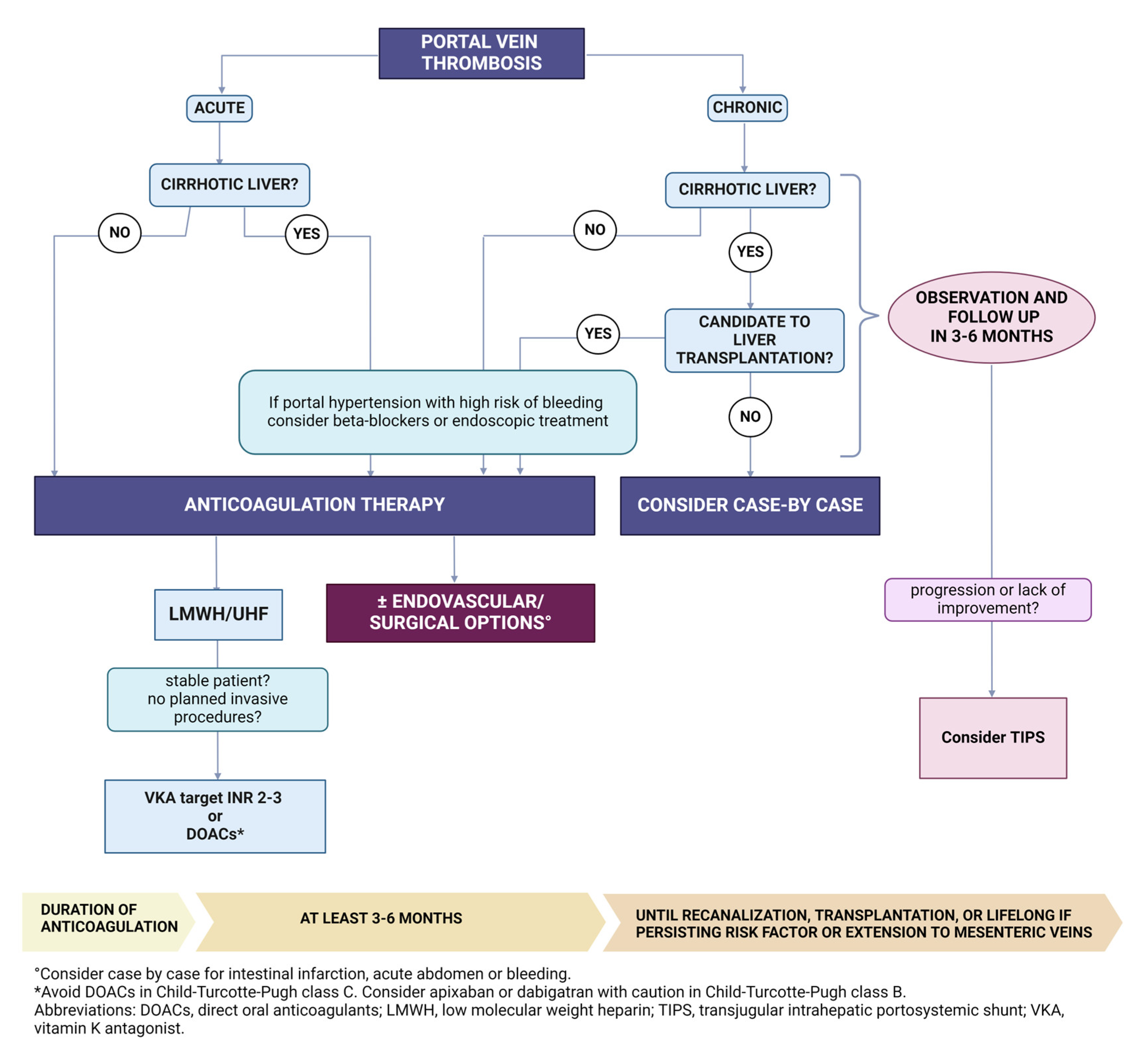
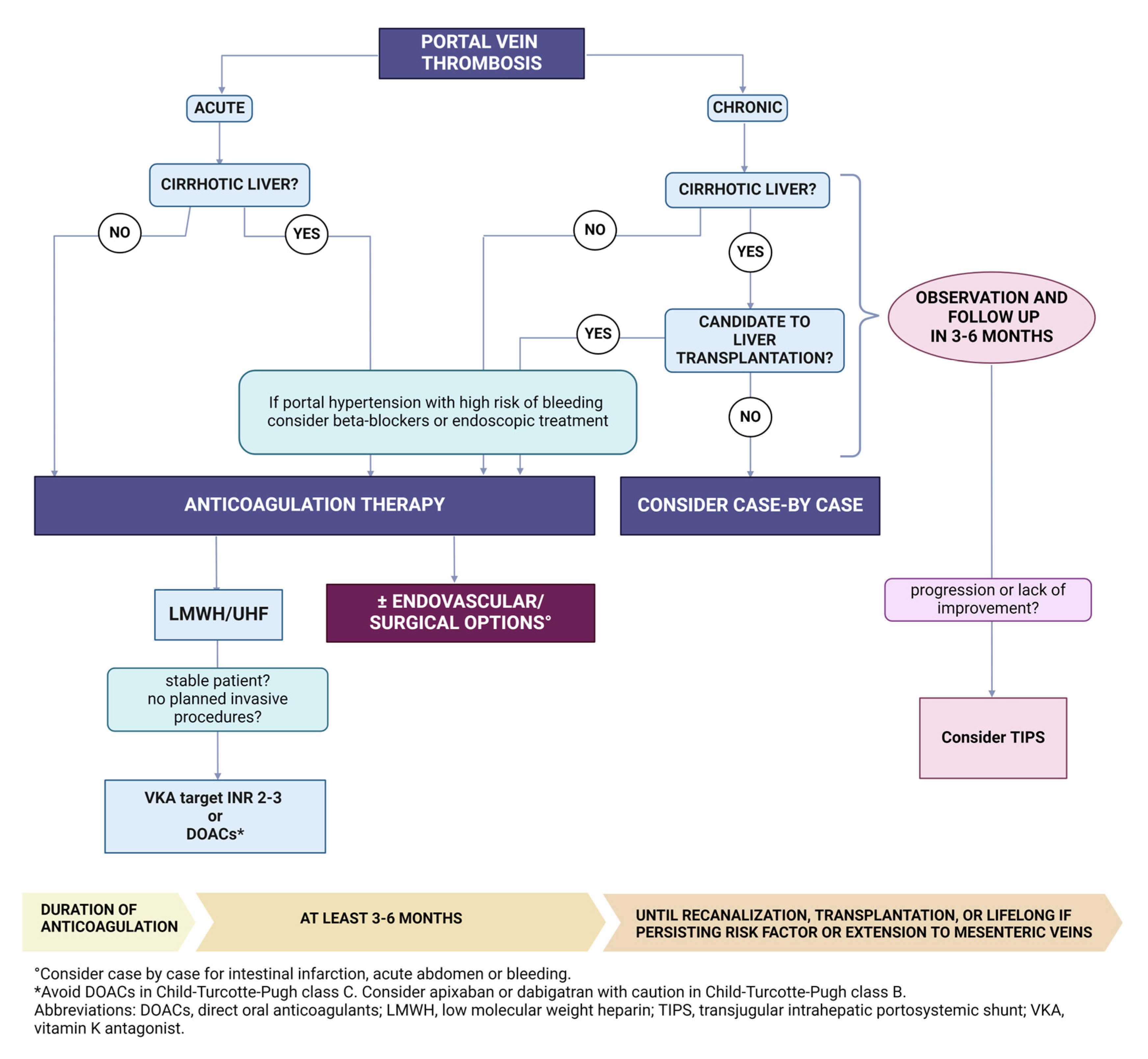
7. PVT Therapy
7.1. Anticoagulant Treatment
7.2. Cirrhotic Patients
7.3. Anticoagulation Duration
7.4. Other Therapeutic Strategies
7.5. Treatment of PVT Complications
8. PVT Prophylaxis
9. Liver Transplant & PVT
10. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Riva, N.; Ageno, W. How to manage splanchnic vein thrombosis in patients with liver disease. Hematology Am. Soc. Hematol. Educ. Program. 2023, 2023, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Monaco, G.; Bucherini, L.; Stefanini, B.; Piscaglia, F.; Foschi, F.G.; Ielasi, L. Direct oral anticoagulants for the treatment of splanchnic vein thrombosis: A state of art. World J. Gastroenterol. 2023, 29, 4962–4974. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Dentali, F.; Pomero, F.; Fenoglio, L.; Squizzato, A.; Pagani, G.; Re, R.; Bonzini, M. Incidence rates and case fatality rates of portal vein thrombosis and Budd-Chiari Syndrome. Thromb. Haemost. 2017, 117, 794–800. [Google Scholar] [PubMed]
- Søgaard, K.K.; Adelborg, K.; Darvalics, B.; Horváth-Puhó, E.; Beyer-Westendorf, J.; Ageno, W.; Sørensen, H.T. Risk of bleeding and arterial cardiovascular events in patients with splanchnic vein thrombosis in Denmark: A population-based cohort study. Lancet Haematol. 2018, 5, e441–e449. [Google Scholar] [PubMed]
- Valla, D.C.; Condat, B.; Lebrec, D. Spectrum of portal vein thrombosis in the West. J. Gastroenterol. Hepatol. 2002, 17 (Suppl. S3), S224–S227. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Sollano, J.D.; Chawla, Y.K.; Amarapurkar, D.; Hamid, S.; Hashizume, M.; Jafri, W.; Kumar, A.; Kudo, M.; A Lesmana, L.; et al. Consensus on extra-hepatic portal vein obstruction. Liver Int. 2006, 26, 512–519. [Google Scholar] [CrossRef]
- Amitrano, L.; Guardascione, M.A.; Brancaccio, V.; Margaglione, M.; Manguso, F.; Iannaccone, L.; Grandonet, E.; Balzano, A.L. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J. Hepatol. 2004, 40, 736–741. [Google Scholar] [CrossRef]
- Orloff, M.J.; Orloff, M.S.; Orloff, S.L.; Girard, B. Portal vein thrombosis in cirrhosis with variceal hemorrhage. J. Gastrointest. Surg. 1997, 1, 123–130. [Google Scholar] [CrossRef]
- Pan, J.; Wang, L.; Gao, F.; An, Y.; Yin, Y.; Guo, X.; Netry, F.G.; Yoshidal, E.M.; Qi, X. Epidemiology of portal vein thrombosis in liver cirrhosis: A systematic review and meta-analysis. Eur. J. Intern. Med. 2022, 104, 21–32. [Google Scholar] [CrossRef]
- Fimognari, F.L.; Violi, F. Portal vein thrombosis in liver cirrhosis. Intern. Emerg. Med. 2008, 3, 213–218. [Google Scholar] [CrossRef]
- Okuda, K.; Ohnishi, K.; Kimura, K.; Matsutani, S.; Sumida, M.; Goto, N.; Musha, H.; Takashi, M.; Suzuki, N.; Shinagawa, T.; et al. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985, 89, 279–286. [Google Scholar] [CrossRef]
- Francoz, C.; Belghiti, J.; Vilgrain, V.; Sommacale, D.; Paradis, V.; Condat, B.; Denninger, M.H.; Sauvanet, A.; Valla, D.; Durand, F. Splanchnic vein thrombosis in candidates for liver transplantation: Usefulness of screening and anticoagulation. Gut 2005, 54, 691–697. [Google Scholar] [CrossRef]
- Turatti, G.; Fedeli, U.; Valerio, L.; Klok, F.A.; Cohen, A.T.; Hunt, B.J.; Simioni, P.; Middeldorp, S.; Ageno, W.; Kucher, N.; et al. Splanchnic vein thrombosis-related mortality in the Veneto region (Italy), 2008–2019: Retrospective analysis of epidemiological data. Thromb. Res. 2022, 209, 41–46. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Caldwell, S.H.; Tripodi, A. Diagnosis, Development, and Treatment of Portal Vein Thrombosis in Patients with and Without Cirrhosis. Gastroenterology 2019, 156, 1582–1599.e1. [Google Scholar] [CrossRef]
- Valeriani, E.; Menichelli, D.; Palumbo, I.M.; Cammisotto, V.; Pastori, D.; Pignatelli, P. How to treat patients with splanchnic vein thrombosis: Recent advances. Pol. Arch. Intern. Med. 2023, 133, 16499. [Google Scholar] [CrossRef]
- Senzolo, M.; Garcia-Tsao, G.; García-Pagán, J.C. Current knowledge and management of portal vein thrombosis in cirrhosis. J. Hepatol. 2021, 75, 442–453. [Google Scholar] [CrossRef]
- Valeriani, E.; Riva, N.; Di Nisio, M.; Ageno, W. Splanchnic Vein Thrombosis: Current Perspectives. Vasc. Health Risk. Manag. 2019, 15, 449–461. [Google Scholar] [CrossRef]
- Kumar, M.; Saraswat, V.A. Natural history of portal cavernoma cholangiopathy. J. Clin. Exp. Hepatol. 2014, 4 (Suppl. S1), S62–S66. [Google Scholar] [CrossRef] [PubMed]
- Sogaard, K.K.; Astrup, L.B.; Vilstrup, H.; Gronbaek, H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol. 2007, 7, 34. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Sharma, P.; Arora, A. Review article: Portal vein obstruction--epidemiology, pathogenesis, natural history, prognosis and treatment. Aliment. Pharmacol. Ther. 2015, 41, 276–292. [Google Scholar] [CrossRef] [PubMed]
- Plessier, A.; Darwish-Murad, S.; Hernandez-Guerra, M.; Consigny, Y.; Fabris, F.; Trebicka, J.; Heller, J.; Morard, I.; Lasser, L.; Langlet, P.; et al. Acute portal vein thrombosis unrelated to cirrhosis: A prospective multicenter follow-up study. Hepatology 2010, 51, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Valla, D.; Casadevall, N.; Huisse, M.G.; Tulliez, M.; Grange, J.D.; Muller, O.; Binda, T.; Varet, B.; Rueff, B.; Benhamou, J.P. Etiology of portal vein thrombosis in adults. A prospective evaluation of primary myeloproliferative disorders. Gastroenterology 1988, 94, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; De Stefano, V.; Wang, J.; Bai, M.; Yang, Z.; Han, G.; Fan, D. Prevalence of inherited antithrombin, protein C, and protein S deficiencies in portal vein system thrombosis and Budd-Chiari syndrome: A systematic review and meta-analysis of observational studies. J. Gastroenterol. Hepatol. 2013, 28, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Ren, W.; De Stefano, V.; Fan, D. Associations of coagulation factor V Leiden and prothrombin G20210A mutations with Budd-Chiari syndrome and portal vein thrombosis: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 1801–1812.e7. [Google Scholar] [CrossRef]
- Giri, S.; Angadi, S.; Varghese, J.; Sundaram, S.; Bhrugumalla, S. Prothrombotic states in portal vein thrombosis and Budd-Chiari syndrome in India: A systematic review and meta-analysis. Indian J. Gastroenterol. 2023, 42, 629–641. [Google Scholar] [CrossRef]
- Ding, J.; Zhao, F.; Cui, J.; Zhu, M.; Zhao, W. Platelet activation is upregulated in cirrhotic patients with portal vein thrombosis. Thromb. Haemost. 2023; ahead of print. [Google Scholar] [PubMed]
- Zanetto, A.; Campello, E.; Senzolo, M.; Simioni, P. The evolving knowledge on primary hemostasis in patients with cirrhosis: A comprehensive review. Hepatology 2024, 79, 460–481. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Burra, P.; Senzolo, M.; Simioni, P. Increased platelet ratio in patients with decompensated cirrhosis indicates a higher risk of portal vein thrombosis. Liver Int. 2023, 43, 155–159. [Google Scholar] [CrossRef]
- Campello, E.; Spiezia, L.; Gavasso, S.; Bizzaro, D.; Cardin, R.; D’Amico, F.; Gringeri, E.; Cillo, U.; Barbiero, G.; Battistel, M.; et al. Endothelial Damage of the Portal Vein is Associated with Heparin-Like Effect in Advanced Stages of Cirrhosis. Thromb. Haemost. 2020, 120, 1173–1181. [Google Scholar]
- Stupia, R.; Lombardi, R.; Cattazzo, F.; Zoncapè, M.; Mantovani, A.; De Marco, L.; Mantovani, A.; Fracanzani, A.L.; Sacerdoti, D.; Dalbeni, A. Prevalence of portal vein thrombosis in non-alcoholic fatty liver disease: A meta-analysis of observational studies. J. Thromb. Thrombolysis 2023, 57, 330–336. [Google Scholar] [CrossRef]
- Boccatonda, A.; Andreetto, L.; D’Ardes, D.; Cocco, G.; Rossi, I.; Vicari, S.; Schiavone, C.; Cipollone, F.; Guagnano, M.T. From NAFLD to MAFLD: Definition, Pathophysiological Basis and Cardiovascular Implications. Biomedicines 2023, 11, 883. [Google Scholar] [CrossRef]
- Kondili, L.A.; Zanetto, A.; Quaranta, M.G.; Ferrigno, L.; Panetta, V.; Calvaruso, V.; Zignego, A.L.; Brunetto, M.R.; Raimondo, G.; Biliotti, E.; et al. Predicting de-novo portal vein thrombosis after HCV eradication: A long-term competing risk analysis in the ongoing PITER cohort. United Eur. Gastroenterol. J. 2023. preprint. [Google Scholar] [CrossRef] [PubMed]
- Campello, E.; Radu, C.M.; Zanetto, A.; Bulato, C.; Shalaby, S.; Spiezia, L.; Franceschet, E.; Burral, P.; Russo, F.P.; Simioni, P. Changes in plasma circulating microvesicles in patients with HCV-related cirrhosis after treatment with direct-acting antivirals. Liver Int. 2020, 40, 913–920. [Google Scholar] [CrossRef]
- Jevtic, D.; Gavrancic, T.; Pantic, I.; Nordin, T.; Nordstrom, C.W.; Antic, M.; Pantic, N.; Kaljevic, M.; Joksimovic, B.; Jovanovic, M.; et al. Suppurative Thrombosis of the Portal Vein (Pylephlebits): A Systematic Review of Literature. J. Clin. Med. 2022, 11, 4992. [Google Scholar] [CrossRef] [PubMed]
- Lessiani, G.; Boccatonda, A.; D’Ardes, D.; Cocco, G.; Di Marco, G.; Schiavone, C. Mondor’s Disease in SARS-CoV-2 Infection: A Case of Superficial Vein Thrombosis in the Era of COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001803. [Google Scholar] [PubMed]
- Boccatonda, A.; Ianniello, E.; D’Ardes, D.; Cocco, G.; Giostra, F.; Borghi, C.; Schiavone, C. Can Lung Ultrasound be Used to Screen for Pulmonary Embolism in Patients with SARS-CoV-2 Pneumonia? Eur. J. Case Rep. Intern. Med. 2020, 7, 001748. [Google Scholar] [CrossRef]
- Boccatonda, A.; Campello, E.; Simion, C.; Simioni, P. Long-term hypercoagulability, endotheliopathy and inflammation following acute SARS-CoV-2 infection. Expert Rev. Hematol. 2023, 16, 1035–1048. [Google Scholar] [CrossRef]
- Boccatonda, A.; Grignaschi, A.; Lanotte, A.M.; Cocco, G.; Vidili, G.; Giostra, F.; Schiavone, C. Role of Lung Ultrasound in the Management of Patients with Suspected SARS-CoV-2 Infection in the Emergency Department. J. Clin. Med. 2022, 11, 2067. [Google Scholar] [CrossRef]
- Boccatonda, A.; Cocco, G.; Ianniello, E.; Montanari, M.; D’Ardes, D.; Borghi, C.; Giostra, F.; Copetti, R.; Schiavone, C. One year of SARS-CoV-2 and lung ultrasound: What has been learned and future perspectives. J. Ultrasound. 2021, 24, 115–123. [Google Scholar] [CrossRef] [PubMed]
- El-Hady, H.A.; Mahmoud Abd-Elwahab, E.S.; Mostafa-Hedeab, G.; Shawky Elfarargy, M. Portal vein thrombosis in patients with COVID-19: A systematic review. Asian J. Surg. 2023, 46, 3017–3026. [Google Scholar] [CrossRef]
- Zheng, X.; Gao, F.; Wang, L.; Meng, Y.; Ageno, W.; Qi, X. Incidence and outcomes of splanchnic vein thrombosis after diagnosis of COVID-19 or COVID-19 vaccination: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2023, 55, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Deltenre, P.; Payancé, A.; Elkrief, L.; La Mura, V.; Artru, F.; Baiges, A.; Cervoni, J.P.; China, L.; Colle, I.; Lemaitre, E.; et al. Splanchnic vein thrombosis associated with SARS-CoV-2 infection: A VALDIG case-control study. JHEP Rep. 2023, 5, 100894. [Google Scholar] [CrossRef]
- Puig, M.; Masnou, H.; Mesonero, F.; Menchén, L.; Bujanda, L.; Castro, J.; González-Partida, I.; Vicente, R.; González-Muñoza, C.; Iborra, M.; et al. Splanchnic Vein Thrombosis in Inflammatory Bowel Disease: An Observational Study from the ENEIDA Registry and Systematic Review. J. Clin. Med. 2023, 12, 7366. [Google Scholar] [CrossRef]
- Boccatonda, A.; Balletta, M.; Vicari, S.; Hoxha, A.; Simioni, P.; Campello, E. The Journey Through the Pathogenesis and Treatment of Venous Thromboembolism in Inflammatory Bowel Diseases: A Narrative Review. Semin. Thromb. Hemost. 2023, 49, 744–755. [Google Scholar] [CrossRef]
- Vazzana, N.; Santilli, F.; Lattanzio, S.; Liani, M.; Giacci, L.; Del Rosso, G.; Salvati, F.; Boccatonda, A.L.; Ferroni, P.; Davì, G. Determinants of thromboxane biosynthesis in patients with moderate to severe chronic kidney disease. Eur. J. Intern. Med. 2016, 33, 74–80. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Spiezia, L.; Burra, P.; Simioni, P.; Russo, F.P. Cancer-Associated Thrombosis in Cirrhotic Patients with Hepatocellular Carcinoma. Cancers 2018, 10, 450. [Google Scholar] [CrossRef]
- García-Villa, A.; Criado-Álvarez, J.J.; Carnevali, M.; Aramberri, M.; Font, C.; Díaz-Pedroche, C. Cancer-associated splanchnic vein thrombosis: Clinical features upon diagnosis and short-term outcomes. Thromb. Res. 2023, 231, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Hultcrantz, M.; Björkholm, M.; Landgren, O.; Kristinsson, S.Y.; Andersson, T.M.L. Risk for Arterial and Venous Thrombosis in Patients with Myeloproliferative Neoplasms. Ann. Intern. Med. 2018, 169, 268. [Google Scholar] [CrossRef] [PubMed]
- Lussana, F.; Carobbio, A.; Randi, M.L.; Elena, C.; Rumi, E.; Finazzi, G.; Bertozzi, I.; Pieri, L.; Ruggeri, M.; Palandri, F.; et al. A lower intensity of treatment may underlie the increased risk of thrombosis in young patients with masked polycythaemia vera. Br. J. Haematol. 2014, 167, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Paes, J.; Silva, G.A.V.; Tarragô, A.M.; Mourão, L.P.S. The Contribution of JAK2 46/1 Haplotype in the Predisposition to Myeloproliferative Neoplasms. Int. J. Mol. Sci. 2022, 23, 12582. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Rumi, E.; Finazzi, G.; Gisslinger, H.; Vannucchi, A.M.; Rodeghiero, F.; Randi, M.L.; Vaidya, R.; Cazzola, M.; Rambaldi, A.; et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: An international study. Leukemia 2013, 27, 1874–1881. [Google Scholar] [CrossRef] [PubMed]
- Sant’Antonio, E.; Guglielmelli, P.; Pieri, L.; Primignani, M.; Randi, M.L.; Santarossa, C.; Rumi, E.; Cervantes, F.; Delaini, F.; Carobbio, A.; et al. Splanchnic vein thromboses associated with myeloproliferative neoplasms: An international, retrospective study on 518 cases. Am. J. Hematol. 2020, 95, 156–166. [Google Scholar] [CrossRef]
- Cattaneo, D.; Gianelli, U.; Bianchi, P.; Cortelezzi, A.; Iurlo, A. Heterogeneity among splanchnic vein thrombosis associated with myeloproliferative neoplasms. Eur. J. Intern. Med. 2018, 52, e25–e26. [Google Scholar] [CrossRef]
- De Stefano, V.; Vannucchi, A.M.; Ruggeri, M.; Cervantes, F.; Alvarez-Larrán, A.; Iurlo, A.; Randi, M.L.; Pieri, L.; Rossi, E.; Guglielmelli, P.; et al. Splanchnic vein thrombosis in myeloproliferative neoplasms: Risk factors for recurrences in a cohort of 181 patients. Blood Cancer J. 2016, 6, e493. [Google Scholar] [CrossRef]
- Dentali, F.; Squizzato, A.; Brivio, L.; Appio, L.; Campiotti, L.; Crowther, M.; Grandi, A.L.M.; Ageno, W. JAK2V617F mutation for the early diagnosis of Ph- myeloproliferative neoplasms in patients with venous thromboembolism: A meta-analysis. Blood 2009, 113, 5617–5623. [Google Scholar] [CrossRef]
- Helman, R.; Pereira, W.O.; Marti, L.C.; Campregher, P.V.; Puga, R.D.; Hamerschlak, N.; Chiattone, C.S.; de Santos, F.P. Granulocyte whole exome sequencing and endothelial JAK2V617F in patients with JAK2V617F positive Budd-Chiari Syndrome without myeloproliferative neoplasm. Br. J. Haematol. 2018, 180, 443–445. [Google Scholar] [CrossRef]
- Guadall, A.; Lesteven, E.; Letort, G.; Awan Toor, S.; Delord, M.; Pognant, D.; Brusson, M.; Verger, E.; Maslah, N.; Giraudier, S.; et al. Endothelial Cells Harbouring the JAK2V617F Mutation Display Pro-Adherent and Pro-Thrombotic Features. Thromb. Haemost. 2018, 118, 1586–1599. [Google Scholar] [CrossRef] [PubMed]
- Guy, A.; Gourdou-Latyszenok, V.; Le Lay, N.; Peghaire, C.; Kilani, B.; Dias, J.V.; Duplaa, C.; Renault, M.-A.; Denis, C.; Villeval, J.L.; et al. Vascular endothelial cell expression of JAK2(V617F) is sufficient to promote a pro-thrombotic state due to increased P-selectin expression. Haematologica 2019, 104, 70–81. [Google Scholar] [CrossRef]
- Castiglione, M.; Jiang, Y.P.; Mazzeo, C.; Lee, S.; Chen, J.S.; Kaushansky, K.; Yin, W.; Lin, R.Z.; Zheng, H.; Zhan, H. Endothelial JAK2V617F mutation leads to thrombosis, vasculopathy, and cardiomyopathy in a murine model of myeloproliferative neoplasm. J. Thromb. Haemost. 2020, 18, 3359–3370. [Google Scholar] [CrossRef]
- Kumar, N.; Sharma, S.; Binota, J.; Ahluwalia, J.; Varma, N.; Naseem, S.; Chand, I.; Uppal, V.; Sinha, S.K. JAK2V617F Mutation in Patient with Splanchnic Vein Thrombosis. Indian J. Hematol. Blood Transfus. 2020, 36, 700–704. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Response Team. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12-March 16, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Yonal, I.; Pinarbası, B.; Hindilerden, F.; Hancer, V.S.; Nalcaci, M.; Kaymakoglu, S.; Diz-Kucukkaya, R. The clinical significance of JAK2V617F mutation for Philadelphia-negative chronic myeloproliferative neoplasms in patients with splanchnic vein thrombosis. J. Thromb. Thrombolysis 2012, 34, 388–396. [Google Scholar] [CrossRef]
- Hermouet, S.; Vilaine, M. The JAK2 46/1 haplotype: A marker of inappropriate myelomonocytic response to cytokine stimulation, leading to increased risk of inflammation, myeloid neoplasm, and impaired defense against infection? Haematologica 2011, 96, 1575–1579. [Google Scholar] [CrossRef]
- Klampfl, T.; Gisslinger, H.; Harutyunyan, A.S.; Nivarthi, H.; Rumi, E.; Milosevic, J.D.; Them, N.C.C.; Berg, T.; Gisslinger, B.; Pietra, D.; et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N. Engl. J. Med. 2013, 369, 2379–2390. [Google Scholar] [CrossRef]
- Turon, F.; Cervantes, F.; Colomer, D.; Baiges, A.; Hernández-Gea, V.; Garcia-Pagán, J.C. Role of calreticulin mutations in the aetiological diagnosis of splanchnic vein thrombosis. J. Hepatol. 2015, 62, 72–74. [Google Scholar] [CrossRef]
- Castro, N.; Rapado, I.; Ayala, R.; Martinez-Lopez, J. CALR mutations screening should not be studied in splanchnic vein thrombosis. Br. J. Haematol. 2015, 170, 588–589. [Google Scholar] [CrossRef]
- Colaizzo, D.; Amitrano, L.; Guardascione, M.A.; Favuzzi, G.; Tiscia, G.L.; D’Andrea, G.; Santacroce, R.; Grandone, E.; Margaglione, M. Clinical utility of screening for CALR gene exon 9 mutations in patients with splanchnic venous thrombosis. Thromb. Haemost. 2015, 113, 1381–1382. [Google Scholar] [CrossRef]
- Rajesh, R.; Gupta, M.; Kaur, N.; Lehl, S.S.; Tahlan, A.; Kaur, D. Prevalence of vascular thrombosis in patients with liver abscess. Trop. Doct. 2023, 54, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Mohammed, A.; Singh, A.; Siddiki, H.; Bhatt, A.; Sanaka, M.R.; Jang, S.; Simons-Linares, C.R.; Stevens, T.; Vargo, J.; et al. Mortality Trends, Outcomes, and Predictors of Portal Vein Thrombosis in Acute Pancreatitis Patients: A Propensity-Matched National Study. Dig. Dis. Sci. 2023, 68, 2674–2682. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, H.; Sohal, A.; Bains, K.; Dhaliwal, A.; Dukovic, D.; Singla, P.; Sharma, R.; Kohli, I.; Chintanaboina, J. Incidence and factors associated with portal vein thrombosis in patients with acute pancreatitis: A United States national retrospective study. Pancreatology 2023, 23, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Tankosic, N.; Stojkovic Lalosevic, M.; Alempijevic, T. Sport-Related Portal Vein Thrombosis: An Unusual Complication. Case Rep. Hepatol. 2017, 2017, 9324246. [Google Scholar] [CrossRef]
- Kassar, E.V.; Bass, J.R.; Douglas, E.; Speake, M.R. Portal and Mesenteric Vein Thrombosis Associated with Decompression Sickness in a 48-Year-Old Deep Sea Self-Contained Underwater Breathing Apparatus (SCUBA) Diver. Am. J. Case Rep. 2022, 23, e935473. [Google Scholar] [CrossRef]
- Wobser, H.; Schölmerich, J.; Büttner, R. 19-year-old kick-boxer with hematemesis and splenomegaly. Internist 2010, 51, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Mühlberg, K.S. Diagnosis and Therapy of Visceral Vein Thrombosis: An Update Based on the Revised AWMF S2k Guideline. Hamostaseologie 2023. [Google Scholar] [CrossRef] [PubMed]
- Primignani, M. Portal vein thrombosis, revisited. Dig. Liver Dis. 2010, 42, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Plemmons, R.M.; Dooley, D.P.; Longfield, R.N. Septic thrombophlebitis of the portal vein (pylephlebitis): Diagnosis and management in the modern era. Clin. Infect. Dis. 1995, 21, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [CrossRef]
- Tessler, F.N.; Gehring, B.J.; Gomes, A.S.; Perrella, R.R.; Ragavendra, N.; Busuttil, R.W.; Grant, E.G.; Tessler, B.J.G.F.N.; Parvey, H.R.; Raval, B.; et al. Diagnosis of portal vein thrombosis: Value of color Doppler imaging. AJR Am. J. Roentgenol. 1991, 157, 293–296. [Google Scholar] [CrossRef]
- Bach, A.M.; Hann, L.E.; Brown, K.T.; Getrajdman, G.I.; Herman, S.K.; Fong, Y.; Blumgart, H. Portal vein evaluation with US: Comparison to angiography combined with CT arterial portography. Radiology 1996, 201, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Giri, S.; Singh, A.; Kolhe, K.; Kozyk, M.; Roy, A. Assessment of portal system hemodynamics for the prediction of portal vein thrombosis in cirrhosis-A systematic review and meta-analysis. J. Clin. Ultrasound. 2023, 51, 1248–1258. [Google Scholar] [CrossRef]
- Rossi, S.; Rosa, L.; Ravetta, V.; Cascina, A.; Quaretti, P.; Azzaretti, A.; Scagnelli, P.; Tinelli, C.; Dionigi, P.; Calliada, F. Contrast-enhanced versus conventional and color Doppler sonography for the detection of thrombosis of the portal and hepatic venous systems. AJR Am. J. Roentgenol. 2006, 186, 763–773. [Google Scholar] [CrossRef]
- Cerrito, L.; Ainora, M.E.; Di Francesco, S.; Galasso, L.; Gasbarrini, A.; Zocco, M.A. The Role of Contrast-Enhanced Ultrasound (CEUS) in the Detection of Neoplastic Portal Vein Thrombosis in Patients with Hepatocellular Carcinoma. Tomography 2023, 9, 1976–1986. [Google Scholar] [CrossRef]
- Catalano, O.A.; Choy, G.; Zhu, A.; Hahn, P.F.; Sahani, D.V. Differentiation of malignant thrombus from bland thrombus of the portal vein in patients with hepatocellular carcinoma: Application of diffusion-weighted MR imaging. Radiology 2010, 254, 154–162. [Google Scholar] [CrossRef]
- Mori, H.; Hayashi, K.; Uetani, M.; Matsuoka, Y.; Iwao, M.; Maeda, H. High-attenuation recent thrombus of the portal vein: CT demonstration and clinical significance. Radiology 1987, 163, 353–356. [Google Scholar] [CrossRef]
- Spaander, M.C.; van Buuren, H.R.; Hansen, B.E.; Janssen, H.L. Ascites in patients with noncirrhotic nonmalignant extrahepatic portal vein thrombosis. Aliment. Pharmacol. Ther. 2010, 32, 529–534. [Google Scholar] [CrossRef]
- Ju, C.; Li, X.; Gadani, S.; Kapoor, B.; Partovi, S. Portal Vein Thrombosis: Diagnosis and Endovascular Management. Rofo 2022, 194, 169–180. [Google Scholar] [CrossRef]
- Sherman, C.B.; Behr, S.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y.; Mehta, N. Distinguishing Tumor from Bland Portal Vein Thrombus in Liver Transplant Candidates with Hepatocellular Carcinoma: The A-VENA Criteria. Liver Transpl. 2019, 25, 207–216. [Google Scholar] [CrossRef]
- Guerrero, A.; Campo, L.D.; Piscaglia, F.; Scheiner, B.; Han, G.; Violi, F.; Ferreira, C.-N.; Téllez, L.; Reiberger, T.; Basili, S. Anticoagulation improves survival in patients with cirrhosis and portal vein thrombosis: The IMPORTAL competing-risk meta-analysis. J. Hepatol. 2023, 79, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Castro, K.I.; Vitale, A.; Fadin, M.; Shalaby, S.; Zerbinati, P.; Sartori, M.T.; Landi, S.; Pettinari, I.; Piscaglia, F.; Han, G.; et al. A prediction model for successful anticoagulation in cirrhotic portal vein thrombosis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Turnes, J.; García-Pagán, J.C.; González, M.; Aracil, C.; Calleja, J.L.; Ripoll, C.; Abraldeṣ, J.G.; Bañares, R.; Villanueva, C.; Albillos, A.; et al. Portal hypertension-related complications after acute portal vein thrombosis: Impact of early anticoagulation. Clin. Gastroenterol. Hepatol. 2008, 6, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Condat, B.; Pessione, F.; Helene Denninger, M.; Hillaire, S.; Valla, D. Recent portal or mesenteric venous thrombosis: Increased recognition and frequent recanalization on anticoagulant therapy. Hepatology 2000, 32, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Amitrano, L.; Guardascione, M.A.; Scaglione, M.; Pezzullo, L.; Sangiuliano, N.; Armellino, M.F.; Manguso, F.; Margaglione, M.; Ames, P.R.J.; Iannaccone, L.; et al. Prognostic factors in noncirrhotic patients with splanchnic vein thromboses. Am. J. Gastroenterol. 2007, 102, 2464–2470. [Google Scholar] [CrossRef]
- Yao, C.; Zhao, M.; Ibrahim, B.; Saab, S. Anticoagulation for the Treatment of Portal Vein Thrombosis in Cirrhosis: A Systematic Review and Meta-Analysis of Comparative Studies. J. Clin. Exp. Hepatol. 2023, 13, 404–413. [Google Scholar] [CrossRef]
- Tarar, Z.I.; Farooq, U.; Kamal, F.; Nawaz, A.; Saleem, S.; Ghous, G.; Basar, O.; Chela, H.K.; Tahan, V.; Daglilar, E. Safety of anticoagulation use for treatment of portal vein thrombosis in liver cirrhosis and its effect on hospital-based outcomes: An insight from a US nationwide database. Postgrad Med. J. 2022, 99, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Candeloro, M.; Valeriani, E.; Monreal, M.; Ageno, W.; Riva, N.; Schulman, S.; Bang, S.-M.; Mellado, M.; Díaz-Peromingo, J.A.; Moisés, J.; et al. Clinical course and treatment of incidentally detected splanchnic vein thrombosis: An individual patient data meta-analysis. J. Thromb. Haemost. 2023, 21, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Li, S.; Zhao, J.; Li, J.; Gao, Y. Anticoagulation therapy early is safe in portal vein thrombosis patients with acute variceal bleeding: A multi-centric randomized controlled trial. Intern Emerg. Med. 2023, 18, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Sun, X.; Zhou, T.; Li, Y.; Chen, X.; Cheng, B.; Gao, Y. Efficacy and Safety of Nadroparin Calcium-Warfarin Sequential Anticoagulation in Portal Vein Thrombosis in Cirrhotic Patients: A Randomized Controlled Trial. Clin. Transl. Gastroenterol. 2020, 11, e00228. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.B.; Shu, R.H.; Yan, S.P.; Wu, H.; Chen, Y.; Wang, L.; Zhu, Q. Efficacy and safety of anticoagulation therapy with different doses of enoxaparin for portal vein thrombosis in cirrhotic patients with hepatitis B. Eur. J. Gastroenterol. Hepatol. 2015, 27, 914–919. [Google Scholar] [CrossRef] [PubMed]
- van Es, N.; Coppens, M.; Schulman, S.; Middeldorp, S.; Büller, H.R. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: Evidence from phase 3 trials. Blood 2014, 124, 1968–1975. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, I.; Tufano, A.; Strano, F.; Rufolo, P.; Donnarumma, S.; Palermo, V.; De Ruberto, F.; Cimino, E.; Guerrino, C.; Conca, P. Efficacy and safety of direct oral anticoagulants in splanchnic vein thrombosis: A pooled analysis of literature studies. J. Thromb. Haemost. 2023, 22, 534–544. [Google Scholar] [CrossRef]
- Li, A.; Zhang, M.C.; Li, P.; Eshaghpour, A.; Li, K.; Carrier, M.; Wells, P.; Crowther, M.A. Direct oral anticoagulants for the treatment of splanchnic vein thrombosis—A systematic review and meta-analysis. Thromb. Res. 2023, 229, 209–218. [Google Scholar] [CrossRef]
- Ai, M.H.; Dong, W.G.; Tan, X.P.; Xu, L.; Xu, C.; Zhang, Q.; Zhang, Y.; Li, J. Efficacy and safety study of direct-acting oral anticoagulants for the treatment of chronic portal vein thrombosis in patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Naymagon, L.; Tremblay, D.; Zubizarreta, N.; Moshier, E.; Naymagon, S.; Mascarenhas, J.; Schiano, T. The Natural History, Treatments, and Outcomes of Portal Vein Thrombosis in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Wang, L.; Gao, F.; Liu, L.; Qi, X. Anticoagulation Therapy for Splanchnic Vein Thrombosis Associated with Acute Pancreatitis: A Systematic Review and Meta-Analysis. Clin. Appl. Thromb. Hemost. 2023, 29. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Riva, N.; Schulman, S.; Beyer-Westendorf, J.; Bang, S.M.; Senzolo, M.; Grandone, E.; Pasca, S.; Di Minno, M.N.; Duce, R.; et al. Long-term Clinical Outcomes of Splanchnic Vein Thrombosis: Results of an International Registry. JAMA Intern. Med. 2015, 175, 1474–1480. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Beyer Westendorf, J.; Contino, L.; Bucherini, E.; Sartori, M.T.; Senzolo, M.; Grandone, E.; Santoro, R.; Carrier, M.; Delluc, A.; et al. Rivaroxaban for the treatment of noncirrhotic splanchnic vein thrombosis: An interventional prospective cohort study. Blood Adv. 2022, 6, 3569–3578. [Google Scholar] [CrossRef] [PubMed]
- Tufano, A.; Ageno, W.; Di Micco, P.; Niglio, A.; Rosa, V.; Ballaz, A.; Braester, A.; Rubio, C.M.; Isern, V.; Imbalzano, E.; et al. Outcomes during anticoagulation in patients with symptomatic vs. incidental splanchnic vein thrombosis. Thromb. Res. 2018, 164, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Riva, N.; Dentali, F.; Rodriguez-Castro, K.; Sartori, M.T.; Bang, S.M.; Martinelli, I.; Schulman, S.; Alatri, A.; Beyer-Westendorf, J.; et al. Long-Term Outcome of Splanchnic Vein Thrombosis in Cirrhosis. Clin. Transl. Gastroenterol. 2018, 9, 176. [Google Scholar] [CrossRef] [PubMed]
- Riva, N.; Ageno, W.; Schulman, S.; Beyer-Westendorf, J.; Duce, R.; Malato, A.; Santoro, R.; Poli, D.; Verhamme, P.; Martinelli, I.; et al. Clinical history and antithrombotic treatment of incidentally detected splanchnic vein thrombosis: A multicentre, international prospective registry. Lancet Haematol. 2016, 3, e267–e275. [Google Scholar] [CrossRef] [PubMed]
- De Gottardi, A.; Trebicka, J.; Klinger, C.; Plessier, A.; Seijo, S.; Terziroli, B.; Magenta, L.; Semela, D.; Buscarini, E.; Langlet, P.; et al. Antithrombotic treatment with direct-acting oral anticoagulants in patients with splanchnic vein thrombosis and cirrhosis. Liver Int. 2017, 37, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Naymagon, L.; Tremblay, D.; Zubizarreta, N.; Moshier, E.; Troy, K.; Schiano, T.; Mascarenhas, J. The efficacy and safety of direct oral anticoagulants in noncirrhotic portal vein thrombosis. Blood Adv. 2020, 4, 655–666. [Google Scholar] [CrossRef]
- Barbui, T.; De Stefano, V.; Carobbio, A.; Iurlo, A.; Alvarez-Larran, A.; Cuevas, B.; Marín, F.F.; Vannucchi, A.M.; Palandri, F.; Harrison, C.; et al. Direct oral anticoagulants for myeloproliferative neoplasms: Results from an international study on 442 patients. Leukemia 2021, 35, 2989–2993. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, D.; Winters, A.; Beckman, J.D.; Naymagon, L.; Patel, R.; Mascarenhas, J.; Schiano, T.D. Splanchnic vein thrombosis associated with myeloproliferative neoplasms. Thromb. Res. 2022, 218, 8–16. [Google Scholar] [CrossRef]
- Finazzi, G.; De Stefano, V.; Barbui, T. Splanchnic vein thrombosis in myeloproliferative neoplasms: Treatment algorithm 2018. Blood Cancer J. 2018, 8, 64. [Google Scholar] [CrossRef] [PubMed]
- Marchioli, R.; Finazzi, G.; Specchia, G.; Cacciola, R.; Cavazzina, R.; Cilloni, D.; De Stefano, V.; Elli, E.; Iurlo, A.; Latagliata, R.; et al. Cardiovascular events and intensity of treatment in polycythemia vera. N. Engl. J. Med. 2013, 368, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Simonetto, D.A.; Singal, A.K.; Garcia-Tsao, G.; Caldwell, S.H.; Ahn, J.; Kamath, P.S. ACG Clinical Guideline: Disorders of the Hepatic and Mesenteric Circulation. Am. J. Gastroenterol. 2020, 115, 18–40. [Google Scholar] [CrossRef]
- Rao, C.Y.; Xue, C.Y.; Fang, Q.Q.; Wu, L.; Huang, X.Q.; Chen, Y.; Chen, S.Y.; Li, F. Prevalence and clinical characteristics of advanced portal vein thrombosis in cirrhotic patients with gastroesophageal variceal hemorrhage. J. Dig. Dis. 2023, 24, 284–292. [Google Scholar] [CrossRef]
- McDowell, H.R.; Chuah, C.S.; Tripathi, D.; Stanley, A.J.; Forrest, E.H.; Hayes, P.C. Carvedilol is associated with improved survival in patients with cirrhosis: A long-term follow-up study. Aliment Pharmacol. Ther. 2021, 53, 531–539. [Google Scholar] [CrossRef]
- Sharma, M.; Singh, S.; Desai, V.; Shah, V.H.; Kamath, P.S.; Murad, M.H.; Simonetto, D.A. Comparison of Therapies for Primary Prevention of Esophageal Variceal Bleeding: A Systematic Review and Network Meta-analysis. Hepatology 2019, 69, 1657–1675. [Google Scholar] [CrossRef]
- Sato, A.; Watanabe, S.; Iseki, M.; Yamada, Y.; Kobayashi, R.; Furuya, M.; Arai, K.; Ohshina, E.; Tashiro, Y.; Nozaka, T.; et al. Anticoagulation against portal vein thrombosis reduces mortality and liver cirrhosis-related complications: A propensity score-matched study. Hepatol. Res. 2023, 53, 1096–1104. [Google Scholar] [CrossRef]
- Delgado, M.G.; Seijo, S.; Yepes, I.; Achécar, L.; Catalina, M.V.; García-Criado, A.; Abraldes, J.G.; de la Peña, J.; Bañares, R.; Albillos, A.; et al. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin. Gastroenterol. Hepatol. 2012, 10, 776–783. [Google Scholar] [CrossRef]
- Benevento, F.; Pecorelli, A.; Stefanescu, H.; Sparchez, Z.; Vukotic, R.; Pettinari, I.; Grigoras, C.-A.; Tovoli, F.; Ravaioli, F.; Stefanini, B.; et al. Presence of Hepatocellular Carcinoma Does Not Affect Course and Response to Anticoagulation of Bland Portal Vein Thrombosis in Cirrhotic Patients. J. Hepatocell. Carcinoma 2023, 10, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Potze, W.; Adelmeijer, J.; Lisman, T. Decreased in vitro anticoagulant potency of Rivaroxaban and Apixaban in plasma from patients with cirrhosis. Hepatology 2015, 61, 1435–1436. [Google Scholar] [CrossRef] [PubMed]
- Intagliata, N.M.; Henry, Z.H.; Maitland, H.; Shah, N.L.; Argo, C.K.; Northup, P.G.; Caldwell, S.H. Direct Oral Anticoagulants in Cirrhosis Patients Pose Similar Risks of Bleeding When Compared to Traditional Anticoagulation. Dig. Dis. Sci. 2016, 61, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Nagaoki, Y.; Aikata, H.; Daijyo, K.; Teraoka, Y.; Shinohara, F.; Nakamura, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Kawaoka, T. Efficacy and safety of edoxaban for treatment of portal vein thrombosis following danaparoid sodium in patients with liver cirrhosis. Hepatol. Res. 2018, 48, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wu, M.; Yu, S.; Xia, H.; Yu, W.; Huang, K.; Chen, Y. Comparison of the efficacy and safety between rivaroxaban and dabigatran in the treatment of acute portal vein thrombosis in cirrhosis. BMC Gastroenterol. 2023, 23, 329. [Google Scholar] [CrossRef] [PubMed]
- Montalvá, E.; Rodríguez-Perálvarez, M.; Blasi, A.; Bonanad, S.; Gavín, O.; Hierro, L.; Lladó, L.; Llop, E.; Pozo-Laderas, J.C.; Colmenero, J. Consensus Statement on Hemostatic Management, Anticoagulation, and Antiplatelet Therapy in Liver Transplantation. Transplantation 2022, 106, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Primignani, M.; Tosetti, G.; Ierardi, A.M. Approach to different thrombolysis techniques and timing of thrombolysis in the management of portal vein thrombosis in cirrhotic patients. J. Transl. Int. Med. 2023, 11, 198–202. [Google Scholar] [CrossRef]
- Hall, T.C.; Garcea, G.; Metcalfe, M.; Bilku, D.; Dennison, A.R. Management of acute non-cirrhotic and non-malignant portal vein thrombosis: A systematic review. World J. Surg. 2011, 35, 2510–2520. [Google Scholar] [CrossRef]
- Hollingshead, M.; Burke, C.T.; Mauro, M.A.; Weeks, S.M.; Dixon, R.G.; Jaques, P.F. Transcatheter thrombolytic therapy for acute mesenteric and portal vein thrombosis. J. Vasc. Interv. Radiol. 2005, 16, 651–661. [Google Scholar] [CrossRef]
- Giri, S.; Singh, A.; Kolhe, K.; Kale, A.; Shukla, A. Natural history of portal vein thrombosis in cirrhosis: A systematic review with meta-analysis. J. Gastroenterol. Hepatol. 2023, 38, 1710–1717. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhong, X.; Zhong, H.; Zhong, L.; Li, J.; Zhu, F.S.; Xia, L.; Yang, C.Q. Predicting the risk of variceal rehemorrhage in cirrhotic patients with portal vein thrombosis: A two-center retrospective study. J. Dig. Dis. 2023. [Google Scholar] [CrossRef]
- Attanasi, M.L.; Bou Daher, H.; Rockey, D.C. Natural History and Outcomes of Cavernous Transformation of the Portal Vein in Cirrhosis. Dig. Dis. Sci. 2023, 68, 3458–3466. [Google Scholar] [CrossRef]
- Luca, A.; Miraglia, R.; Caruso, S.; Milazzo, M.; Sapere, C.; Maruzzelli, L.; Vizzini, G.; Tuzzolino, F.; Gridelli, B.; Bosch, J. Short- and long-term effects of the transjugular intrahepatic portosystemic shunt on portal vein thrombosis in patients with cirrhosis. Gut 2011, 60, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Thornburg, B.; Desai, K.; Hickey, R.; Hohlastos, E.; Kulik, L.; Ganger, D.; Baker, T.; Abecassis, M.; Caicedo, J.C.; Ladner, D.; et al. Pretransplantation Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal Vein Thrombosis: Final Analysis of a 61-Patient Cohort. J. Vasc. Interv. Radiol. 2017, 28, 1714–1721.e2. [Google Scholar] [CrossRef] [PubMed]
- Mukund, A.; Marri, U.K.; Jindal, A.; Choudhury, A.; Patidar, Y.; Sarin, S.K. Safety and Efficacy of Transjugular Intrahepatic Portosystemic Shunt for Non-tumoral Cirrhotic Portal Vein Thrombosis Not Responding to Anticoagulation Therapy. Dig. Dis. Sci. 2023, 68, 3174–3184. [Google Scholar] [CrossRef] [PubMed]
- Villa, E.; Cammà, C.; Marietta, M.; Luongo, M.; Critelli, R.; Colopi, S.; Tata, C.; Zecchini, R.; Gitto, S.; Petta, S.; et al. Enoxaparin prevents portal vein thrombosis and liver decompensation in patients with advanced cirrhosis. Gastroenterology 2012, 143, 1253–1260.e4. [Google Scholar] [CrossRef]
- Kawanaka, H.; Akahoshi, T.; Itoh, S.; Iguchi, T.; Harimoto, N.; Uchiyama, H.; Yoshizumi, T.; Shirabe, K.; Takenaka, K.; Maehara, Y. Optimizing risk stratification in portal vein thrombosis after splenectomy and its primary prophylaxis with antithrombin III concentrates and danaparoid sodium in liver cirrhosis with portal hypertension. J. Am. Coll. Surg. 2014, 219, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Bai, D.S.; Xia, B.L.; Zhang, C.; Ye, J.; Qian, J.J.; Jin, S.J.; Jiang, G.Q. Warfarin versus aspirin prevents portal vein thrombosis after laparoscopic splenectomy and azygoportal disconnection: A randomized clinical trial. Int. J. Surg. 2019, 64, 16–23. [Google Scholar] [CrossRef]
- Bogari, H.; Patanwala, A.E.; Cosgrove, R.; Katz, M. Risk-assessment and pharmacological prophylaxis of venous thromboembolism in hospitalized patients with chronic liver disease. Thromb. Res. 2014, 134, 1220–1223. [Google Scholar] [CrossRef]
- Davis, J.P.E.; O’Leary, K.E.; Intagliata, N.M. Overuse of venous thromboembolism prophylaxis among hospitalized patients with liver disease. Eur. J. Haematol. 2020, 104, 223–229. [Google Scholar] [CrossRef]
- Barclay, S.M.; Jeffres, M.N.; Nguyen, K.; Nguyen, T. Evaluation of pharmacologic prophylaxis for venous thromboembolism in patients with chronic liver disease. Pharmacotherapy 2013, 33, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Shatzel, J.; Dulai, P.S.; Harbin, D.; Cheung, H.; Reid, T.N.; Kim, J.; James, S.L.; Khine, H.; Batman, S.; Whyman, J.; et al. Safety and efficacy of pharmacological thromboprophylaxis for hospitalized patients with cirrhosis: A single-center retrospective cohort study. J. Thromb. Haemost. 2015, 13, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Moorehead, K.J.; Jeffres, M.N.; Mueller, S.W. A Retrospective Cohort Analysis of Pharmacologic VTE Prophylaxis and Padua Prediction Score in Hospitalized Patients with Chronic Liver Disease. J. Pharm. Pract. 2017, 30, 58–63. [Google Scholar] [CrossRef]
- Yerke, J.; Bauer, S.R.; Bass, S.; Torbic, H.; Militello, M.; Roach, E.; Hanouneh, I.; Welch, S. Effectiveness of venous thromboembolism prophylaxis in patients with liver disease. World J. Hepatol. 2019, 11, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.; Burd, C.; Abeles, D.; Sherman, D. Decision making in venous thromboembolism prophylaxis: Is LWMH being inappropriately withheld from patients admitted with chronic liver disease? Clin. Med. 2015, 15, 31–34. [Google Scholar] [CrossRef]
- Boccatonda, A.; D’Ardes, D.; Rossi, I.; Grignaschi, A.; Lanotte, A.; Cipollone, F.; Guagnano, M.T.; Giostra, F. Platelet Count in Patients with SARS-CoV-2 Infection: A Prognostic Factor in COVID-19. J. Clin. Med. 2022, 11, 4112. [Google Scholar] [CrossRef]
- Roberts, L.N.; Hernandez-Gea, V.; Magnusson, M.; Stanworth, S.; Thachil, J.; Tripodi, A.; Lisman, T. Thromboprophylaxis for venous thromboembolism prevention in hospitalized patients with cirrhosis: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2022, 20, 2237–2245. [Google Scholar] [CrossRef]
- Swartz, D.E.; Hood, L.; Swartz, D.R.; Gupta, S. 30-Day Post-Discharge Prophylaxis with Rivaroxaban Prevents Porto-mesenteric Venous Thrombosis Following Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2023, 33, 1026–1031. [Google Scholar] [CrossRef]
- Ghabril, M.; Agarwal, S.; Lacerda, M.; Chalasani, N.; Kwo, P.; Tector, A.J. Portal Vein Thrombosis Is a Risk Factor for Poor Early Outcomes After Liver Transplantation: Analysis of Risk Factors and Outcomes for Portal Vein Thrombosis in Waitlisted Patients. Transplantation 2016, 100, 126–133. [Google Scholar] [CrossRef]
- Kotsifa, E.; Kykalos, S.; Machairas, N.; Nikiteas, N.; Sotiropoulos, G.C. Management of portal vein thrombosis in cirrhotic patients enlisted for liver transplantation: From diagnosis to treatment (Review). Biomed. Rep. 2021, 15, 94. [Google Scholar] [CrossRef]
- Zanetto, A.; Rodriguez-Kastro, K.I.; Germani, G.; Ferrarese, A.; Cillo, U.; Burra, P.; Senzolo, M. Mortality in liver transplant recipients with portal vein thrombosis—An updated meta-analysis. Transpl. Int. 2018, 31, 1318–1329. [Google Scholar] [CrossRef] [PubMed]
- Yeo, J.W.; Law, M.S.; Lim, J.C.; Ng, C.H.; Tan, D.J.; Tay, P.W.; Syn, N.; Tham, H.Y.; Huang, D.Q.; Siddiqui, M.S.; et al. Meta-analysis and systematic review: Prevalence, graft failure, mortality, and post-operative thrombosis in liver transplant recipients with pre-operative portal vein thrombosis. Clin. Transplant. 2022, 36, e14520. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, V.A.; O’Farrell, B.; Imber, C.; McCormack, L.; Northup, P.G.; Song, G.W.; Spiro, M.; Raptis, D.A.; Durand, F.; the ERAS4OLT.org Working Group. What is the optimal management of thromboprophylaxis after liver transplantation regarding prevention of bleeding, hepatic artery, or portal vein thrombosis? A systematic review of the literature and expert panel recommendations. Clin. Transplant. 2022, 36, e14629. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Type of Classification | Features |
|---|---|
| PVT site | Type 1: only trunk Type 2: only branch: 2A one branch and 2B both branches Type 3: trunk and branches |
| Portal venous system occlusion | OCCLUSIVE: no flow in PV lumen NON OCCLUSIVE: flow visible in PV lumen |
| Duration and presentation | RECENT: first time detected in previous patent PV, presence of hyperdense thrombus on imaging, absent or limited collateral circulation, dilated PV at the site of occlusion -asymptomatic -symptomatic CHRONIC: no hyperdense thrombus; previously diagnosed PVT on follow up, portal cavernoma -asymptomatic -symptomatic: portal hypertension |
| Persistent Acquired Risk Factors | Transient Acquired Risk Factors | Inherited Risk Factors |
|---|---|---|
|
|
|
| Title | Ageno W, et al. JAMA Intern Med. 2015 [105] | Ageno W, et al. Blood Adv. 2022 [106] | Tufano A, et al. Thromb Res. 2018 [107] | Ai MH et al. Eur J Gastroenterol Hepatol. 2020 [102] | Senzolo M et al. Clin Transl Gastroenterol. 2018 [108] | Riva N et al. Lancet Haematol. 2016 [109] | Gao Z et al. Intern Emerg Med. 2023 [96] | Zhou T et al. Clin Transl Gastroenterol. 2020 [97] | De Gottardi A et al. Liver Int. 2017 [110] | Cui S et al. Eur J Gastroenterol Hepatol. 2015 [98] |
|---|---|---|---|---|---|---|---|---|---|---|
| Type of study | Prospective cohort study | International single-arm clinical trial | RIETE (Registro Informatizado Enfermedad Trombo Embólica) registry | Prospective cohort study | Prospective cohort study | International, multicenter prospective cohort study | Randomized controlled trial | Single-center, single-blinded randomized controlled trial | Registry | Prospective clinical trial |
| Duration of intervention | 2 years | 6 months | 3 months | 6 months | 2 years | 2 years | 6 months | 6 months | Median 15 months (cirrhotic) and 26.5 months (non-cirrhotic) | 6 months |
| Condition | SVT diagnosis | Patients with a first episode of noncirrhotic, symptomatic, objectively diagnosed SVT | Patients with symptomatic and incidental SVT | Patients with liver cirrhosis older and ultrasound and CT portal venography suggesting PVT | SVT diagnosis | Incidentally detected SVT | PVT patients having cirrhosis and acute variceal bleeding | Cirrhotic patients with PVT who have not received anticoagulation therapy | Patients without cirrhosis (n = 58) Patients with cirrhosis (n = 36) | PVT in cirrhotic patients with hepatitis B |
| Sample size | 604 patients | 100 patients | 521 patients with SVT (212 symptomatic SVT and 309 incidental SVT) | 80 patients with cirrhosis and chronic PVT | 604 patients | 177 patients | 86 patients | 64 patients | 94 patients | 65 patients |
| Intervention | Anticoagulation was administered to 465 patients in the entire cohort (77.0%); 175 of the anticoagulant group (37.6%) received parenteral treatment only, and 290 patients (62.4%) were receiving vitamin K antagonists | Rivaroxaban 15 mg twice daily for 3 weeks, followed by 20 mg daily for an intended duration of 3 months | - | DOACs group (oral rivaroxaban tablets or dabigatran etexilate capsules). For patients with CP B or C grade, which are not suitable for rivaroxaban, dabigatran etexilate capsules 150 mg were administered orally twice daily | - | - | 1-month nadroparin calcium by subcutaneous injection following 5-month warfarin through oral administration | 1-month nadroparin calcium by subcutaneous injection followed by 5-month warfarin by oral administration | - | Enoxaparin 1 mg/kg subcutaneously every 12 h |
| Comparator | - | - | - | No anticoagulant treatment | - | - | Control group (without any anticoagulation therapy) | No anticoagulation therapy | - | Enoxaparin 1.5 mg/kg subcutaneously every 24 h |
| Primary endpoints | Major bleeding | Major bleeding | Rate and severity of symptomatic VTE recurrences and major bleeding events | Efficacy and safety of rivaroxaban and dabigatran for treatment of chronic PVT in liver cirrhosis patient | Major bleeding, thrombotic events, and all-cause mortality | Major bleeding (ISTH definition plus the need for hospital admission), thrombotic events (venous or arterial thromboses), and mortality | Rate of PVT recanalization | Overall recanalization rate, both complete and partial | To identify indications and reasons for starting or switching to DOACs and to report adverse effects, complications, and short-term outcome | To evaluate the efficacy and safety of anticoagulation therapy with different doses of enoxaparin for PVT |
| Secondary endpoints | Bleeding requiring hospitalization; thrombotic events, including venous and arterial thrombosis; all-cause mortality. | Death, recurrent SVT and complete vein recanalization within 3 months | - | - | - | - | Major bleeding events mainly referring to variceal rebleeding (5-day failure, 14-day, 4-week, 6-week, and 6-month rebleeding rates) and mortality after endoscopic variceal ligation | Bleeding rates, consisting of rates of hematemesis, melena, epistaxis, injection-site hemorrhage, and other bleeding events | - | - |
| Efficacy findings | The incidence rates were 7.3 per 100 patient-years (95% CI 5.8–9.3) for thrombotic events, and 10.3 per 100 patient-years (95% CI 8.5–12.5) for all-cause mortality. During anticoagulant treatment, the rate was 5.6 per 100 patient-years (95% CI 3.9–8.0) for thrombotic events. After treatment discontinuation, the rate was 10.5 per 100 patient-years (95% CI 6.8–16.3). The highest rate of thrombotic events during the whole study period was observed in patients with cirrhosis (11.3 per 100 patient-years [95% CI 7.7–16.8]; the lowest rate was in patients with SVT secondary to transient risk factors 3.2 per 100 patient-years [95% CI 1.4–7.0]. | Complete recanalization was documented in 47.3% of patients. One additional major bleeding event and 1 recurrent SVT occurred at 6 months. | Most (93%) patients received anticoagulant therapy (median, 147 days). During the course of anticoagulation, 20 patients developed symptomatic VTE recurrences. Patients with incidental SVT had a non-significantly higher risk for symptomatic VTE recurrences (a[HR]: 2.04; 95% CI: 0.71–5.88) than those with symptomatic SVT. Active cancer was associated with at increased risk for VTE recurrences (HR: 3.06; 95% CI: 1.14–8.17). | The complete/partial recanalization rate of DOACs was 12.8%. After 6 months of DOACs treatment, the PVT complete/partial recanalization rate of DOACs was 28.2%. The recanalization rate and portal vein flow velocity improvement were higher than those in the control group (p < 0.05). Patients’ total bilirubin level and Child–Pugh scores were improved in the DOACs group. The TEG coagulation index was lower in the DOACs group than in the control group (p < 0.05). | Vessel recanalization was documented in 47/98 patients with a radiological follow-up. Anticoagulation was associated with a 3.33-fold higher of recanalization rate, and a lower recurrent thrombosis rate. Mortality rates were 6.8 per 100 patient-years for patients with thrombosis completely or partially resolving during the follow-up, and 15.4 per 100 patient-years for those with stable or progressing thrombosis. An impact of SVT on survival was only apparent in patients with more advanced liver disease (CP B-C). | Anticoagulant treatment was prescribed to 62% patients. Median duration of anticoagulation was 6 months (IQR 5–12) for patients who received parenteral anticoagulants alone and 24 months (IQR 12–24) for patients treated with vitamin K antagonists. The incidence of thrombotic events was 8·0 events (95% CI 5.2–12.1) per 100 patient-years. On-treatment incidence was 3·9 events (95% CI 1.6–9.5) per 100 patient-years for thrombotic events. In patients with clinically suspected SVT, the incidence of thrombotic events was 7·0 events (95% CI 5.2–9.3) per 100 patient-years. | The overall recanalization rate in the nadroparin calcium-warfarin sequential therapy group was significantly higher than that in the control group (67.4% vs. 39.5%, p = 0.009). Low CP score (p = 0.039, OR: 0.692, 95% CI 0.488–0.982), D-dimer < 2.00 ug/mL (p = 0.030, OR: 3.600, 95% CI 1.134–11.430), and nadroparin calcium-warfarin sequential anticoagulation therapy (p = 0.002, OR: 4.189, 95% CI 1.660–10.568) were the predictors of PVT recanalization through univariate analysis. Nadroparin calcium-warfarin sequential anticoagulation therapy (p = 0.003, OR: 4.506, 95% CI 1.687–12.037) was the independent factor of recanalization through multivariate analysis. | Complete or partial recanalization of PVT was observed in 20/32 nadroparin calcium-warfarin sequential therapy group patients vs. 11/32 control group patients (62.5% vs. 34.4%, p = 0.024). CP score (p = 0.023), D-dimer < 2.00 μg/mL (p = 0.020), and nadroparin calcium-warfarin sequential anticoagulation therapy (p = 0.004) were predictors associated with the recanalization. Nadroparin calcium-warfarin sequential anticoagulation therapy (p = 0.008) was an independent predicting factor of recanalization. | Adverse events occurred in 17% of patients and included one case of recurrent PVT. The major reasons for choosing DOACs were no need for monitoring or inadequacy of INR to guide anticoagulation in cirrhotic patients. | About 78.5% achieved complete/partial recanalization of PVT after 6 months of anticoagulation therapy. CP scores were lower in the 51 patients who achieved complete/partial recanalization than those of the 14 nonresponders (p < 0.01). |
| Safety findings | The incidence rate was 3.8 per 100 patient-years (95% CI 2.7–5.2) for major bleeding. During anticoagulant treatment, the rate was 3.9 per 100 patient-years (95% CI 2.6–6.0) for major bleeding. After treatment discontinuation, rates were 1.0 per 100 patient-years (95% CI 0.3–4.2). The highest rate of major bleeding during the whole study period was observed in patients with cirrhosis (10.0 per 100 patient-years [95% CI 6.6–15.1]; the lowest rate was in patients with SVT secondary to transient risk factors (0.5 per 100 patient-years [95% CI 0.1–3.7]. | At 3 months, 2 patients (2.1%; 95% CI 0.6–7.2) had major bleeding events (both gastrointestinal). One (1.0%) patient died due to a non-SVT-related cause, 2 had recurrent SVT (2.1%). One additional major bleeding event occurred at 6 months. | About 26 patients had major bleeding (fatal bleeding, 5). Patients with incidental SVT had a similar risk for major bleeding (HR: 1.12; 95% CI: 0.47–2.63) than those with symptomatic SVT. Anemia (HR: 4.11; 95% CI: 1.45–11.6) or abnormal prothrombin time (HR: 4.10; 95% CI: 1.68–10.1) were associated with at increased risk for major bleeding. | There was no statistically significant difference between the DOACs group and control group in the cases of bleeding (p > 0.05). | Patients with and without anticoagulation experienced a similar rate of major bleedings. | On-treatment incidence was 3.2 events (95% CI 1.2–8.4) per 100 patient-years for major bleeding. In multivariate analysis, anticoagulant treatment as a time-dependent variable reduced the incidence of thrombotic events (HR 0·85, 95% CI 0.76–0.96) without increasing the risk of major bleeding (p > 0.05). In patients with clinically suspected SVT, the incidence of major bleeding was 3·9 events (95% CI 2.6–5.7) per 100 patient-years. | Nobody bled except for variceal rebleeding. Five-day failure and 14-day rebleeding were zero. There were no significantly different in 4-week (2.3% vs. 4.7%, p = 1.000), 6-week (4.7% vs. 9.3%, p = 0.672) and 6-month rebleeding (18.6% vs. 20.9%, p = 0.787) between the two groups. There was no mortality during six months follow-up. Low serum albumin (p = 0.011, OR: 0.844, 95% CI 0.741–0.962), high MELD score (p = 0.003, OR: 1.564, 95% CI 1.167–2.097) and CP score (p = 0.006, OR: 1.950, 95% CI 1.206–3.155) were predictors of rebleeding by univariate analysis. | No statistically significant difference in bleeding rate. | Five cases of bleeding. Treatment with DOACs was stopped in three cases. Renal and liver function did not change during treatment. | No patients showed variceal bleeding during anticoagulation therapy in the two groups. The rates of nonvariceal bleeding with the use of 1.5 mg/kg every 24 h (23.5%) were higher than those with the use of 1 mg/kg every 12 h (6.4%). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccatonda, A.; Gentilini, S.; Zanata, E.; Simion, C.; Serra, C.; Simioni, P.; Piscaglia, F.; Campello, E.; Ageno, W. Portal Vein Thrombosis: State-of-the-Art Review. J. Clin. Med. 2024, 13, 1517. https://doi.org/10.3390/jcm13051517
Boccatonda A, Gentilini S, Zanata E, Simion C, Serra C, Simioni P, Piscaglia F, Campello E, Ageno W. Portal Vein Thrombosis: State-of-the-Art Review. Journal of Clinical Medicine. 2024; 13(5):1517. https://doi.org/10.3390/jcm13051517
Chicago/Turabian StyleBoccatonda, Andrea, Simone Gentilini, Elisa Zanata, Chiara Simion, Carla Serra, Paolo Simioni, Fabio Piscaglia, Elena Campello, and Walter Ageno. 2024. "Portal Vein Thrombosis: State-of-the-Art Review" Journal of Clinical Medicine 13, no. 5: 1517. https://doi.org/10.3390/jcm13051517
APA StyleBoccatonda, A., Gentilini, S., Zanata, E., Simion, C., Serra, C., Simioni, P., Piscaglia, F., Campello, E., & Ageno, W. (2024). Portal Vein Thrombosis: State-of-the-Art Review. Journal of Clinical Medicine, 13(5), 1517. https://doi.org/10.3390/jcm13051517