

Durability of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation

 , , and
, , and
Abstract
1. Introduction
2. Patients and Methods
2.1. Ethical Statement
2.2. Study Population
3. Statistics
4. Results
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CO | cardiac output |
| CPB | cardiopulmonary bypass |
| CT | computed tomography |
| GI | gastro-intestinal |
| LVAD | left ventricular assist device |
| MCS | mechanical circulatory support |
| MELD | Model of End Stage Liver Disease |
| RHF | right heart failure |
| RVAD | right ventricular assist device |
| TR | tricuspid regurgitation |
| TVR | tricuspid valve repair |
References
- Nath, J.; Foster, E.; Heidenreich, P.A. Impact of tricuspid regurgitation on long-term survival. J. Am. Coll. Cardiol. 2004, 43, 405–409. [Google Scholar] [CrossRef]
- Topilsky, Y.; Maltais, S.; Medina Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tricuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef]
- Kelly, B.J.; Luxford, J.M.H.; Butler, C.G.; Huang, C.-C.; Wilusz, K.; Ejiofor, J.I.; Rawn, J.D.; Fox, J.A.; Shernan, S.K.; Muehlschlegel, J.D. Severity of tricuspid regurgitation is associated with long-term mortality. J. Thorac. Cardiovasc. Surg. 2018, 155, 1032–1038.e2. [Google Scholar] [CrossRef]
- Axtell, A.L.; Bhambhani, V.; Moonsamy, P.; Healy, E.W.; Picard, M.H.; Sundt, T.M.; Wasfy, J.H. Surgery Does Not Improve Survival in Patients with Isolated Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Färber, G.; Marx, J.; Scherag, A.; Saqer, I.; Diab, M.; Sponholz, C.; Doenst, T. Risk stratification for isolated tricuspid valve surgery assisted using the Model for End-Stage Liver Disease score. J. Thorac. Cardiovasc. Surg. 2022, 166, 1433–1441.e1. [Google Scholar] [CrossRef]
- Girdauskas, E.; Bernhardt, A.M.; Sinning, C.; Reichenspurner, H.; Sill, B.; Subbotina, I. Comparison of Outcomes of Tricuspid Valve Surgery in Patients with Reduced and Normal Right Ventricular Function. Thorac. Cardiovasc. Surg. 2017, 65, 617–625. [Google Scholar] [CrossRef]
- Miller, L.W.; Pagani, F.D.; Russell, S.D.; John, R.; Boyle, A.J.; Aaronson, K.D.; Conte, J.V.; Naka, Y.; Mancini, D.; Delgado, R.M.; et al. Use of a Continuous-Flow Device in Patients Awaiting Heart Transplantation. N. Engl. J. Med. 2007, 357, 885–896. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, M.S.; Rogers, J.G.; Milano, C.A.; Russell, S.D.; Conte, J.V.; Feldman, D.; Sun, B.; Tatooles, A.J.; Delgado, R.M., III; Long, J.W.; et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N. Engl. J. Med. 2009, 361, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- Pagani, F.D.; Miller, L.W.; Russell, S.D.; Aaronson, K.D.; John, R.; Boyle, A.J.; Conte, J.V.; Bogaev, R.C.; MacGillivray, T.E.; Naka, Y.; et al. Extended Mechanical Circulatory Support with a Continuous-Flow Rotary Left Ventricular Assist Device. J. Am. Coll. Cardiol. 2009, 54, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.C.; Koelling, T.M.; Pagani, F.D.; Aaronson, K.D. The Right Ventricular Failure Risk Score: A Pre-Operative Tool for Assessing the Risk of Right Ventricular Failure in Left Ventricular Assist Device Candidates. J. Am. Coll. Cardiol. 2008, 51, 2163–2172. [Google Scholar] [CrossRef]
- Fitzpatrick, J.R., 3rd; Frederick, J.R.; Hiesinger, W.; Hsu, V.M.; McCormick, R.C.; Kozin, E.D.; Laporte, C.M.; Lou, O.M.; Howell, E.; Dougherty, D.; et al. Early planned institution of biventricular mechanical circulatory support results in improved outcomes compared with delayed conversion of a left ventricular assist device to a biventricular assist device. J. Thorac. Cardiovasc. Surg. 2009, 137, 971–977. [Google Scholar] [CrossRef]
- Soliman, O.I.; Akin, S.; Muslem, R.; Boersma, E.; Manintveld, O.C.; Krabatsch, T.; Gummert, J.F.; de By, T.M.M.H.; Bogers, A.J.C.C.; Zijlstra, F.; et al. Derivation and validation of a novel right-sided heart failure model after implantation of continuous flow left ventricular assist devices: The EUROMACS (European Registry for Patients with Mechanical Circulatory Support) right-sided heart failure risk score. Circulation 2018, 137, 891–906. [Google Scholar]
- Kormos, R.L.; Teuteberg, J.J.; Pagani, F.D.; Russell, S.D.; John, R.; Miller, L.W.; Massey, T.; Milano, C.A.; Moazami, N.; Sundareswaran, K.S.; et al. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricular assist device: Incidence, risk factors, and effect on outcomes. J. Thorac. Cardiovasc. Surg. 2010, 139, 1316–1324. [Google Scholar] [CrossRef]
- Dandel, M.; Krabatsch, T.; Falk, V. Left ventricular vs. biventricular mechanical support: Decision making and strategies for avoidance of right heart failure after left ventricular assist device implantation. Int. J. Cardiol. 2015, 198, 241–250. [Google Scholar] [CrossRef]
- Sparrow, C.T.; Nassif, M.E.; Raymer, D.S.; Novak, E.; LaRue, S.J.; Schilling, J.D. Pre-Operative Right Ventricular Dysfunction Is Associated with Gastrointestinal Bleeding in Patients Supported with Continuous-Flow Left Ventricular Assist Devices. JACC Heart Fail. 2015, 3, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Kapelios, C.J.; Lund, L.H.; Wever-Pinzon, O.; Selzman, C.H.; Myers, S.L.; Cantor, R.S.; Stehlik, J.; Chamogeorgakis, T.; McKellar, S.H.; Koliopoulou, A.; et al. Right Heart Failure Following Left Ventricular Device Implantation: Natural History, Risk Factors, and Outcomes: An Analysis of the STS INTERMACS Database. Circ. Heart Fail. 2022, 15, e008706. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, K.; Homma, S.; Han, J.; Takayama, H.; Colombo, P.C.; Yuzefpolskaya, M.; Garan, A.R.; Farr, M.A.; Kurlansky, P.; Di Tullio, M.R.; et al. Usefulness of Tricuspid Annular Diameter to Predict Late Right Sided Heart Failure in Patients with Left Ventricular Assist Device. Am. J. Cardiol. 2018, 122, 115–120. [Google Scholar] [CrossRef]
- Barac, Y.D.; Nicoara, A.; Bishawi, M.; Schroder, J.N.; Daneshmand, M.A.; Hashmi, N.K.; Velazquez, E.; Rogers, J.G.; Patel, C.B.; Milano, C.A. Durability and Efficacy of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. JACC Heart Fail. 2020, 8, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Veen, K.M.; Caliskan, K.; De By, T.M.M.H.; Mokhles, M.M.; Soliman, O.I.; Mohacsi, P.; Schoenrath, F.; Gummert, J.; Paluszkiewicz, L.; Netuka, I.; et al. Outcomes after tricuspid valve surgery concomitant with left ventricular assist device implantation in the EUROMACS registry: A propensity score matched analysis. Eur. J. Cardio-Thorac. Surg. 2019, 56, 1081–1089. [Google Scholar] [CrossRef]
- Mihalj, M.; Jezovnik, M.K.; Benk, J.; Heg, D.; Podstatzky-Lichtenstein, T.; Beyersdorf, F.; Radovancevic, R.; Gregoric, I.D.; Hunziker, L.; Siepe, M.; et al. Concomitant tricuspid valve repair in left ventricular assist device implantation may increase the risk for temporary right ventricular support but does not impact overall outcomes. Eur. J. Cardio-Thorac. Surg. 2022, 63, ezac555. [Google Scholar] [CrossRef]
- Beyersdorf, F.; Vahanian, A.; Milojevic, M.; Praz, F.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardio-Thorac. Surg. 2021, 60, 727–800. [Google Scholar] [CrossRef]
- Zaidi, A.; Oxborough, D.; Augustine, D.X.; Bedair, R.; Harkness, A.; Rana, B.; Robinson, S.; Badano, L.P. Education Committee of the British Society of Echocardiography Echocardiographic assessment of the tricuspid and pulmonary valves: A practical guideline from the British Society of Echocardiography. Echo Res. Pract. 2020, 7, G95–G122. [Google Scholar] [CrossRef] [PubMed]
- Mulzer, J.; Krastev, H.; Hoermandinger, C.; Meyer, A.; Haese, T.; Stein, J.; Müller, M.; Schoenrath, F.; Knosalla, C.; Starck, C.; et al. Development of tricuspid regurgitation and right ventricular performance after implantation of centrifugal left ventricular assist devices. Ann. Cardiothorac. Surg. 2021, 10, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Maltais, S.; Topilsky, Y.; Tchantchaleishvili, V.; McKellar, S.H.; Durham, L.A.; Joyce, L.D.; Daly, R.C.; Park, S.J. Surgical treatment of tricuspid valve insufficiency promotes early reverse remodeling in patients with axial-flow left ventricular assist devices. J. Thorac. Cardiovasc. Surg. 2012, 143, 1370–1376.e1. [Google Scholar] [CrossRef] [PubMed]
- Brewer, R.J.; Cabrera, R.; El-Atrache, M.; Zafar, A.; Hrobowski, T.N.; Nemeh, H.M.; Selektor, Y.; Paone, G.; Williams, C.T.; Velez, M.; et al. Relationship of Tricuspid Repair at the Time of Left Ventricular Assist Device Implantation and Survival. Int. J. Artif. Organs 2014, 37, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Takeda, K.; Takayama, H.; Kurlansky, P.A.; Mauro, C.M.; Colombo, P.C.; Yuzefpolskaya, M.; Fukuhara, S.; Truby, L.K.; Topkara, V.K.; et al. Durability and clinical impact of tricuspid valve procedures in patients receiving a continuous-flow left ventricular assist device. J. Thorac. Cardiovasc. Surg. 2016, 151, 520–527.e1. [Google Scholar] [CrossRef] [PubMed]
- Potapov, E.V.; Antonides, C.; Crespo-Leiro, M.G.; Combes, A.; Färber, G.; Hannan, M.M.; Kukucka, M.; de Jonge, N.; Loforte, A.; Lund, L.H.; et al. 2019 EACTS Expert Consensus on long-term mechanical circulatory support. Eur. J. Cardio-Thorac. Surg. 2019, 56, 230–270. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Takagi, H.; Kuno, T. Impact of Different Annuloplasty Methods for Tricuspid Regurgitation: A Network Meta-Analysis. Ann. Thorac. Surg. 2021, 111, 2004–2010. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | ||
|---|---|---|
| (n = 94) | ||
| Age [years] | 59.8 ± 11.4 | |
| Male [%] | 84 (89.4) | |
| BMI [kg/m2] | 26.9 ± 4.8 | |
| PM/ICD | 56 (59.6) | |
| COPD | 10 (10.6) | |
| Diabetes, insulin dependent | 28 (39.8) | |
| ICM/DCM | 37 (39.4)/56 (59.6) | |
| DT/BTT/BTD | 40 (42.6)/31 (33)/23 (24.5) | |
| INTERMACS level | 1 | 15 (16.0) |
| 2 | 20 (21.3) | |
| 3 | 30 (31.9) | |
| 4 | 29 (30.9) | |
| Preoperative MCS | 12 (12.8) | |
| Echocardiographic data | ||
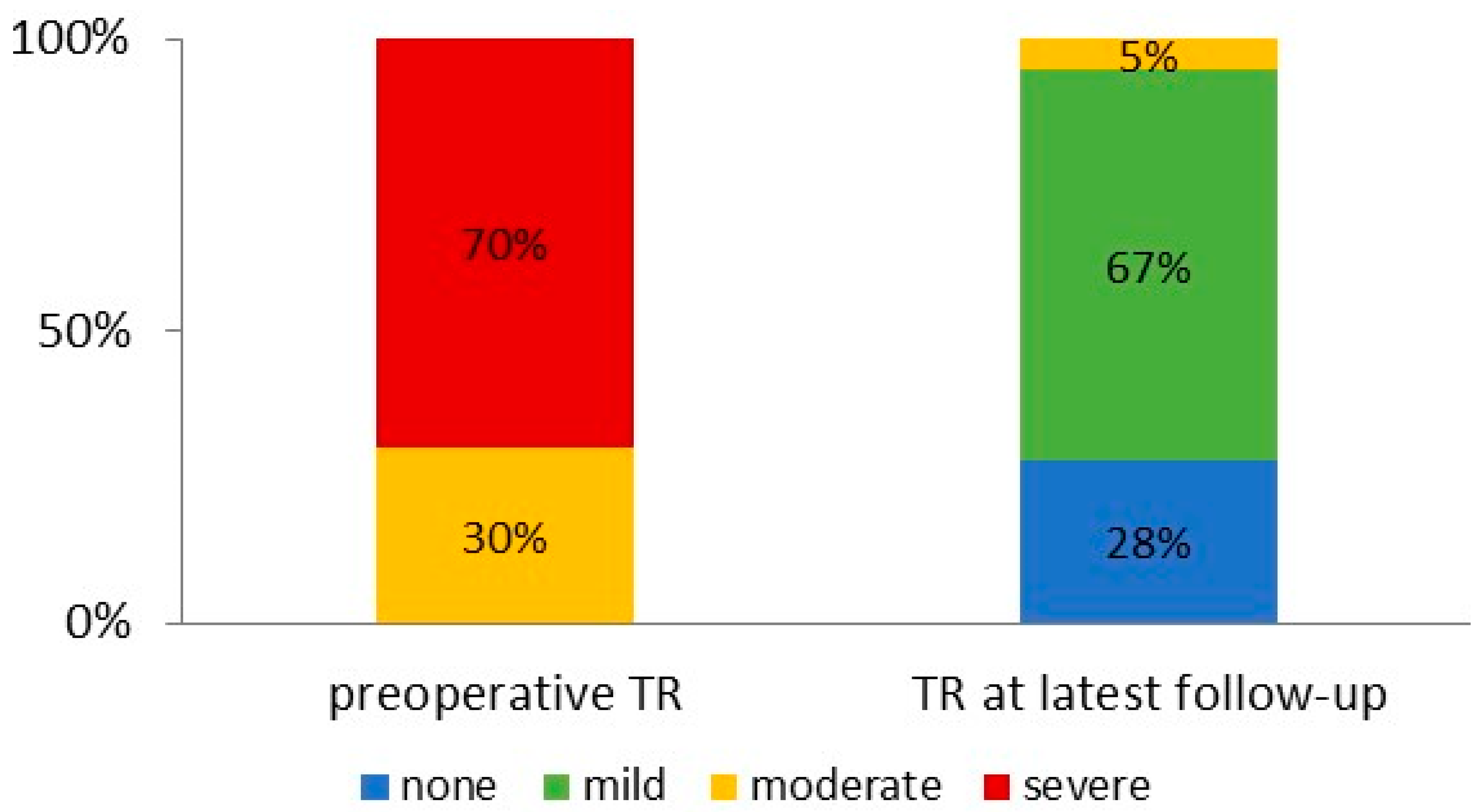
| Degree of TR | Moderate | 28 (29.8) |
| Severe | 66 (70.2) | |
| Severe RV dysfunction | 61 (64.9) | |
| TAPSE [mm] | 12.6 ± 3.8 | |
| Right heart catheterization: | ||
| CVP [mmHg] | 14.1 ± 6.8 | |
| Mean PAP [mmHg] | 37.2 ± 13.2 | |
| PCWP [mmHg] | 26.7 ± 8.7 | |
| Cardiac index [L/min/m2] | 1.9 ± 0.6 | |
| PVR | 235.2 ± 170.4 | |
| CVP/PCWP [mmHg] | 0.53 ± 0.3 | |
| PAPi | 1.9 ± 1.1 | |
| EUROMACS right heart failure score | ||
| 0–2 | 15 (15.9) | |
| >2–4 | 19 (20.2) | |
| >4 | 60 (63.8) | |
| All Patients | |
|---|---|
| (n = 94) | |
| Procedural duration [hours] | 3.8 ± 1.1 |
| CPB time [min] | 110.7 ± 30.5 |
| Redo surgery | 19 (20.2) |
| HeartMate II (Abbott) | 14 (14.9) |
| HeartMate 3 (Abbott) | 71 (75.3) |
| HVAD (Medtronic) | 6 (6.4) |
| HeartAssist 5 (Micromed Cardiovascular) | 3 (3.2) |
| TV annuloplasty ring type | |
| Medtronic Simplici-T | 7 (50.0) |
| Cosgrove-Edwards | 46 (48.9) |
| Medtronic Simulus | 1 (1.1) |
| Concomitant procedures (other than TVR) | |
| Aortic valve replacement | 14 (14.9) |
| ASD/PFO closure | 18 (19.1) |
| CABG | 3 (3.2) |
| Postoperative adverse events | |
| RVAD implantation | 2 (2.1) |
| Renal insufficiency requiring dialysis | 18 (19.1) |
| Pump thrombosis | none |
| Arrythmia | 7 (7.4) |
| Visceral ischemia | 2 (2.1) |
| Perioperative stroke | 5 (5.3) |
| All Patients | ||
|---|---|---|
| (n = 94) | ||
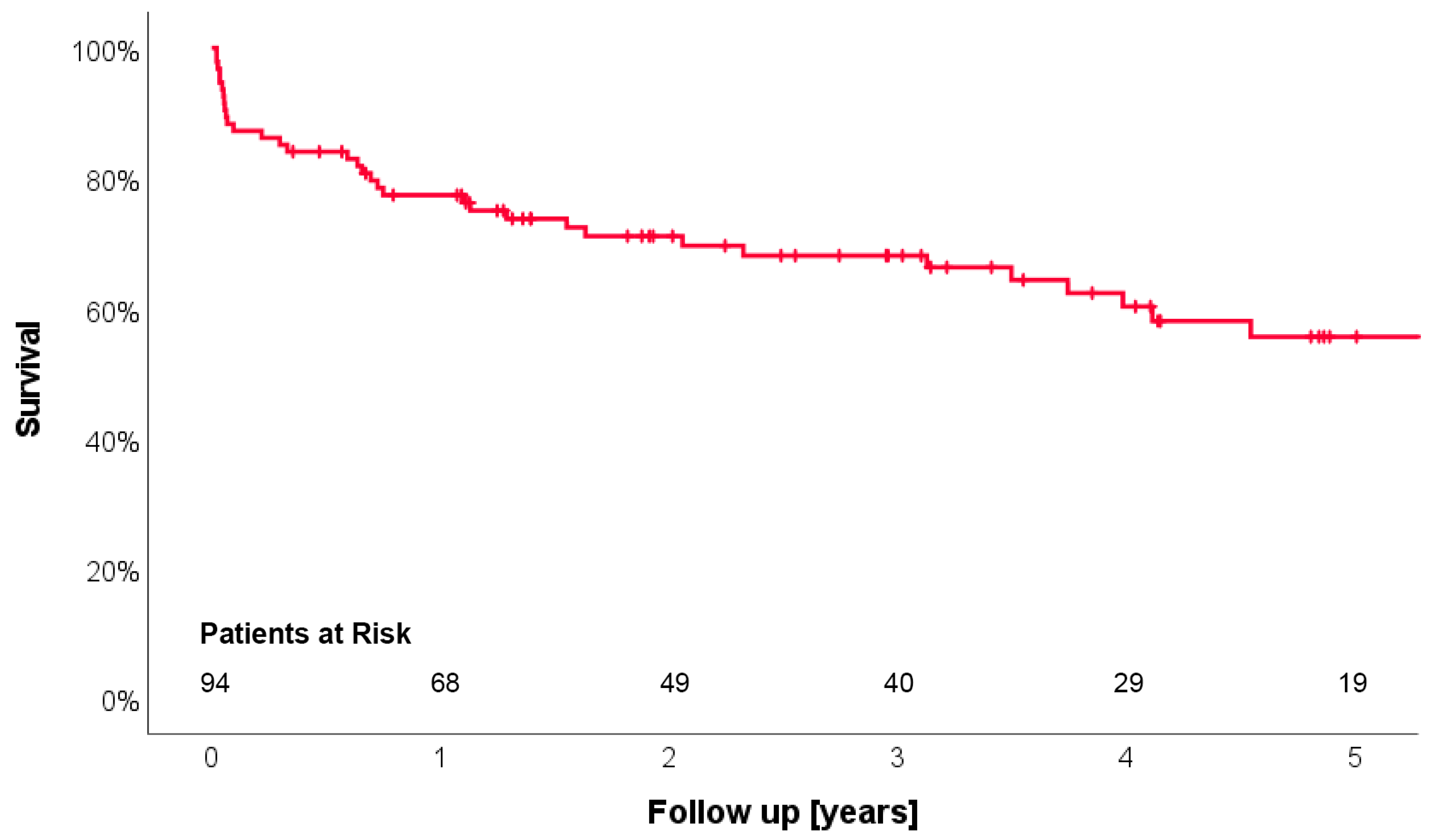
| Follow-up time [years] | 2.8 ± 2.3 (7 days to 10.6 years) | |
| Pump thrombosis | 2 (2.1) | |
| Stroke | 8 (8.5) | |
| GI bleeding | 9 (9.6) | |
| Rehospitalization due to RHF | 2 (2.0) | |
| Heart transplantation | 12 (12.8) | |
| Echocardiographic data | ||
| Degree of TR | None/trace | 26 (27.7) |
| Mild | 63 (67.0) | |
| Moderate | 5 (5.3) | |
| Severe | none | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Färber, G.; Schwan, I.; Kirov, H.; Rose, M.; Tkebuchava, S.; Schneider, U.; Caldonazo, T.; Diab, M.; Doenst, T. Durability of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. J. Clin. Med. 2024, 13, 1411. https://doi.org/10.3390/jcm13051411
Färber G, Schwan I, Kirov H, Rose M, Tkebuchava S, Schneider U, Caldonazo T, Diab M, Doenst T. Durability of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. Journal of Clinical Medicine. 2024; 13(5):1411. https://doi.org/10.3390/jcm13051411
Chicago/Turabian StyleFärber, Gloria, Imke Schwan, Hristo Kirov, Marcel Rose, Sophie Tkebuchava, Ulrich Schneider, Tulio Caldonazo, Mahmoud Diab, and Torsten Doenst. 2024. "Durability of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation" Journal of Clinical Medicine 13, no. 5: 1411. https://doi.org/10.3390/jcm13051411
APA StyleFärber, G., Schwan, I., Kirov, H., Rose, M., Tkebuchava, S., Schneider, U., Caldonazo, T., Diab, M., & Doenst, T. (2024). Durability of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. Journal of Clinical Medicine, 13(5), 1411. https://doi.org/10.3390/jcm13051411