
Performance of ECG-Derived Digital Biomarker for Screening Coronary Occlusion in Resuscitated Out-of-Hospital Cardiac Arrest Patients: A Comparative Study between Artificial Intelligence and a Group of Experts

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. The AI Algorithm
2.2. Study Setting, Participants, and Data Preparation
2.3. Definitions
2.4. Measurements of Human and AI Performance
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. QCG Biomarker Versus Expert Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621, Correction in Circulation 2023, 147, e622. [Google Scholar] [CrossRef]
- Hawkes, C.; Booth, S.; Ji, C.; Brace-McDonnell, S.J.; Whittington, A.; Mapstone, J.; Cooke, M.W.; Deakin, C.D.; Gale, C.P.; Fothergill, R.; et al. Epidemiology and outcomes from out-of-hospital cardiac arrests in England. Resuscitation 2016, 110, 133–140. [Google Scholar] [CrossRef]
- Chen, N.; Callaway, C.W.; Guyette, F.X.; Rittenberger, J.C.; Doshi, A.A.; Dezfulian, C.; Elmer, J. Arrest etiology among patients resuscitated from cardiac arrest. Resuscitation 2018, 130, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, C.M.; Joly, L.-M.; Rosenberg, A.; Monchi, M.; Weber, S.N.; Dhainaut, J.-F.A.; Carli, P. Immediate Coronary Angiography in Survivors of Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 1997, 336, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Noc, M.; Fajadet, J.; Lassen, J.F.; Kala, P.; MacCarthy, P.; Olivecrona, G.K.; Windecker, S.; Spaulding, C. Invasive coronary treatment strategies for out-of-hospital cardiac arrest: A consensus statement from the European Association for Percutaneous Cardiovascular Interventions (EAPCI)/Stent For Life (SFL) groups. EuroIntervention 2014, 10, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Batista, L.M.; Lima, F.O.; Januzzi, J.L.; Donahue, V.; Snydeman, C.; Greer, D.M. Feasibility and safety of combined percutaneous coronary intervention and therapeutic hypothermia following cardiac arrest. Resuscitation 2010, 81, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Welsford, M.; Bossard, M.; Shortt, C.; Pritchard, J.; Natarajan, M.K.; Belley-Côté, E.P. Does Early Coronary Angiography Improve Survival After out-of-Hospital Cardiac Arrest? A Systematic Review with Meta-Analysis. Can. J. Cardiol. 2018, 34, 180–194. [Google Scholar] [CrossRef]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.; Dubois, E.A.; Meuwissen, M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2019, 380, 1397–1407. [Google Scholar] [CrossRef]
- Staudacher, I.I.; den Uil, C.; Jewbali, L.; van Zandvoort, L.; Zijlstra, F.; Van Mieghem, N.; Boersma, E.; Daemen, J. Timing of coronary angiography in survivors of out-of-hospital cardiac arrest without obvious extracardiac causes. Resuscitation 2018, 123, 98–104. [Google Scholar] [CrossRef]
- Hollenbeck, R.D.; McPherson, J.A.; Mooney, M.R.; Unger, B.T.; Patel, N.C.; McMullan, P.W.; Hsu, C.-H.; Seder, D.B.; Kern, K.B. Early cardiac catheterization is associated with improved survival in comatose survivors of cardiac arrest without STEMI. Resuscitation 2014, 85, 88–95. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Peberdy, M.A.; Callaway, C.W.; Neumar, R.W.; Geocadin, R.G.; Zimmerman, J.L.; Donnino, M.; Gabrielli, A.; Silvers, S.M.; Zaritsky, A.L.; Merchant, R.; et al. Part 9: Post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122 (18 Suppl. 3), S768–S786, Correction in Circulation 2011, 123, e237. [Google Scholar] [CrossRef]
- Alpert, J.S.; Thygesen, K.; Antman, E.; Bassand, J.P. Myocardial infarction redefined—A consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J. Am. Coll. Cardiol. 2000, 36, 959–969. [Google Scholar]
- Kim, Y.-J.; Min, S.-Y.; Lee, D.H.; Lee, B.K.; Jeung, K.W.; Lee, H.J.; Shin, J.; Ko, B.S.; Ahn, S.; Nam, G.-B.; et al. The Role of Post-Resuscitation Electrocardiogram in Patients With ST-Segment Changes in the Immediate Post-Cardiac Arrest Period. JACC Cardiovasc. Interv. 2017, 10, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Park, M.J.; Ko, Y.; Soh, M.-S.; Kim, H.M.; Kim, C.H.; Lee, E.; Kim, J. Artificial intelligence versus physicians on interpretation of printed ECG images: Diagnostic performance of ST-elevation myocardial infarction on electrocardiography. Int. J. Cardiol. 2022, 363, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; De Simone, G.; Ford, E.S.; et al. Heart Disease and Stroke Statistics-2011 Update A Report From the American Heart Association. Circulation 2011, 123, e18–e209. [Google Scholar] [CrossRef] [PubMed]
- Desch, S.; Freund, A.; Akin, I.; Behnes, M.; Preusch, M.R.; Zelniker, T.A.; Skurk, C.; Landmesser, U.; Graf, T.; Eitel, I.; et al. Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation. N. Engl. J. Med. 2021, 385, 2544–2553. [Google Scholar] [CrossRef] [PubMed]
- Lemkes, J.S.; Janssens, G.N.; van der Hoeven, N.W.; Jewbali, L.S.; Dubois, E.A.; Meuwissen, M.M.; Rijpstra, T.A.; Bosker, H.A.; Blans, M.J.; Bleeker, G.B.; et al. Coronary Angiography After Cardiac Arrest Without ST Segment Elevation: One-Year Outcomes of the COACT Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Joffre, J.; Varenne, O.; Bougouin, W.; Rosencher, J.; Mira, J.-P.; Cariou, A. Stent thrombosis: An increased adverse event after angioplasty following resuscitated cardiac arrest. Resuscitation 2014, 85, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Laver, S.; Farrow, C.; Turner, D.; Nolan, J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensiv. Care Med. 2004, 30, 2126–2128. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef] [PubMed]
- Madsen, L.H.; Christensen, G.; Lund, T.; Serebruany, V.L.; Granger, C.B.; Hoen, I.; Grieg, Z.; Alexander, J.H.; Jaffe, A.S.; Van Eyk, J.E.; et al. Time course of degradation of cardiac troponin I in patients with acute ST-elevation myocardial infarction: The ASSENT-2 troponin substudy. Circ. Res. 2006, 99, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Wereski, R.; Chapman, A.R.; Lee, K.K.; Smith, S.W.; Lowe, D.J.; Gray, A.; Mills, N.L. High-Sensitivity Cardiac Troponin Concentrations at Presentation in Patients With ST-Segment Elevation Myocardial Infarction. JAMA Cardiol. 2020, 5, 1302–1304. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Schnaubelt, S.; Caputo, M.L.; Klersy, C.; Clodi, C.; Bruno, J.; Compagnoni, S.; Benvenuti, C.; Domanovits, H.; Burkart, R.; et al. Association of Timing of Electrocardiogram Acquisition After Return of Spontaneous Circulation With Coronary Angiography Findings in Patients With Out-of-Hospital Cardiac Arrest. JAMA Netw. Open 2021, 4, e2032875. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Occlusion | No Occlusion | p | ||
|---|---|---|---|---|
| (n = 24) | (n = 34) | |||
| Age, mean (SD) | 55.1 (10.4) | 51.8 (13.5) | 0.318 | |
| Sex, frequency (%) | 1.000 | |||
| Male | 21 (87.5) | 29 (85.3) | ||
| Female | 3 (12.5) | 5 (14.7) | ||
| Height, median (IQR) | 170.0 (166.5–175.0) | 170.0 (165.0–176.0) | 0.623 | |
| Weight, mean (SD) | 68.6 (10.1) | 70.0 (12.9) | 0.664 | |
| HTN, frequency (%) | 1.000 | |||
| Yes | 10 (41.7) | 14 (41.2) | ||
| No | 14 (58.3) | 20 (58.8) | ||
| DM, frequency (%) | 0.883 | |||
| Yes | 4 (16.7) | 4 (11.8) | ||
| No | 20 (83.3) | 30 (88.2) | ||
| CVD, frequency (%) | 0.706 | |||
| Yes | 5 (20.8) | 8 (23.5) | ||
| No | 17 (70.8) | 21 (61.8) | ||
| Unknown | 2 (8.3) | 5 (14.7) | ||
| Witnessed, frequency (%) | 1.000 | |||
| Yes | 20 (83.3) | 29 (85.3) | ||
| No | 4 (16.7) | 5 (14.7) | ||
| Bystander CPR, frequency (%) | 0.474 | |||
| Yes | 17 (70.8) | 28 (82.4) | ||
| No | 7 (29.2) | 6 (17.6) | ||
| 30-day Survival, frequency (%) | 0.755 | |||
| Yes | 20 (83.3) | 26 (76.5) | ||
| No | 2 (8.3) | 5 (14.7) | ||
| Unknown | 2 (8.3) | 3 (8.8) | ||
| Discharge CPC, frequency (%) | 0.765 | |||
| 1 | 17 (70.8) | 22 (64.7) | ||
| 2 | 3 (12.5) | 3 (8.8) | ||
| 3 | 0 (0.0) | 0 (0.0) | ||
| 4 | 2 (8.3) | 3 (8.8) | ||
| 5 | 2 (8.3) | 4 (11.8) | ||
| Unknown | 0 (0.0) | 2 (5.9) | ||
| Emergency Angiography (<24 h), frequency (%) | 0.016 | |||
| Emergency | 19 (79.2) | 15 (44.1) | ||
| Delayed | 5 (20.8) | 19 (55.9) | ||
| Initial Rhythm (Prehospital), frequency (%) | 0.583 | |||
| Shockable | 21 (87.5) | 29 (85.3) | ||
| Asystole | 1 (4.2) | 3 (8.8) | ||
| PEA | 2 (8.3) | 1 (2.9) | ||
| Unknown | 0 (0.0) | 1 (2.9) | ||
| Initial Rhythm (ED Arrival), frequency (%) | 0.172 | |||
| Shockable | 5 (20.8) | 1 (2.9) | ||
| Asystole | 1 (4.2) | 2 (5.9) | ||
| PEA | 3 (12.5) | 4 (11.8) | ||
| Prehospital ROSC | 15 (62.5) | 27 (79.4) | ||
| Rhythm (After ROSC), frequency (%) | 0.329 | |||
| Sinus Rhythm | 8 (33.3) | 15 (44.1) | ||
| Sinus Tachycardia | 5 (20.8) | 10 (29.4) | ||
| Atrial Fibrillation | 7 (29.2) | 4 (11.8) | ||
| Accelerated Junctional Rhythm | 3 (12.5) | 1 (2.9) | ||
| Atrial Flutter | 0 (0.0) | 1 (2.9) | ||
| Escape Bradycardia | 1 (4.2) | 0 (0.0) | ||
| Escape Capture Bigeminy | 0 (0.0) | 1 (2.9) | ||
| Supraventricular Tachycardia | 0 (0.0) | 1 (2.9) | ||
| Ventricular Bigeminy | 0 (0.0) | 1 (2.9) | ||
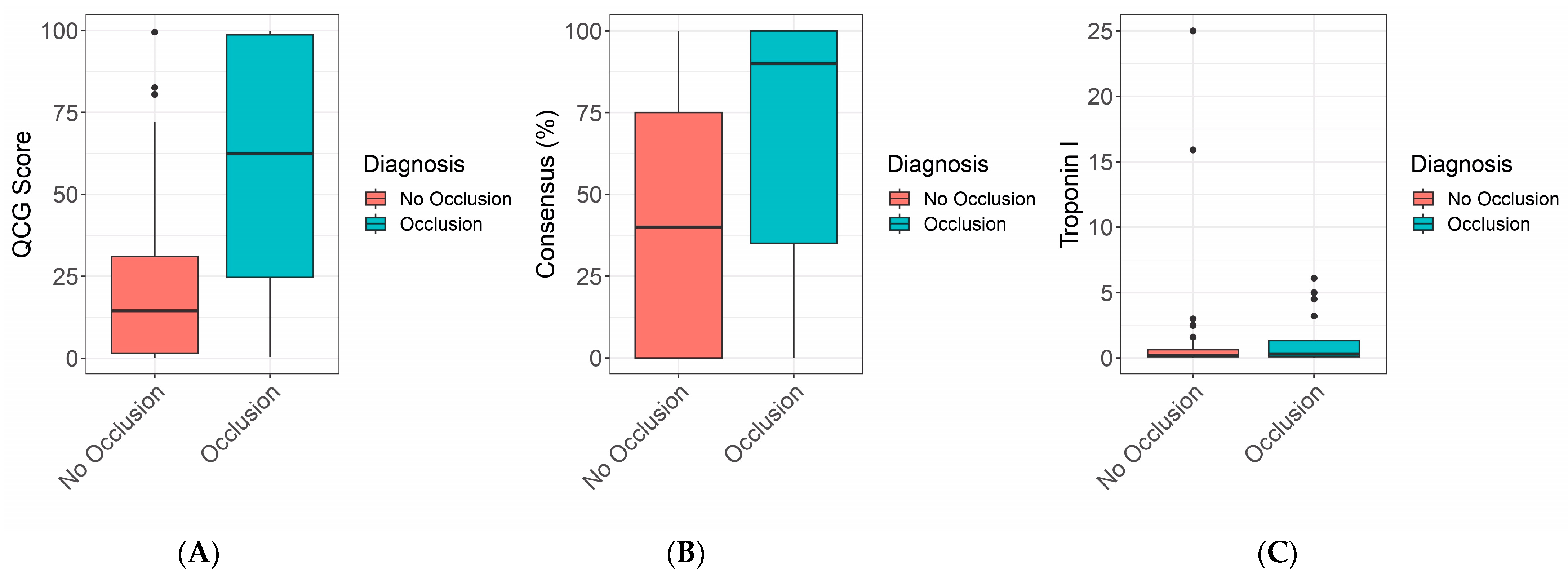
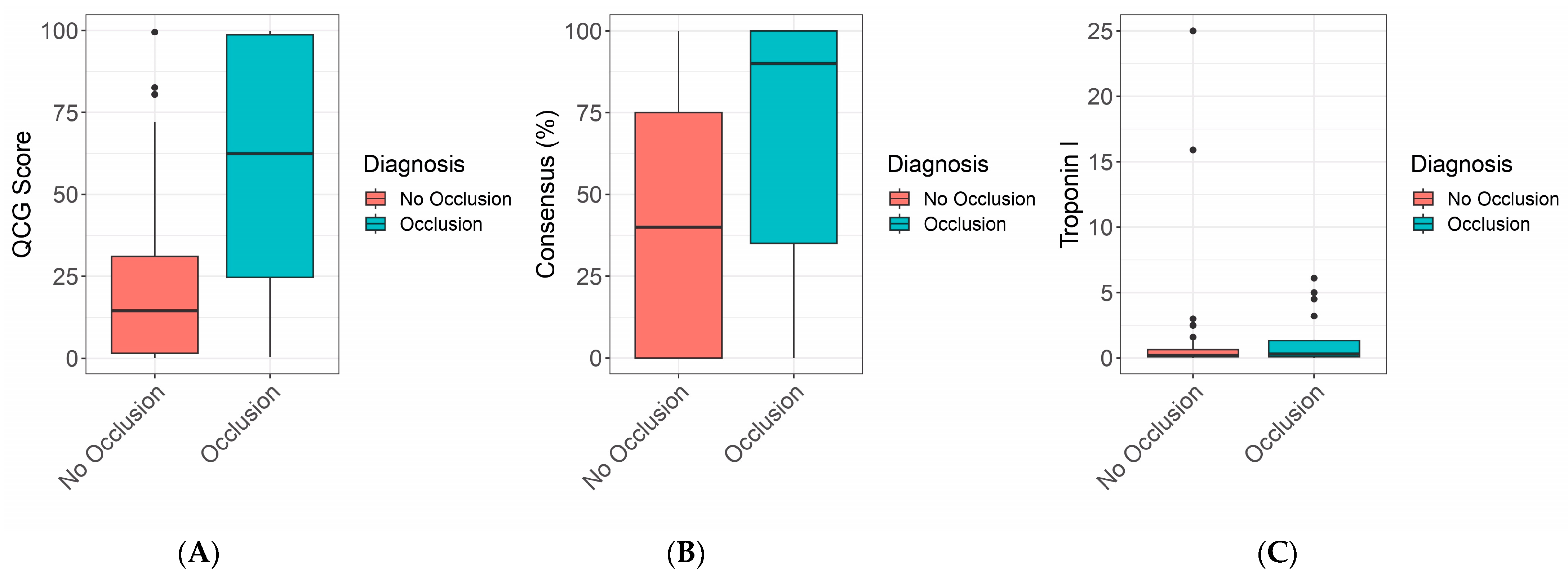
| Troponin I *, ng/mL, median (IQR) | 0.300 (0.100–1.350) | 0.200 (0.100–0.700) | 0.381 | |
| QCG, median (IQR) | 0.625 (0.208–0.988) | 0.145 (0.015–0.320) | 0.001 | |
| Consensus Score, median (IQR) | 0.9 (0.3–1.0) | 0.4 (0.0–0.8) | 0.2 | |
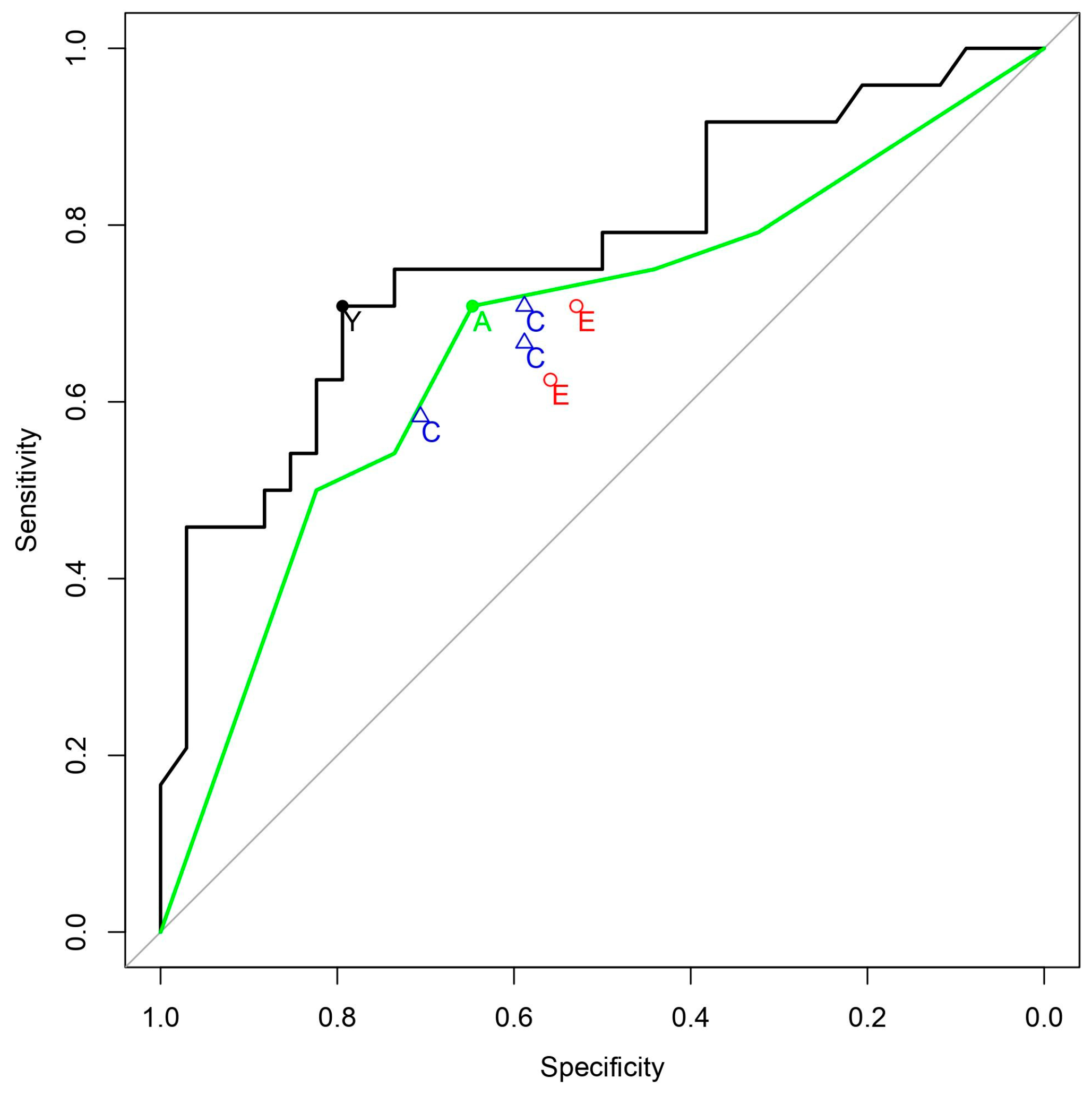
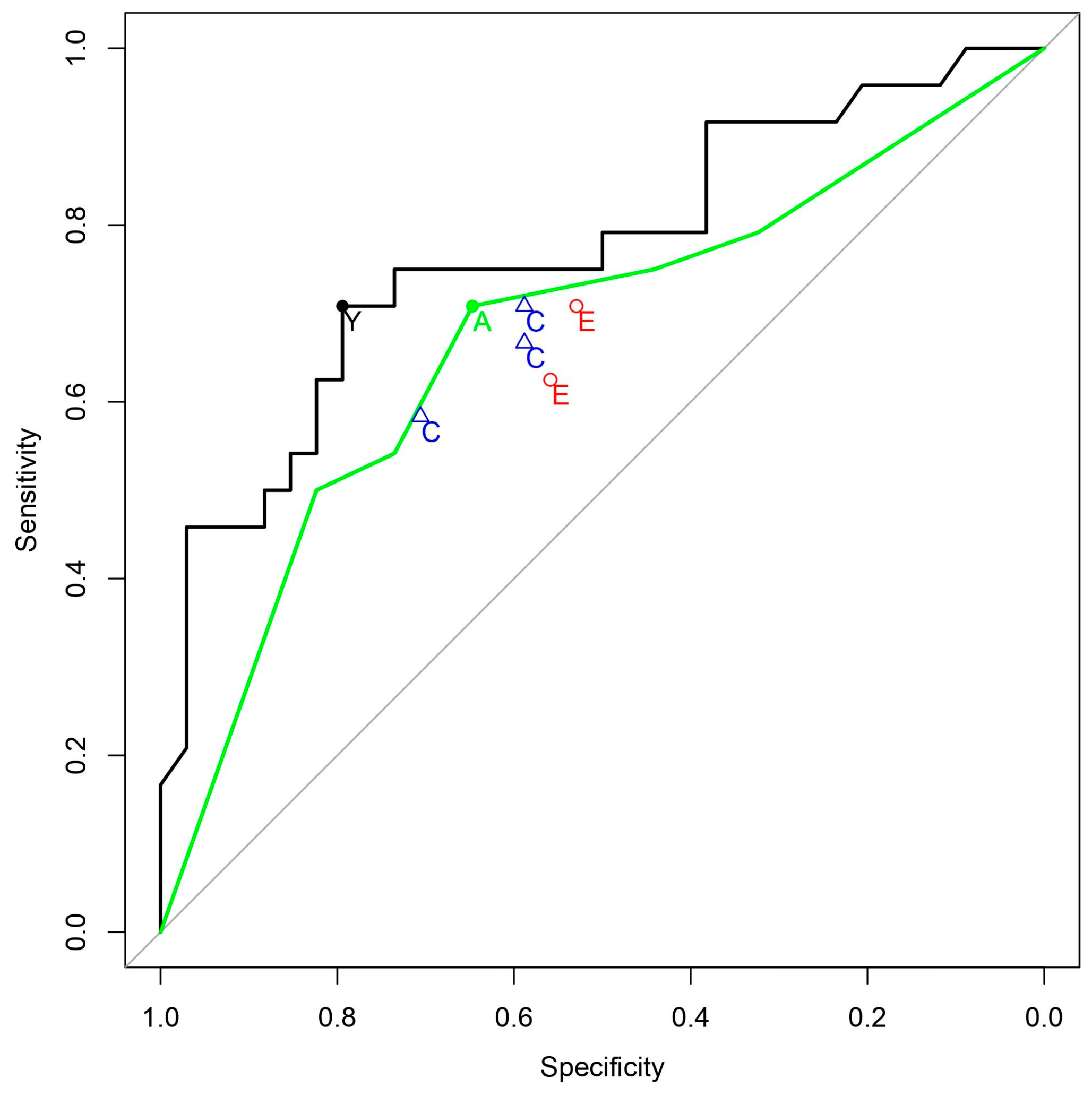
| AUC (95% CI) | Threshold | Sensitivity (95% CI) | Specificity (95% CI) | PLR (95% CI) | NLR (95% CI) | PPV (95% CI) | NPV (95% CI) | |
|---|---|---|---|---|---|---|---|---|
| QCG | 0.770 | 0.376 | 70.8 | 79.4 | 3.44 | 0.37 | 70.8 | 79.4 |
| (0.641–0.900) | (48.9–87.4) | (62.1–91.3) | (1.69–6.99 | (0.19–0.70 | (54.5–83.1) | (66.9–88.0) | ||
| Consensus * | 0.676 | 0.500 | 70.8 | 64.7 | 2.01 | 0.45 | 58.6 | 75.9 |
| (0.532–0.820) | (48.9–87.4) | (46.5–80.3) | (1.19–3.38) | (0.23–0.88) | (45.7–70.5) | (61.6–86.0) | ||
| EP#1 | 0.619 | - | 70.8 | 52.9 | 1.51 | 0.55 | 51.5 | 72.0 |
| (0.493–0.745) | (48.9–87.4) | (35.1–70.2) | (0.97–2.34) | (0.27–1.11) | (40.6–62.3) | (56.1–83.8) | ||
| EP#2 | 0.592 | - | 62.5 | 55.9 | 1.42 | 0.67 | 50.0 | 67.9 |
| (0.462–0.722) | (40.6–81.2) | (37.9–72.8) | (0.87–2.31) | (0.37–1.22) | (38.0–62.0) | (53.8–79.3) | ||
| CA#1 | 0.645 | - | 58.3 | 70.6 | 1.98 | 0.59 | 58.3 | 70.6 |
| (0.517–0.772) | (36.6–77.9) | (52.5–84.9) | (1.07–3.69) | (0.35–0.99) | (42.9–72.3) | (58.8–80.2) | ||
| CA#2 | 0.648 | - | 70.8 | 58.8 | 1.72 | 0.50 | 54.8 | 74.1 |
| (0.523–0.773) | (48.9–87.4) | (40.7–75.4) | (1.07–2.77) | (0.25–0.98) | (43.0–66.2) | (59.1–85.0) | ||
| CA#3 | 0.627 | - | 66.7 | 58.8 | 1.62 | 0.57 | 53.3 | 71.4 |
| (0.500–0.755) | (44.7–84.4) | (40.7–75.4) | (0.99–2.65) | (0.30–1.07) | (41.2–65.1) | (57.1–82.5) |
| Non-Inferiority Margin | Difference | 95% CI | Non-Inferiority |
|---|---|---|---|
| −0.05 | 0.094 | −0.017 to 0.205 | Confirmed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.J.; Choi, Y.J.; Shim, M.; Cho, Y.; Park, J.; Choi, J.; Kim, J.; Lee, E.; Kim, S.-Y. Performance of ECG-Derived Digital Biomarker for Screening Coronary Occlusion in Resuscitated Out-of-Hospital Cardiac Arrest Patients: A Comparative Study between Artificial Intelligence and a Group of Experts. J. Clin. Med. 2024, 13, 1354. https://doi.org/10.3390/jcm13051354
Park MJ, Choi YJ, Shim M, Cho Y, Park J, Choi J, Kim J, Lee E, Kim S-Y. Performance of ECG-Derived Digital Biomarker for Screening Coronary Occlusion in Resuscitated Out-of-Hospital Cardiac Arrest Patients: A Comparative Study between Artificial Intelligence and a Group of Experts. Journal of Clinical Medicine. 2024; 13(5):1354. https://doi.org/10.3390/jcm13051354
Chicago/Turabian StylePark, Min Ji, Yoo Jin Choi, Moonki Shim, Youngjin Cho, Jiesuck Park, Jina Choi, Joonghee Kim, Eunkyoung Lee, and Seo-Yoon Kim. 2024. "Performance of ECG-Derived Digital Biomarker for Screening Coronary Occlusion in Resuscitated Out-of-Hospital Cardiac Arrest Patients: A Comparative Study between Artificial Intelligence and a Group of Experts" Journal of Clinical Medicine 13, no. 5: 1354. https://doi.org/10.3390/jcm13051354
APA StylePark, M. J., Choi, Y. J., Shim, M., Cho, Y., Park, J., Choi, J., Kim, J., Lee, E., & Kim, S.-Y. (2024). Performance of ECG-Derived Digital Biomarker for Screening Coronary Occlusion in Resuscitated Out-of-Hospital Cardiac Arrest Patients: A Comparative Study between Artificial Intelligence and a Group of Experts. Journal of Clinical Medicine, 13(5), 1354. https://doi.org/10.3390/jcm13051354