
A Narrative Review on Robotic Surgery as Treatment for Renal Cell Carcinoma with Inferior Vena Cava Thrombus

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Methods
3. Results and Discussion
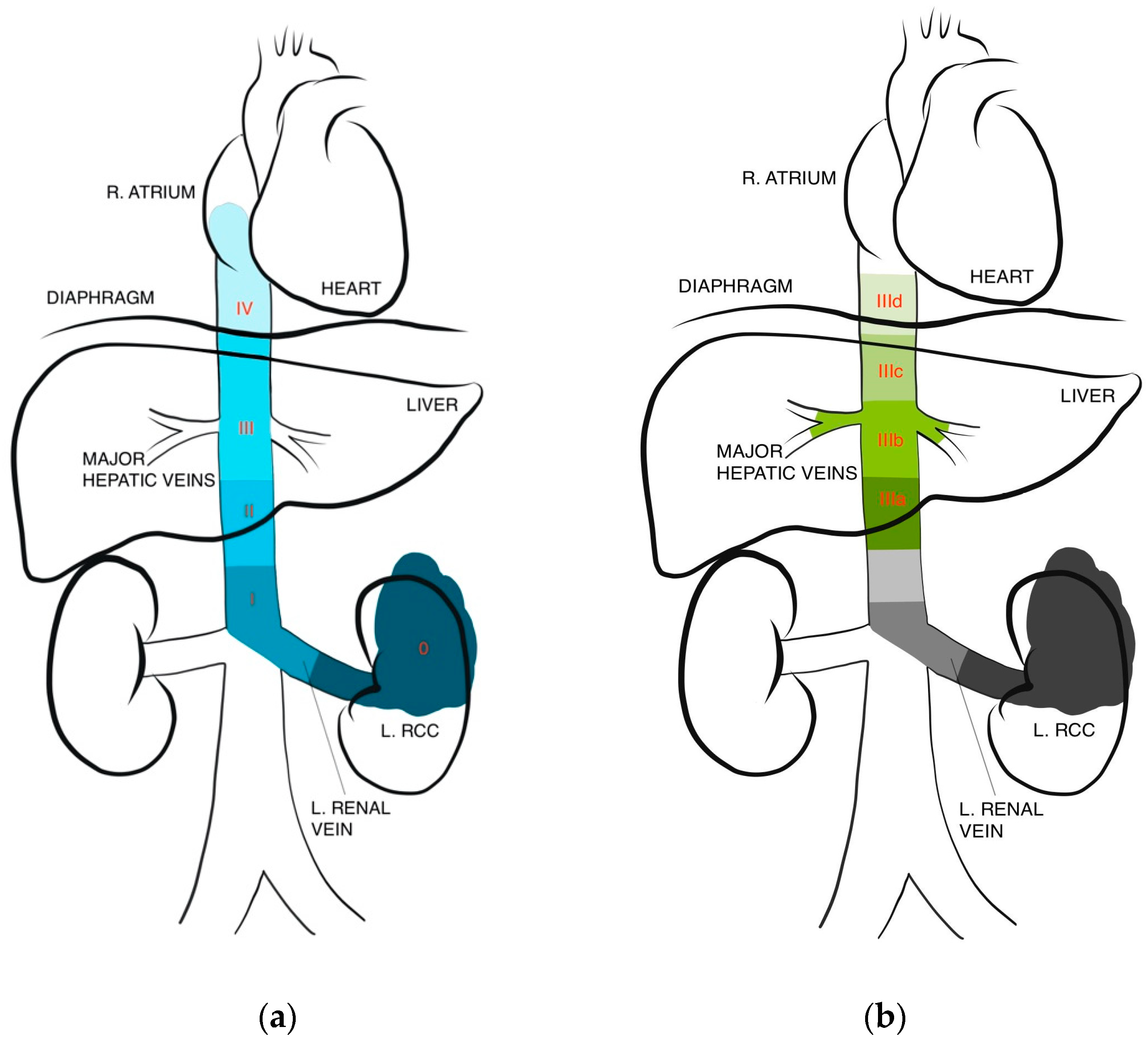
3.1. IVC Level Thrombus Classifications
3.2. Surgical Techniques
3.3. Right-Sided Tumor
3.4. Left-Sided Tumor
3.5. Case Reports and Studies for Level I and II
3.6. Case Reports and Studies for Level III
3.7. Case Reports and Studies for Level IV
3.8. Preoperative Evaluation
3.9. Preoperative Renal Artery Embolization
3.10. Multidisciplinary Team
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Key Statistics about Kidney Cancer; American Cancer Society: Atlanta, GA, USA, 2023. [Google Scholar]
- Chen, Z.; Yang, F.; Ge, L.; Qiu, M.; Liu, Z.; Liu, C.; Tian, X.; Zhang, S.; Ma, L. Outcomes of renal cell carcinoma with associated venous tumor thrombus: Experience from a large cohort and short time span in a single center. BMC Cancer 2021, 21, 766. [Google Scholar] [CrossRef]
- Laguna, M.P.; Algaba, F.; Cadeddu, J.; Clayman, R.; Gill, I.; Gueglio, G.; Hohenfellner, M.; Joyce, A.; Landman, J.; Lee, B.; et al. Current patterns of presentation and treatment of renal masses: A clinical research office of the endourological society prospective study. J. Endourol. 2014, 28, 861–870. [Google Scholar] [CrossRef]
- Ciancio, G.; Manoharan, M.; Katkoori, D.; Santos, R.D.L.; Soloway, M.S. Long-term survival in patients undergoing radical nephrectomy and inferior vena cava thrombectomy: Single-center experience. Eur. Urol. 2010, 57, 667–672. [Google Scholar] [CrossRef]
- Nouh, M.A.A.-M.; Inui, M.; Kakehi, Y. Renal Cell Carcinoma with IVC Thrombi; Current Concepts and Future Perspectives. Clin. Med. Insights Oncol. 2008, 2, 247–256. [Google Scholar] [CrossRef]
- European Association of Urology. EAU Guidelines on Renal Cell Carcinnoma. 2023. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Renal-Cell-Carcinoma-2023.pdf (accessed on 15 February 2023).
- National Comprehensive Cancer Network. Kidney Cancer (Version 4.2023). 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf (accessed on 15 February 2023).
- Chan, V.W.; Tan, W.S.; Leow, J.J.; Tan, W.P.; Ong, W.L.; Chiu, P.K.; Gurung, P.; Pirola, G.M.; Orecchia, L.; Liew, M.P.; et al. Delayed surgery for localised and metastatic renal cell carcinoma: A systematic review and meta-analysis for the COVID-19 pandemic. World J. Urol. 2021, 39, 4295–4303. [Google Scholar] [CrossRef]
- Vergho, D.C.; Loeser, A.; Kocot, A.; Spahn, M.; Riedmiller, H. Tumor thrombus of inferior vena cava in patients with renal cell carcinoma—Clinical and oncological outcome of 50 patients after surgery. BMC Res. Notes 2012, 5, 264. [Google Scholar] [CrossRef]
- Niedworok, C.; Dörrenhaus, B.; Dorp, F.V.; Piotrowski, J.A.; Tschirdewahn, S.; Szarvas, T.; Rübben, H.; Schenck, M. Renal cell carcinoma and tumour thrombus in the inferior vena cava: Clinical outcome of 98 consecutive patients and the prognostic value of preoperative parameters. World J. Urol. 2015, 33, 1541–1552. [Google Scholar] [CrossRef]
- Nesbitt, J.C.; Soltero, E.R.; Dinney, C.P.; Walsh, G.L.; Schrump, D.S.; A Swanson, D.; Pisters, L.L.; Willis, K.D.; Putnam, J.B. Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Ann. Thorac. Surg. 1997, 63, 1592–1600. [Google Scholar] [CrossRef]
- Skinner, D.G.; Pritchett, T.R.; Lieskovsky, G.; Boyd, S.D.; Stiles, Q.R. Vena caval involvement by renal cell carcinoma. Surgical resection provides meaningful long-term survival. Ann. Surg. 1989, 210, 387–394. [Google Scholar] [CrossRef]
- Hatcher, P.A.; Anderson, E.E.; Paulson, D.F.; Carson, C.C.; Robertson, J.E. Surgical Management and Prognosis of Renal Cell carcinoma Invading the Vena Cava. J. Urol. 1991, 145, 20–23. [Google Scholar] [CrossRef]
- Skinner, D.G.; Pfister, R.F.; Colvin, R. Extension of renal cell carcinoma into the vena cava: The rationale for aggressive surgical management. J. Urol. 1972, 107, 711–716. [Google Scholar] [CrossRef]
- Faegh, A.; Moeinafshar, A.; Rezaei, N. Nephrectomy and IVC thrombectomy in renal cancer: A narrative review. Clin. Transl. Oncol. 2023, 26, 574–583. [Google Scholar] [CrossRef]
- Clayman, R.V.; Kavoussi, L.R.; Soper, N.J.; Dierks, S.M.; Meretyk, S.; Darcy, M.D.; Roemer, F.D.; Pingleton, E.D.; Thomson, P.G.; Long, S.R. Laparoscopic Nephrectomy: Initial Case Report. J. Urol. 1991, 146, 278–282. [Google Scholar] [CrossRef]
- Abaza, R. Initial series of robotic radical nephrectomy with vena caval tumor thrombectomy. Eur. Urol. 2011, 59, 652–656. [Google Scholar] [CrossRef]
- Ma, S.; Jia, W.; Hou, G.; Quan, P.; Zhang, L.; Fan, X.; Yang, B.; Su, X.; Jiao, J.; Wang, F.; et al. Case reports of robot-assisted laparoscopic radical nephrectomy and inferior vena cava tumor thrombectomy: A retrospective analysis. Medicine 2021, 100, e26886. [Google Scholar] [CrossRef]
- Zhang, Y.; Bi, H.; Yan, Y.; Liu, Z.; Wang, G.; Song, Y.; Zhang, S.; Liu, C.; Ma, L. Comparative analysis of surgical and oncologic outcomes of robotic, laparoscopic and open radical nephrectomy with venous thrombectomy: A propensity-matched cohort study. Int. J. Clin. Oncol. 2023, 28, 145–154. [Google Scholar] [CrossRef]
- Jurado, A.; Romeo, A.; Gueglio, G.; Marchiñena, P.G. Current Trends in Management of Renal Cell Carcinoma with Venous Thrombus Extension. Curr. Urol. Rep. 2021, 22, 23. [Google Scholar] [CrossRef]
- Neves, R.; Zincke, H. Surgical treatment of renal cancer with vena cava extension. BJU Int. 1987, 59, 390–395. [Google Scholar] [CrossRef]
- Ciancio, G.; Vaidya, A.; Savoie, M.; Soloway, M. Management of renal cell carcinoma with level iii thrombus in the inferior vena cava. J. Urol. 2002, 168, 1374–1377. [Google Scholar] [CrossRef]
- Blute, M.L.; Leibovich, B.C.; Lohse, C.M.; Cheville, J.C.; Zincke, H. The Mayo Clinic experience with surgical management, complications and outcome for patients with renal cell carcinoma and venous tumour thrombus. BJU Int. 2004, 94, 33–41. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, Q.; Zhao, X.; Zhu, G.; Tang, S.; Hong, P.; Ge, L.; Zhang, S.; Wang, G.; Tian, X.; et al. Inferior vena cava interruption in renal cell carcinoma with tumor thrombus: Surgical strategy and perioperative results. BMC Surg. 2021, 21, 402. [Google Scholar] [CrossRef]
- Almatari, A.L.; Sathe, A.; Wideman, L.; Dewan, C.A.; Vaughan, J.P.; Bennie, I.C.; Buscarini, M. Renal cell carcinoma with tumor thrombus: A review of relevant anatomy and surgical techniques for the general urologist. Urol. Oncol. Semin. Orig. Investig. 2023, 41, 153–165. [Google Scholar] [CrossRef]
- Psutka, S.P.; Leibovich, B.C. Management of inferior vena cava tumor thrombus in locally advanced renal cell carcinoma. Ther. Adv. Urol. 2015, 7, 216–229. [Google Scholar] [CrossRef]
- Garg, H.; Psutka, S.P.; Hakimi, A.A.; Kim, H.L.; Mansour, A.M.; Pruthi, D.K.; Liss, M.A.; Wang, H.; Gaspard, C.S.; Ramamurthy, C.; et al. A Decade of Robotic-Assisted Radical Nephrectomy with Inferior Vena Cava Thrombectomy: A Systematic Review and Meta-Analysis of Perioperative Outcomes. J. Urol. 2022, 208, 542–560. [Google Scholar] [CrossRef]
- Hevia, V.; Ciancio, G.; Gómez, V.; Álvarez, S.; Díez-Nicolás, V.; Burgos, F.J. Surgical technique for the treatment of renal cell carcinoma with inferior vena cava tumor thrombus: Tips, tricks and oncological results. SpringerPlus 2016, 5, 132. [Google Scholar] [CrossRef]
- Gill, I.S.; Metcalfe, C.; Abreu, A.; Duddalwar, V.; Chopra, S.; Cunningham, M.; Thangathurai, D.; Ukimura, O.; Satkunasivam, R.; Hung, A.; et al. Robotic Level III Inferior Vena Cava Tumor Thrombectomy: Initial Series. J. Urol. 2015, 194, 929–938. [Google Scholar] [CrossRef]
- Shen, D.; Du, S.; Huang, Q.; Gao, Y.; Fan, Y.; Gu, L.; Liu, K.; Peng, C.; Xuan, Y.; Li, P.; et al. A modified sequential vascular control strategy in robot-assisted level III–IV inferior vena cava thrombectomy: Initial series mimicking the open ‘milking’ technique principle. BJU Int. 2020, 126, 447–456. [Google Scholar] [CrossRef]
- Duty, B.; Daneshmand, S. Venous Resection in Urological Surgery. J. Urol. 2008, 180, 2338–2342. [Google Scholar] [CrossRef]
- Masic, S.; Smaldone, M.C. Robotic renal surgery for renal cell carcinoma with inferior vena cava thrombus. Transl. Androl. Urol. 2021, 10, 2195–2198. [Google Scholar] [CrossRef]
- Aghazadeh, M.A.; Goh, A.C. Robotic Left-sided Level II Caval Thrombectomy and Nephrectomy Using a Novel Supine, Single-dock Approach: Primary Description. Urology 2018, 112, 205–208. [Google Scholar] [CrossRef]
- Du, S.; Huang, Q.; Yu, H.; Shen, D.; Gu, L.; Yan, F.; Liu, F.; Zhang, X.; Ma, X.; Wang, B. Initial Series of Robotic Segmental Inferior Vena Cava Resection in Left Renal Cell Carcinoma With Caval Tumor Thrombus. Urology 2020, 142, 125–132. [Google Scholar] [CrossRef]
- Wang, B.; Li, H.; Ma, X.; Zhang, X.; Gu, L.; Li, X.; Fan, Y.; Gao, Y.; Liu, K.; Zhu, J. Robot-assisted Laparoscopic Inferior Vena Cava Thrombectomy: Different Sides Require Different Techniques. Eur. Urol. 2016, 69, 1112–1119. [Google Scholar] [CrossRef]
- Shi, T.; Huang, Q.; Liu, K.; Du, S.; Fan, Y.; Yang, L.; Peng, C.; Shen, D.; Wang, Z.; Gao, Y.; et al. Robot-assisted Cavectomy Versus Thrombectomy for Level II Inferior Vena Cava Thrombus: Decision-making Scheme and Multi-institutional Analysis. Eur. Urol. 2020, 78, 592–602. [Google Scholar] [CrossRef]
- Motoyama, D.; Ito, T.; Sugiyama, T.; Otsuka, A.; Miyake, H. Robot-assisted radical nephrectomy and inferior vena cava tumor thrombectomy: Initial experience in Japan. IJU Case Rep. 2022, 5, 145–148. [Google Scholar] [CrossRef]
- Shao, P.; Li, J.; Qin, C.; Lv, Q.; Ju, X.; Li, P.; Shao, Y.; Ni, B.; Yin, C. Laparoscopic Radical Nephrectomy and Inferior Vena Cava Thrombectomy in the Treatment of Renal Cell Carcinoma. Eur. Urol. 2015, 68, 115–122. [Google Scholar] [CrossRef]
- Ramirez, D.; Maurice, M.J.; Cohen, B.; Krishnamurthi, V.; Haber, G.-P. Robotic Level III IVC Tumor Thrombectomy: Duplicating the Open Approach. Urology 2016, 90, 204–207. [Google Scholar] [CrossRef]
- Chopra, S.; Simone, G.; Metcalfe, C.; Abreu, A.L.d.C.; Nabhani, J.; Ferriero, M.; Bove, A.M.; Sotelo, R.; Aron, M.; Desai, M.M.; et al. Robot-assisted Level II–III Inferior Vena Cava Tumor Thrombectomy: Step-by-Step Technique and 1-Year Outcomes. Eur. Urol. 2017, 72, 267–274. [Google Scholar] [CrossRef]
- Djaladat, H.; Ghoreifi, A.; Basin, M.F.; Hugen, C.; Aslzare, M.; Miranda, G.; Hwang, D.H.; Schuckman, A.K.; Aron, M.; Thangathurai, D.; et al. Perioperative Outcome of Suprarenal Resection of Vena Cava Without Reconstruction in Urologic Malignancies: A Case Series and Review of the Literature. Urology 2020, 142, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Palacios, A.R.; Schmeusser, B.N.; Midenberg, E.; Patil, D.; Xie, L.; Nabavizadeh, R.; Ogan, K.; Cardona, K.; Maithel, S.K.; Master, V.A. Resection of retroperitoneal tumors with inferior vena cava involvement without caval reconstruction. J. Surg. Oncol. 2022, 126, 1306–1315. [Google Scholar] [CrossRef] [PubMed]
- Grosso, A.A.; Di Maida, F.; Giudici, S.; Mari, A.; Muiesan, P.; Taddei, A.; Campi, R.; Minervini, A. Robotic surgery for renal tumors with inferior vena cava thrombosis: Indications and technical nuances. Urol. Video J. 2021, 13, 100111. [Google Scholar] [CrossRef]
- Wang, B.; Huang, Q.; Liu, K.; Fan, Y.; Peng, C.; Gu, L.; Shi, T.; Zhang, P.; Chen, W.; Du, S.; et al. Robot-assisted Level III-IV Inferior Vena Cava Thrombectomy: Initial Series with Step-by-step Procedures and 1-yr Outcomes. Eur. Urol. 2020, 78, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Gill, I.S.; E Cacciamani, G.; Duddalwar, V.; Thangathurai, D.; Cunningham, M. Renal cancer with extensive level IV intracardiac tumour thrombus removed by robot. Lancet 2020, 396, e88. [Google Scholar] [CrossRef] [PubMed]
- Palma-Zamora, I.; Dalela, D.; Barod, R.; Hsu, L.; Menon, M.; Rogers, C.G. Initial robotic assistance in the surgical management of renal cell carcinoma with level 4 cavoatrial thrombus. J. Robot. Surg. 2017, 12, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Bhat, K.R.S.; Moschovas, M.C.; Onol, F.F.; Rogers, T.; Roof, S.; Patel, V.R.; Schatloff, O. Robotic renal and adrenal oncologic surgery: A contemporary review. Asian J. Urol. 2020, 8, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Lawindy, S.M.; Kurian, T.; Kim, T.; Mangar, D.; Armstrong, P.A.; Alsina, A.E.; Sheffield, C.; Sexton, W.J.; Spiess, P.E. Important surgical considerations in the management of renal cell carcinoma (RCC) with inferior vena cava (IVC) tumour thrombus. BJU Int. 2012, 110, 926–939. [Google Scholar] [CrossRef] [PubMed]
- Gohji, K.; Yamashita, C.; Ueno, K.; Shimogaki, H.; Kamidono, S. Preoperative computerized tomography detection of extensive invasion of the inferior vena cava by renal cell carcinoma: Possible indication for resection with partial cardiopulmonary bypass and patch grafting. J. Urol. 1994, 152, 1993–1996. [Google Scholar] [CrossRef] [PubMed]
- Zini, L.; Destrieux-Garnier, L.; Leroy, X.; Villers, A.; Haulon, S.; Lemaitre, L.; Koussa, M. Renal vein ostium wall invasion of renal cell carcinoma with an inferior vena cava tumor thrombus: Prediction by renal and vena caval vein diameters and prognostic significance. J. Urol. 2008, 179, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Psutka, S.P.; Boorjian, S.A.; Thompson, R.H.; Schmit, G.D.; Schmitz, J.J.; Bower, T.C.; Stewart, S.B.; Lohse, C.M.; Cheville, J.C.; Leibovich, B.C. Clinical and radiographic predictors of the need for inferior vena cava resection during nephrectomy for patients with renal cell carcinoma and caval tumour thrombus. BJU Int. 2014, 116, 388–396. [Google Scholar] [CrossRef]
- Lawrentschuk, N.; Gani, J.; Riordan, R.; Esler, S.; Bolton, D.M. Multidetector computed tomography vs magnetic resonance imaging for defining the upper limit of tumour thrombus in renal cell carcinoma: A study and review. BJU Int. 2005, 96, 291–295. [Google Scholar] [CrossRef]
- Kallman, D.A.; King, B.F.; Hattery, R.R.; Charboneau, J.W.; Ehman, R.L.; Guthman, D.A.; Blute, M.L. Renal Vein and Inferior Vena Cava Tumor Thrombus in Renal Cell Carcinoma: CT, US, MRI, and Venacavography. J. Comput. Assist. Tomogr. 1992, 16, 240–247. [Google Scholar] [CrossRef]
- Hallscheidt, P.J.; Fink, C.; Haferkamp, A.; Bock, M.; Luburic, A.; Zuna, I.; Noeldge, G.; Kauffmann, G. Preoperative Staging of Renal Cell Carcinoma With Inferior Vena Cava Thrombus Using Multidetector CT and MRI. J. Comput. Assist. Tomogr. 2005, 29, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Nazim, S.M.; Ather, M.H.; Hafeez, K.; Salam, B. Accuracy of multidetector CT scans in staging of renal carcinoma. Int. J. Surg. 2011, 9, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.-F.; Song, Y.; Na, Y.-Q. Value of abdominal ultrasound scan, CT and MRI for diagnosing inferior vena cava tumour thrombus in renal cell carcinoma. Chin. Med. J. 2009, 122, 2299–2302. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Chen, X.; Wang, J.; He, W.; Niu, Z. Adjuvant instant preoperative renal artery embolization facilitates the radical nephrectomy and thrombectomy in locally advanced renal cancer with venous thrombus: A retrospective study of 54 cases. World J. Surg. Oncol. 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, H.; Szmigielski, S.; Petrovich, Z. Comparison of preoperative embolization followed by radical nephrectomy with radical nephrectomy alone for renal cell carcinoma. Am. J. Clin. Oncol. 2000, 23, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Bakke, A.; Göthlin, J.H.; A Haukaas, S.; Kalland, T. Augmentation of natural killer cell activity after arterial embolization of renal carcinomas. Cancer Res. 1982, 42, 3880–3883. [Google Scholar]
- Kato, T.; Sato, K.; Abe, R.; Moriyama, M. The role of embolization/chemoembolization in the treatment of renal cell carcinoma. Prog. Clin. Biol. Res. 1989, 303, 697–705. [Google Scholar]
- Nakano, H.; Nihira, H.; Toge, T. Treatment of renal cancer patients by transcatheter embolization and its effects on lymphocyte proliferative responses. J. Urol. 1983, 130, 24–27. [Google Scholar] [CrossRef]
- Schwartz, M.J.; Smith, E.B.; Trost, D.W.; Vaughan, E.D. Renal artery embolization: Clinical indications and experience from over 100 cases. BJU Int. 2006, 99, 881–886. [Google Scholar] [CrossRef] [PubMed]
- May, M.; Brookman-Amissah, S.; Pflanz, S.; Roigas, J.; Hoschke, B.; Kendel, F. Pre-operative renal arterial embolisation does not provide survival benefit in patients with radical nephrectomy for renal cell carcinoma. Br. J. Radiol. 2009, 82, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.S.; Stephenson, A.J.; Goldfarb, D.A.; Fergany, A.F.; Novick, A.C.; Krishnamurthi, V. Utility of preoperative renal artery embolization for management of renal tumors with inferior vena caval thrombi. Urology 2009, 74, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Gayed, B.A.; Youssef, R.; Darwish, O.; Kapur, P.; Bagrodia, A.; Brugarolas, J.; Raj, G.; DiMaio, J.M.; Sagalowsky, A.; Margulis, V. Multi-disciplinary surgical approach to the management of patients with renal cell carcinoma with venous tumor thrombus: 15 year experience and lessons learned. BMC Urol. 2016, 16, 43. [Google Scholar] [CrossRef] [PubMed]
- Master, V.A.; Ethun, C.G.; Kooby, D.A.; Staley, C.A.; Maithel, S.K. The value of a cross-discipline team-based approach for resection of renal cell carcinoma with IVC tumor thrombus: A report of a large, contemporary, single-institution experience. J. Surg. Oncol. 2018, 118, 1219–1226. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Items | Specification |
|---|---|
| Date of search (specified to date, month, and year | 18 January 2023–15 February 2023 |
| Databases and other sources searched | Pubmed, Thomas Jefferson University library system |
| Search terms used (including MeSH and free text search terms and filters) Note: please use an independent supplement table to present detailed search strategy of one database as an example | “Renal cell carcinoma”, “IVC thrombus”, “Thrombus level”, “Robotic surgery”, “Minimally invasive”, “Laparoscopic surgery”, “IVC thrombus level classification”, “Surgical techniques” |
| Timeframe | To present |
| Inclusion and exclusion criteria (study type, language restrictions, etc.) | English language, all study types |
| Selection process (who conducted the selection, whether it was conducted independently, how consensus was obtained, etc.) | KW, YS, RR searched for literature independently; papers were shared and reviewed by all to reach consensus for inclusion |
| Any additional considerations, if applicable |
| Level | Description | Surgical Approach |
|---|---|---|
| 0 | Limited to renal vein | Renal vein ligation |
| I | In the renal vein, <2 cm above renal vein | Tumor can be milked into the renal vein, clamp renal vein |
| II | >2 cm above renal vein, below hepatic veins | Rummel tourniquet or clamps on, clamping of intrahepatic IVC just below major hepatic veins |
| III | Above hepatic veins | Requires mobilization of the liver, intraoperative transesophageal electrocardiography, potential clamping of the hepatic veins and cardiopulmonary or venovenous bypass, clamping of suprahepatic IVC |
| IIIa | Retrohepatic IVC but below hepatic veins | |
| IIIb | Retrohepatic IVC reaching the hepatic veins, may extend into hepatic veins | |
| IIIc | Suprahepatic but subdiaphragmatic | |
| IIId | Supradiaphragmatic | |
| IV | Into the right atrium | Thoracic and abdominal approach, involves cardiothoracic surgery, cardiopulmonary bypass, and circulatory arrest |
| Author/Year | Thrombus Level: N | Side | Approach | Operation Time (min) Mean/Median (Range) | Blood Loss (mL) Mean/Median (Range) | Hospital Stay (Days) Mean/Median (Range) | Complication Rate | Other Findings |
|---|---|---|---|---|---|---|---|---|
| Abaza 2011 [17] | I: 5 | Right | Left lateral decubitus position at 90° | 327 (240–411) | 170 (50–400 | 1.2 (1–2) | 0 | All patients managed with oral pain control and ketorolac; no IV narcotics No recurrence of disease at a mean 15.4 month follow up |
| Motoyama 2021 [37] | I: 1 | Right | Transperitoneal | 211 | 150 | 5 | 0 | |
| Wang 2016 [35] | I: 4 II: 13 | Right: 13 Left: 4 | Left lateral decubitus position with 70° bump | Right: 131 (100–150) Left: 250 (190–275) | 240 (145–320) | 5.2 (4–6) | 2 out of 17 grade II—postoperative hypoproteinemia with lymphatic leakage grade IV—bleeding from tributaries of IVC | IVC clamping time: 17 min (12–25 min) No recurrence or tumor emboli infringement at IVC at mean 14 month follow up Left RCC: Right-side warm ischemic time 18 min (14–22 min) |
| Aghazadeh and Goh 2018 [33] | II: 1 | Left | Supine Single dock Switch camera ports between thrombectomy and nephrectomy | 420 | 500 | 5 | grade I—acute on chronic renal failure | IVC clamping time: 27 min No recurrence of disease at 12 mos No renal artery embolization or repositioning for a L-sided RCC |
| Du 2020 [34] | II: 5 III: 6 | Left | 30–45° dorsal elevated lithotomy | 420 | 1700 | 3 ICU 6 total | 4 Clavien grade II in 2 patients—lower extremity edema, diuretics required | First segmental IVC resection without caval replacement or shunt reconstruction |
| Shao 2015 [38] | II: 6 | Right | Left lateral decubitus position | 155 (135–210) | 271 (150–510) | 9 | 2 patients with grade I–II complications | IVC clamping time: 16.5 min (13–20 min) No recurrence of disease at a mean 32.5 mo (16–52 mos) follow up |
| Shi 2020 [36] | II: 90 | R: 65 L: 25 | Information not available | Thrombectomy: 190 Cavectomy: 268 | Thrombectomy: 400 (200–1000) Cavectomy: 1500 (970–2000) | Thrombectomy: 12/60 required intraoperative blood transfusion grade I–II Cavectomy: 23/30 required intraoperative blood transfusion, 2 grade II—bleeding from spleen injury and fistula from intestinal injury, both requiring reoperation | Compared thrombectomies to cavectomies At mean 18 mo (1–75 mos) follow up, thrombectomy: new metastases in 17/60 patients and 6 deaths; cavectomy: new metastases in 19/30 patients and 13 deaths |
| Author/Year | Thrombus Level: N | Side | Approach | Operation Time (min) Mean/Median (Range) | Blood Loss (mL) Mean/Median (Range) | Hospital Stay (Days) Mean/Median (Range) | Complication Rate | Other Findings |
|---|---|---|---|---|---|---|---|---|
| Chopra 2017 [40] | II: 13 III: 11 | R:17 L: 7 | 75° lateral decubitus position with table fully flexed R: whole procedure with right side up L: right side up first for thrombectomy, then repositioned left side up for rest of procedure | 270 (180–480) | 240 (100–7000) | 4 (1–22) | 5 received intraoperative transfusions 2 grade II—DVT, PE 1 grade IIIa—chylous ascites 1 grade IIIb—subphrenic abscess | “IVC first, kidney last” technique with minimal IVC touch 3 patients had positive lymph nodes At median follow up 16 mo (12–39 mos), all patients were alive; 11 had new-onset metastatic disease; 10 received adjuvant therapy |
| Gill 2015 [29] | III: 9 | R: 6 L: 3 | R: Right side up, 60° lateral position L: Right side up first for thrombectomy, then repositioned left side up for nephrectomy and lymphadenopathy | 306 (270–378) | 493 (200–7000) | 6.8 (2–10) | 1 grade IIIb—subphrenic abscess 3 required intraoperative transfusion | No evidence of disease or progression at median follow up 7 mo (1–18 mos) |
| Grosso 2022 [43] | III: 1 | Left | Step 1: Right flank Step 2: Supine Step 3: Left flank | 600 | 400 | 6 | None | IVC clamping time: 15 min |
| Ramirez 2016 [39] | III: 1 | Right | Modified left lateral decubitus position with 60° table flexion at the anterior superior iliac spine | 353 | 150 | 3 | None | IVC clamping time: 39 min |
| Wang 2020 [44] | III: 7 Plus 1 level IV treated like a level III | R: 3 L: 4 | 30–45° dorsal elevated lithotomy for liver mobilization Repositioned to left lateral decubitus position with 70° bump for thrombectomy | 430 (355–550) | 1100 (800–2600) | 11.3 ± 1.9 | 1 grade I 1 grade II 1 grade IV 7/8 (87.5%) required transfusion | 1 progression of metastases at median follow up 18 mo (12–37 mos) Included one case of urothelial carcinoma on postoperative histology |
| Author/Year | Thrombus Level: N | Side | Approach | Operation Time (min) Mean/Median (Range) | Blood Loss (mL) Mean/Median (Range) | Hospital Stay (Days) Mean/Median (Range) | Complication Rate | Other Findings |
|---|---|---|---|---|---|---|---|---|
| Gill 2020 [45] | IV: 1 | Right | 6 cm mini thoracotomy Anterograde-retrograde approach for thrombectomy CPB with hypothermic cardiac arrest | Information not available | Information not available | 6 | Information not available | Follow up 3.5 years later, on immunotherapy for lung metastases |
| Palma-Zamora 2018 [46] | IV: 1 | Left | Hybrid robotic + open procedure Modified left flank position to modified right flank position to supine CPB | 224 (robotic portion) | 200 (robotic portion) | Information not available | Information not available | “Minimal touch” technique to decrease risk of tumor thrombus dislodgement due to kidney and renal vein manipulation CPB time: 159 min Circulatory arrest time: 25 min Disease free at 18 mo follow up |
| Wang 2020 [44] | IV: 6 Exclude 1 level IV treated like a level III | Right | 30–45° dorsal elevated lithotomy for liver mobilization Repositioned to left lateral decubitus position with 70° bump for thrombectomy CPB 6 cm incision at 5th intercostal for thoracoscopy | 510 (338–653) | 2800 (1500–6500) | 15.4 ± 2.8 | 1 death POD 1 due to extensive 12,000 mL blood loss 3 grade II 2 grade IV All required transfusion | “Segmented thrombectomy” 1 case underwent “kidney first IVC last” technique CPB time: 72 min (51–87 min) Included one case of urothelial carcinoma on postoperative histology |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, M.S.; Wang, K.R.; Shah, Y.B.; Ragam, R.; Simhal, R.K.; Ghodoussipour, S.; Djaladat, H.; Mark, J.R.; Lallas, C.D.; Chandrasekar, T. A Narrative Review on Robotic Surgery as Treatment for Renal Cell Carcinoma with Inferior Vena Cava Thrombus. J. Clin. Med. 2024, 13, 1308. https://doi.org/10.3390/jcm13051308
Shah MS, Wang KR, Shah YB, Ragam R, Simhal RK, Ghodoussipour S, Djaladat H, Mark JR, Lallas CD, Chandrasekar T. A Narrative Review on Robotic Surgery as Treatment for Renal Cell Carcinoma with Inferior Vena Cava Thrombus. Journal of Clinical Medicine. 2024; 13(5):1308. https://doi.org/10.3390/jcm13051308
Chicago/Turabian StyleShah, Mihir S., Kerith R. Wang, Yash B. Shah, Radhika Ragam, Rishabh K. Simhal, Saum Ghodoussipour, Houman Djaladat, James R. Mark, Costas D. Lallas, and Thenappan Chandrasekar. 2024. "A Narrative Review on Robotic Surgery as Treatment for Renal Cell Carcinoma with Inferior Vena Cava Thrombus" Journal of Clinical Medicine 13, no. 5: 1308. https://doi.org/10.3390/jcm13051308
APA StyleShah, M. S., Wang, K. R., Shah, Y. B., Ragam, R., Simhal, R. K., Ghodoussipour, S., Djaladat, H., Mark, J. R., Lallas, C. D., & Chandrasekar, T. (2024). A Narrative Review on Robotic Surgery as Treatment for Renal Cell Carcinoma with Inferior Vena Cava Thrombus. Journal of Clinical Medicine, 13(5), 1308. https://doi.org/10.3390/jcm13051308