
Effects of High-Intensity Interval Training on Muscle Strength for the Prevention and Treatment of Sarcopenia in Older Adults: A Systematic Review of the Literature

 , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Eligibility Criteria
2.3. Information Sources and Search
2.4. Data Extraction
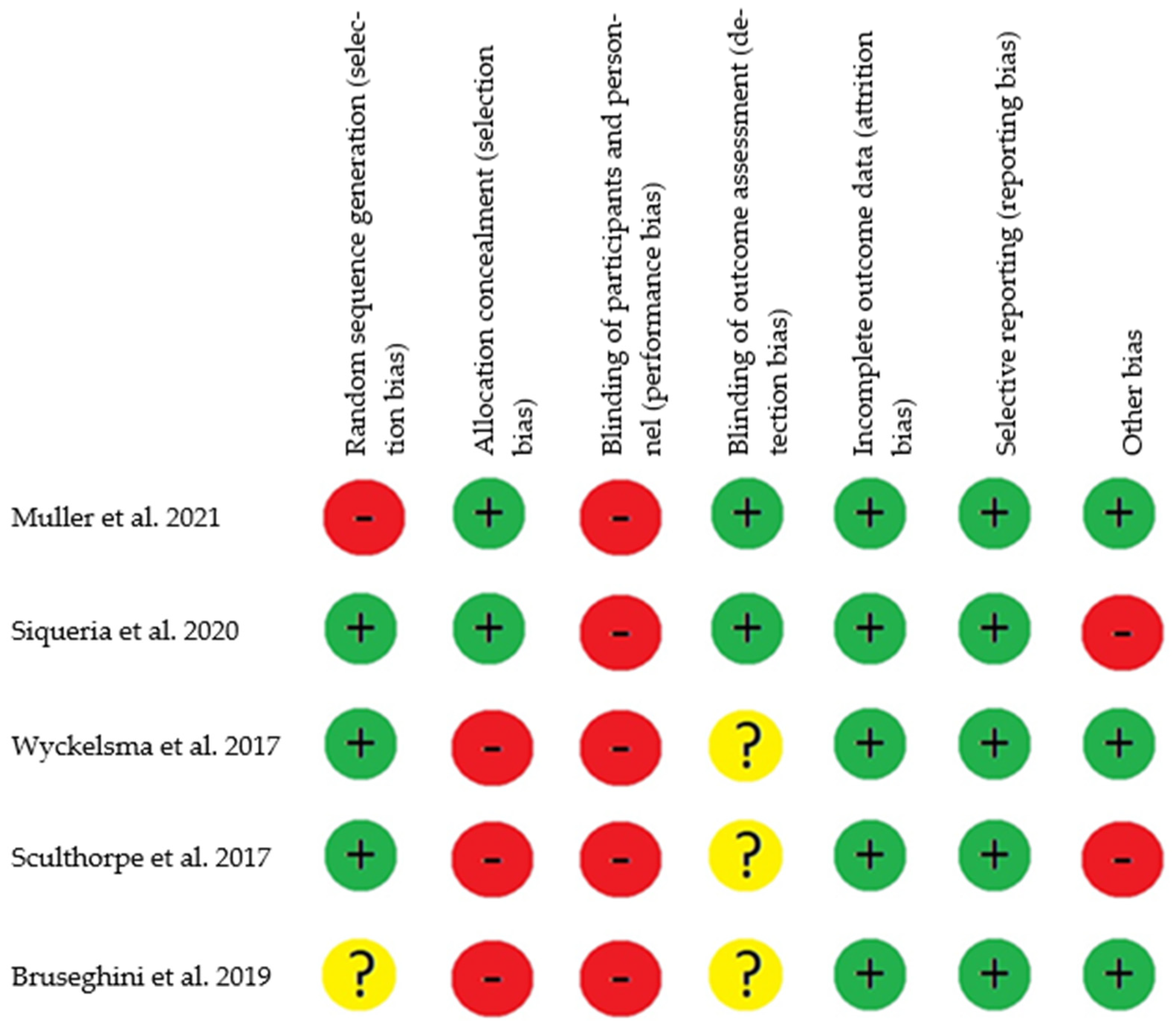
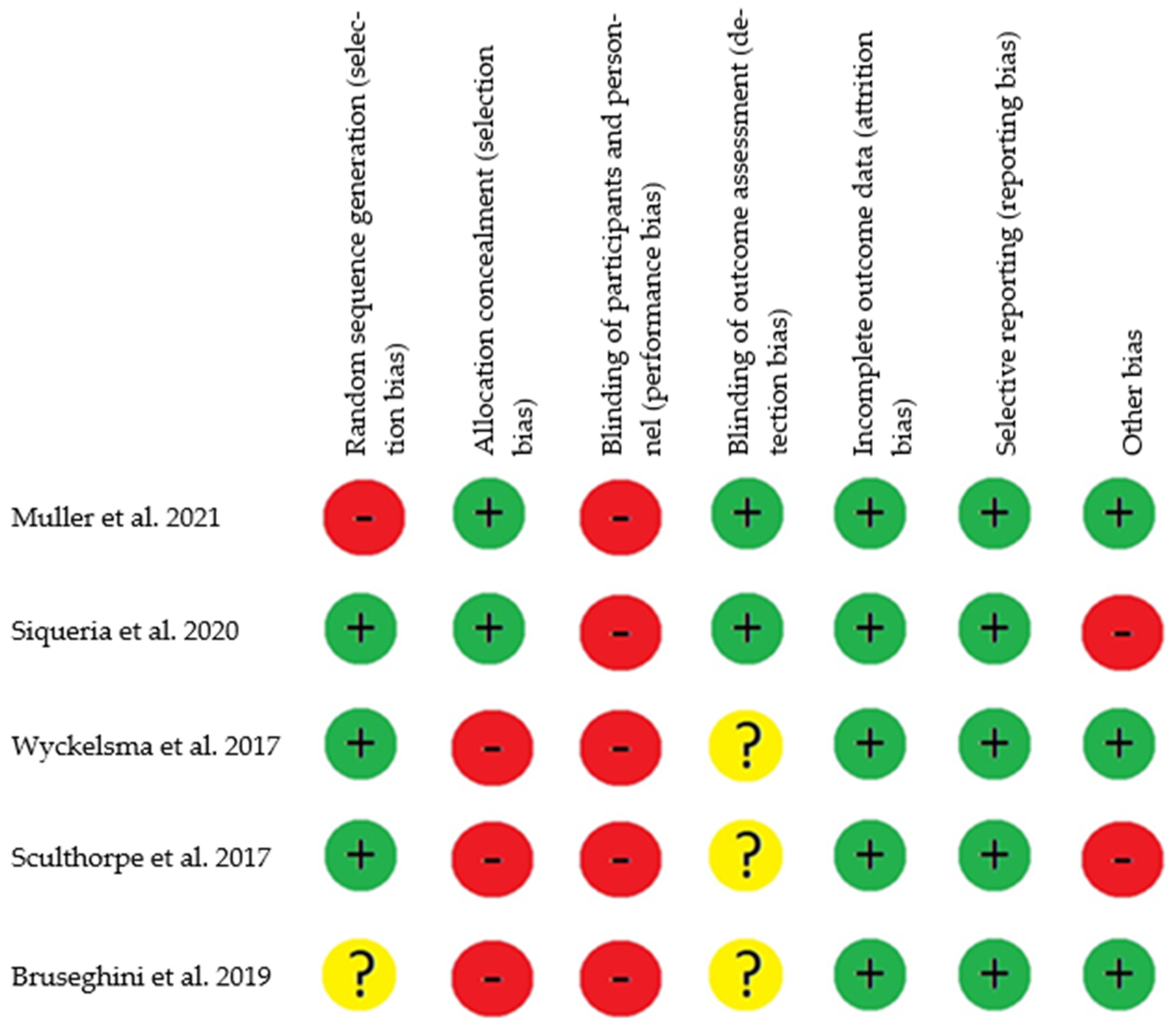
2.5. Risk of Bias Assessment
2.6. Methodological Quality Assessment
- -
- -
- Only one study had an adequate concealment of the allocation sequence [26].
- -
- -
- -
- -
- -
- -
- -
3. Results
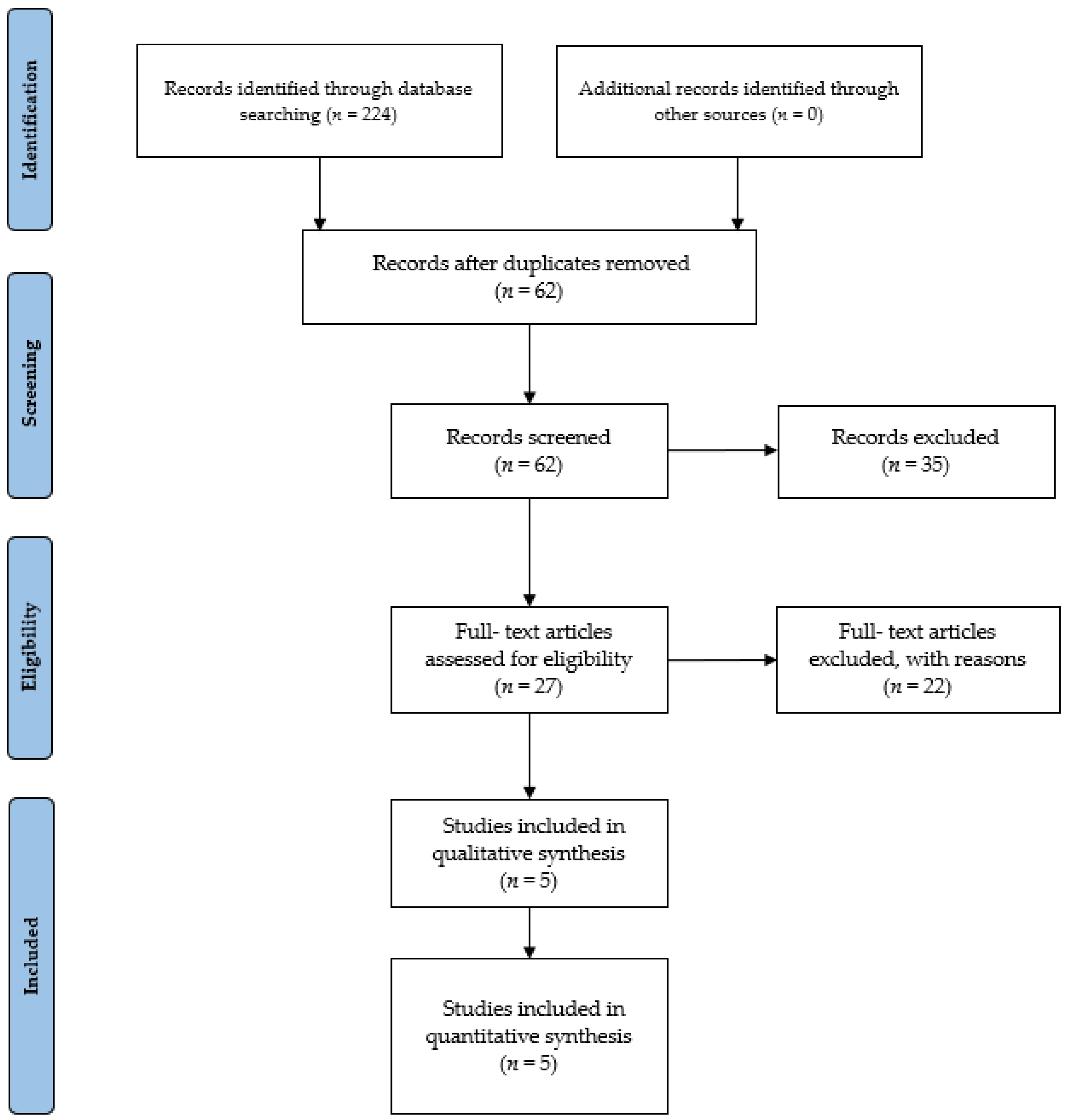
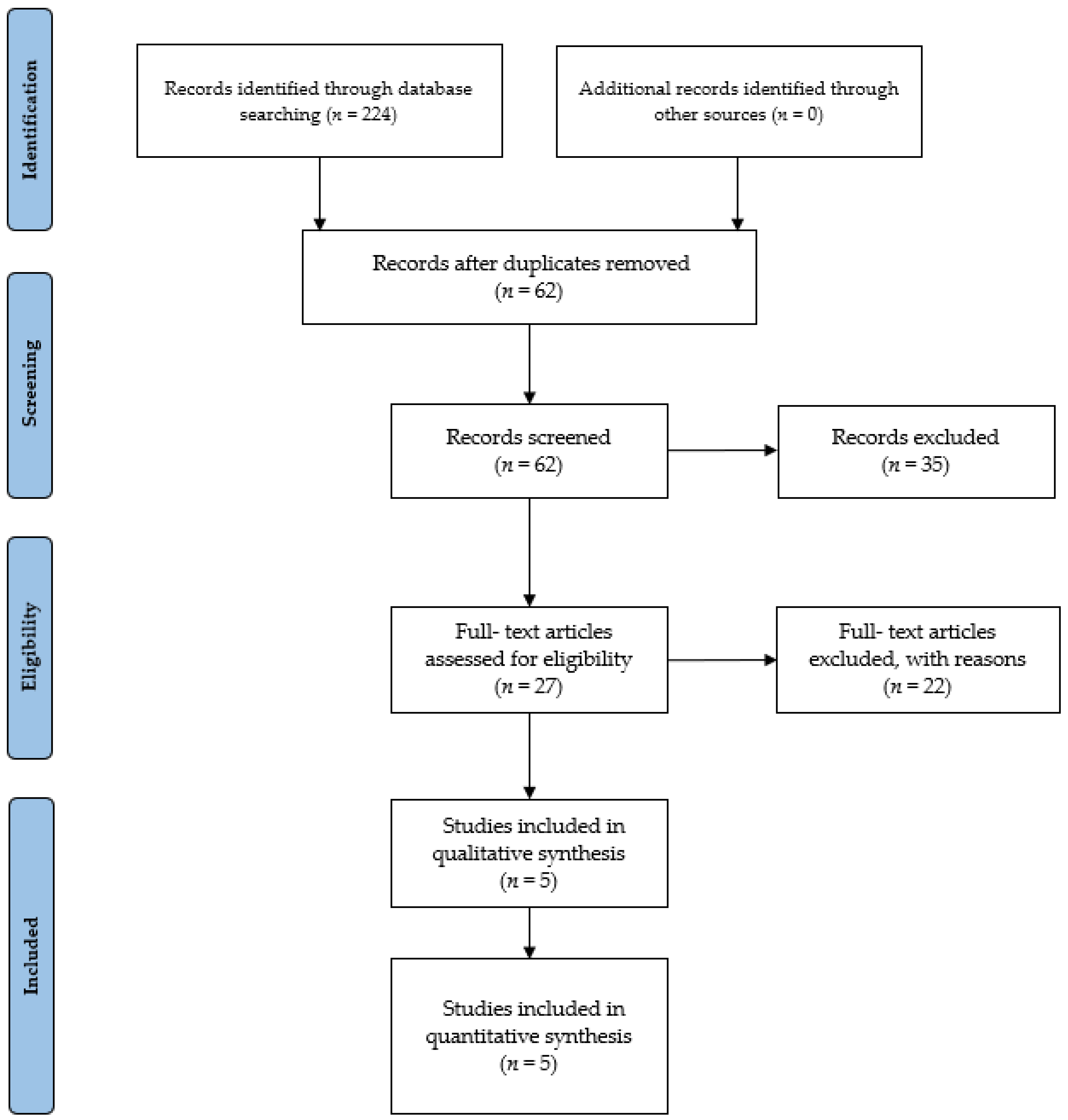
3.1. Study Identification and Selection
3.2. Study Characteristics and Context
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef]
- Rolland, Y.; Czerwinski, S.; van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Kakehi, S.; Wakabayashi, H.; Inuma, H.; Inose, T.; Shioya, M.; Aoyama, Y.; Hara, T.; Uchimura, K.; Tomita, K.; Okamoto, M.; et al. Rehabilitation Nutrition and Exercise Therapy for Sarcopenia. World J. Mens. Health 2022, 40, 1. [Google Scholar] [CrossRef]
- Burgos, R. Enfoque terapéutico global de la sarcopenia. Nutr. Hosp. 2006, 21, 51–60. [Google Scholar]
- Padilla, C.; Sánchez, P.; Cuevas, M.J. Beneficios del entrenamiento de fuerza para la prevención y tratamiento de la sarcopenia. Nutr. Hosp. 2014, 29, 979–988. [Google Scholar]
- Palop Montoro, M.V.; Párraga Montilla, J.A.; Lozano Aguilera, E.; Arteaga Checa, M. El entrenamiento vibratorio en la sarcopenia: Repercusiones en el sistema neuromuscular de los adultos mayores. Nutr. Hosp. 2015, 32, 1454–1461. [Google Scholar] [PubMed]
- Ito, S. High-intensity interval training for health benefits and care of cardiac diseases—The key to an efficient exercise protocol. World J. Cardiol. 2019, 11, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Ahn, D.; Yu, J.; Liou, K.; Keech, A. High-Intensity Interval Training for Patients With Cardiovascular Disease—Is It Safe? A Systematic Review. J. Am. Heart Assoc. 2018, 7, e009305. [Google Scholar] [CrossRef]
- Yue, T.; Wang, Y.; Liu, H.; Kong, Z.; Qi, F. Effects of High-Intensity Interval vs. Moderate-Intensity Continuous Training on Cardiac Rehabilitation in Patients With Cardiovascular Disease: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 845225. [Google Scholar] [CrossRef]
- Liu, Q.-Q.; Xie, W.-Q.; Luo, Y.-X.; Li, Y.-D.; Huang, W.-H.; Wu, Y.-X.; Li, Y.-S. High Intensity Interval Training: A Potential Method for Treating Sarcopenia. Clin. Interv. Aging 2022, 17, 857–872. [Google Scholar] [CrossRef] [PubMed]
- Alzar-Teruel, M.; Aibar-Almazán, A.; Hita-Contreras, F.; del Carmen Carcelén-Fraile, M.; Martínez-Amat, A.; Jiménez-García, J.D.; Fábrega-Cuadros, R.; Castellote-Caballero, Y. High-intensity interval training among middle-aged and older adults for body composition and muscle strength: A systematic review. Front. Public Healh 2022, 10, 992706. [Google Scholar] [CrossRef]
- Hayes, L.D.; Elliott, B.T.; Yasar, Z.; Bampouras, T.M.; Sculthorpe, N.F.; Sanal-Hayes, N.E.M.; Hurst, C. High Intensity Interval Training (HIIT) as a Potential Countermeasure for Phenotypic Characteristics of Sarcopenia: A Scoping Review. Front. Physiol. 2021, 12, 715044. [Google Scholar] [CrossRef]
- Escriche-Escuder, A.; Fuentes-Abolafio, I.J.; Roldán-Jiménez, C.; Cuesta-Vargas, A.I. Effects of exercise on muscle mass, strength, and physical performance in older adults with sarcopenia: A systematic review and meta-analysis according to the EWGSOP criteria. Exp. Gerontol. 2021, 151, 111420. [Google Scholar] [CrossRef]
- Rubio del Peral, J.A.; Gracia, M.S. Ejercicios de resistencia en el tratamiento y prevención de la sarcopenia en ancianos. Revisión sistemática. Rev. Gerokomos 2017, 29, 133–137. [Google Scholar]
- Redín, M.I. (Ed.) Biomecánica y Bases Neuromusculares de la Actividad Física y el Deporte; Editorial Médica Panamericana: Madrid, Spain, 2008; ISBN 9788498350234. [Google Scholar]
- Gómez, A.E. Sarcopenia puesta al día. Ámbito farmacéutico. Divulg. Sanit. 2011, 30, 60–65. [Google Scholar]
- Chen, Y.C.; Chen, W.-C.; Liu, C.-W.; Huang, W.-Y.; Lu, I.; Lin, C.W.; Huang, R.Y.; Chen, J.S.; Huang, C.H. Is moderate resistance training adequate for older adults with sarcopenia? A systematic review and network meta-analysis of RCTs. Eur. Rev. Aging Phys. Act. 2023, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Triana, F.C.; Gómez-Cabrera, M.C.; López-Soto, A.; Masanés, F.; Martín, P.M.; Rexach, J.A.S.; Hidalgo, D.R.; Salvà, A.; Viña, J.; et al. La eclosión de la sarcopenia: Informe preliminar del Observatorio de la Sarcopenia de la Sociedad Española de Geriatría y Gerontología. Rev. Esp. Geriatr. Gerontol. 2011, 46, 100–110. [Google Scholar] [CrossRef]
- López, J.; Campos, V. Hiit. Entrenamiento Interválico de Alta Intensidad: Bases Fisiológicas y Aplicaciones Prácticas; Exercise Physiology & Training, Fisiología del Ejercicio: Madrid, Spain, 2018; ISBN 978-84-09-00923-7. [Google Scholar]
- Keating, C.J.; Párraga Montilla, J.Á.; Latorre Román, P.Á.; Moreno del Castillo, R. Comparison of High-Intensity Interval Training to Moderate-Intensity Continuous Training in Older Adults: A Systematic Review. J. Aging Phys. Act. 2020, 28, 798–807. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Group CCCR. Data Extraction Template for Included Studies. 2016. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/uploads/det_2015_revised_final_june_20_2016_nov_29_revised.doc (accessed on 1 December 2023).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Müller, D.C.; Boeno, F.P.; Izquierdo, M.; Aagaard, P.; Teodoro, J.L.; Grazioli, R.; Cunha, G.; Ferrari, R.; Saez de Asteasu, M.L.; Pinto, R.S.; et al. Effects of high-intensity interval training combined with traditional strength or power training on functionality and physical fitness in healthy older men: A randomized controlled trial. Exp. Gerontol. 2021, 149, 111321. [Google Scholar] [CrossRef] [PubMed]
- Andrade, L.S.; Pinto, S.S.; Silva, M.R.; Schaun, G.Z.; Portella, E.G.; Nunes, G.N.; David, G.B.; Wilhelm, E.N.; Alberton, C.L. Water-based continuous and interval training in older women: Cardiorespiratory and neuromuscular outcomes (WATER study). Exp. Gerontol. 2020, 134, 110914. [Google Scholar] [CrossRef] [PubMed]
- Wyckelsma, V.L.; Levinger, I.; Murphy, R.M.; Petersen, A.C.; Perry, B.D.; Hedges, C.P.; Anderson, M.J.; McKenna, M.J. Intense interval training in healthy older adults increases skeletal muscle [3 H]ouabain-binding site content and elevates Na+,K+-ATPase α 2 isoform abundance in Type II fibers. Physiol. Rep. 2017, 5, e13219. [Google Scholar] [CrossRef]
- Sculthorpe, N.F.; Herbert, P.; Grace, F. One session of high-intensity interval training (HIIT) every 5 days, improves muscle power but not static balance in lifelong sedentary ageing men. Medicine 2017, 96, e6040. [Google Scholar] [CrossRef] [PubMed]
- Bruseghini, P.; Capelli, C.; Calabria, E.; Rossi, A.P.; Tam, E. Effects of High-Intensity Interval Training and Isoinertial Training on Leg Extensors Muscle Function, Structure, and Intermuscular Adipose Tissue in Older Adults. Front. Physiol. 2019, 10, 1260. [Google Scholar] [CrossRef] [PubMed]
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle tissue changes with aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Rogeri, P.S.; Zanella, R.; Martins, G.L.; Garcia, M.D.A.; Leite, G.; Lugaresi, R.; Gasparini, S.O.; Sperandio, G.A.; Ferreira, L.H.B.; Souza-Junior, T.P.; et al. Strategies to Prevent Sarcopenia in the Aging Process: Role of Protein Intake and Exercise. Nutrients 2021, 14, 52. [Google Scholar] [CrossRef] [PubMed]
- Marriott, C.F.S.; Petrella, A.F.M.; Marriott, E.C.S.; Boa Sorte Silva, N.C.; Petrella, R.J. High-Intensity Interval Training in Older Adults: A Scoping Review. Sports Med.-Open 2021, 7, 49. [Google Scholar] [CrossRef]
- Stern, G.; Psycharakis, S.G.; Phillips, S.M. Effect of High-Intensity Interval Training on Functional Movement in Older Adults: A Systematic Review and Meta-analysis. Sports Med.-Open 2023, 9, 5. [Google Scholar] [CrossRef]
- Batacan, R.B.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Blue, M.N.M.; Smith-Ryan, A.E.; Trexler, E.T.; Hirsch, K.R. The effects of high intensity interval training on muscle size and quality in overweight and obese adults. J. Sci. Med. Sport 2018, 21, 207–212. [Google Scholar] [CrossRef]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; Van Essen, M.; Wilkin, G.P.; Burgomaster, K.A.; Safdar, A.; Raha, S.; Tarnopolsky, M.A. Short-term sprint interval versus traditional endurance training: Similar initial adaptations in human skeletal muscle and exercise performance. J. Physiol. 2006, 575, 901–911. [Google Scholar] [CrossRef]
- Rennie, M.J.; Wackerhage, H.; Spangenburg, E.E.; Booth, F.W. Control of the Size of the Human Muscle Mass. Annu. Rev. Physiol. 2004, 66, 799–828. [Google Scholar] [CrossRef] [PubMed]
- Smith-Ryan, A.E.; Melvin, M.N.; Wingfield, H.L. High-intensity interval training: Modulating interval duration in overweight/obese men. Phys. Sportsmed. 2015, 43, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Trapp, E.G.; Chisholm, D.J.; Freund, J.; Boutcher, S.H. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int. J. Obes. 2008, 32, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Scalzo, R.L.; Peltonen, G.L.; Binns, S.E.; Shankaran, M.; Giordano, G.R.; Hartley, D.A.; Klochak, A.L.; Lonac, M.C.; Paris, H.L.R.; Szallar, S.E.; et al. Greater muscle protein synthesis and mitochondrial biogenesis in males compared with females during sprint interval training. FASEB J. 2014, 28, 2705–2714. [Google Scholar] [CrossRef] [PubMed]
- Di Donato, D.M.; West, D.W.D.; Churchward-Venne, T.A.; Breen, L.; Baker, S.K.; Phillips, S.M. Influence of aerobic exercise intensity on myofibrillar and mitochondrial protein synthesis in young men during early and late postexercise recovery. Am. J. Physiol. Metab. 2014, 306, E1025–E1032. [Google Scholar] [CrossRef] [PubMed]
- Damas, F.; Phillips, S.M.; Libardi, C.A.; Vechin, F.C.; Lixandrão, M.E.; Jannig, P.R.; Costa, L.A.R.; Bacurau, A.V.; Snijders, T.; Parise, G.; et al. Resistance training-induced changes in integrated myofibrillar protein synthesis are related to hypertrophy only after attenuation of muscle damage. J. Physiol. 2016, 594, 5209–5222. [Google Scholar] [CrossRef] [PubMed]
- Hvid, L.G.; Strotmeyer, E.S.; Skjødt, M.; Magnussen, L.V.; Andersen, M.; Caserotti, P. Voluntary muscle activation improves with power training and is associated with changes in gait speed in mobility-limited older adults—A randomized controlled trial. Exp. Gerontol. 2016, 80, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J.; Lexell, J. Human Aging, Muscle Mass, and Fiber Type Composition. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50A, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, U.H.; Johnson, A.W.; Vehrs, P.R.; Feland, J.B.; Hilton, S.C. Performance on the Functional Movement Screen in older active adults. J. Sport Healh Sci. 2016, 5, 119–125. [Google Scholar] [CrossRef]
- Metter, E.J.; Conwit, R.; Tobin, J.; Fozard, J.L. Age-Associated Loss of Power and Strength in the Upper Extremities in Women and Men. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52A, B267–B276. [Google Scholar] [CrossRef] [PubMed]
- Lexell, J.; Taylor, C.C.; Sjöström, M. What is the cause of the ageing atrophy? J. Neurol. Sci. 1988, 84, 275–294. [Google Scholar] [CrossRef]
- WHO. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2015.
- Gómez-López, M.; Gallegos, A.G.; Extremera, A.B. Perceived barriers by university students in the practice of physical activities. J. Sports Sci. Med. 2010, 9, 374–381. [Google Scholar]
- Ferreira, L.F.; de Oliveira, A.R.; Schiefelbein, M.L.; Garcia, E.; da Rosa, L.H.T. Aerobic Training Does not Decrease the Prevalence of Sarcopenia in Older Women: Cross-Sectional Study. Ageing Int. 2023, 48, 563–574. [Google Scholar] [CrossRef]
- Robinson, M.M.; Dasari, S.; Konopka, A.R.; Johnson, M.L.; Manjunatha, S.; Esponda, R.R.; Carter, R.E.; Lanza, I.R.; Nair, K.S. Enhanced Protein Translation Underlies Improved Metabolic and Physical Adaptations to Different Exercise Training Modes in Young and Old Humans. Cell Metab. 2017, 25, 581–592. [Google Scholar] [CrossRef]
- Liu, Y.; Guo, C.; Liu, S.; Zhang, S.; Mao, Y.; Fang, L. Eight Weeks of High-Intensity Interval Static Strength Training Improves Skeletal Muscle Atrophy and Motor Function in Aged Rats via the PGC-1α/FNDC5/UCP1 Pathway. Clin. Interv. Aging 2021, 16, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Fyfe, J.J.; Bartlett, J.D.; Hanson, E.D.; Stepto, N.K.; Bishop, D.J. Endurance Training Intensity Does Not Mediate Interference to Maximal Lower-Body Strength Gain during Short-Term Concurrent Training. Front. Physiol. 2016, 7, 487. [Google Scholar] [CrossRef] [PubMed]
- Leuchtmann, A.B.; Mueller, S.M.; Aguayo, D.; Petersen, J.A.; Ligon-Auer, M.; Flück, M.; Jung, H.H.; Toigo, M. Resistance training preserves high-intensity interval training induced improvements in skeletal muscle capillarization of healthy old men: A randomized controlled trial. Sci. Rep. 2020, 10, 6578. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.; Thoma, C.; Houghton, D.; Trenell, M.I. High-intensity interval training: A review of its impact on glucose control and cardiometabolic health. Diabetologia 2017, 60, 7–23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Populations without any injury or illness, with normal vision, and no history of neuropsychological impairment and/or other special conditions | Studies carried out with animals. Populations with special conditions (some types of pathology other than sarcopenia, type II diabetes, cardiovascular pathology, and obesity). Populations aged less than 65 years old. |
| Intervention | Studies with high-intensity interval training protocols studying the effects of strength exercises designed with an intervention group and a control group | Studies with high-intensity interval training protocols combined with another type of intervention that could mask the results of the former intervention (either another type of training, nutritional, or pharmacological ergogenic aids). |
| Comparison/comparator | Passive control conditions | Intervention conditions other than passive conditions. |
| Outcome | Muscle strength improvements | Physiological or physical conditions not related to the included outcomes. |
| Study design | Counterbalanced cross-over design (either randomized or non-randomized since none of them reveals significant differences in control conditions) | Study designs that do not allow within-subjects comparisons for the two conditions. |
| Additional criteria | Only indexed, original, full-text studies | Articles other than original research (e.g., reviews, letters to editors, trial registrations, proposals for protocols, editorials, book chapters, and conference abstracts). |
| Müller et al. [26] | ||||||||||||||||
| Population | Participants | Age (Years) | Sex | Body Mass (Kg) | Height (Cm) | BMI | Sample | Exclusion Pathologies | Assistance | |||||||
| 35 | 65.8 ± 3.9 | M | 89.3 ± 9.9 | 172.4 cm ± 7.4 | 18.75 | TST + HIIT: N = 18 | Neuromuscular, cognitive, metabolic, hormonal, cardiovascular, smokers. | 100% | ||||||||
| 84.7 ± 14.8 | TPT + HIIT: N = 17 | |||||||||||||||
| 85.3 ± 12.8 | HIIT: N = 35 | |||||||||||||||
| Intervention | Duration (Week)/ Frequency (Day) | Ig | Cg | Intensity/Velocity | Phase/Time | Characteristics | Measurement | Exercise | Questionnaire | |||||||
| 16/2 | TST + HIIT | No | 65–80% RM | 2 s (concentric and eccentric) | Week 1–4: 2 x (12–15 rep 65% RM x 180 s rest) Week 13–16: 4 x (6–8 rep 80% RM x 180 s rest) | Functional capacity | Sit-to-Stand (>n° rep x 30 s), Timed- Up and Go, climbing stairs (16 cm) | - | ||||||||
| TPT + HIIT | 40–60% RM | 2 s eccentric and maximum concentric | Week 1–4: 3 x (8 rep 40% RM x 180 s rest) Week 13–16: 4 x (6 rep 60% RM x 180 s rest) | Cardiorespiratory capacity | Peak power in cycling: Wmax, VO2max, cycling economy | |||||||||||
| HIIT | 75–90% VO2max | - | Cycle-ergometer: Warming 5 min 60–65% HRmax Cadence 70–75 rpm Week 1–4: 3 x (4 min 75–85% HRmax x 2 min active rest) Week 13–16 3 x (4 min 85–90% HRmax x 2 min active rest) | Body composition (DEXA) | Before intervention, 8 weeks, 16 weeks: body fat mass, lean body mass, total body fat mass, total lean body mass | |||||||||||
| Results | Measurement | Exercise/Parameter | TST | TPT | ||||||||||||
| Functional capacity | Sit-to-Stand | 8 weeks: ↑ 13.3% (p < 0.001) ES = 0.91 16 weeks: ↑ 15.9% (p < 0.001) | 8 weeks: ↑ 30% (p < 0.001) ES = 1.46 16 weeks: ↑ 27.1% (p < 0.001) | |||||||||||||
| Timed Up and Go | 8 weeks: (p < 0.001) No differences ES = 0.47. 16 weeks: ↑ 10% (p < 0.001) | 16 weeks: ↑ 14% (p < 0.001) ES = 0.54 | ||||||||||||||
| Climbing stairs | 8 weeks: ↑ 13.2% (p < 0.005) 16 weeks: ↑ 15.2% (p < 0.001) ES = 0.54 | 8 weeks: ↑ 13.9% (p < 0.005) 16 weeks: ↑ 12.3% (p < 0.001) ES = 0.78 | ||||||||||||||
| Cardiorespiratory capacity | Wmax | 8 weeks: ↑ 6.7% (p < 0.001) 16 weeks: ↑ 9.9% (p < 0.001) ES = 0.75 | 8 weeks: ↑ 8% (p < 0.001) 16 weeks: ↑ 11.1% (p < 0.001) ES = 1.17 | |||||||||||||
| VO2max | 8 weeks: ↑ 7.8% (p < 0.005) 16 weeks: ↑ 10% (p < 0.001) ES = 0.53 | 8 weeks: ↑ 22.3% (p < 0.005) 16 weeks: ↑ 37.8% (p < 0.001) ES = 0.54 | ||||||||||||||
| Cycling economy | 8 weeks: ↑ 9.9% (p < 0.001) 16 weeks: ↑ 9.5% (p < 0.001) ES = −0.6 | 8 weeks: ↑ 10.7% (p < 0.001) 16 weeks: ↑ 17.2% (p < 0.001) ES = 0.34 | ||||||||||||||
| Siqueria et al. [27] | ||||||||||||||||
| Population | Participants | Age (Years) | Sex | Body Mass (Kg) | Height (cm) | BMI | Sample | Exclusion Pathologies | Assistance | |||||||
| 41 | 63.9 ± 2.5 | F | 74.4 ± 14.7 | 153.4 cm ± 4.3 | 31.5 | CG: n = 21 | Cardiovascular disease and osteo-articular restrictions for exercising. | CG: 82.6% | ||||||||
| 64.8 ± 3.6 | 74.4 ± 14.7 | 155.1 cm ± 5.8 | 30.1 | IG: n = 20 | IG: 82.2% | |||||||||||
| Intervention | Duration (Week)/ Frequency (Day) | IG | CG | Intensity/Velocity | Phase/Time | Characteristics | Measurement | Exercise | Questionnaire | |||||||
| 12/2 | CG | No | Borg Scale (6–20) RPE: 13–16/- | 2 s (concentric and eccentric) | Week 1–4: 36 min RPE: 13 Week 5–8: 36 min RPE: 14 Week 9–10: 36 min RPE 15 Week 11–12: 36 min RPE 16 | Cardiorespiratory capacity | Stationary running, front kick and cross-country skiing Aquatic intervention | Informed consent form | ||||||||
| IG | RPE: 11–18/- | 2 s (concentric and eccentric) | Week 1–4: 9 rep x (2 min RPE:16 + 2 min RPE 11) Week 5–8: 12 x (1.5 min RPE:17 + 1.5 min RPE 11) Week 9–10: 18 x (1 min RPE:18 + 1 min RPE 11) Week 11–12: 18 x (1 min RPE:18 + 1 min RPE 11) | Neuromuscular capacity | ||||||||||||
| Results | Measurement | Exercise Parameter | CG | IG | ||||||||||||
| Cardiorespiratory capacity | Cycle-ergometer RHR (bpm) | ↓ 15.4% (p < 0.05) Pre CG: 83 ± 21 Post CG: 75 ± 11 | ↓ 11.8% (p < 0.05) Pre: 80 ± 14 Post: 75 ± 14 | |||||||||||||
| VO2max (mL·kg−1·min−1) | ↑ 10.3% (p < 0.05) Pre: 26.30 ± 3.68 Post: 28.76 ± 5.05 | ↑ 16.5% (p < 0.05) Pre: 24.07 ± 4.10 Post: 26.01 ± 7.95 | ||||||||||||||
| Exhaustion tolerance | ↑ 5.6% (p < 0.05) Pre: 13.08 ± 1.91 Post: 14.02 ± 1.88 | ↑ 13.5% (p < 0.05) Pre: 12.75 ± 1.45 Post: 14.04 ± 1.40 | ||||||||||||||
| Neuromuscular capacity | Maximal dynamic strength (kg) | ↑ 5.9% (p < 0.05) Pre: 30.92 ± 6.29 Post: 32.42 ± 6.42 | ↑ 12.5% (p < 0.05) Pre: 28.00 ± 5.68 Post: 29.50 ± 5.21 | |||||||||||||
| Dynamic resistance | ↑ 15.3% (p < 0.05) Pre: 11.83 ± 2.21 Post: 13.08 ± 3.48 | ↑ 6.7% (p < 0.05) Pre: 12.63 ± 2.07 Post: 14.00 ± 2.62 | ||||||||||||||
| Neuromuscular activation (uV) | ↑ 38.4% (p < 0.05) Pre: 94.16 ± 40.82 Post: 102.30 ± 45.26 | ↑ 47.7% (p < 0.05) Pre: 121.00 ± 67.62 Post: 151.13 ± 72.62 | ||||||||||||||
| Muscular thickness (cm) | ↑ 4.8% (p < 0.05) Pre: 6.07 ± 0.79 Post: 6.35 ± 0.87 | ↑ 6.7% (p < 0.05) Pre: 6.26 ± 0.98 Post: 6.62 ± 1.11 | ||||||||||||||
| Muscular volume (cm3) | ↑ 68.2 cm3 Post-IRT compared to Pre-IRT (p = 0.001) | ↑ 42.2 cm3 Post-HIIT compared to Pre-HIIT (p = 0.003) | ||||||||||||||
| ACSA in relation to IMAT intermuscular adipose tissue: | 50% LF ↓ Post-IRT compared to Pre-IRT (p = 0.008) 75% LF ↓ Post-IRT compared to Pre-IRT (p = 0.001) | 50% LF ↓ Post-HIIT compared to Pre-HIIT (p = 0.001) CI: 95%; 75% LF: No significance (p > 0.05) | ||||||||||||||
| Muscular torque | IRT ↑ 7.8% TMVC: 90° ↑ 11.5 N·m ± 17.1 (p = 0.040) IRT ↑ TC: 120° s−1 ↑ 8.8 N·m ± 13.0 (p = 0.008) | HIIT no significance | ||||||||||||||
| Pennation angle, PCSA and specific torque | PCSA 50% LG: ↑ Post-IRT compared to Pre-IRT (p = 0.025) Significant effect time-training IRT ↑ Post-IRT compared to Pre-IRT (p = 0.004) | Significant effect time-training IRT ↑ Post-HIIT compared to Pre-HIIT (p = 0.001) | ||||||||||||||
| Specific isometric strength (Strength/ACSA) | With IMAT torque·cm2 from ACSA it remained unchanged Without IMAT torque·cm2 from ACSA: Pre-IRT (63.8 N·cm−2 ± 5.6) Post-IRT (63.0, N·cm−2 ± 9.1) | With IMAT torque·cm2 from ACSA it remained unchanged Without IMAT torque·cm2 from ACSA: Pre-HIIT 66.4 N·cm−2 ± 6.1; Post-HIIT 60.8 N·cm−2 ± 7.5 | ||||||||||||||
| Neuromuscular activation | ↑ Post-IRT compared to Pre-IRT (p = 0.011) | - | ||||||||||||||
| Wyckelsma et al. [28] | ||||||||||||||||
| Population | Participants | Age (Years) | Sex | Body Mass (Kg) | Height (cm) | BMI | Sample | Exclusion Pathologies | Assistance | |||||||
| Beginning: 15 | 69.4 ± 3.5 | 6 M 2 F | 75.2 ± 13.0 | 170.8 ± 10.4 cm | 21.6 | IG: n = 8 | Type I or type II diabetes, chronic heart disease, severe hypertension, severe overweight/obesity, uncontrolled metabolic disease, cardiovascular disease and injuries. | IG: 83% (30/36 sessions) | ||||||||
| Intervention: 13 | 3 M 4 F | CG: n = 7 | ||||||||||||||
| Intervention | Duration (Week)/Frequency (Day) | IG | CG | Intensity/Velocity | Phase/Time | Characteristics | Measurement | Exercise | Questionnaire | |||||||
| 12/3 | IG | No | RPE 17/- | - | Warming: 5 min cycle-ergometer PP: 4 rep x (4 min 90–94%HRmax x 4 min active resting 50–60% HRmax), Calm down: 5 min cycle-ergometer | Cardiorespiratory capacity Plasma changes (K+), union of (3H) muscular ouabain and NKA isoforms | Cycle-ergometer | - | ||||||||
| Results | Measurement | Exercise Parameter | CG | IG | ||||||||||||
| Cardiorespiratory capacity | HR peak (b x min−1) | Pre: 141 ± 11 Post: 142 ± 14 | ↑ 6.8% (p < 0.05) Pre: 136.2 ± 16.4 Post: 144.3 ± 14.4 | |||||||||||||
| VO2peak (mL x kg−1 x min−1) | Pre: 23.6 ± 5.3 Post: 23.8 ± 5.3 | ↑ 16.2% (p < 0.05) Pre: 24.7 ± 5.4 Post: 28.7 ± 5.1 | ||||||||||||||
| Performance capacity | WRpeak (W) | Pre: 142.0 ± 46.4 Post: 147.1 ± 40.2 | ↑ 25.23% (p < 0.05) Pre: 145.0 ± 49.5 Post: 181.2 ± 52.4 | |||||||||||||
| Work (J) | Pre: 47.914 ± 24.408 Post: 47.486 ± 24.834 | ↑ 60.46% (p < 0.05) Pre: 43.725 ± 21.282 Post: 70.050 ± 31.834 | ||||||||||||||
| Time to RPE-17 (min) | Pre: 9.6 ± 3.1 Post: 9.7 ± 3.1 | Pre: 7.3 ± 3.7 Post: 9.4 ± 4.5 | ||||||||||||||
| Physiological capacity | [K+ ]v peak (mmol.L−1) | Pre: 4.88 ± 0.33 Post: 4.90 ± 0.42 | ↑ 10% (p = 0.056) Pre: 4.74 ± 0.41 Post: 5.23 ± 0.57 | |||||||||||||
| Δ[K+ ]v x work−1 (nmolx L−1 x J−1) | Pre: 22.3 ± 10.9 Post: 21.1 ± 14.7 | (p > 0.05) No differences Pre: 21.4 ± 10.6 Post: 17.4 ± 4.5 | ||||||||||||||
| Sculthorpe et al. [29] | ||||||||||||||||
| Population | Participants | Age (Years) | Sex | Body Mass (Kg) | Height(cm) | BMI | Sample Number | Exclusion Pathologies | Assistance | |||||||
| 33 | 62.3 ± 4.1 | M | 89.9 ± 17.1 | 175 ± 5.2 | 29.4 | HITT: n = 22 | - | 100% | ||||||||
| 61.6 ± 5.0 | 87.5 ± 14.3 | 173 ± 5.5 | 29.1 | CG: n = 11 | ||||||||||||
| Intervention | Duration (Week)/ Frequency (Day) | IG | CG | Intensity/Velocity | Phase/Time | Characteristics | Measurement | Exercise | Questionnaire | |||||||
| 6/5 | Conditioning | No | Week 1–2: 55% HRR/- Week 3–4: 60% HRR/- Week 5–6: 65% HRR/- | - | Perform the activity of participant’s preference, taking into account duration, HR and recommended intensity. | Body composition, static equilibrium and start point | Walking, jogging, cycling | PAR-Q | ||||||||
| 6/1.4 | HIIT | No | 40–50% PP 90% HRR | - | Warming: 5 min cycle-ergometer PP: 6 rep sprints x (30 s 50% PP90% HRR x 3 min active resting) | Cycle-ergometer | IPAQ | |||||||||
| Results | Measurement | Exercise Parameter | CG | IG | ||||||||||||
| Performance capacity | WRpeak (W) | Phase A: 655 W Phase B: 661 W Phase C: 657 W Phase A–B: ↑ 1% ↑ 6 W (p > 0.05) Phase B–C: ↓ 0.6% ↓ 4 W (p > 0.05) Phase A–C: ↑ 2 W (p > 0.05) | Phase A: 699 W Phase B: 706 W Phase C: 831 W Phase A–B: ↑ 1% ↑ 7 W (p > 0.05) Phase B–C: ↑ 17.6% ↑ 125 W (p < 0.01) Phase A–C: ↑ 132 W (p < 0.01) Phase A: IG ↑ 44 W (↑ 6.7%) compared to CG Phase B: IG ↑ 44.7 W (↑ 6.7%) compared to CG Phase C: IG ↑ 173.8 W (↑ 26%) compared to CG | |||||||||||||
| Relative WRpeak (W/Kg) | Phase A–B: No improvement (p > 0.05) Phase B–C: No improvement (p > 0.05) | Phase A–B: No improvement (p > 0.05) Phase B–C: ↑ 1.53 W/Kg ↑ 14% (p < 0.01) Phase C: IG ↑ 1.67 W/Kg (↑ 15%) compared to CG | ||||||||||||||
| Body composition | Total body mass | No effect PP on phase or, group (p > 0.05) | No effect PP on phase or, group (p > 0.05) | |||||||||||||
| Total body lean mass | Phase A: 63.4 Kg Phase B: 63.7 Kg Phase C: 63.6 Kg Phase A–B: ↑ 0.4% (p > 0.05) Phase B–C: ↓ 0.1 (p> 0.05) | Phase A: 65.9 Kg Phase B: 66.1 Kg Phase C: 68.1 Kg Phase A–B: ↑ 0.3% (p > 0.05) Phase B–C: ↑ 3% (p < 0.05) Phase A: IG ↑ 2.5 Kg (↑ 3.9%) compared to CG Phase B: IG ↑ 2.4 Kg (↑ 3.7%) compared to CG Phase C: IG ↑ 4.5 Kg (↑ 7%) compared to CG | ||||||||||||||
| Total body fat mass | Phase A: 19.8 Kg Phase B: 19.9 Kg Phase C: 19.3 Kg Phase A–B: ↑ 0.1% (p > 0.05) Phase B–C: ↓ 0.7% (p > 0.05) | Phase A: 23.9 Kg Phase B: 22.8 Kg Phase C: 20.8 Kg Phase A–B: (p < 0.05) CI: 95% Phase B–C: (p < 0.05) CI: 95% Phase A: IG ↓ 4.1 Kg compared to CG Phase B: IG ↓ 2.9 Kg compared to CG Phase C: IG ↓ 1.5 Kg compared to CG | ||||||||||||||
| Bruseghini et al. [30] | ||||||||||||||||
| Population | Participants | Age (Years) | Sex | Body Mass (Kg) | Height (cm) | BMI | Sample Number | Exclusion Pathologies | Assistance | |||||||
| 12 | 69.3 ± 4.2 | M | 77.8 ± 10.4 | 172 ± 5.0 | 26.5 | HIIT aerobic training: n = 12 | Abnormal EKG, hypertension, cardiovascular, respiratory, metabolic, kidney failure, neurological, orthopaedics, anticoagulant treatment and antiplatelet therapy contraindication, drugs and alcohol abuse | 100% | ||||||||
| IRT: n = 12 | ||||||||||||||||
| Intervention | Duration (Week)/ Frequency (Day) | IG | CG | Intensity/Velocity | Phase/Time | Characteristics | Measurement | Exercise | Questionnaire | |||||||
| 8/3 | HIIT | No | 85–95% VO2max/- | - | Warming:10 min cycle-ergometer PP: 7 rep x (2 min 85–95% VO2max x 2 min 40% VO2max) | Strength, mass, architecture and muscular quality, IMAT, and neuromuscular activation | Cycle-ergometer | IPAQ | ||||||||
| IRT | Maximal concentric contraction | Warming: 10 min 3 rep x (7 submaximal knee extension) PP: 4 rep x (7 maximal concentric knee extension and eccentric knee flexion) | Cycle-ergometer Iso-inertial machine Yoyo Technology AB | |||||||||||||
| Results | Measurement | Exercise Parameter | IRT | HIIT | ||||||||||||
| Neuromuscular capacity | ACSA (cm2) | 25% LF ↑ IRT compared to HIIT (p = 0.024) 75% LF ↑ IRT compared to Post-HIIT (p = 0.08) 75% LF ↑ IRT compared to Pre-HIIT (p = 0.011) ↑ 4.47 cm2 Post-IRT compared to Pre-IRT (p = 0.001) | 25% LF ↑ 3.19 cm (p = 0.001) 50% LF ↑ 3.03 cm (p = 0.005) 75% LF ↑ 3.40 cm (p = 0.004) ↑ 3.9 cm2 Post-HIIT compared to Pre-HIIT (p = 0.001) | |||||||||||||
| Muscular volume (cm3) | ↑ 68.2 cm3 Post-IRT compared to Pre-IRT (p = 0.001) | ↑ 42.2 cm3 Post-HIIT compared to Pre-HIIT (p = 0.003) | ||||||||||||||
| ACSA in relation to IMAT intermuscular adipose tissue | 50% LF ↓ Post-IRT compared to Pre-IRT (p = 0.008) 75% LF ↓ Post-IRT compared to Pre-IRT (p = 0.001) | 50% LF ↓ Post-HIIT compared to Pre-HIIT (p = 0.001) CI: 95%; 75% LF: No significance (p > 0.05) | ||||||||||||||
| Muscular torque | IRT ↑ 7.8% MVC: 90° ↑ 11.5 N·m ± 17.1 (p = 0.040) IRT ↑ TC: 120° s−1 ↑ 8.8 N·m ± 13.0 (p = 0.008) | HIIT no significance | ||||||||||||||
| Pennation angle, PCSA and specific torque | PCSA 50% LG: ↑ Post-IRT compared to Pre-IRT (p = 0.025) Significant effect time-training IRT ↑ Post-IRT compared to Pre-IRT (p = 0.004) | Significant effect time-training IRT ↑ Post-HIIT compared to Pre-HIIT (p = 0.001) | ||||||||||||||
| Specific isometric strength (Strength/ACSA) | With IMAT torque·cm2 from ACSA it remained unchanged Without IMAT torque·cm2 from ACSA: Pre-IRT (63.8 N·cm−2 ± 5.6) Post-IRT (63.0, N·cm−2 ± 9.1) | With IMAT torque·cm2 from ACSA it remained unchanged Without IMAT torque·cm2 from ACSA: Pre-HIIT 66.4 N·cm−2 ± 6.1; Post-HIIT 60.8 N·cm−2 ± 7.5 | ||||||||||||||
| Neuromuscular activation | ↑ Post-IRT compared to Pre-IRT (p = 0.011) | - | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morcillo-Losa, J.A.; Díaz-Martínez, M.d.P.; Ceylan, H.İ.; Moreno-Vecino, B.; Bragazzi, N.L.; Párraga Montilla, J. Effects of High-Intensity Interval Training on Muscle Strength for the Prevention and Treatment of Sarcopenia in Older Adults: A Systematic Review of the Literature. J. Clin. Med. 2024, 13, 1299. https://doi.org/10.3390/jcm13051299
Morcillo-Losa JA, Díaz-Martínez MdP, Ceylan Hİ, Moreno-Vecino B, Bragazzi NL, Párraga Montilla J. Effects of High-Intensity Interval Training on Muscle Strength for the Prevention and Treatment of Sarcopenia in Older Adults: A Systematic Review of the Literature. Journal of Clinical Medicine. 2024; 13(5):1299. https://doi.org/10.3390/jcm13051299
Chicago/Turabian StyleMorcillo-Losa, José Alfonso, Maria del Pilar Díaz-Martínez, Halil İbrahim Ceylan, Beatriz Moreno-Vecino, Nicola Luigi Bragazzi, and Juan Párraga Montilla. 2024. "Effects of High-Intensity Interval Training on Muscle Strength for the Prevention and Treatment of Sarcopenia in Older Adults: A Systematic Review of the Literature" Journal of Clinical Medicine 13, no. 5: 1299. https://doi.org/10.3390/jcm13051299
APA StyleMorcillo-Losa, J. A., Díaz-Martínez, M. d. P., Ceylan, H. İ., Moreno-Vecino, B., Bragazzi, N. L., & Párraga Montilla, J. (2024). Effects of High-Intensity Interval Training on Muscle Strength for the Prevention and Treatment of Sarcopenia in Older Adults: A Systematic Review of the Literature. Journal of Clinical Medicine, 13(5), 1299. https://doi.org/10.3390/jcm13051299