
Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction

 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. SII Determinants in the STEMI Population
4.2. SIRI Determinants in the STEMI Population
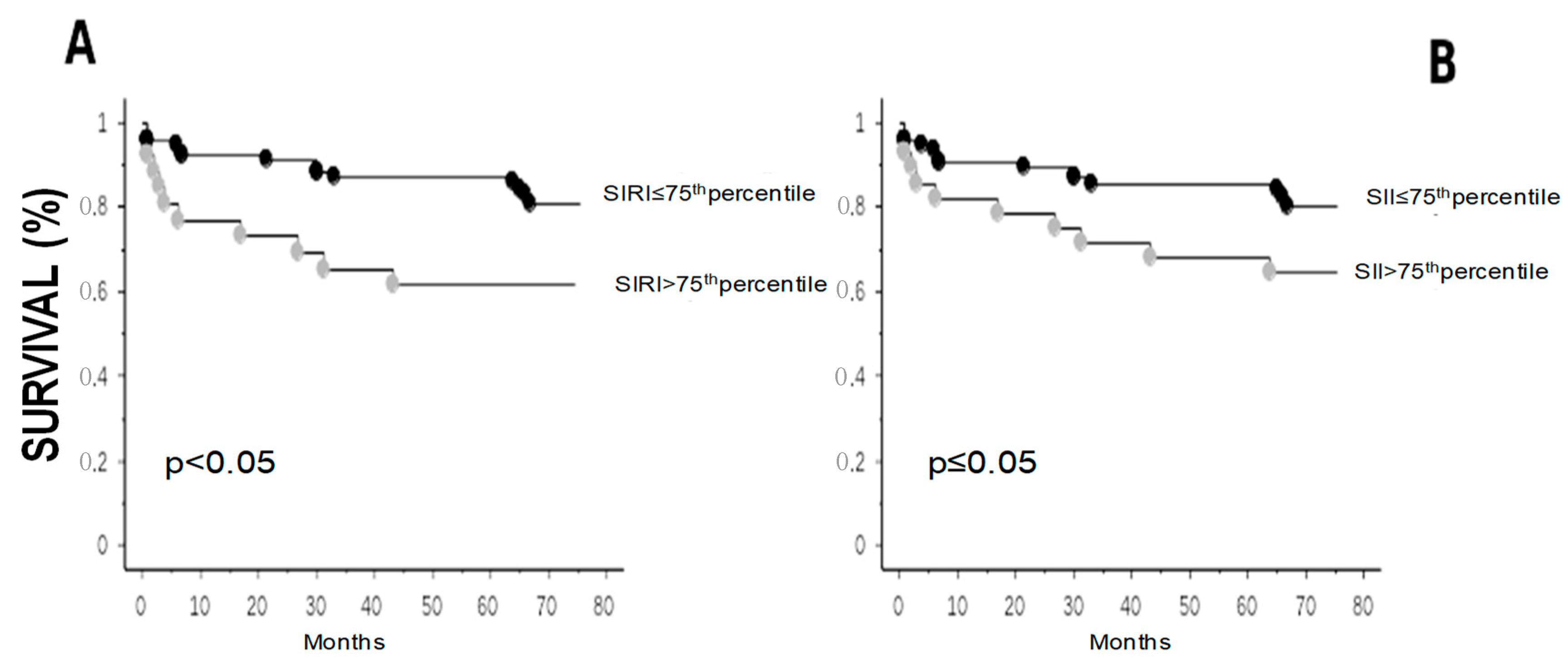
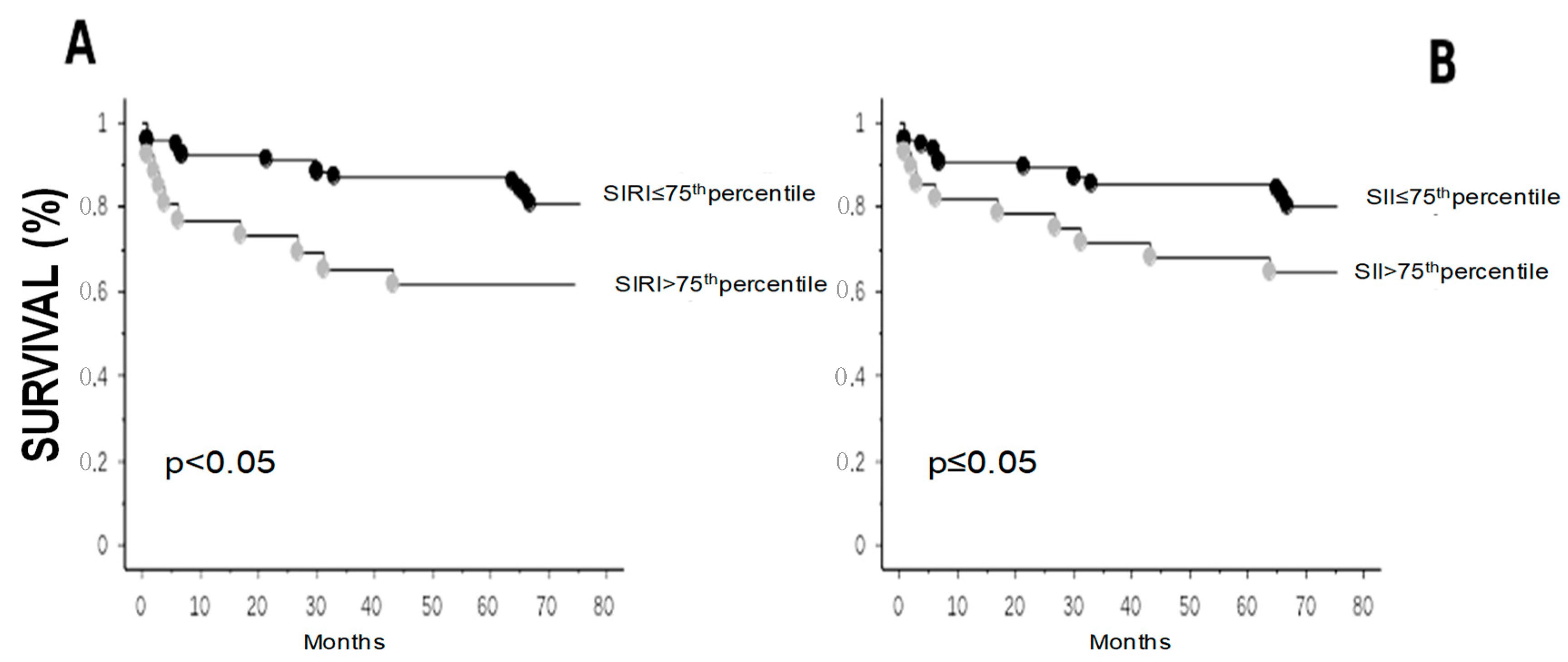
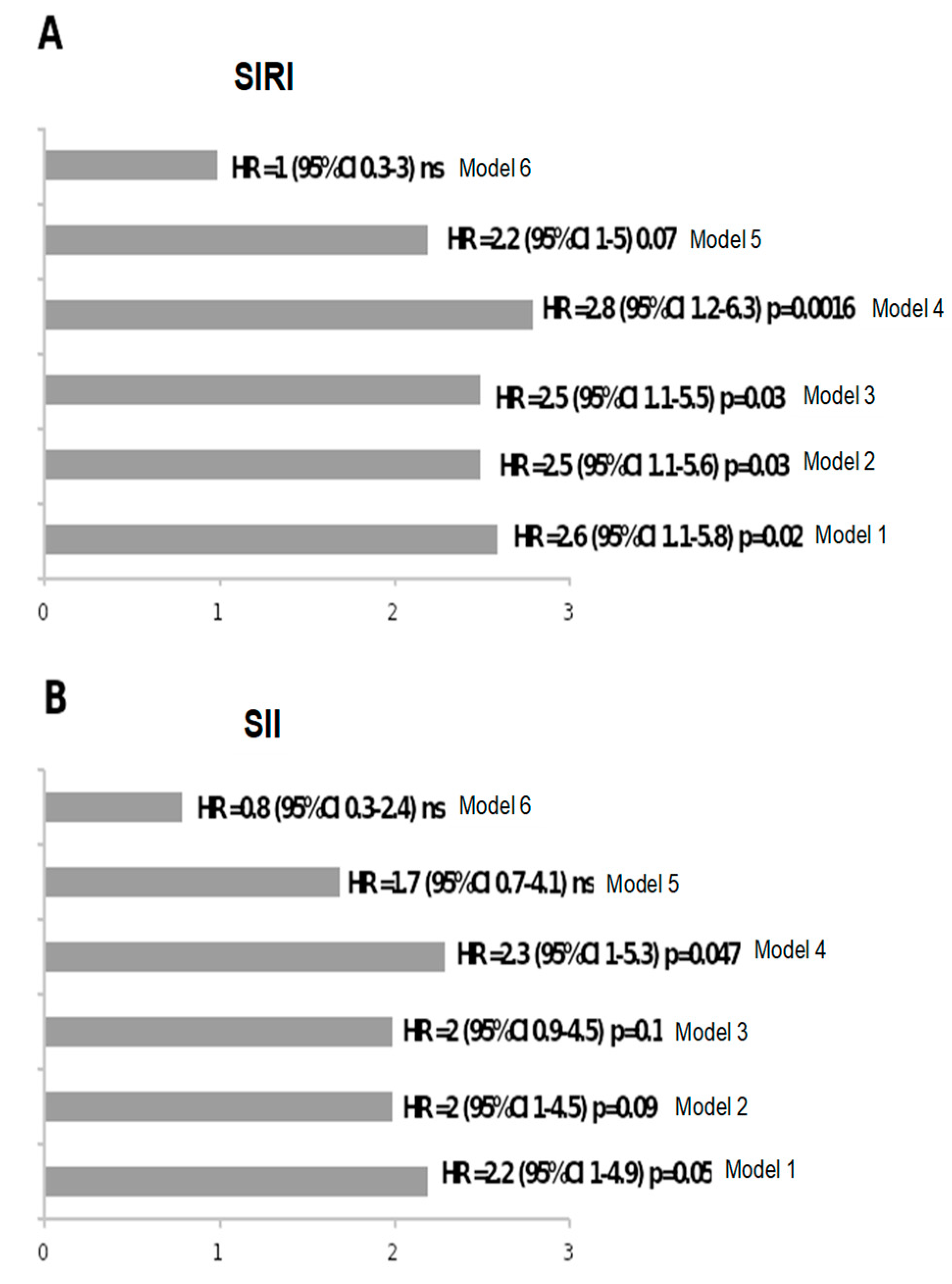
4.3. Follow-Up
5. Discussion
Limitations and Strengths of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Ma, X.; Shao, Q.; Yang, Z.; Wang, Y.; Gao, F.; Zhou, Y.; Yang, L.; Wang, Z. Prognostic Impact of Multiple Lymphocyte-Based Inflammatory Indices in Acute Coronary Syndrome Patients. Front. Cardiovasc. Med. 2022, 9, 811790. [Google Scholar] [CrossRef]
- Fan, W.; Wei, C.; Liu, Y.; Sun, Q.; Tian, Y.; Wang, X.; Liu, J.; Zhang, Y.; Sun, L. The Prognostic Value of Hematologic Inflammatory Markers in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. Clin. Appl. Thromb. Hemost. 2022, 28, 10760296221146183. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Zhuang, L.; Shen, Y.; Geng, Y.; Yu, S.; Chen, H.; Liu, L.; Meng, Z.; Wang, P.; Chen, Z. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer 2016, 122, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Meng, L.; Yang, Y.; Hu, X.; Zhang, R.; Li, X. Prognostic value of the pretreatment systemic immune-inflammation index in patients with prostate cancer: A systematic review and meta-analysis. J. Transl. Med. 2023, 21, 79. [Google Scholar] [CrossRef]
- Yang, Y.L.; Wu, C.H.; Hsu, P.F.; Chen, S.C.; Huang, S.S.; Chan, W.L.; Lin, S.J.; Chou, C.Y.; Chen, J.W.; Pan, J.P.; et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur. J. Clin. Investig. 2020, 50, e13230. [Google Scholar] [CrossRef] [PubMed]
- Mangalesh, S.; Dudani, S.; Mahesh, N.K. Development of a Novel Inflammatory Index to Predict Coronary Artery Disease Severity in Patients with Acute Coronary Syndrome. Angiology 2024, 75, 231–239. [Google Scholar] [CrossRef]
- Han, K.; Shi, D.; Yang, L.; Wang, Z.; Li, Y.; Gao, F.; Liu, Y.; Ma, X.; Zhou, Y. Prognostic value of systemic inflammatory response index in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Ann. Med. 2022, 54, 1667–1677. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, H. A nonlinear relationship between systemic inflammation response index and short-term mortality in patients with acute myocardial infarction: A retrospective study from MIMIC-IV. Front. Cardiovasc. Med. 2023, 10, 1208171. [Google Scholar] [CrossRef]
- Chen, Y.; Xie, K.; Han, Y.; Xu, Q.; Zhao, X. An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction. J. Inflamm. Res. 2023, 16, 4061–4071. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Q.; Wang, R.; Ji, H.; Chen, Y.; Quan, X.; Zhang, C. Systemic Immune-Inflammatory Index Predicts Clinical Outcomes for Elderly Patients with Acute Myocardial Infarction Receiving Percutaneous Coronary Intervention. Med. Sci. Monit. 2019, 25, 9690–9701. [Google Scholar] [CrossRef]
- Su, G.; Zhang, Y.; Xiao, R.; Zhang, T.; Gong, B. Systemic immune-inflammation index as a promising predictor of mortality in patients with acute coronary syndrome: A real-world study. J. Int. Med. Res. 2021, 49, 3000605211016274. [Google Scholar] [CrossRef]
- Tosu, A.R.; Kalyoncuoglu, M.; Biter, H.İ.; Cakal, S.; Selcuk, M.; Çinar, T.; Belen, E.; Can, M.M. Prognostic Value of Systemic Immune-Inflammation Index for Major Adverse Cardiac Events and Mortality in Severe Aortic Stenosis Patients after TAVI. Medicina 2021, 7, 588. [Google Scholar] [CrossRef]
- Gur, D.O.; Efe, M.M.; Alpsoy, S.; Akyüz, A.; Uslu, N.; Çelikkol, A.; Gur, O. Systemic Immune-Inflammatory Index as a Determinant of Atherosclerotic Burden and High-Risk Patients with Acute Coronary Syndromes. Arq. Bras. Cardiol. 2022, 119, 382–390. [Google Scholar]
- Yildiz, C.; Yuksel, Y.; Efe, S.C.; Altintas, M.S.; Katkat, F.; Ayca, B.; Karabulut, D.; Çağlar, F.N.T.; Köse, S. Value of systemic inflammation-response index in predicting contrast-induced nephropathy in patients with ST-elevation myocardial infarction. Acta Cardiol. 2023, 78, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Kelesoglu, S.; Yilmaz, Y.; Elcık, D.; Çetınkaya, Z.; Inanc, M.T.; Dogan, A.; Oguzhan, A.; Kalay, N. Systemic Immune Inflammation Index: A Novel Predictor of Contrast-Induced Nephropathy in Patients with Non-ST Segment Elevation Myocardial Infarction. Angiology 2021, 72, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Li, D.; Xu, T.; Chen, Z.; Shan, Y.; Zhao, L.; Fu, G.; Luan, Y.; Xia, S.; Zhang, W. Systemic Immune-Inflammation Index Predicts Contrast-Induced Acute Kidney Injury in Patients Undergoing Coronary Angiography: A Cross-Sectional Study. Front. Med. 2022, 9, 841601. [Google Scholar] [CrossRef]
- Zhu, Y.; Qiu, H.; Wang, Z.; Shen, G.; Li, W. Predictive value of systemic immune-inflammatory index combined with CHA2DS2-VASC score for contrast-induced acute kidney injury in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Int. Urol. Nephrol. 2023, 55, 2897–2903. [Google Scholar] [CrossRef]
- Guo, W.; Song, Y.; Sun, Y.; Du, H.; Cai, Y.; You, Q.; Fu, H.; Shao, L. Systemic immune-inflammation index is associated with diabetic kidney disease in Type 2 diabetes mellitus patients: Evidence from NHANES 2011–2018. Front. Endocrinol. 2022, 13, 1071465. [Google Scholar] [CrossRef]
- Li, X.; Wang, L.; Liu, M.; Zhou, H.; Xu, H. Association between neutrophil-to-lymphocyte ratio and diabetic kidney disease in type 2 diabetes mellitus patients: A cross-sectional study. Front. Endocrinol. 2024, 14, 1285509. [Google Scholar] [CrossRef]
- Zheng, H.; Yin, Z.; Luo, X.; Zhou, Y.; Zhang, F.; Guo, Z. Associations between systemic immunity-inflammation index and heart failure: Evidence from the NHANES 1999–2018. Int. J. Cardiol. 2024, 395, 131400. [Google Scholar] [CrossRef] [PubMed]
- Balci, K.; Erbay, İ.; Demirkan, B.; Balci, M.M.; Temizhan, A. The association of hemodynamic markers of right ventricular dysfunction with SII index and clinical outcomes in reduced ejection fraction heart failure. Medicine 2023, 102, e34809. [Google Scholar] [CrossRef] [PubMed]
- Chi, R.; Shan, X.; Guan, C.; Yang, H.; Wang, X.; Li, B.; Zhang, Q. Association between systemic inflammatory response index and left ventricular remodeling and systolic dysfunction in atrial fibrillation patients. BMC Cardiovasc. Disord. 2023, 23, 37. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction. Circulation 2018, 138, e618–e651. [Google Scholar]
- Michelucci, E.; Rocchiccioli, S.; Gaggini, M.; Ndreu, R.; Berti, S.; Vassalle, C. Ceramides and Cardiovascular Risk Factors, Inflammatory Parameters and Left Ventricular Function in AMI Patients. Biomedicines 2022, 10, 429. [Google Scholar] [CrossRef] [PubMed]
- Paradossi, U.; Taglieri, N.; Massarelli, G.; Palmieri, C.; De Caterina, A.R.; Bruno, A.G.; Taddei, A.; Nardi, E.; Ghetti, G.; Palmerini, T.; et al. Female gender and mortality in ST-segment-elevation myocardial infarction treated with primary PCI. J. Cardiovasc. Med. 2022, 23, 234–241. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Adatia, K.; Farag, M.F.; Gue, Y.X.; Srinivasan, M.; Gorog, D.A. Relationship of Platelet Reactivity and Inflammatory Markers to Recurrent Adverse Events in Patients with ST-Elevation Myocardial Infarction. Thromb. Haemost. 2019, 119, 1785–1794. [Google Scholar] [CrossRef]
- Mehu, M.; Narasimhulu, C.A.; Singla, D.K. Inflammatory Cells in Atherosclerosis. Antioxidants 2022, 11, 233. [Google Scholar] [CrossRef]
- Doran, A.C.; Lipinski, M.J.; Oldham, S.N.; Garmey, J.C.; Campbell, K.A.; Skaflen, M.D.; Cutchins, A.; Lee, D.J.; Glover, D.K.; Kelly, K.A.; et al. B-cell aortic homing and atheroprotection depend on Id3. Circ. Res. 2012, 110, e1–e12. [Google Scholar] [CrossRef]
- Biswas, M.; Suvarna, R.; Krishnan, S.V.; Devasia, T.; Shenoy Belle, V.; Prabhu, K. The mechanistic role of neutrophil lymphocyte ratio perturbations in the leading non communicable lifestyle diseases. F1000Res 2022, 11, 960. [Google Scholar] [CrossRef]
- Arı, E.; Köseoğlu, H.; Eroğlu, T. Predictive value of SIRI and SII for metastases in RCC: A prospective clinical study. BMC Urol. 2024, 24, 14. [Google Scholar] [CrossRef]
- Wenpei, G.; Yuan, L.; Liangbo, L.; Jingjun, M.; Bo, W.; Zhiqiang, N.; Yijie, N.; Lixin, L. Predictive value of preoperative inflammatory indexes for postoperative early recurrence of hepatitis B-related hepatocellular carcinoma. Front. Oncol. 2023, 13, 1142168. [Google Scholar] [CrossRef]
- Atasever Akkas, E.; Erdis, E.; Yucel, B. Prognostic value of the systemic immune-inflammation index, systemic inflammation response index, and prognostic nutritional index in head and neck cancer. Eur. Arch. Otorhinolaryngol. 2023, 280, 3821–3830. [Google Scholar] [CrossRef]
- Xu, M.; Chen, R.; Liu, L.; Liu, X.; Hou, J.; Liao, J.; Zhang, P.; Huang, J.; Lu, L.; Chen, L.; et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: The Dongfeng-Tongji cohort study. Atherosclerosis 2021, 323, 20–29. [Google Scholar] [CrossRef]
- Xia, Y.; Xia, C.; Wu, L.; Li, Z.; Li, H.; Zhang, J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and Risk of All-Cause Mortality and Cardiovascular Mortality: A 20-Year Follow-Up Cohort Study of 42,875 US Adults. J. Clin. Med. 2023, 12, 1128. [Google Scholar] [CrossRef]
- Jin, Z.; Wu, Q.; Chen, S.; Gao, J.; Li, X.; Zhang, X.; Zhou, Y.; He, D.; Cheng, Z.; Zhu, Y.; et al. The Associations of Two Novel Inflammation Indexes, SII and SIRI with the Risks for Cardiovascular Diseases and All-Cause Mortality: A Ten-Year Follow-Up Study in 85,154 Individuals. J. Inflamm. Res. 2021, 14, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Mo, C.; Li, Y.; Gui, C. Systemic immune-inflammation index associated with contrast-induced nephropathy after elective percutaneous coronary intervention in a case-control study. Coron. Artery Dis. 2023, 34, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Almeida, I.; Chin, J.; Santos, H.; Miranda, H.; Santos, M.; Sá, C.; Almeida, S.; Sousa, C.; Almeida, L. National Cardiology Data Collection Center, Portuguese Society of Cardiology, Coimbra, Portugal, National Register of Acute Coronary Syndromes Investigators. Prognostic value of brain natriuretic peptide in ST-elevation myocardial infarction patients: A Portuguese registry. Rev. Port. Cardiol. 2022, 41, 87–95. [Google Scholar] [PubMed]
- Zuo, H.; Xie, X.; Peng, J.; Wang, L.; Zhu, R. Predictive Value of Novel Inflammation-Based Biomarkers for Pulmonary Hypertension in the Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Anal. Cell. Pathol. 2019, 2019, 5189165. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; He, H.; Qiu, H.; Shen, G.; Wang, Z.; Li, W. Prognostic Value of Systemic Immune-Inflammation Index and NT-proBNP in Patients with Acute ST-Elevation Myocardial Infarction. Clin. Interv. Aging 2023, 18, 397–407. [Google Scholar] [CrossRef]
- Ząbczyk, M.; Ariëns, R.A.S.; Undas, A. Fibrin clot properties in cardiovascular disease: From basic mechanisms to clinical practice. Cardiovasc. Res. 2023, 119, 94–111. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Number | 105 |
| Age (years) | 70 ± 11 |
| Males/Females | 74 (70)/31 (30) |
| Diabetes | 20 (19) |
| Hypertension | 63 (60) |
| Dyslipidemia | 52 (49) |
| BMI (Kg/m2) | 27 ± 5 |
| Smoking history (current or former smoking habit) | 44 (43) |
| LVEF (%) | 48 ± 9 |
| BNP (ng/L) | 128 (51–245) |
| Creatinine (mg/dL)) | 1 ± 0.3 |
| Neutrophils (103/µL) | 6 (4.7–8.1) |
| Lymphocytes (103/µL) | 1.8 (1.4–2.1) |
| Monocytes (103/µL) | 0.8 (0.6–1) |
| Platelets (103/µL) | 234 ± 76 |
| Variable | Standard Coefficient | t-Value | p Value |
|---|---|---|---|
| Creatinine | 0.17 | 1.6 | ns |
| BNP | 0.26 | 2.5 | <0.05 |
| Variable | Standard Coefficient | t-Value | p Value |
|---|---|---|---|
| Creatinine | 0.28 | 2.7 | <0.01 |
| BNP | 0.15 | 1.3 | ns |
| Age | 0.1 | 0.8 | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchi, F.; Pylypiv, N.; Parlanti, A.; Storti, S.; Gaggini, M.; Paradossi, U.; Berti, S.; Vassalle, C. Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction. J. Clin. Med. 2024, 13, 1256. https://doi.org/10.3390/jcm13051256
Marchi F, Pylypiv N, Parlanti A, Storti S, Gaggini M, Paradossi U, Berti S, Vassalle C. Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction. Journal of Clinical Medicine. 2024; 13(5):1256. https://doi.org/10.3390/jcm13051256
Chicago/Turabian StyleMarchi, Federica, Nataliya Pylypiv, Alessandra Parlanti, Simona Storti, Melania Gaggini, Umberto Paradossi, Sergio Berti, and Cristina Vassalle. 2024. "Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction" Journal of Clinical Medicine 13, no. 5: 1256. https://doi.org/10.3390/jcm13051256
APA StyleMarchi, F., Pylypiv, N., Parlanti, A., Storti, S., Gaggini, M., Paradossi, U., Berti, S., & Vassalle, C. (2024). Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction. Journal of Clinical Medicine, 13(5), 1256. https://doi.org/10.3390/jcm13051256