
Assessing the Effectiveness of Rehabilitation Interventions through the World Health Organization Disability Assessment Schedule 2.0 on Disability—A Systematic Review

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
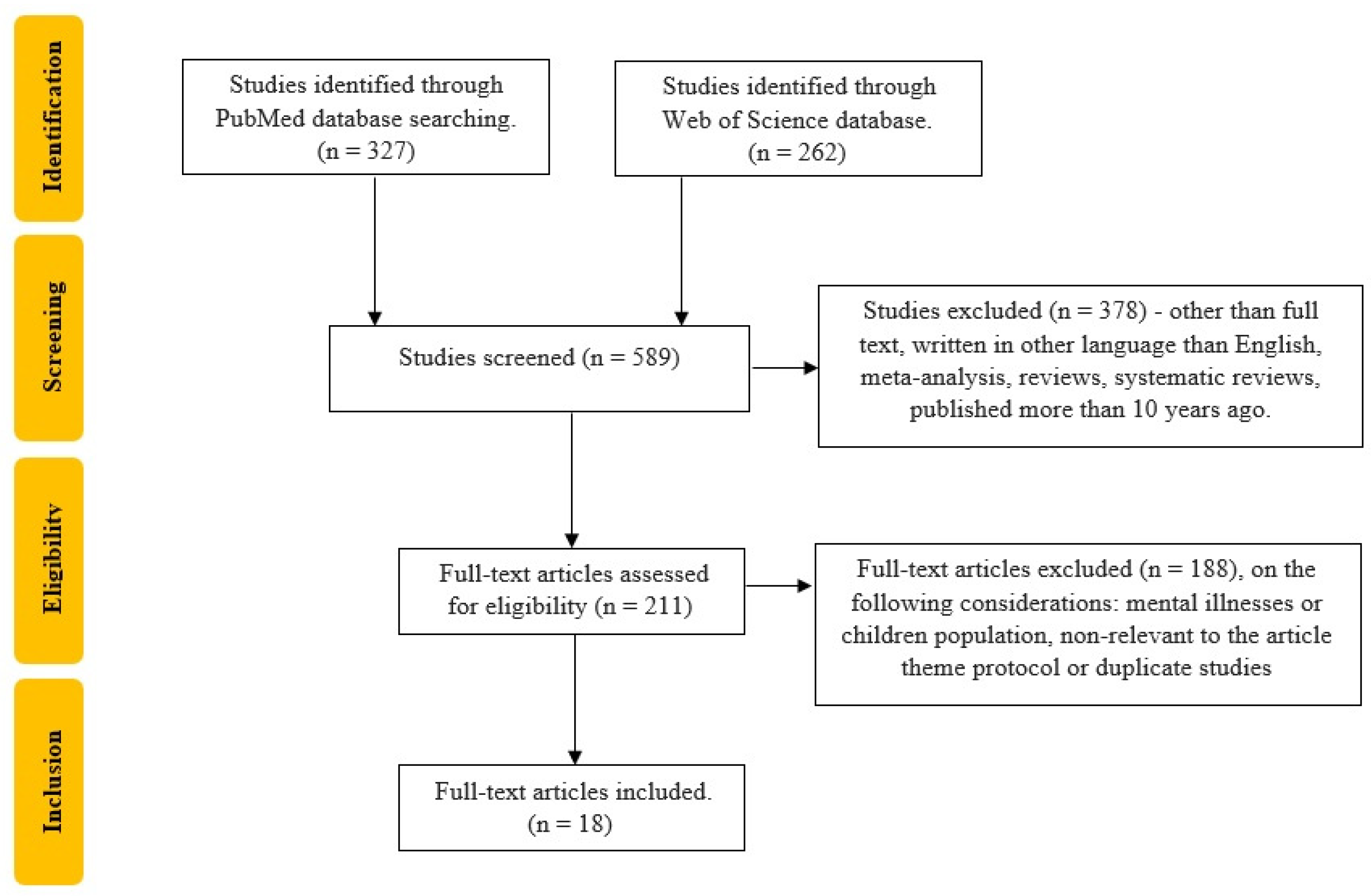
2.1. Research Question and Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
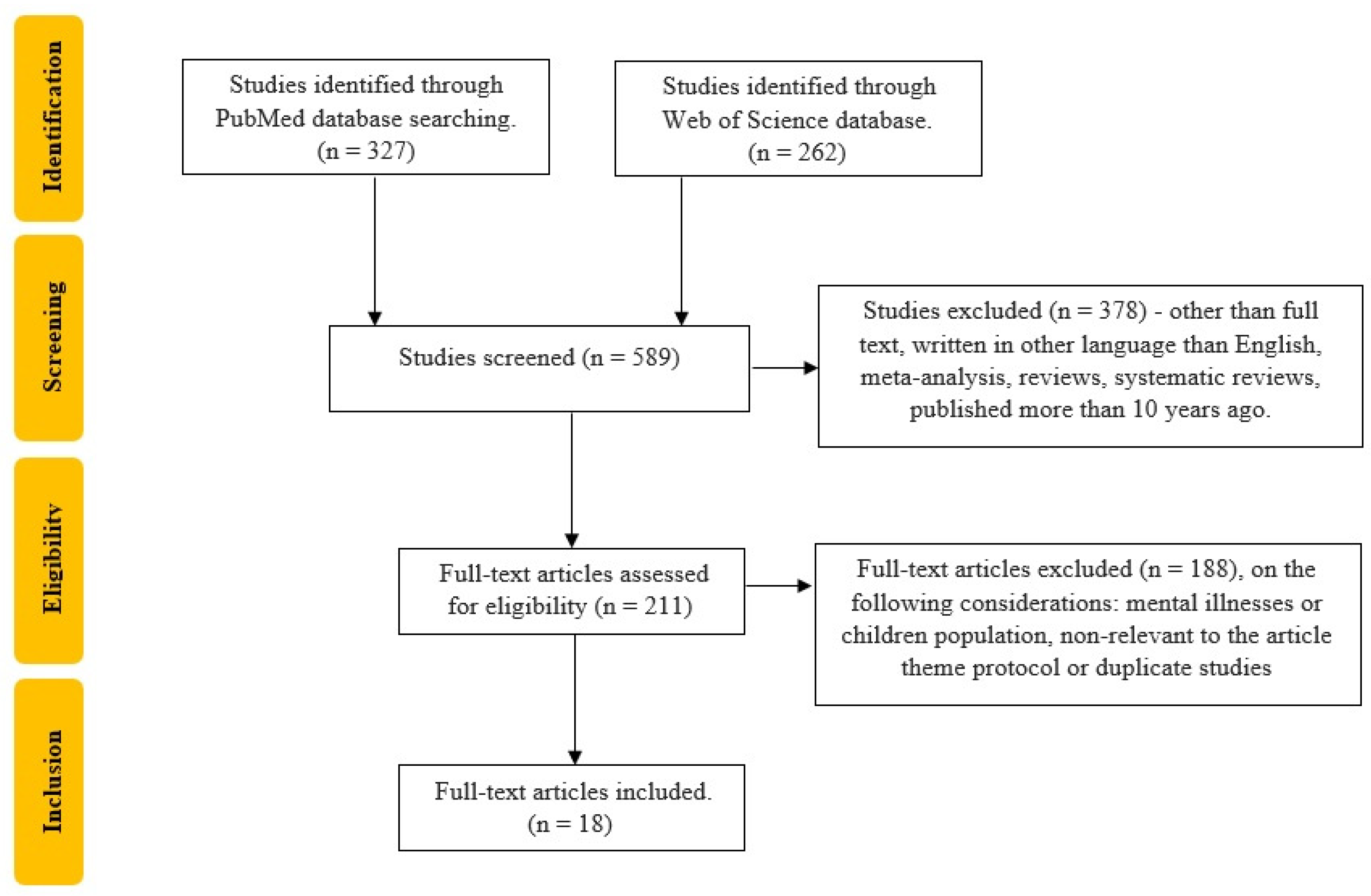
2.4. Selection of Studies
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Strategy for Data Synthesis
3. Results
- Disease-specific scales: PDQ-39 (Parkinson’s Disease Questionnaire-39) for PD [32];
- Usability and acceptance scales: SUS (System Usability Scale), TAM3 (Technology Acceptance Model 3), and SUTAQ (Service User Technology Acceptance Model) [23];
- Physical activity and diet measures: Physical Activity Questionnaire, DASH-Q (Dietary Approaches to Stop Hypertension Quality questionnaire), IPAQ-SF (International Physical Activity Questionnaire, short version) [29];
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007.
- Fung, K.W.; Xu, J.; Bodenreider, O. The New International Classification of Diseases 11th Edition: A Comparative Analysis with ICD-10 and ICD-10-CM. J. Am. Med. Inform. Assoc. 2020, 27, 738–746. [Google Scholar] [CrossRef]
- WHO. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease; WHO: Geneva, Switzerland, 1994.
- Pfeiffer, D. The ICIDH and the Need for Its Revision. Disabil. Soc. 1998, 13, 503. [Google Scholar] [CrossRef]
- Bickenbach, J. Ethics, Disability and the International Classification of Functioning, Disability and Health. Am. J. Phys. Med. Rehabil. 2012, 91, S163–S167. [Google Scholar] [CrossRef]
- Officer, A.; Posarac, A. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011.
- Sen, A. Health: Perception versus Observation: Self Reported Morbidity Has Severe Limitations and Can Be Extremely Misleading. BMJ 2002, 324, 860–861. [Google Scholar] [CrossRef]
- Albrecht, G.L.; Devlieger, P.J. The Disability Paradox: High Quality of Life against All Odds. Soc. Sci. Med. 1999, 48, 977–988. [Google Scholar] [CrossRef]
- Üstün, T.B. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010.
- Federici, S.; Meloni, F. WHODAS II: Disability Self-Evaluation in the ICF Conceptual Frame. In International Encyclopedia of Rehabilitation; Stone, J.H., Blouin, M., Eds.; Center for International Rehabilitation Research Information and Exchange: Buffalo, NY, USA, 2010; pp. 1–22. Available online: https://www.researchgate.net/publication/228079041_WHODAS_II_Disability_self-evaluation_in_the_ICF_conceptual_frame (accessed on 18 February 2024).
- Federici, S.; Bracalenti, M.; Meloni, F.; Luciano, J.V. World Health Organization Disability Assessment Schedule 2.0: An International Systematic Review. Disabil. Rehabil. 2017, 39, 2347–2380. [Google Scholar] [CrossRef]
- Zanca, J.M.; Dijkers, M.P. Describing What We Do: A Qualitative Study of Clinicians’ Perspectives on Classifying Rehabilitation Interventions. Arch. Phys. Med. Rehabil. 2014, 95, S55–S65. [Google Scholar] [CrossRef]
- Wade, D.T. Describing Rehabilitation Interventions. Clin. Rehabil. 2005, 19, 811–818. [Google Scholar] [CrossRef]
- Potcovaru, C.-G.; Filip, P.V.; Neagu, O.-M.; Diaconu, L.S.; Salmen, T.; Cinteză, D.; Pantea Stoian, A.; Bobirca, F.; Berteanu, M.; Pop, C. Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review. J. Clin. Med. 2023, 12, 4713. [Google Scholar] [CrossRef]
- Poenaru, D.; Sandulescu, M.I.; Cinteza, D. Pain Modulation in Chronic Musculoskeletal Disorders: Botulinum Toxin, a Descriptive Analysis. Biomedicines 2023, 11, 1888. [Google Scholar] [CrossRef]
- Poenaru, D.; Ojoga, F.; Sandulescu, M.; Cinteza, D. Conservative Therapy in Ulnar Neuropathy at the Elbow. Exp. Ther. Med. 2022, 24, 517. [Google Scholar] [CrossRef]
- Moldoveanu, A.; Ferche, O.-M.; Moldoveanu, F.; Lupu, R.G.; Cinteză, D.; Irimia, D.C.; Toader, C. The TRAVEE System for a Multimodal Neuromotor Rehabilitation. IEEE Access 2019, 7, 8151–8171. [Google Scholar] [CrossRef]
- Nasui, B.A.; Talaba, P.; Nasui, G.A.; Sirbu, D.M.; Borda, I.M.; Pop, A.L.; Ciortea, V.M.; Irsay, L.; Purcar-Popescu, A.I.; Cinteza, D. The Influence of Diet and Physical Activity on Oxidative Stress in Romanian Females with Osteoarthritis. Nutrients 2022, 14, 4159. [Google Scholar] [CrossRef]
- Munteanu, C.; Delia, C. Cercetarea Ştiinţificã a Factorilor Naturali Terapeutici; Balneara: Bucharest, Romania, 2011. [Google Scholar]
- Manolescu, B.N.; Berteanu, M.; Cintezã, D. Effect of the Nutritional Supplement ALAnerv® on the Serum PON1 Activity in Post-Acute Stroke Patients. Pharmacol. Rep. 2013, 65, 743–750. [Google Scholar] [CrossRef]
- Dabrowska, M.; Pastucha, D.; Janura, M.; Tomaskova, H.; Honzikova, L.; Banikova, S.; Filip, M.; Fiedorova, I. Effect of Virtual Reality Therapy on Quality of Life and Self-Sufficiency in Post-Stroke Patients. Medicina 2023, 59, 1669. [Google Scholar] [CrossRef]
- Fukuta, Y.; Arizono, S.; Tanaka, S.; Kawaguchi, T.; Tsugita, N.; Fuseya, T.; Magata, J.; Tawara, Y.; Segawa, T. Effects of Real-Time Remote Cardiac Rehabilitation on Exercise Capacity and Quality of Life: A Quasi-Randomised Controlled Trial. BMC Geriatr. 2023, 23, 388. [Google Scholar] [CrossRef]
- Rossetto, F.; Borgnis, F.; Isernia, S.; Foglia, E.; Garagiola, E.; Realdon, O.; Baglio, F.; SIDERA B Consortium. System Integrated Digital Empowering and teleRehabilitation to Promote Patient Activation and Well-Being in Chronic Disabilities: A Usability and Acceptability Study. Front. Public Health 2023, 11, 1154481. [Google Scholar] [CrossRef]
- Kilkki, M.; Stolt, M.; Rannikko, S.; Pasanen, M.; Tarvonen-Schröder, S. Patient- and Proxy-Perceptions on Functioning after Stroke Rehabilitation Using the 12-Item WHODAS 2.0: A Longitudinal Cohort Study. Disabil. Rehabil. 2023, 46, 783–792. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, L.; Quigley, K.; Lu, S.; Litke, D.; Rath, J.; Lange, G.; Santos, S.; Anastasides, N.; Petrakis, B.; Greenberg, L.; et al. Effect of Problem-Solving Treatment on Self-Reported Disability Among Veterans with GulfWar Illness A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2245272. [Google Scholar] [CrossRef] [PubMed]
- Jen, H.; Kao, C.; Chang, K.; Yen, C.; Liao, H.; Chi, W.; Chung, W.; Liou, T. Assessment of Functioning Using the WHODAS 2.0 among People with Stroke in Taiwan: A 4-Year Follow-up Study. Ann. Phys. Rehabil. Med. 2021, 64, 101442. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Gu, M.; He, C.; Xiong, C.; Xu, J.; Huang, X. Robot-Assisted Arm Training in Stroke Individuals with Unilateral Spatial Neglect: A Pilot Study. Front. Neurol. 2021, 12, 691444. [Google Scholar] [CrossRef]
- Campbell, E.; Hynynen, J.; Burger, B.; Vainionpää, A.; Ala-Ruona, E. Vibroacoustic Treatment to Improve Functioning and Ability to Work: A Multidisciplinary Approach to Chronic Pain Rehabilitation. Disabil. Rehabil. 2021, 43, 2055–2070. [Google Scholar] [CrossRef]
- Nguyen, L.; Do, B.; Vu, D.; Pham, K.; Vu, M.; Nguyen, H.; Tran, T.; Le, H.; Nguyen, T.; Nguyen, Q.; et al. Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients. Nutrients 2021, 13, 1641. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Chafranskaia, A.; Lopez, C.; Maganti, M.; Bernstein, L.; Chang, E.; Langelier, D.; Obadia, M.; Edwards, B.; Oh, P.; et al. CaRE @ Home: Pilot Study of an Online Multidimensional Cancer Rehabilitation and Exercise Program for Cancer Survivors. J. Clin. Med. 2020, 9, 3092. [Google Scholar] [CrossRef]
- Hustoft, M.; Biringer, E.; Gjesdal, S.; Moen, V.; Assmus, J.; Hetlevik, O. The Effect of Team Collaboration and Continuity of Care on Health and Disability among Rehabilitation Patients: A Longitudinal Survey-Based Study from Western Norway. Qual. Life Res. 2019, 28, 2773–2785. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, D.; Trippo, K.; Duarte, G.; Neto, M.; Santos, K.; Oliveira, J. The Effects of Functional Training, Bicycle Exercise, and Exergaming on Walking Capacity of Elderly Patients with Parkinson Disease: A Pilot Randomized Controlled Single-Blinded Trial. Arch. Phys. Med. Rehabil. 2018, 99, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Ya, L.; Petrini, M.A. Effects of a Home-Based Resistance Exercise in Chinese Individuals Living with Physical Disability: Resistance Exercise on PWPD. Rehabil. Nurs. J. 2018, 43, 174–182. [Google Scholar] [CrossRef]
- Galli, T.; Mirata, P.; Foglia, E.; Croce, D.; Porazzi, E.; Ferrario, L.; Ricci, E.; Garagiola, E.; Pagani, R.; Banfi, G. A Comparison between WHODAS 2.0 and Modified Barthel Index: Which Tool Is More Suitable for Assessing the Disability and the Recovery Rate in Orthopedic Rehabilitation? Clin. Outcomes Res. 2018, 10, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Teixeira-Machado, L.; Azevedo-Santos, I.; DeSantana, J. Dance Improves Functionality and Psychosocial Adjustment in Cerebral Palsy: A Randomized Controlled Clinical Trial. Am. J. Phys. Med. Rehabil. 2017, 96, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Shahbazi, M.; Foroughan, M.; Rahgozar, M.; Roghani, R. Effects of adult day care services on disability in older persons: Evaluation of a designed service package in Iran. J. Rehabil. Med. 2016, 48, 719–724. [Google Scholar] [CrossRef]
- Pettersson, I.; Hagberg, L.; Fredriksson, C.; Hermansson, L.N. The Effect of Powered Scooters on Activity, Participation and Quality of Life in Elderly Users. Disabil. Rehabil. Assist. Technol. 2016, 11, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Martinez, O.; Jometón, A.; Pérez, M.; Lázaro, E.; Amayra, I.; López-Paz, J.F.; Oliva, M.; Parada, P.; Berrocoso, S.; Iglesias, A. Effectiveness of Teleassistance at Improving Quality of Life in People with Neuromuscular Diseases. Span. J. Psychol. 2014, 17, E86. [Google Scholar] [CrossRef] [PubMed]
- Meade, M.A.; Mahmoudi, E.; Lee, S.-Y. The Intersection of Disability and Healthcare Disparities: A Conceptual Framework. Disabil. Rehabil. 2015, 37, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.; Marin, J.J.; Blanco, T.; de la Torre, J.; Salcedo, I.; Martitegui, E. Is My Patient Improving? Individualized Gait Analysis in Rehabilitation. Appl. Sci. 2020, 10, 8558. [Google Scholar] [CrossRef]
- Sewell, L.; Singh, S.J.; Williams, J.E.; Collier, R.; Morgan, M.D. Can Individualized Rehabilitation Improve Functional Independence in Elderly Patients with COPD? Chest 2005, 128, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Franssen, F.M.; Alter, P.; Bar, N.; Benedikter, B.J.; Iurato, S.; Maier, D.; Maxheim, M.; Roessler, F.K.; Spruit, M.A.; Vogelmeier, C.F.; et al. Personalized Medicine for Patients with COPD: Where Are We? Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1465–1484. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Siewiorek, D.P.; Smailagic, A.; Bernardino, A.; Badia, S.B. Towards Personalized Interaction and Corrective Feedback of a Socially Assistive Robot for Post-Stroke Rehabilitation Therapy. In Proceedings of the 2020 29th IEEE International Conference on Robot and Human Interactive Communication (RO-MAN), Naples, Italy, 31 August–4 September 2020; pp. 1366–1373. [Google Scholar] [CrossRef]
- Cheng, T.-M. The Taiwanese Health Care System. Int. Profiles Health Care Syst. 2020, 201. Available online: https://www.researchgate.net/profile/Adriano-Massuda-2/publication/352750082_The_Brazilian_Health_Care_System/links/60d63a1e299bf1ea9ebe48df/The-Brazilian-Health-Care-System.pdf#page=199 (accessed on 18 February 2024).
- Fellinghauer, B.; Reinhardt, J.D.; Stucki, G.; Bickenbach, J. Explaining the Disability Paradox: A Cross-Sectional Analysis of the Swiss General Population. BMC Public Health 2012, 12, 655. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Andresen, E.M.; Nosek, M.A.; Krahn, G.L. Response Shift Theory: Important Implications for Measuring Quality of Life in People with Disability. Arch. Phys. Med. Rehabil. 2007, 88, 529–536. [Google Scholar] [CrossRef]
- Potcovaru, C.G.; Salmen, T.; Chitu, M.C.; Dima, V.; Mihai, M.B.; Bohiltea, R.E.; Cinteza, D.; Berteanu, M. Assessment Tools of Disability Status after Stroke. Rom. J. Neurol. 2022, 21, 208. [Google Scholar] [CrossRef]
- Cook, C.; Bakker, K. Water Security: Debating an Emerging Paradigm. Glob. Environ. Chang. 2012, 22, 94–102. [Google Scholar] [CrossRef]
- Ghaneh, B.; Saeed-Banadaky, S.H.; Rahaei, Z.; Rezaeipandari, H.; Mohiti Ardakani, E. Disability and Self-Care among Elders in Yazd. Elder. Health J. 2016, 2, 39–44. [Google Scholar]
- Haylett, R.; Gustafson, O. A feasibility study to assess pre-admission status and six month outcomes of major trauma patients admitted to an intensive care unit, using the WHO DAS 2.0. J. Crit. Care 2018, 48, 140–144. [Google Scholar] [CrossRef]
- Tudosie, A.; Popescu, S.; Cinteza, D.; Romanescu, S.; Roxana, P.; Sandu, A.; Romila, A.; Tiniuc, A.M.; Florea, R. Rehabilitation in a Patient with Replantation of Amputated Distal Leg. Maedica 2011, 6, 36. [Google Scholar]
- Groce, N. Everyone Here Spoke Sign Language. Beginning with Disability—A Primer; Routledge: Abingdon-on-Thames, UK, 2017; pp. 68–77. [Google Scholar]
- Ozkaraoglu, D.K.; Tarakci, D.; Algun, Z.C. Comparison of Two Different Electrotherapy Methods in Low Back Pain Treatment. J. Back Musculoskelet. Rehabil. 2020, 33, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Tousignant-Laflamme, Y.; Martel, M.O.; Joshi, A.B.; Cook, C.E. Rehabilitation Management of Low Back Pain—It’s Time to Pull It All Together! J. Pain Res. 2017, 10, 2373–2385. [Google Scholar] [CrossRef]
- Dehem, S.; Gilliaux, M.; Stoquart, G.; Detrembleur, C.; Jacquemin, G.; Palumbo, S.; Frederick, A.; Lejeune, T. Effectiveness of Upper-Limb Robotic-Assisted Therapy in the Early Rehabilitation Phase after Stroke: A Single-Blind, Randomised, Controlled Trial. Ann. Phys. Rehabil. Med. 2019, 62, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.F.; Snir, O.; Liebermann, D.G.; Weingarden, H.; Weiss, P.L. Virtual Reality Versus Conventional Treatment of Reaching Ability in Chronic Stroke: Clinical Feasibility Study. Neurol. Ther. 2012, 1, 3. [Google Scholar] [CrossRef]
- Lakka, T.A.; Laaksonen, D.E. Physical Activity in Prevention and Treatment of the Metabolic Syndrome. Appl. Physiol. Nutr. Metab. 2007, 32, 76–88. [Google Scholar] [CrossRef]
- Radu, F.; Potcovaru, C.-G.; Salmen, T.; Filip, P.V.; Pop, C.; Fierbințeanu-Braticievici, C. The Link between NAFLD and Metabolic Syndrome. Diagnostics 2023, 13, 614. [Google Scholar] [CrossRef]
- Lavoie, V.; Bouchard, M.; Turcotte, S.; Tousignant, M. Telerehabilitation for Individuals with Parkinson’s Disease and a History of Falls: A Pilot Study. Physiother. Can. 2021, 73, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A.; et al. Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients’ Rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef] [PubMed]
- Ayele, T.A.; Alamneh, T.S.; Shibru, H.; Sisay, M.M.; Yilma, T.M.; Melak, M.F.; Bisetegn, T.A.; Belachew, T.; Haile, M.; Zeru, T. Effect of COVID-19 Pandemic on Missed Medical Appointment among Adults with Chronic Disease Conditions in Northwest Ethiopia. PLoS ONE 2022, 17, e0274190. [Google Scholar] [CrossRef]
- Bittner, A.K.; Yoshinaga, P.D.; Rittiphairoj, T.; Li, T. Telerehabilitation for People with Low Vision. Cochrane Database Syst. Rev. 2023, 1. [Google Scholar] [CrossRef]
- Oh-Park, M.; Lew, H.L.; Raghavan, P. Telerehabilitation for Geriatrics. Phys. Med. Rehabil. Clin. 2021, 32, 291–305. [Google Scholar] [CrossRef]
- Davidoff, C.; Maltser, S. Chapter 6—Telerehabilitation in Cancer Care. In Telerehabilitation; Alexander, M., Ed.; Elsevier: New Delhi, India, 2022; pp. 71–89. [Google Scholar] [CrossRef]
- Lamoth, C.J.C.; Alingh, R.; Caljouw, S.R. Exergaming for Elderly: Effects of Different Types of Game Feedback on Performance of a Balance Task. In Annual Review of Cybertherapy and Telemedicine 2012; IOS Press: Amsterdam, The Netherlands, 2012; Volume 2012, pp. 103–107. [Google Scholar] [CrossRef]
- Hou, H.-Y.; Chen, J.; Hai, L.; Wang, P.; Zhang, J.-X.; Li, H.-J. Effects of Exergame and Bicycle Exercise Intervention on Blood Pressure and Executive Function in Older Adults with Hypertension: A Three-Group Randomized Controlled Study. Exp. Gerontol. 2023, 173, 112099. [Google Scholar] [CrossRef]
- Cinteza, D. Update in Physical Medicine and Rehabilitation: New Technologies and Robots versus Classical Training in Gait Rehabilitation after Stroke. Maedica 2011, 6, 160. [Google Scholar]
- Shahabi, S.; Kiekens, C.; Etemadi, M.; Mojgani, P.; Teymourlouei, A.A.; Lankarani, K.B. Integrating Rehabilitation Services into Primary Health Care: Policy Options for Iran. BMC Health Serv. Res. 2022, 22, 1317. [Google Scholar] [CrossRef]
- Hagberg, L.; Hermansson, L.; Fredriksson, C.; Pettersson, I. Cost-Effectiveness of Powered Mobility Devices for Elderly People with Disability. Disabil. Rehabil. Assist. Technol. 2017, 12, 115–120. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Author (Reference) | Selection | Comparability | Outcome | Total Score | Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Follow-Up Long Enough for Outcomes to Occur | Adequacy of Follow-Up of Cohorts | |||
| Dabrowska et al. [21], 2023 | * | * | * | - | * | * | - | * | 6 | good |
| Fukuta et al. [22], 2023 | * | * | * | * | * | * | - | * | 7 | good |
| Rossetto et al. [23], 2023 | * | - | * | * | - | * | - | * | 5 | fair |
| Kilkki et al. [24], 2023 | * | * | * | * | * | * | - | * | 7 | good |
| McAndrew et al. [25], 2022 | * | - | * | * | * | * | - | * | 6 | good |
| Jen et al. [26], 2021 | * | - | * | * | - | * | * | * | 6 | good |
| Chen et al. [27], 2021 | * | * | * | * | * | * | * | * | 8 | good |
| Campbell et al. [28], 2019 | * | - | * | * | - | * | * | * | 6 | good |
| Nguyen et al. [29], 2021 | * | - | * | * | - | * | * | * | 6 | good |
| MacDonald et al. [30], 2020 | * | - | * | * | - | * | * | * | 6 | good |
| Hustoft et al. [31], 2019 | * | - | * | * | - | * | * | * | 6 | good |
| Ferraz et al. [32], 2018 | * | - | * | * | - | * | * | * | 6 | good |
| Ya and Petrini [33], 2017 | * | * | * | * | - | * | * | * | 7 | good |
| Galli et al. [34], 2018 | * | * | * | * | - | * | * | * | 7 | good |
| Teixeira-Machado et al. [35], 2017 | * | * | * | * | - | * | * | * | 7 | good |
| Shahbazi et al. [36], 2016 | * | * | * | * | * | * | * | * | 8 | good |
| Petterson et al. [37], 2015 | * | - | * | * | - | * | * | * | 6 | good |
| Martinez et al. [38], 2014 | * | * | * | * | * | * | * | * | 8 | good |
| Author (Reference) | Country | WHODAS 2.0 Items | Type of Study | Number of Patients | Mean Age in Years (SD) | The Condition That Led to Disability |
|---|---|---|---|---|---|---|
| Dabrowska et al. [21], 2023 | Czech Republic | 36 items, interview | RCT | 50 | IG 59.36; CG 62.96 | Ischaemic stroke in the arteria cerebri media |
| Fukuta et al. [22], 2023 | Japan | 12 items | Quasi-RCT | 31 | IG 72.2 (10.4); CG 77.3 (4.8) | CVD |
| Rossetto et al. [23], 2023 | Italy | 36 items | Usability and acceptability study—user experience research | 112 | 70.6 | CVD CHF PD COPD |
| Kilkki et al. [24], 2023 | Finland | 12 items (self and proxy) | Longitudinal cohort study | 65 | 62.7 | Stroke (ischemic, ICH, SAH) |
| McAndrew et al. [25], 2022 | United States | 12 items at screening, 36 items at 4, 12 weeks and 6 months | Multicentre RCT | 268 | 52.9 (7.3) | Gulf War illness and disability |
| Jen et al. [26], 2021 | Taiwan | 36 items | Longitudinal follow-up study | 3506 | 62.2 (12.5) | Stroke |
| Chen et al. [27], 2021 | China | 36 items | Assessor-blinded, prospective, pilot RCT | 20 | IG 46.2 (7); CG 48.6 (9.95) | Right-hemisphere stroke with left-sided unilateral spatial neglect |
| Campbell et al. [28], 2019 | Finland | 12 items, self-completed | Mixed methods | 4 | 43.25 (11.03) | Chronic pain and potential comorbid depressive and anxious symptoms |
| Nguyen et al. [29], 2021 | Vietnam | 12 items | Cross-sectional | 951 | Not reported | Stroke and comorbid conditions |
| MacDonald et al. [30], 2020 | Canada | 12 items | Mixed-method pilot study | 35 | 55 (15.9) | Cancer |
| Hustoft et al. [31], 2019 | Norway | 36 items | Longitudinal survey-based design | 701 | Not reported | Cancer, disease of the nervous system/musculoskeletal system/circulatory system |
| Ferraz et al. [32], 2018 | Brazil | 36 items | Randomized, controlled, single-blinded | 62 | 69 (5) | Elderly patients with PD |
| Ya and Petrini [33], 2017 | China | 36 items | Quasi-experimental nonrandomized trial | 24 | IG 48.69 (11.10); CG 47.73 (10.82) | Polio, traumatic injury, born with disability, CP, spastic paraplegia |
| Galli et al. [34], 2018 | Italy | 36 items, 12-item version | Prospective multicentre observational study | 80 (48 hip prostheses, 32 knee prostheses) | 70.1 (1.067) | Elective hip or knee arthroplasty |
| Teixeira-Machado et al. [35], 2017 | Brazil | 12 items | RCT | 26 | CG 18 (3.46); IG 17.07 (2.36) | CP |
| Shahbazi et al. [36], 2016 | Iran | 36 items | Case control | 92 (46 + 46) | 68.53 (6.1) | Chronic disease, older people, frailty |
| Petterson et al. [37], 2015 | Sweden | 36 items | Prospective study | 45 | Men 79.1 (5.76); women 74.3 (7.11) | Old individuals with mobility limitations |
| Martinez et al. [38], 2014 | Spain | 36 items | Quasi-experimental study with a pre-test and post-test design | 45 (21 CG, 24 EG) | Not reported | NDs MG, FSHD, BMD, LGMD |
| Author (Reference) | Rehabilitation Intervention | Time of Evaluation | WHODAS 2.0 IG | WHODAS 2.0 CG | WHODAS 2.0 | p | Evaluation Tools |
|---|---|---|---|---|---|---|---|
| Dabrowska et al. [21], 2023 | IG = VR + CnvT CG = CnvT | Baseline | 31.5 (18–62.6) | 27.4 (17.2–36.8) | NR | 0.261 | MMSE BI EBI BBS WHODAS 2.0 FAC |
| After the intervention | 22.6 (11.3–50.7) | 21.6 (15.3–30.6) | NR | 0.740 | |||
| 4 weeks after the intervention | 20.1 (9.2–43.8) | 20.6 (15.1–29.2) | NR | 0.996 | |||
| Fukuta et al. [22], 2023 | IG = remote CR for 12 weeks CG = hospital-based CR for 12 weeks | Baseline | 21.6 ± 14.3 | 19.3 ± 21.8 | NR | 0.06 | WHOQOL-BREF WHODAS 2.0 |
| CG baseline vs. 12 weeks after therapy | NR | NR | 12.3 ± 7.4 | 0.31 | |||
| IG baseline vs. 12 weeks after therapy | NR | NR | 21.5 ± 23 | <0.05 | |||
| Rossetto et al. [23], 2023 | Telerehabilitation program—SIDERA^B | Baseline (PD, COPD, CHF) | NR | NR | 15.95 | 0.346 | WHODAS 2.0 SUS TAM3 SUTAQ |
| Kilkki et al. [24], 2023 | Rehabilitation, self-perceived | Discharge Md (IQR) | 15.0 (14) | 0.004 | WHODAS 2.0 mRS FIM | ||
| 9–50 month Md (IQR) | 9.00 (18) | ||||||
| Rehabilitation, proxy-perceived | Discharge Md (IQR) | 20.0 (22) | <0.00001 | ||||
| 9–50 month Md (IQR) | 10.0 (21) | ||||||
| McAndrew et al. [25], 2022 | IG = PST CG = HE | Baseline mean (SE) | 46.7 (1.9) | 45.1 (1.9) | NR | WHODAS 2.0 Problem-solving inventory 3-item pain scale Pain Disability Index Fatigue Severity Scale | |
| 4 weeks | 42.5 (2.0) | 44.6 (2.0) | NR | ||||
| 12 weeks | 43.9 (2.0) | 42.8 (2.0) | 0.78 | ||||
| 6 months | 44.1 (2.2) | 46.2 (2.1) | 0.04 | ||||
| Jen et al. [26], 2021 | Existing Taiwanese healthcare system services | Baseline | 49.8 | <0.05 | WHODAS 2.0 | ||
| 4 years | 47.3 | ||||||
| Chen et al. [27], 2021 | IG = RAT CG = CnvT | Baseline (SD) | 122.10 (10.84) | 124 (11.43) | 0.71 | MoCA BIT-C CBS FMA-UE MBI WHODAS 2.0 | |
| 4 weeks (SD) | 98.60 (8.70) | 107.80 (11.70) | NR | ||||
| Campbell et al. [28], 2019 | Vibroacoustic treatment Self-care treatment | Phase I beginning | P1-17 | WHODAS 2.0 VAS Beck’s Depression Inventory-II Hospital Anxiety and Depression Scale | |||
| P2-22 | |||||||
| P3-25 | |||||||
| P4-11 | |||||||
| Phase I ending | P1-17 | ||||||
| P2-20 | |||||||
| P3-12 | |||||||
| P4-8 | |||||||
| Phase III beginning | P1-17 | ||||||
| P2-28 | |||||||
| P3-9 | |||||||
| P4-9 | |||||||
| Phase III ending | P1-18 | ||||||
| P2-23 | |||||||
| P3-5 | |||||||
| P4-5 | |||||||
| Follow-up | P1-19 | ||||||
| P2-28 | |||||||
| P3-10 | |||||||
| P4-9 | |||||||
| Nguyen et al. [29], 2021 | IG = Diet-quality modifications CG = PA | 32.3 (13.5) | Physical Activity Questionnaire, short version DASH-Q IPAQ-SF CCI | ||||
| MacDonald et al. [30], 2020 | CaRE@Home intervention | Baseline | 9.84 (1.14) | NR | WHODAS 2.0 GSLTPAQ iMTA PCQ 6 MWT Grip strength BMI Resting heart rate Blood pressure | ||
| 8-weeks post-intervention | 8.17 (1.01) | 0.03 | |||||
| 3 months post-intervention | 7.56 (1.10) | 0.008 | |||||
| Hustoft et al. [31], 2019 | 3-week rehabilitation process | Baseline | 28.6 (15.9) | NR | WHODAS 2.0 EQ-VAS NCQ-N | ||
| 1 year | 24.1 (15.9) | ||||||
| Ferraz et al. [32], 2018 | Functional training | Baseline | 73.3 (22.0) | 0.018 | 6MWT 10MWT SRT BMI PDQ-39 WHODAS 2.0 15-item Geriatric Depression Scale | ||
| 8 weeks | 63.91 (14.0) | ||||||
| Bicycle exercise | Baseline | 66.2 (17.7) | 0.019 | ||||
| 8 weeks | 61.9 (16.2) | ||||||
| Exergaming with Xbox 360 video game Kinect | Baseline | 70.75 (19.6) | 0.041 | ||||
| 8 weeks | 64.3 (19.2) | ||||||
| Ya and Petrini [33], 2017 | Home-based resistance exercise | Baseline | 19.30 (13.58) | 0.007 | 6MWT FTSST 10MWT TUG One-repetition maximum, WHODAS 2.0 SF-36 1RM | ||
| 12 weeks | 11.19 (8.23) | ||||||
| Encouraged to do more exercise | Baseline | 11.42 (12.31) | 0.848 | ||||
| 12 weeks | 11.77 (12.40) | ||||||
| Galli et al. [34], 2018 | Inpatients rehabilitation | Baseline | 37.28 (9.070) | ADL BI WHODAS 2.0 | |||
| 30 days | 15.65 (11.658) | 0.002 | |||||
| Teixeira-Machado et al. [35], 2017 | IG- = dance class sessions CG = kinesiotherapy | Baseline | 84.56 (%) | 84.45 (%) | 0.33 | WHODAS 2.0 FIM GMFCS | |
| After 24 sessions | 39.90 (%) | 69.55 (%) | 0.04 | ||||
| Shahbazi et al. [36], 2016 | IG—care service package CG—potential candidates for receiving care service package | Baseline | 23.08 (12.16) | 21.98 (11.55) | 0.659 | WHODAS 2.0 | |
| Before treatment | 22.6 (11.2) | 22.0 (11.5) | |||||
| 2 months after treatment | 19.3 (10.6) | 22.6 (11.0) | |||||
| 4 months after treatment | 17.6 (9.3) | 24.7 (11.1) | |||||
| 6 months after treatment | 17.4 (8.9) | 25.8 (10.8) | <0.001 | ||||
| Petterson et al. [37], 2015 | IG—4 months after PMDs CG—before PMD | 24.57 (12.16) | 28.12 (13.20) | 0.248 | WHODAS 2.0 IPPA SF-36 | ||
| Martinez et al. [38], 2014 | IG—online intervention CG—no intervention | Pre-intervention | 34.71 (18.96) | 14.47 (12.38) | 0.002 | WHODAS SIP SF-36 | |
| Post-intervention | 25 (17.79) | 16.3 (14.55) | 0.180 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potcovaru, C.-G.; Salmen, T.; Bîgu, D.; Săndulescu, M.I.; Filip, P.V.; Diaconu, L.S.; Pop, C.; Ciobanu, I.; Cinteză, D.; Berteanu, M. Assessing the Effectiveness of Rehabilitation Interventions through the World Health Organization Disability Assessment Schedule 2.0 on Disability—A Systematic Review. J. Clin. Med. 2024, 13, 1252. https://doi.org/10.3390/jcm13051252
Potcovaru C-G, Salmen T, Bîgu D, Săndulescu MI, Filip PV, Diaconu LS, Pop C, Ciobanu I, Cinteză D, Berteanu M. Assessing the Effectiveness of Rehabilitation Interventions through the World Health Organization Disability Assessment Schedule 2.0 on Disability—A Systematic Review. Journal of Clinical Medicine. 2024; 13(5):1252. https://doi.org/10.3390/jcm13051252
Chicago/Turabian StylePotcovaru, Claudia-Gabriela, Teodor Salmen, Dragoș Bîgu, Miruna Ioana Săndulescu, Petruța Violeta Filip, Laura Sorina Diaconu, Corina Pop, Ileana Ciobanu, Delia Cinteză, and Mihai Berteanu. 2024. "Assessing the Effectiveness of Rehabilitation Interventions through the World Health Organization Disability Assessment Schedule 2.0 on Disability—A Systematic Review" Journal of Clinical Medicine 13, no. 5: 1252. https://doi.org/10.3390/jcm13051252
APA StylePotcovaru, C.-G., Salmen, T., Bîgu, D., Săndulescu, M. I., Filip, P. V., Diaconu, L. S., Pop, C., Ciobanu, I., Cinteză, D., & Berteanu, M. (2024). Assessing the Effectiveness of Rehabilitation Interventions through the World Health Organization Disability Assessment Schedule 2.0 on Disability—A Systematic Review. Journal of Clinical Medicine, 13(5), 1252. https://doi.org/10.3390/jcm13051252