
Patient-Reported Outcomes of Maxillomandibular Surgery for Obstructive Sleep Apnea Treatment: A Scoping Review

 ,
, 
 ,
,  , ,
, ,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Database Search Protocol
2.3. Analysis of Eligibility Criteria, Selection of Studies and Data Collection
3. Results
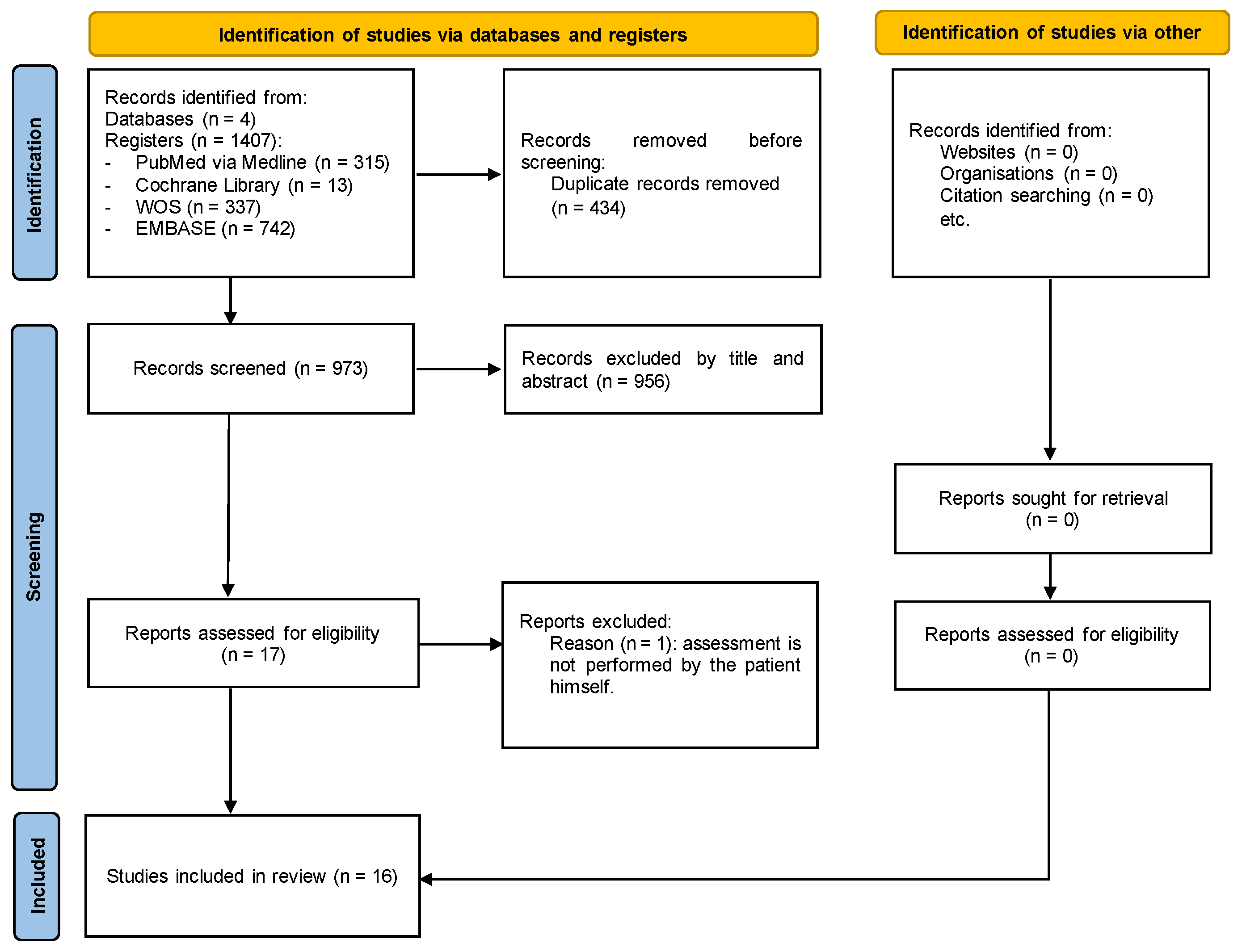
3.1. Study Selection
3.2. Characteristics of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Available online: https://aasm.org/clinical-resources/international-classification-sleep-disorders/ (accessed on 12 January 2024).
- Fagundes, N.C.F.; Minervini, G.; Furio Alonso, B.; Nucci, L.; Grassia, V.; d’Apuzzo, F.; Puigdollers, A.; Perillo, L.; Flores-Mir, C. Patient-reported outcomes while managing obstructive sleep apnea with oral appliances: A scoping review. J. Evid. Based Dent. Pract. 2023, 23, 101786. [Google Scholar] [CrossRef]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.-M.; Liao, D.; Calhoun, S.; Vela-Bueno, A.; Fedok, F.; Vlasic, V.; Graff, G. Sleep Disordered Breathing in Children in a General Population Sample: Prevalence and Risk Factors. Sleep 2009, 32, 731–736. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of Obstructive Sleep Apnea in the General Population: A Systematic Review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Arens, R.; Marcus, C.L. Pathophysiology of Upper Airway Obstruction: A Developmental Perspective. Sleep 2004, 27, 997–1019. [Google Scholar] [CrossRef]
- Morsy, N.E.; Farrag, N.S.; Zaki, N.F.W.; Badawy, A.Y.; Abdelhafez, S.A.; El-Gilany, A.-H.; El Shafey, M.M.; Pandi-Perumal, S.R.; Spence, D.W.; BaHammam, A.S. Obstructive Sleep Apnea: Personal, Societal, Public Health, and Legal Implications. Rev. Environ. Health 2019, 34, 153–169. [Google Scholar] [CrossRef]
- Jennum, P.; Rejkjær-Knudsen, M.; Ibsen, R.; Kiær, E.K.; von Buchwald, C.; Kjellberg, J. Long-Term Health and Socioeconomic Outcome of Obstructive Sleep Apnea in Children and Adolescents. Sleep Med. 2020, 75, 441–447. [Google Scholar] [CrossRef]
- Javaheri, S.; Barbe, F.; Campos-Rodriguez, F.; Dempsey, J.A.; Khayat, R.; Javaheri, S.; Malhotra, A.; Martinez-Garcia, M.A.; Mehra, R.; Pack, A.I.; et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 2017, 69, 841–858. [Google Scholar] [CrossRef]
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea. JAMA 2020, 323, 1389. [Google Scholar] [CrossRef]
- Alansari, R.A. The Role of Orthodontics in Management of Obstructive Sleep Apnea. Saudi Dent. J. 2022, 34, 194–201. [Google Scholar] [CrossRef]
- Levine, M.; Bennett, K.; Cantwell, M.; Postol, K.; Schwartz, D. Dental Sleep Medicine Standards for Screening, Treating, and Managing Adults with Sleep-Related Breathing Disorders. J. Dent. Sleep Med. 2018, 5, 61–68. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. STOP Questionnaire. Anesthesiology 2008, 108, 812–821. [Google Scholar] [CrossRef]
- Netzer, N.C.; Stoohs, R.A.; Netzer, C.M.; Clark, K.; Strohl, K.P. Using the Berlin Questionnaire To Identify Patients at Risk for the Sleep Apnea Syndrome. Ann. Intern. Med. 1999, 131, 485. [Google Scholar] [CrossRef]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric Sleep Questionnaire (PSQ): Validity and Reliability of Scales for Sleep-Disordered Breathing, Snoring, Sleepiness, and Behavioral Problems. Sleep Med. 2000, 1, 21–32. [Google Scholar] [CrossRef]
- Ramar, K.; Dort, L.C.; Katz, S.G.; Lettieri, C.J.; Harrod, C.G.; Thomas, S.M.; Chervin, R.D. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Clin. Sleep Med. 2015, 11, 773–827. [Google Scholar] [CrossRef]
- Gurgel, M.; Cevidanes, L.; Pereira, R.; Costa, F.; Ruellas, A.; Bianchi, J.; Cunali, P.; Bittencourt, L.; Junior, C.C. Three-Dimensional Craniofacial Characteristics Associated with Obstructive Sleep Apnea Severity and Treatment Outcomes. Clin. Oral Investig. 2022, 26, 875–887. [Google Scholar] [CrossRef]
- Vanderveken, O.; Hoekema, A. How to Treat Patients That Do Not Tolerate Continuous Positive Airway Pressure. Breathe 2010, 7, 157–167. [Google Scholar] [CrossRef]
- Mansukhani, M.P.; Olson, E.J.; Caples, S.M. Upper Airway Surgery for Obstructive Sleep Apnea. JAMA 2020, 324, 1161. [Google Scholar] [CrossRef]
- Lin, S.; Su, Y.; Wu, Y.; Chang, J.Z.; Tu, Y. Management of Paediatric Obstructive Sleep Apnoea: A Systematic Review and Network Meta-analysis. Int. J. Paediatr. Dent. 2020, 30, 156–170. [Google Scholar] [CrossRef]
- Nazarali, N.; Altalibi, M.; Nazarali, S.; Major, M.P.; Flores-Mir, C.; Major, P.W. Mandibular Advancement Appliances for the Treatment of Paediatric Obstructive Sleep Apnea: A Systematic Review. Eur. J. Orthod. 2015, 37, 618–626. [Google Scholar] [CrossRef]
- Huynh, N.T.; Desplats, E.; Almeida, F.R. Orthodontics Treatments for Managing Obstructive Sleep Apnea Syndrome in Children: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2016, 25, 84–94. [Google Scholar] [CrossRef]
- Holty, J.-E.C.; Guilleminault, C. Maxillomandibular Advancement for the Treatment of Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2010, 14, 287–297. [Google Scholar] [CrossRef]
- Varghese, R.; Adams, N.G.; Slocumb, N.L.; Viozzi, C.F.; Ramar, K.; Olson, E.J. Maxillomandibular Advancement in the Management of Obstructive Sleep Apnea. Int. J. Otolaryngol. 2012, 2012, 373025. [Google Scholar] [CrossRef]
- Li, K.K.; Riley, R.W.; Powell, N.B.; Guilleminault, C. Maxillomandibular Advancement for Persistent Obstructive Sleep Apnea After Phase I Surgery in Patients without Maxillomandibular Deficiency. Laryngoscope 2000, 110, 1684–1688. [Google Scholar] [CrossRef]
- Zaghi, S.; Holty, J.-E.C.; Certal, V.; Abdullatif, J.; Guilleminault, C.; Powell, N.B.; Riley, R.W.; Camacho, M. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 58. [Google Scholar] [CrossRef]
- Dattilo, D.J.; Drooger, S.A. Outcome Assessment of Patients Undergoing Maxillofacial Procedures for the Treatment of Sleep Apnea: Comparison of Subjective and Objective Results. J. Oral Maxillofac. Surg. 2004, 62, 164–168. [Google Scholar] [CrossRef]
- Abdelwahab, M.; Huang, A.; Chou, C.; Fleury, T.; Riley, R.; Most, S.; Liu, S. Patient’s Perception of Nasal Function and Cosmesis After Maxillomandibular Advancement for Obstructive Sleep Apnea. Facial Plast. Surg. Aesthet. Med. 2023, 25, 132–140. [Google Scholar] [CrossRef]
- Cillo, J.E.; Dattilo, D.J. Maxillomandibular Advancement for Obstructive Sleep Apnea Produces Long-Term Horizontal Advancement of the Maxilla and Mandible. J. Oral Maxillofac. Surg. 2019, 77, 2524–2528. [Google Scholar] [CrossRef]
- Cillo, J.E.; Dattilo, D.J. Oral Functional Behavior and Neurosensation After Adult Maxillomandibular Advancement for Obstructive Sleep Apnea in the Long-Term. J. Oral Maxillofac. Surg. 2020, 78, 255–260. [Google Scholar] [CrossRef]
- De Ruiter, M.H.T.; Apperloo, R.C.; Milstein, D.M.J.; de Lange, J. Facial Esthetics and Subjective Impairment Assessed after Maxillomandibular Advancement Surgery for Patients with Obstructive Sleep Apnea. In CRANIO®; Taylor & Francis: Abingdon, UK, 2023; Volume 41, pp. 16–21. [Google Scholar] [CrossRef]
- Rossi, D.S.; Goker, F.; Cullati, F.; Baj, A.; Pignatelli, D.; Beltramini, G.; Russillo, A.; Giannì, A.B.; Lucchina, A.G.; Mortellaro, C.; et al. Analysis and Comparison of Quality of Life and Patients’ Satisfaction between Dental-Skeletal Dysmorphisms and Obstructive Sleep Apnea (OSA) Patients Following Orthognathic Surgery. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 62–77. [Google Scholar]
- Rossi, D.S.; Goker, F.; Cullati, F.; Baj, A.; Pignatelli, D.; Gianni, A.B.; Del Fabbro, M. Post-Operative Patients’ Satisfaction and Quality of Life Assessment in Adult Patients with Obstructive Sleep Apnea Syndrome (OSAS). Int. J. Environ. Res. Public Health 2022, 19, 6273. [Google Scholar] [CrossRef]
- Martin, M.J.; Khanna, A.; Srinivasan, D.; Sovani, M.P. Patient-Reported Outcome Measures Following Maxillomandibular Advancement Surgery in Patients with Obstructive Sleep Apnoea Syndrome. Br. J. Oral Maxillofac. Surg. 2022, 60, 963–968. [Google Scholar] [CrossRef]
- Goodday, R.H.; Bourque, S.E.; Edwards, P.B. Objective and Subjective Outcomes Following Maxillomandibular Advancement Surgery for Treatment of Patients with Extremely Severe Obstructive Sleep Apnea (Apnea-Hypopnea Index > 100). J. Oral Maxillofac. Surg. 2016, 74, 583–589. [Google Scholar] [CrossRef]
- Butterfield, K.J.; Marks, P.L.G.; McLean, L.; Newton, J. Quality of Life Assessment After Maxillomandibular Advancement Surgery for Obstructive Sleep Apnea. J. Oral Maxillofac. Surg. 2016, 74, 1228–1237. [Google Scholar] [CrossRef]
- Beranger, T.; Garreau, E.; Ferri, J.; Raoul, G. Morphological Impact on Patients of Maxillomandibular Advancement Surgery for the Treatment of Obstructive Sleep Apnea-Hypopnea Syndrome. Int. Orthod. 2017, 15, 40–53. [Google Scholar] [CrossRef]
- Lin, C.-H.; Chin, W.-C.; Huang, Y.-S.; Wang, P.-F.; Li, K.K.; Pirelli, P.; Chen, Y.-H.; Guilleminault, C. Objective and Subjective Long Term Outcome of Maxillomandibular Advancement in Obstructive Sleep Apnea. Sleep Med. 2020, 74, 289–296. [Google Scholar] [CrossRef]
- Boyd, S.B.; Chigurupati, R.; Cillo, J.E.; Eskes, G.; Goodday, R.; Meisami, T.; Viozzi, C.F.; Waite, P.; Wilson, J. Maxillomandibular Advancement Improves Multiple Health-Related and Functional Outcomes in Patients with Obstructive Sleep Apnea: A Multicenter Study. J. Oral Maxillofac. Surg. 2019, 77, 352–370. [Google Scholar] [CrossRef]
- Pottel, L.; Neyt, N.; Hertegonne, K.; Pevernagie, D.; Veys, B.; Abeloos, J.; De Clercq, C. Long-Term Quality of Life Outcomes of Maxillomandibular Advancement Osteotomy in Patients with Obstructive Sleep Apnoea Syndrome. Int. J. Oral Maxillofac. Surg. 2019, 48, 332–340. [Google Scholar] [CrossRef]
- Boyd, S.B.; Walters, A.S.; Waite, P.; Harding, S.M.; Song, Y. Long-Term Effectiveness and Safety of Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea. J. Clin. Sleep Med. 2015, 11, 699–708. [Google Scholar] [CrossRef]
- González, M.B.; Casellas, J.B.; Fernández Mondragón, M.P.; Nuño, V.C.; Amezaga, J.A.; De Carlos Villafra, F. Clinical, Esthetic, and Quality of Life Outcomes after Telegnathic Surgery in Caucasian OSAS Patients. In CRANIO®; Taylor & Francis: Abingdon, UK, 2022; Volume 40, pp. 425–432. [Google Scholar] [CrossRef]
- Young, A.; Brookes, S.; Rumsey, N.; Blazeby, J. Agreement on What to Measure in Randomised Controlled Trials in Burn Care: Study Protocol for the Development of a Core Outcome Set. BMJ Open 2017, 7, e017267. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Checklist for Assessing the Methodological Quality of Studies on Measurement Properties of Health Status Measurement Instruments: An International Delphi Study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef]
- Scharf, M.T. Reliability and Efficacy of the Epworth Sleepiness Scale: Is There Still a Place for It? Nat. Sci. Sleep 2022, 14, 2151–2156. [Google Scholar] [CrossRef]
- Puretić, H.; Bosnar Puretić, M.; Pavliša, G.; Jakopović, M. Revisiting the Epworth Sleepiness Scale. In Wiener Klinische Wochenschrift; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar] [CrossRef]
- Gonçalves, M.T.; Malafaia, S.; Moutinho dos Santos, J.; Roth, T.; Marques, D.R. Epworth Sleepiness Scale: A Meta-Analytic Study on the Internal Consistency. Sleep Med. 2023, 109, 261–269. [Google Scholar] [CrossRef]
- Silva, G.; Goodwin, J.; Vana, K.; Quan, S. Obstructive Sleep Apnea and Quality of Life: Comparison of the SAQLI, FOSQ, and SF-36 Questionnaires. Southwest J. Pulm. Crit. Care 2016, 13, 137–149. [Google Scholar] [CrossRef]
- Izci, B.; Firat, F.; Ardic, S.; Kokturk, O.; Gelir, E.; Altinors, M. Adaptation of Functional Outcomes of Sleep Questionnaire (FOSQ) to Turkish Population. Tüberküloz Toraks Derg. 2004, 52, 224–230. [Google Scholar]

{kind=link}
| Research Question | |
|---|---|
| Population | Patients diagnosed with OSAS |
| Intervention | Patients who underwent orthognathic surgery |
| Outcome | Patients’ perspectives (PROMs) |
| Data Bases | Search Keys | ||
|---|---|---|---|
| PubMed | (“Sleep Apnea Syndromes”[Mesh] OR “Sleep Apnea*” OR “Apnea Syndrome, Sleep” OR “Apnea Syndromes, Sleep” OR “Sleep Hypopnea*” OR “Hypopnea, Sleep” OR “Hypopneas, Sleep” OR “Apnea, Sleep” OR “Apneas, Sleep” OR “Hypersomnia with Periodic Respiration” OR “Sleep-Disordered Breathing” OR “Breathing, Sleep-Disorder*” OR “Sleep Disordered Breathing” OR “Sleep-Disorder Breathing” OR “Sleep Disorder Breathing” OR “OSA” OR “OSAS”) AND (“Orthognathic Surgery”[Mesh] OR “Orthognathic Surger*” OR “Surgery, Orthognathic” OR “Surgeries, Orthognathic” OR “Orthognathic Surgical Procedures”[Mesh] OR “Orthognathic Surgical Procedure*” OR “Procedure, Orthognathic Surgical” OR “Procedures, Orthognathic Surgical” OR “Surgical Procedure, Orthognathic” OR “Surgical Procedures, Orthognathic” OR “Jaw Surger*” OR “Surgeries, Jaw” OR “Surgery, Jaw” OR “Maxillo-Mandibular Surger*” OR “Maxillo Mandibular Surger*” OR “Surgeries, Maxillo-Mandibular” OR “Surgery, Maxillo-Mandibular” OR “Surgeries, Maxillofacial Orthognathic” OR “Surgery, Maxillofacial Orthognathic”). Filters: languages—EN, SP, FR, and PT. | ||
| All Web of Science Databases | (“Sleep Apnea*” OR “Apnea Syndrome, Sleep” OR “Apnea Syndromes, Sleep” OR “Sleep Hypopnea*” OR “Hypopnea, Sleep” OR “Hypopneas, Sleep” OR “Apnea, Sleep” OR “Apneas, Sleep” OR “Hypersomnia with Periodic Respiration” OR “Sleep-Disordered Breathing” OR “Breathing, Sleep-Disordered” OR “Sleep Disordered Breathing” OR “OSA” OR “OSAS”) AND (“Orthognathic Surger*” OR “Surgery, Orthognathic” OR “Surgeries, Orthognathic” OR “Orthognathic Surgical Procedure*” OR “Procedure, Orthognathic Surgical” OR “Procedures, Orthognathic Surgical” OR “Surgical Procedure, Orthognathic” OR “Surgical Procedures, Orthognathic” OR “Jaw Surger*” OR “Surgeries, Jaw” OR “Surgery, Jaw” OR “Maxillo-Mandibular Surger*” OR “Maxillo Mandibular Surger*” OR “Surgeries, Maxillo-Mandibular” OR “Surgery, Maxillo-Mandibular” OR “Surgeries, Maxillofacial Orthognathic” OR “Surgery, Maxillofacial Orthognathic”) (Topic) and English or French or Spanish or Portuguese (Languages) and Review Article or Abstract or Meeting or Letter or Editorial Material or Patent or Book (Exclude—Document Types). Filters: languages—EN, SP, FR, and PT. | ||
| Embase | (“sleep apnea*”: ti,ab,kw OR “apnea syndrome, sleep”: ti,ab,kw OR “apnea syndromes, sleep’”: ti,ab,kw OR “sleep hypopnea*”:ti,ab,kw OR “hypopnea, sleep”: ti,ab,kw OR “hypopneas, sleep”: ti,ab,kw OR “apnea, sleep”: ti,ab,kw OR “apneas, sleep”: ti,ab,kw OR “hypersomnia with periodic respiration”: ti,ab,kw OR “sleep disordered breathing”/exp OR “sleep-disordered breathing”: ti,ab,kw OR “breathing, sleep disordered”: ti,ab,kw OR osa: ti,ab,kw OR osas: ti,ab,kw) AND (“orthognathic surgery”/exp OR “orthognathic surger*”: ti,ab,kw OR “surgery, orthognathic”: ti,ab,kw OR “surgeries, orthognathic”: ti,ab,kw OR “orthognathic surgical procedure*”: ti,ab,kw OR “procedure, orthognathic surgical”: ti,ab,kw OR “procedures, orthognathic surgical”: ti,ab,kw OR “surgical procedure, orthognathic”: ti,ab,kw OR “surgical procedures, orthognathic”: ti,ab,kw OR “jaw surger*”: ti,ab,kw OR “surgeries, jaw”: ti,ab,kw OR “surgery, jaw”: ti,ab,kw OR “maxillomandibular surger*”: ti,ab,kw OR “maxillo mandibular surger*”: ti,ab,kw OR “surgeries, maxillo-mandibular”: ti,ab,kw OR “surgery, maxillo-mandibular”: ti,ab,kw OR “maxillofacial orthognathic surger*”: ti,ab,kw OR “orthognathic surgeries, maxillofacial”: ti,ab,kw OR “orthognathic surgery, maxillofacial”: ti,ab,kw OR “surgeries, maxillofacial orthognathic”: ti,ab,kw OR “surgery, maxillofacial orthognathic”: ti,ab,kw) AND ([english]/lim OR [french]/lim OR [portuguese]/lim OR [spanish]/lim) AND ([article]/lim OR [article in press]/lim OR [data papers]/lim OR [letter]/lim) Filters: languages—EN, SP, FR, and PT. | ||
| Cochrane | ID | Search | Hits |
| #1 | MeSH descriptor: [Sleep Apnea Syndromes] explode all trees | 3389 | |
| #2 | “sleep apnea” | 8129 | |
| #3 | “sleep apneas” | 111 | |
| #4 | “apnea syndrome, sleep” | 14 | |
| #5 | “apnea syndromes, sleep” | 869 | |
| #6 | “sleep hypopnea” | 0 | |
| #7 | “sleep hypopneas” | 1 | |
| #8 | “hypopnea, sleep” | 7 | |
| #9 | “hypopneas, sleep” | 0 | |
| #10 | “apnea, sleep” | 412 | |
| #11 | “apneas, sleep” | 3 | |
| #12 | hypersomnia with periodic respiration | 0 | |
| #13 | “sleep-disordered breathing” | 3381 | |
| #14 | “breathing, sleep-disordered” | 4 | |
| #15 | “sleep disordered breathing” | 3381 | |
| #16 | OSA | 3950 | |
| #17 | OSAS | 709 | |
| #18 | MeSH descriptor: [Orthognathic Surgery] explode all trees | 64 | |
| #19 | “orthognathic surgery” | 601 | |
| #20 | “orthognathic surgeries” | 29 | |
| #21 | “surgery, orthognathic” | 40 | |
| #22 | “surgeries, orthognathic” | 0 | |
| #23 | MeSH descriptor: [Orthognathic Surgical Procedures] explode all trees | 279 | |
| #24 | “orthognathic surgical procedure” | 5 | |
| #25 | “orthognathic surgical procedures” | 199 | |
| #26 | “procedure, orthognathic surgical” | 0 | |
| #27 | “procedures, orthognathic surgical” | 8 | |
| #28 | “surgical procedure, orthognathic” | 0 | |
| #29 | “surgical procedures, orthognathic” | 7 | |
| #30 | “jaw surgery” | 65 | |
| #31 | “jaw surgeries” | 4 | |
| #32 | “surgeries, jaw” | 2 | |
| #33 | “surgery, jaw” | 11 | |
| #34 | “maxillo-mandibular surgery” | 0 | |
| #35 | “maxillo-mandibular surgeries” | 0 | |
| #36 | “maxillo mandibular surgery” | 0 | |
| #37 | “maxillo mandibular surgeries” | 0 | |
| #38 | “surgeries, maxillo-mandibular” | 0 | |
| #39 | “surgery, maxillo-mandibular” | 0 | |
| #40 | “maxillofacial orthognathic surgery” | 1 | |
| #41 | “maxillofacial orthognathic surgeries” | 0 | |
| #42 | “orthognathic surgeries, maxillofacial” | 0 | |
| #43 | “orthognathic surgery, maxillofacial” | 3 | |
| #44 | “surgeries, maxillofacial orthognathic” | 0 | |
| #45 | “surgery, maxillofacial orthognathic” | 0 | |
| #46 | (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17) AND (#18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45) | ||
| Author/ Year | Study Design | Sample Size | Mean Age of Patients | Sex | Instruments | Outcomes |
|---|---|---|---|---|---|---|
| Cillo et al., 2020 [30] | Retrospective cohort | 27 | 59.1 ± 11.7 years old | M = 15 F = 12 | Ottawa Sleep Apnea | Sleep quality |
| Daytime function | ||||||
| Physical health | ||||||
| Emotional health | ||||||
| Sexual desires | ||||||
| Functional desires | ||||||
| Dental function | ||||||
| Personal Satisfaction | ||||||
| Cillo et al., 2019 [29] | Retrospective cohort | 27 | 59.8 years old | M = 15 F = 12 | Modified survey from Cunningham et al. using seven-point visual analog scale | Chewing |
| Swallowing food | ||||||
| Swallowing fluids | ||||||
| Smiling | ||||||
| Spitting | ||||||
| Kissing | ||||||
| Eating | ||||||
| Drooling | ||||||
| Speaking | ||||||
| Perioral neurosensory | ||||||
| Dattilo, Drooger, et al., 2004 [27] | Prospective cohort | 57 | 47.2 years old | M = 43 F = 14 | Epworth Sleepiness Scale | Probability of falling asleep in a variety of situations (sitting, reading, watching TV and driving) |
| Rossi et al., 2022 [32] | Retrospective cohort | 18 | 44.39 ± 9.43 years old | M = 17 F = 1 | - Rustemeyer’s questionnaire - Post-operative quality-of-life questions specific for OSA | Rustemeyer’s questionnaire: -Facial aesthetics -Chewing function -Well-being Post-operative quality-of-life questions specific for OSA: -Quality of sleep -Day time function/activity -Emotional situation -Physical OSAS symptoms -Work activity |
| Rossi et al., 2022 [33] | Retrospective case-control | 61 (21-OSA) | 34.75 ± 11.33 | M = 33 F = 29 | - Rustemeyer’s questionnaire (only after surgery) - SF-36 questionnaire (pre- and post-operatively) | Rustemeyer’s questionnaire: -Facial aesthetics -Chewing function -Well-being SF-36 questionnaire: -Emotional well-being -General health -Health transition -Physical functioning -Role limitations due to physical health -Role limitations due to Emotional problems -Energy/fatigue -Social functioning -Bodily Pain |
| Boyd et al., 2019 [39] | Prospective cohort | 30 | 45.9 ± 9.8 years | M = 19 F = 11 | - Epworth Sleepiness Scale - Functional Outcomes of Sleep Questionnaire - SF-36 questionnaire | Epworth Sleepiness Scale: -Sleepiness Functional Outcomes of Sleep Questionnaire: -General productivity -Social outcome -Activity level -Vigilance -Intimate relationship and sexual activity SF-36 questionnaire: -Physical function -Role physical -Role emotional -Vitality -Mental health -Social function -Bodily pain -General health -Health change |
| Butterfield et al., 2016 [36] | Retrospective cohort | 22 | 45.9 ± 11.6 years | M = 19 F = 3 | - Ottawa Sleep Apnea | Sleep quality |
| Daytime function | ||||||
| Physical health | ||||||
| Mental and emotional health | ||||||
| Sexual health | ||||||
| Recovery | ||||||
| Dental function | ||||||
| Martin et al., 2022 [34] | Cohort | 10 | 49.9 years | M = 7 F = 3 | - Patient-reported outcome measures questionnaire (five-point Likert scale) - Epworth Sleepiness score - 10-point visual analogue scale | Patient-Reported Outcome Measurements (PROMs) questionnaire (five-point Likert scale): -Sleep quality -Daytime sleepiness -Energy levels -Appearance -Daily activities -Mood Epworth Sleepiness score: -Daytime sleepiness 10-point visual analogue scale: -Quality of life |
| Pottel et al., 2019 [40] | Retrospective cohort | 12 | 43.5 years | M = 10 F = 2 | - OSAS questionnaire - The Epworth Sleepiness Scale | OSAS questionnaire: -Headache -Daytime sleepiness -Night-time awakening -Concentration -Frequent nocturnal diuresis -Snoring -Sexual activity -Facial aesthetic -Self-confidence Epworth Sleepiness Scale: -Daytime sleepiness |
| Goodday, RH et al., 2016 [35] | Retrospective cohort | 13 | 38.6 ± 8.4 | NR | - Epworth Sleepiness Scale - General satisfaction survey | Epworth Sleepiness Scale: -Daytime sleepiness General satisfaction survey: -Recommendation -Benefit |
| Lin, CH et al., 2020 [20] | Cohort | 53 | 35.66 ± 11.66 | M = 40 F = 13 | - Epworth Sleepiness Scale - Pittsburgh Sleep Quality Index - Insomnia Severity Index - Beck Anxiety Inventory - Beck Depression Index - Short form of quality of life (SF-36) | Epworth Sleepiness Scale: -Daytime sleepiness Pittsburgh Sleep Quality Index: -Quality and patterns of sleep Insomnia Severity Index: -Insomnia Beck Anxiety Inventory: -Anxiety Beck Depression Index: -Depression Short form of quality of life (SF-36): -Physical functioning -Role physical -Bodily pain -General Health -Vitality -Social Functioning -Role emotional -Mental Health |
| Ruiter MHT et al., 2020 [31] | Cohort | 41 | 55 ± 10 | M = 35 F= 20 | - EQ-5D-3L - Epworth Sleepiness Scale - Functional Outcomes of Sleep - Visual Analog Scale | EQ-5D-3L: -Mobility -Self-care -Daily activities -Pain/discomfort -Mood Epworth Sleepiness Scale: -Daytime sleepiness Functional Outcomes of Sleep: -Activity level -Vigilance -Intimacy and sexual relationships -General productivity -Social outcomes Visual Analog Scale: Facial appearance |
| González, MB et al., 2020 [42] | Retrospective cohort | 25 | 46.68 | M = 23 F = 2 | SF-36 questionnaire | Facial appearance through two questions: - “Do you consider your esthetic change to be positive after surgery?” - “Do you consider your facial profile to be more youthful after surgery?” |
| Beranger T et al., 2017 [37] | Retrospective cohort | 23 | 45.7 | M = 15 F = 8 | Epworth Sleepiness Scale | - Facial appearance (modifications of the face, modifications smile, more smiley and youthful appearance) |
| Boyd, SB et al., 2015 [41] | Cohort | 30 | 50.5 ± 9.6 | M = 24 F = 6 | - Epworth Sleepiness Scale - Functional Outcome of Sleep Questionnaire - Sleep Apnea Quality of Life Index | Epworth Sleepiness Scale: -Sleepiness Sleep Apnea Quality of Life Index: -Daily functioning -Social interactions -Emotional functioning -Symptoms -Treatment-related symptoms |
| Abdelwahab, M et al., 2023 [28] | Prospective cohort | 31 | 38 ± 11 | M = 28 F = 3 | - Standardized Cosmesis and Health Nasal Outcomes Survey - Visual analog scale for nasal function and cosmesis (VAS-F and VAS-C) - Epworth sleepiness scale | Function (obstruction) Cosmesis Epworth sleepiness scale: -Daytime sleepiness |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francisco, I.; Nunes, C.; Baptista Paula, A.; Marques, F.; Prata Ribeiro, M.; McEvoy, M.; Santos, M.; Oliveira, C.; Marto, C.M.; Spagnuolo, G.; et al. Patient-Reported Outcomes of Maxillomandibular Surgery for Obstructive Sleep Apnea Treatment: A Scoping Review. J. Clin. Med. 2024, 13, 1232. https://doi.org/10.3390/jcm13051232
Francisco I, Nunes C, Baptista Paula A, Marques F, Prata Ribeiro M, McEvoy M, Santos M, Oliveira C, Marto CM, Spagnuolo G, et al. Patient-Reported Outcomes of Maxillomandibular Surgery for Obstructive Sleep Apnea Treatment: A Scoping Review. Journal of Clinical Medicine. 2024; 13(5):1232. https://doi.org/10.3390/jcm13051232
Chicago/Turabian StyleFrancisco, Inês, Catarina Nunes, Anabela Baptista Paula, Filipa Marques, Madalena Prata Ribeiro, Mariana McEvoy, Mariana Santos, Catarina Oliveira, Carlos Miguel Marto, Gianrico Spagnuolo, and et al. 2024. "Patient-Reported Outcomes of Maxillomandibular Surgery for Obstructive Sleep Apnea Treatment: A Scoping Review" Journal of Clinical Medicine 13, no. 5: 1232. https://doi.org/10.3390/jcm13051232
APA StyleFrancisco, I., Nunes, C., Baptista Paula, A., Marques, F., Prata Ribeiro, M., McEvoy, M., Santos, M., Oliveira, C., Marto, C. M., Spagnuolo, G., Carrilho, E., Travassos, R., & Vale, F. (2024). Patient-Reported Outcomes of Maxillomandibular Surgery for Obstructive Sleep Apnea Treatment: A Scoping Review. Journal of Clinical Medicine, 13(5), 1232. https://doi.org/10.3390/jcm13051232