


Treatment Efficiency of Maxillary and Mandibular Orovestibular Tooth Expansion and Compression Movements with the Invisalign® System in Adolescents and Adults
 , and
, and
Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Patient Collective
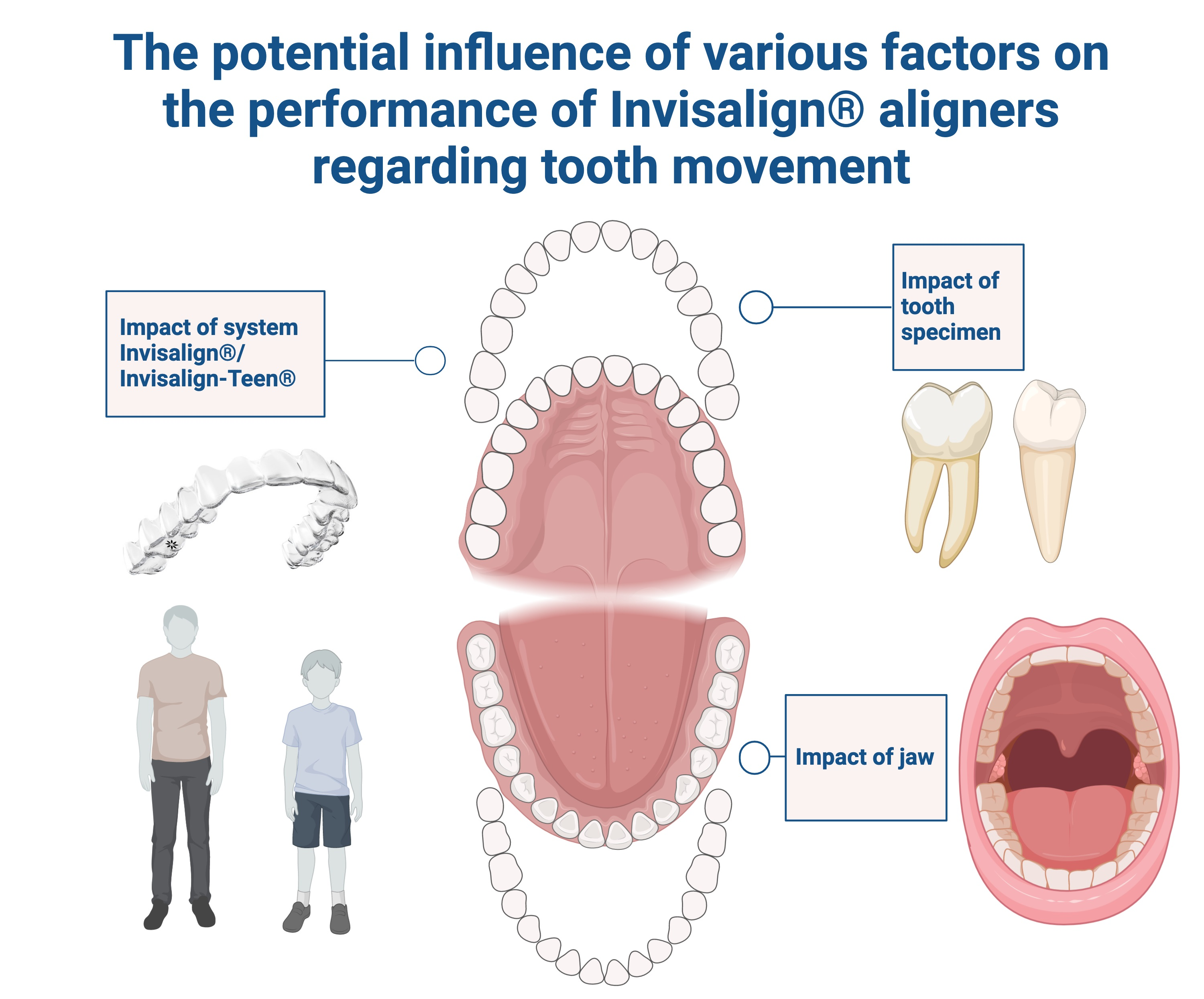
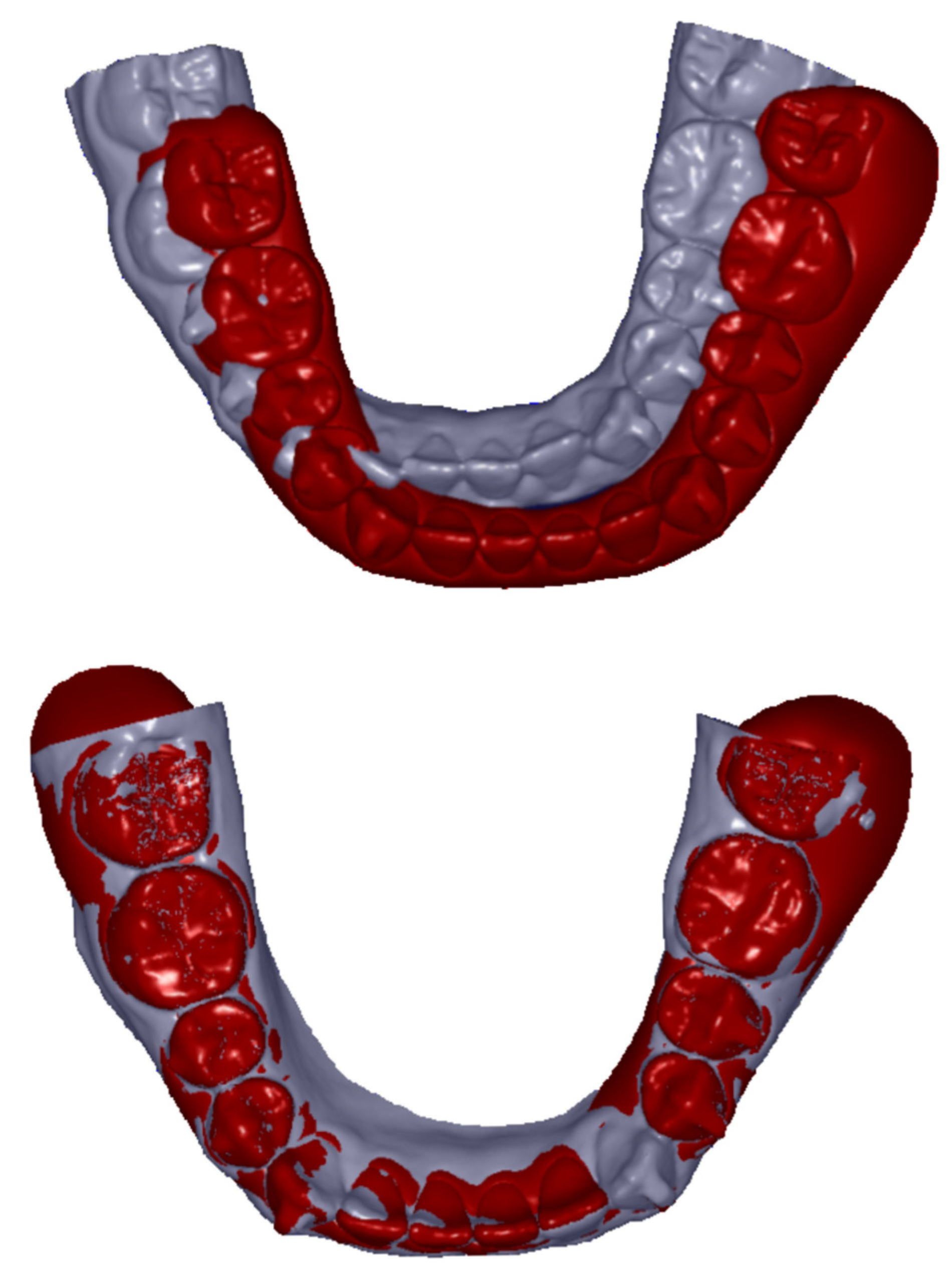
2.2. Data Selection and Preparation
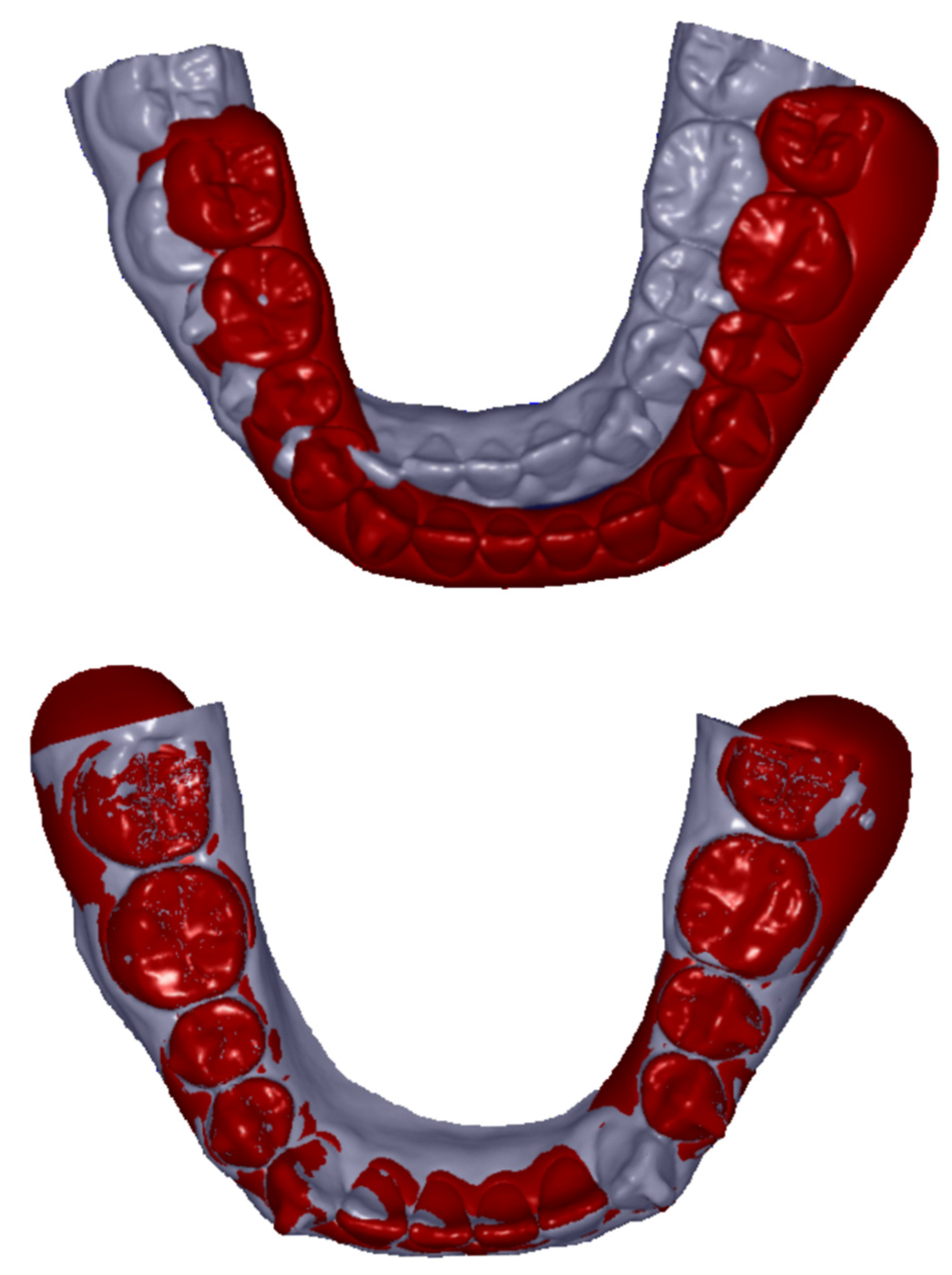
2.3. Methodology of Investigations
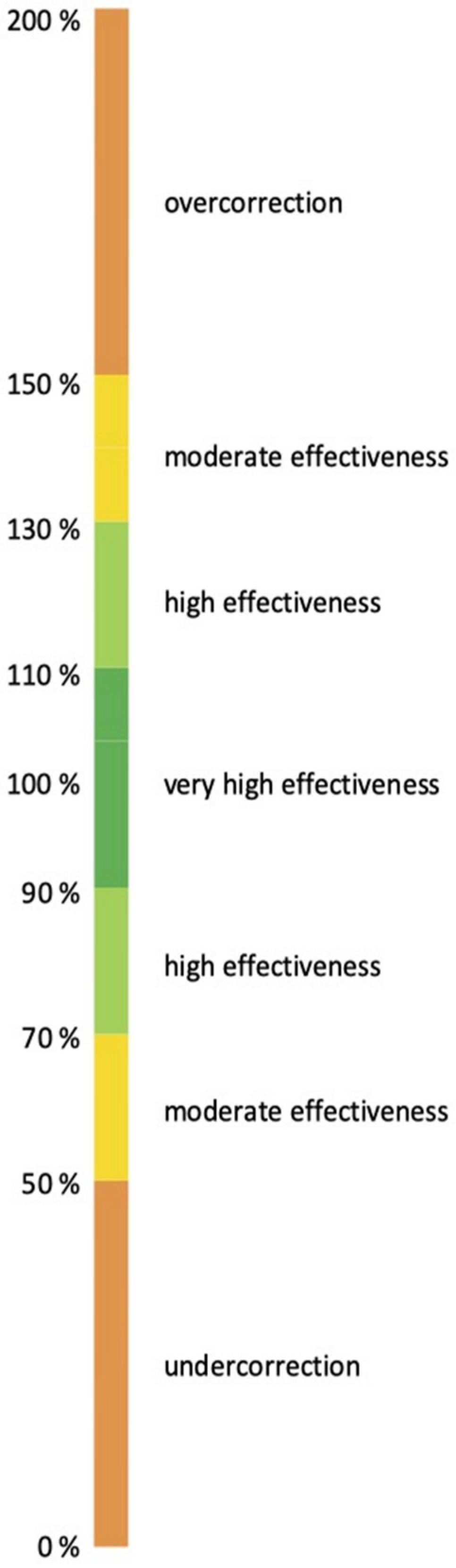
2.4. Data Analysis and Statistics
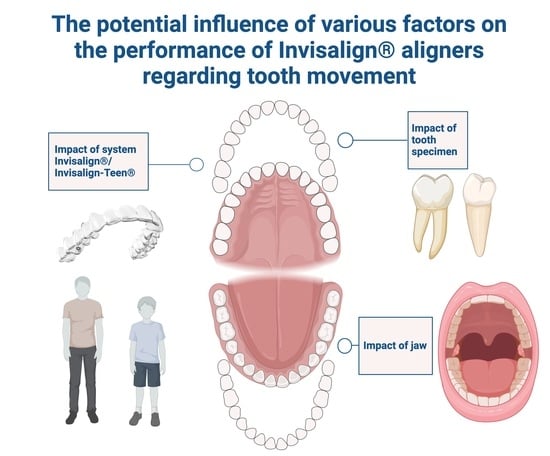
- Whether there were significant differences in the realization of expansion and compression movements with regard to the tooth type, namely incisors, canines, premolars and molars.
- Whether the fact that bone structure differs in maxilla and mandibula was reflected by different effectivity of these orovestibular movements.
- Whether due to either aspect 1 or 2, Group 1 and Group 2 exhibit significant variances.
3. Results
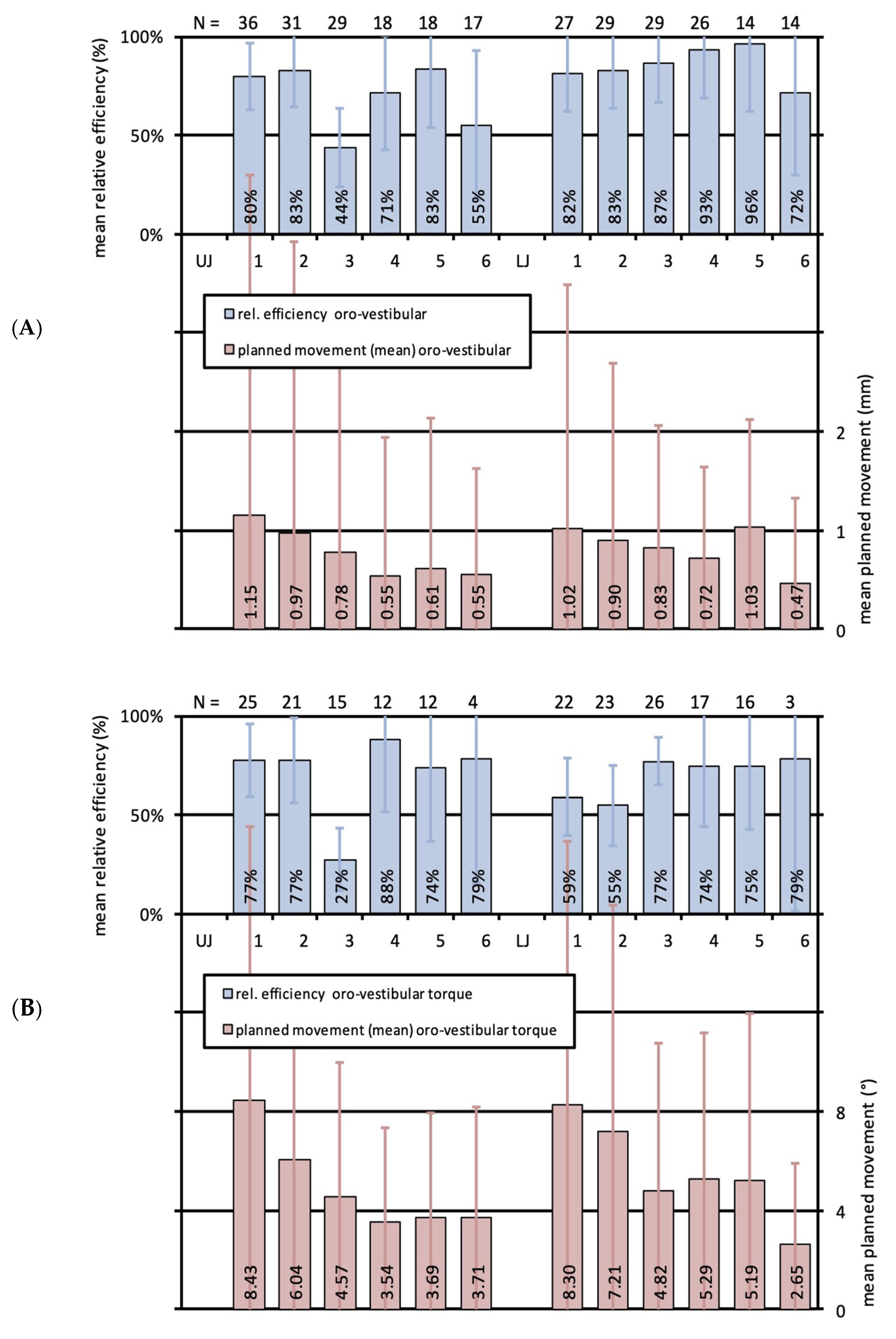
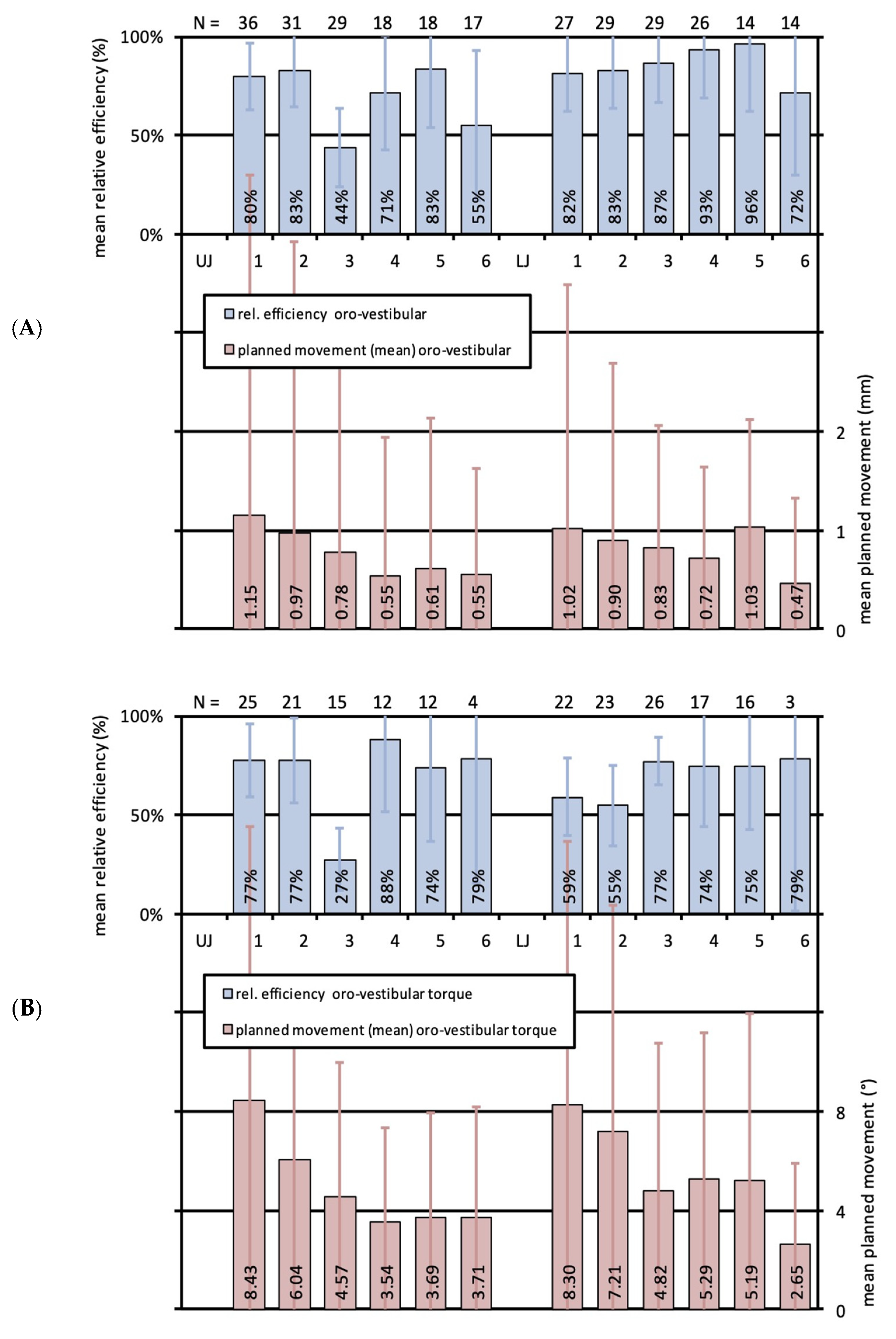
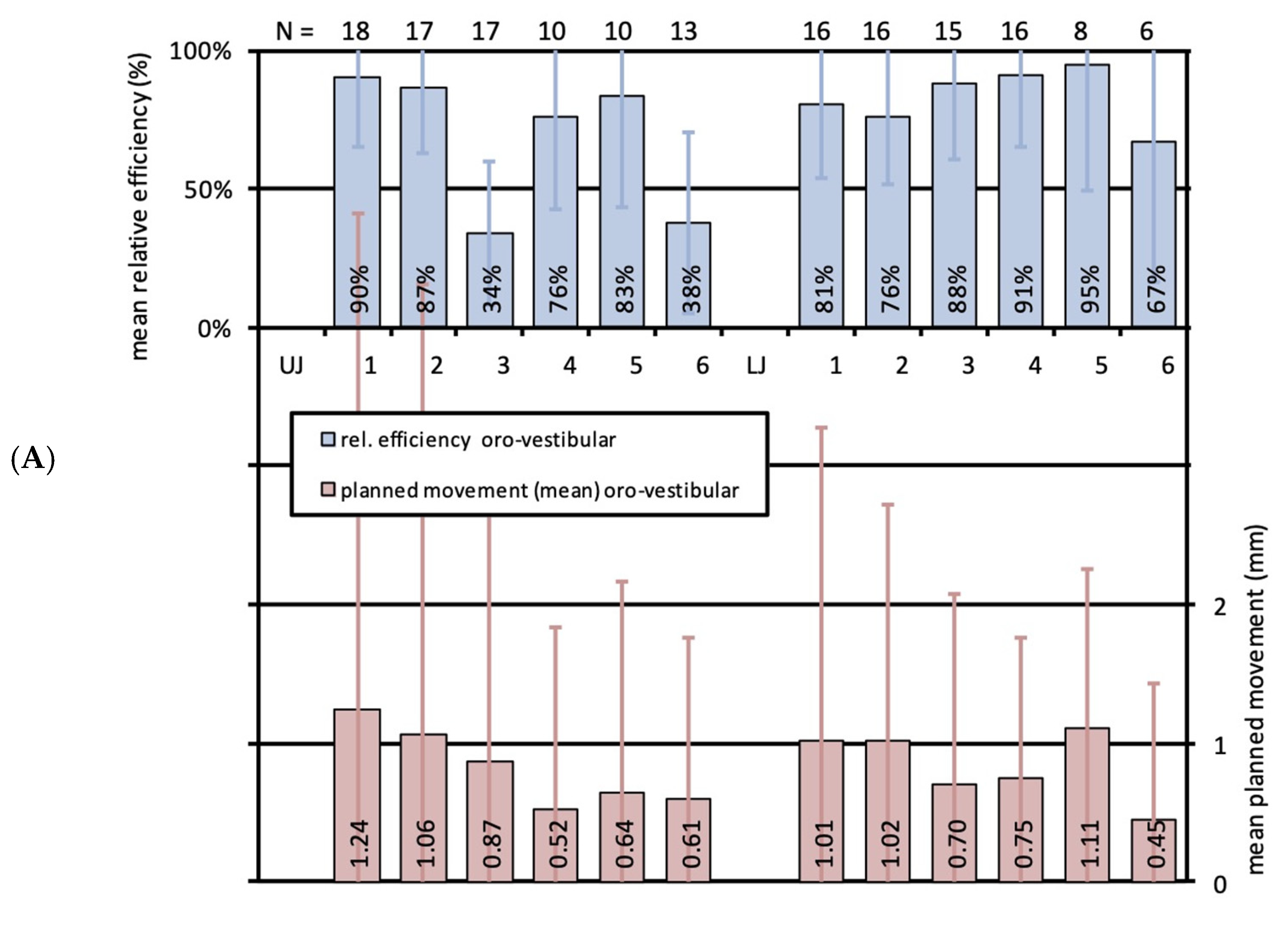
3.1. Effectiveness of Translational Movements for the Different Tooth Types of Upper and Lower Jaws
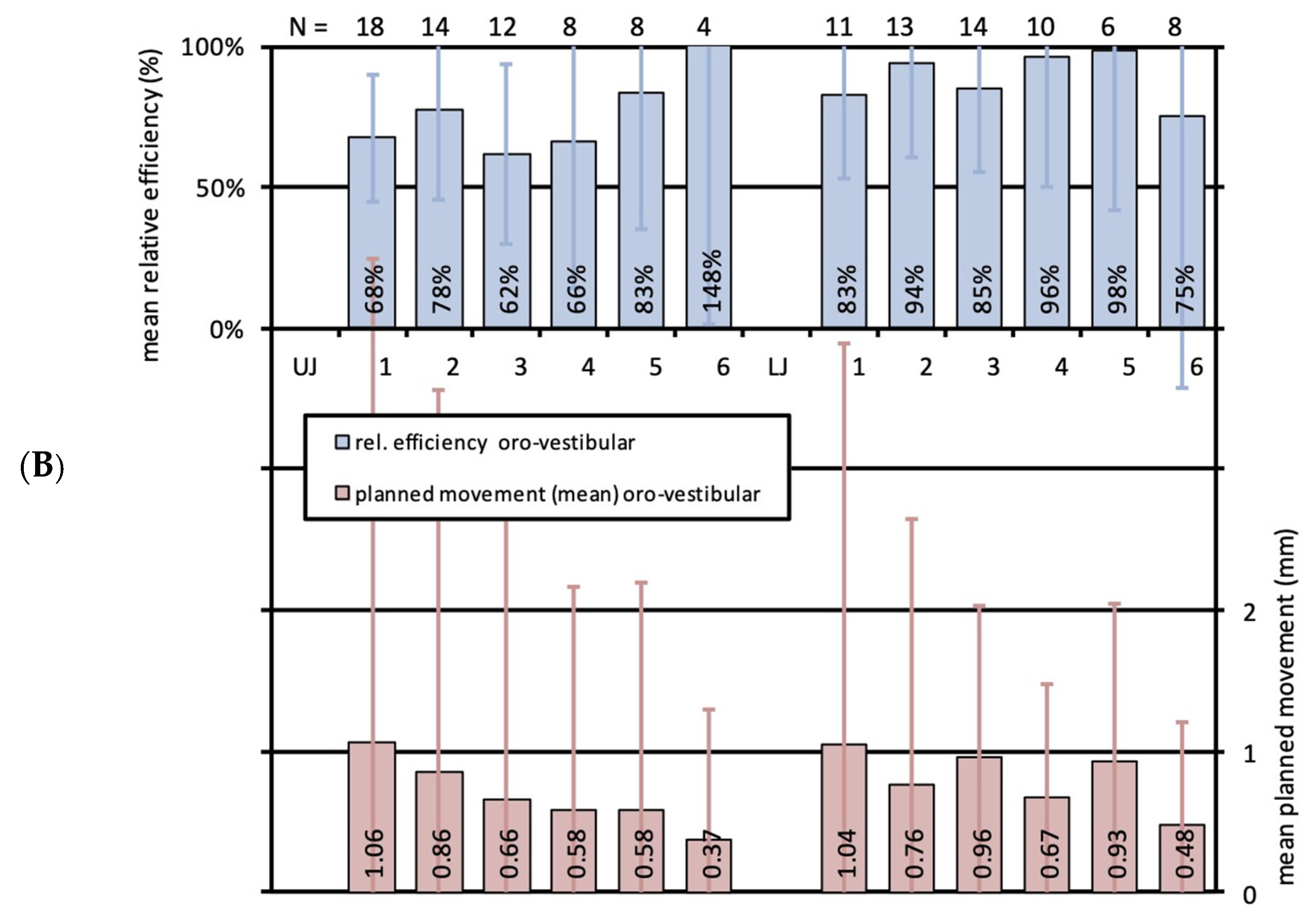
3.2. Effectiveness of Orovestibular Tipping for the Different Tooth Types of Upper and Lower Jaws
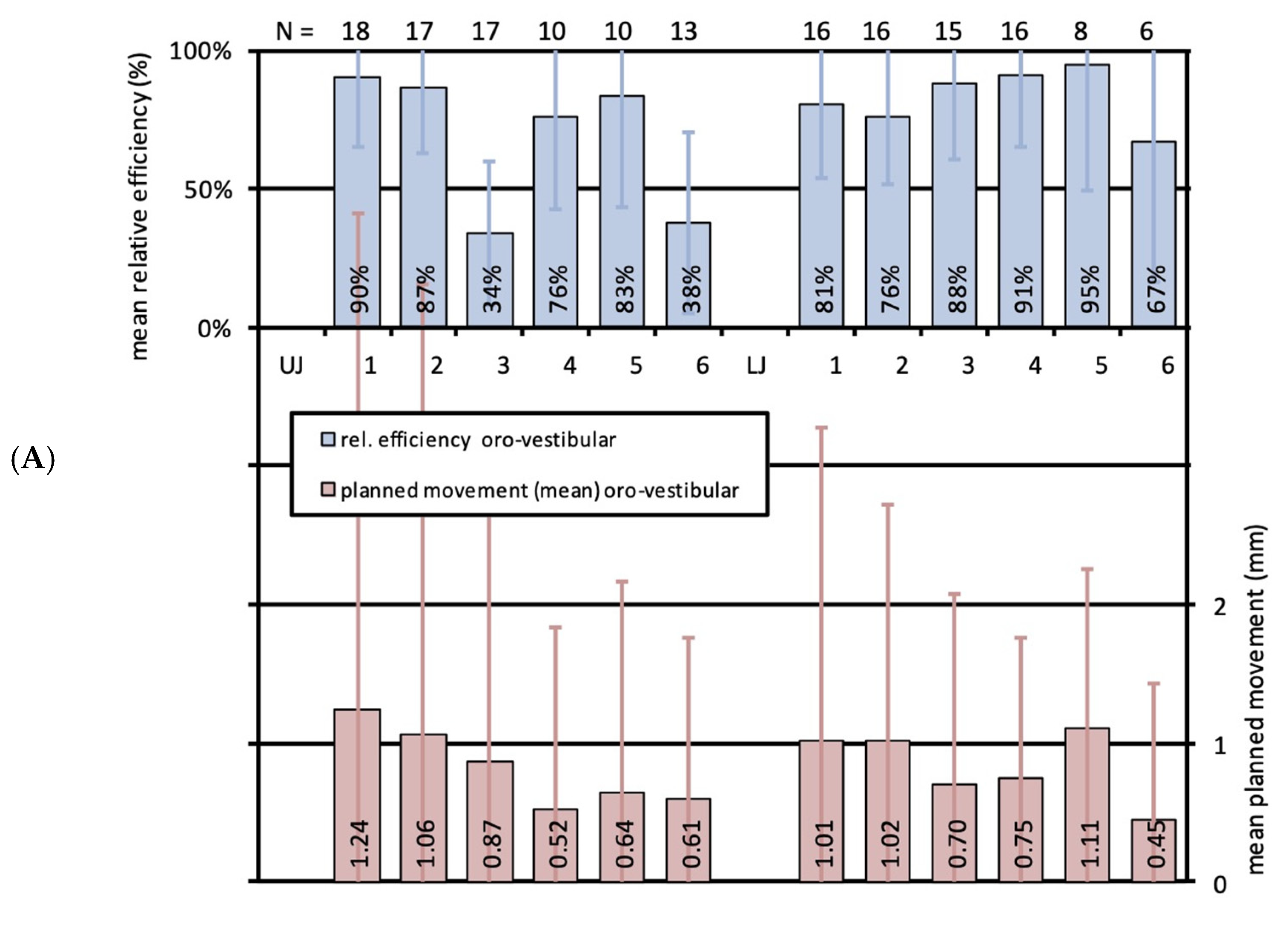
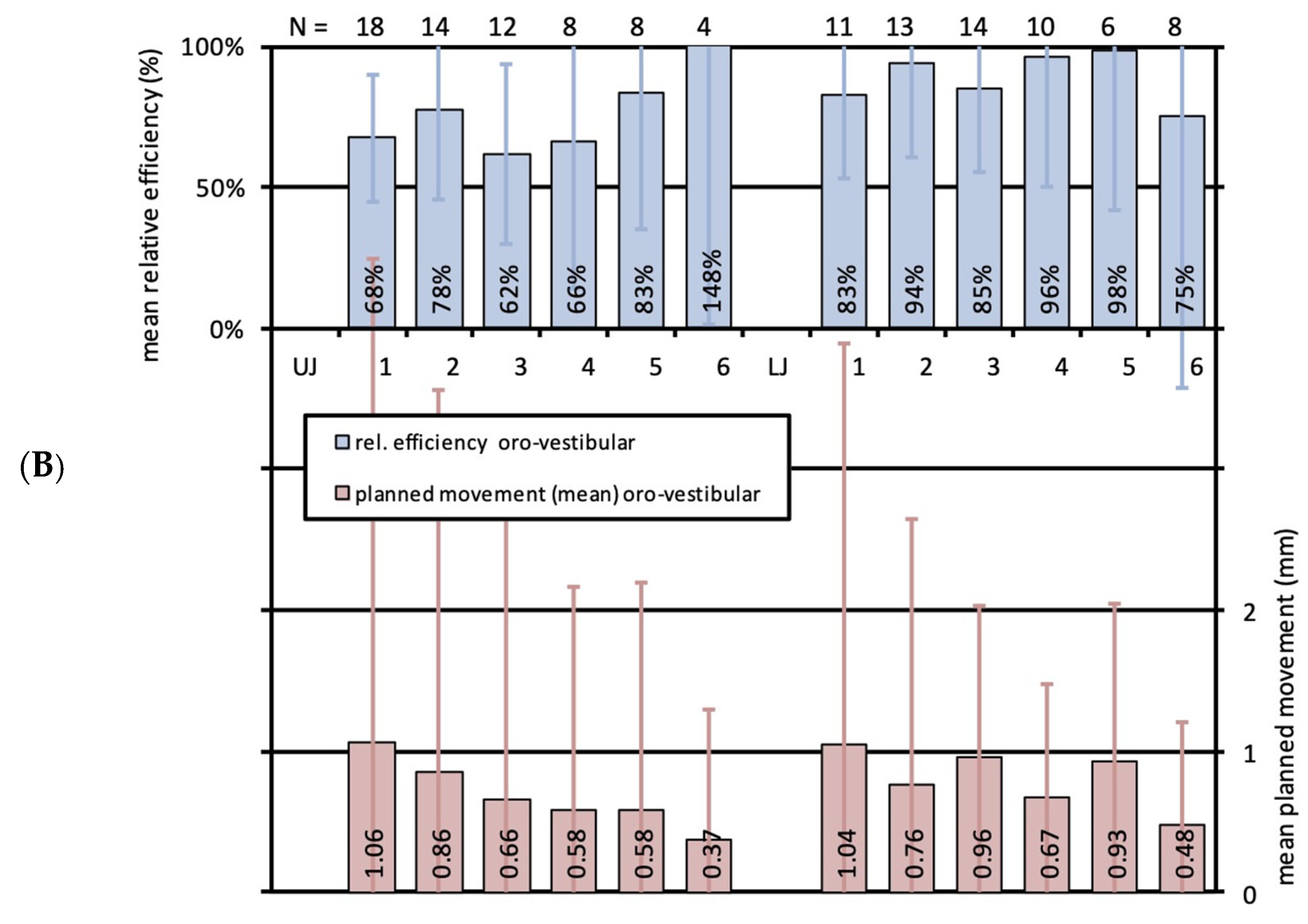
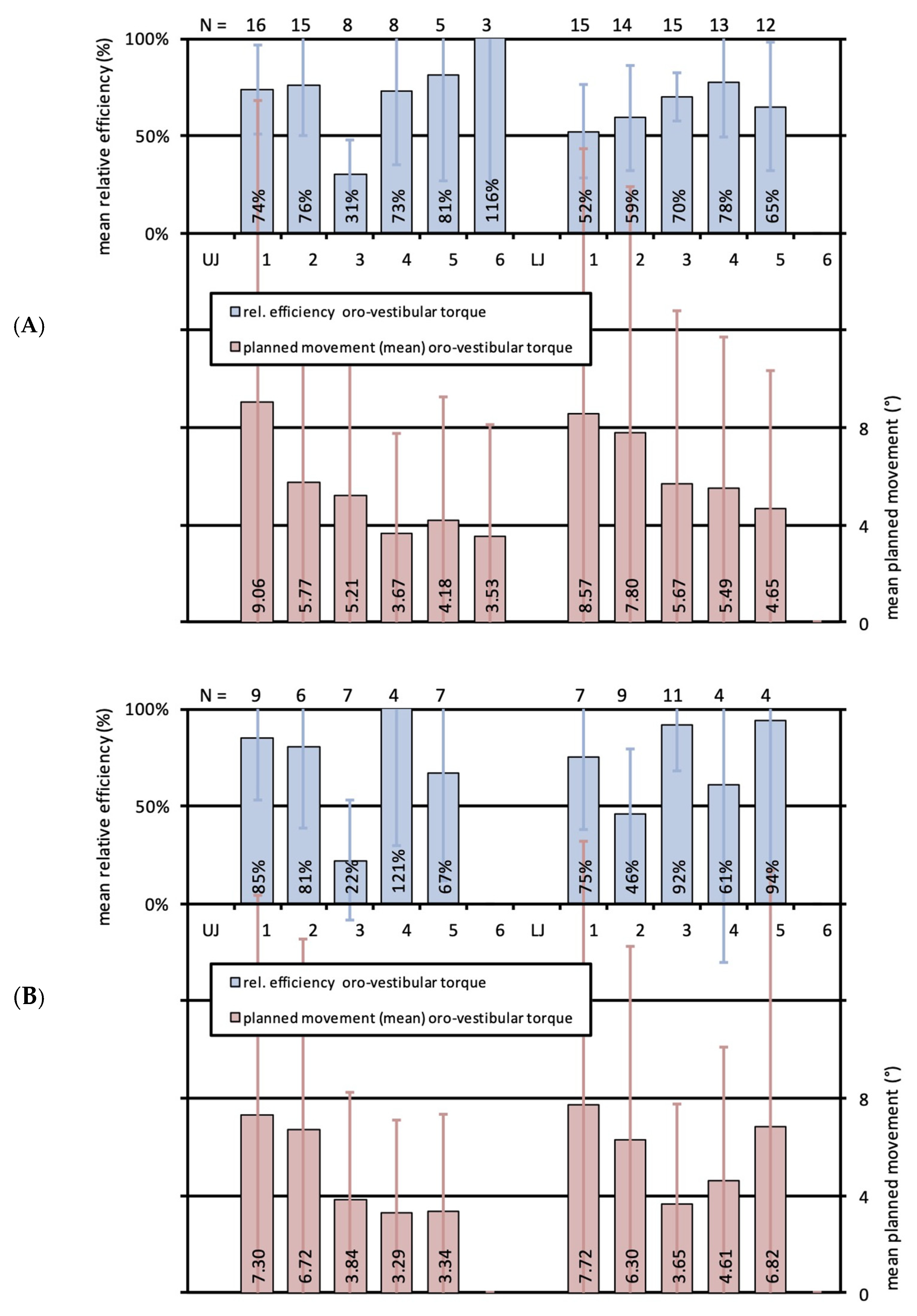
3.3. Effectiveness of Translational Movements in Upper and Lower Jaws for Adolescent and Adult Patients
3.4. Effectiveness of Orovestibular Tipping in Upper and Lower Jaws for Adolescent and Adult Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phan, X.; Ling, P.H. Clinical limitations of Invisalign. J. Can. Dent. Assoc. 2007, 73, 263–266. [Google Scholar] [PubMed]
- Boyd, R.L.; Waskalic, V. Three-dimensional diagnosis and orthodontic treatment of complex malocclusions with the invisalign appliance. Semin. Orthod. 2001, 7, 274–293. [Google Scholar] [CrossRef]
- Abbate, G.M.; Caria, M.P.; Montanari, P.; Mannu, C.; Orrù, G.; Caprioglio, A.; Levrini, L. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J. Orofac. Orthop. 2015, 76, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.; Willershausen, B. Braces versus Invisalign®: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Houle, J.P.; Piedade, L.; Todescan, R., Jr.; Pinheiro, F.H. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef]
- Krieger, E.; Seiferth, J.; Marinello, I.; Jung, B.A.; Wriedt, S.; Jacobs, C.; Wehrbein, H. Invisalign® treatment in the anterior region: Were the predicted tooth movements achieved? J. Orofac. Orthop. 2012, 73, 365–376. [Google Scholar] [CrossRef]
- Nedwed, V.; Miethke, R.R. Motivation, acceptance and problems of invisalign patients. J. Orofac. Orthop. 2005, 66, 162–173. [Google Scholar] [CrossRef]
- Schott, T.C.; Göz, G. Color fading of the blue compliance indicator encapsulated in removableclear Invisalign TeenHaligners. Angle Orthod. 2011, 81, 185–191. [Google Scholar] [CrossRef]
- Tuncay, O.C.; Bowman, S.J.; Nicozisis, J.L.; Amy, B.D. Effectiveness of a compliance indicator for clear aligners. J. Clin. Orthod. 2009, 43, 263–268. [Google Scholar]
- Djeu, G.; Shelton, C.; Maganzini, A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 292–298; discussion 298. [Google Scholar] [CrossRef] [PubMed]
- Kassam, S.K.; Stoops, F.R. Are clear aligners as effective as conventional fixed appliances? Evid. Based Dent. 2020, 21, 30–31. [Google Scholar] [CrossRef]
- Ke, Y.; Zhu, Y.; Zhu, M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Gandini, P.; Castroflorio, T.; Garino, F.; Mergati, L.; D’Anca, K.; Trovati, F.; Scribante, A. Buccolingual Inclination Control of Upper Central Incisors of Aligners: A Comparison with Conventional and Self-Ligating Brackets. Biomed. Res. Int. 2018, 2018, 9341821. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Tang, J.S.; Skulski, B.; Fields, H.W., Jr.; Beck, F.M.; Firestone, A.R.; Kim, D.G.; Deguchi, T. Evaluation of Invisalign treat-ment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating index. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, J.; Garvey, T.; Al-Awadhi, E.A. A randomized clinicaltrial comparing mandibular incisor proclination produced by fixedlabial appliances and clear aligners. Angle Orthod. 2016, 86, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, D.K.; King, G.; Ramsay, D.S.; Huang, G.; Bollen, A.M. Activation time and material stiffness of sequential removable orthodontic appliances. Part 3: Premolar extraction patients. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Bollen, A.M.; Huang, G.; King, G.; Hujoel, P.; Ma, T. Activation time and material stiffness of sequential removable orthodontic appliances. Part 1: Ability to complete treatment. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.D.; Kusnoto, B.; Agran, B.; Viana, G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. A prospective clinical study. Angle Orthod. 2008, 78, 682–687. [Google Scholar] [CrossRef]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef]
- Weckmann, J.; Scharf, S.; Graf, I.; Schwarze, J.; Keilig, L.; Bourauel, C.; Braumann, B. Influence of attachment bonding protocol on precision of the attachment in aligner treatments. J. Orofac. Orthop. 2020, 81, 30–40. [Google Scholar] [CrossRef]
- Boyd, R.L.; Miller, R.; Vlaskalic, V. The invisalign system in adult orthodontics: Mild crowding and space closure cases. J. Clin. Orthod. 2000, 34, 203–213. [Google Scholar]
- Charalampakis, O.; Iliadi, A.; Ueno, H.; Oliver, D.R.; Kim, K.B. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 47–54. [Google Scholar] [CrossRef]
- Morales-Burruezo, I.; Gandía-Franco, J.L.; Cobo, J.; Vela-Hernández, A.; Bellot-Arcís, C. Arch expansion with the Invisalign system: Efficacy and predictability. PLoS ONE 2020, 15, e0242979. [Google Scholar] [CrossRef] [PubMed]
- Solano-Mendoza, B.; Sonnemberg, B.; Solano-Reina, E.; Iglesias-Linares, A. How effective is the Invisalign® system in expansion movement with Ex30’ aligners? Clin. Oral Investig. 2017, 21, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Guo, J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthod. 2020, 90, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Keilig, L.; Piesche, K.; Jäger, A.; Bourauel, C. Applications of surface-surface matching algorithms for determination of orthodontic tooth movements. Comput. Methods Biomech. Biomed. Eng. 2003, 6, 353–359. [Google Scholar] [CrossRef]
- Condo’, R.; Pazzini, L.; Cerroni, L.; Pasquantonio, G.; Lagana’, G.; Pecora, A.; Mussi, V.; Rinaldi, A.; Mecheri, B.; Licoccia, S.; et al. Mechanical properties of “two generations” of teeth aligners: Change analysis during oral permanence. Dent. Mater. J. 2018, 37, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hui, S.; Gui, L.; Jin, F. Effects of upper arch expansion using clear aligners on different stride and torque: A three-dimensional finite element analysis. BMC Oral Health 2023, 23, 891. [Google Scholar] [CrossRef]
- Yao, S.; Jiang, W.; Wang, C.; He, Y.; Wang, C.; Huang, L. Improvements of tooth movement efficiency and torque control in expanding the arch with clear aligners: A finite element analysis. Front. Bioeng. Biotechnol. 2023, 11, 1120535. [Google Scholar] [CrossRef]
- Rocha, A.S.; Gonçalves, M.; Oliveira, A.C.; Azevedo, R.M.S.; Pinho, T. Efficiency and Predictability of Coronal Maxillary Expansion Repercussion with the Aligners System: A Retrospective Study. Dent. J. 2023, 11, 258. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, A.; Ayache, S.; Monteiro, F.; Silva, F.S.; Pinho, T. Efficiency of Invisalign First® to promote expansion movement in mixed dentition: A retrospective study and systematic review. Eur. J. Paediatr. Dent. 2023, 24, 112–123. [Google Scholar] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keilig, L.; Brieskorn, L.; Schwarze, J.; Schupp, W.; Bourauel, C.; Konermann, A. Treatment Efficiency of Maxillary and Mandibular Orovestibular Tooth Expansion and Compression Movements with the Invisalign® System in Adolescents and Adults. J. Clin. Med. 2024, 13, 1267. https://doi.org/10.3390/jcm13051267
Keilig L, Brieskorn L, Schwarze J, Schupp W, Bourauel C, Konermann A. Treatment Efficiency of Maxillary and Mandibular Orovestibular Tooth Expansion and Compression Movements with the Invisalign® System in Adolescents and Adults. Journal of Clinical Medicine. 2024; 13(5):1267. https://doi.org/10.3390/jcm13051267
Chicago/Turabian StyleKeilig, Ludger, Lena Brieskorn, Jörg Schwarze, Werner Schupp, Christoph Bourauel, and Anna Konermann. 2024. "Treatment Efficiency of Maxillary and Mandibular Orovestibular Tooth Expansion and Compression Movements with the Invisalign® System in Adolescents and Adults" Journal of Clinical Medicine 13, no. 5: 1267. https://doi.org/10.3390/jcm13051267
APA StyleKeilig, L., Brieskorn, L., Schwarze, J., Schupp, W., Bourauel, C., & Konermann, A. (2024). Treatment Efficiency of Maxillary and Mandibular Orovestibular Tooth Expansion and Compression Movements with the Invisalign® System in Adolescents and Adults. Journal of Clinical Medicine, 13(5), 1267. https://doi.org/10.3390/jcm13051267