
Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review

 ,
, 
Abstract
1. Introduction
2. Background
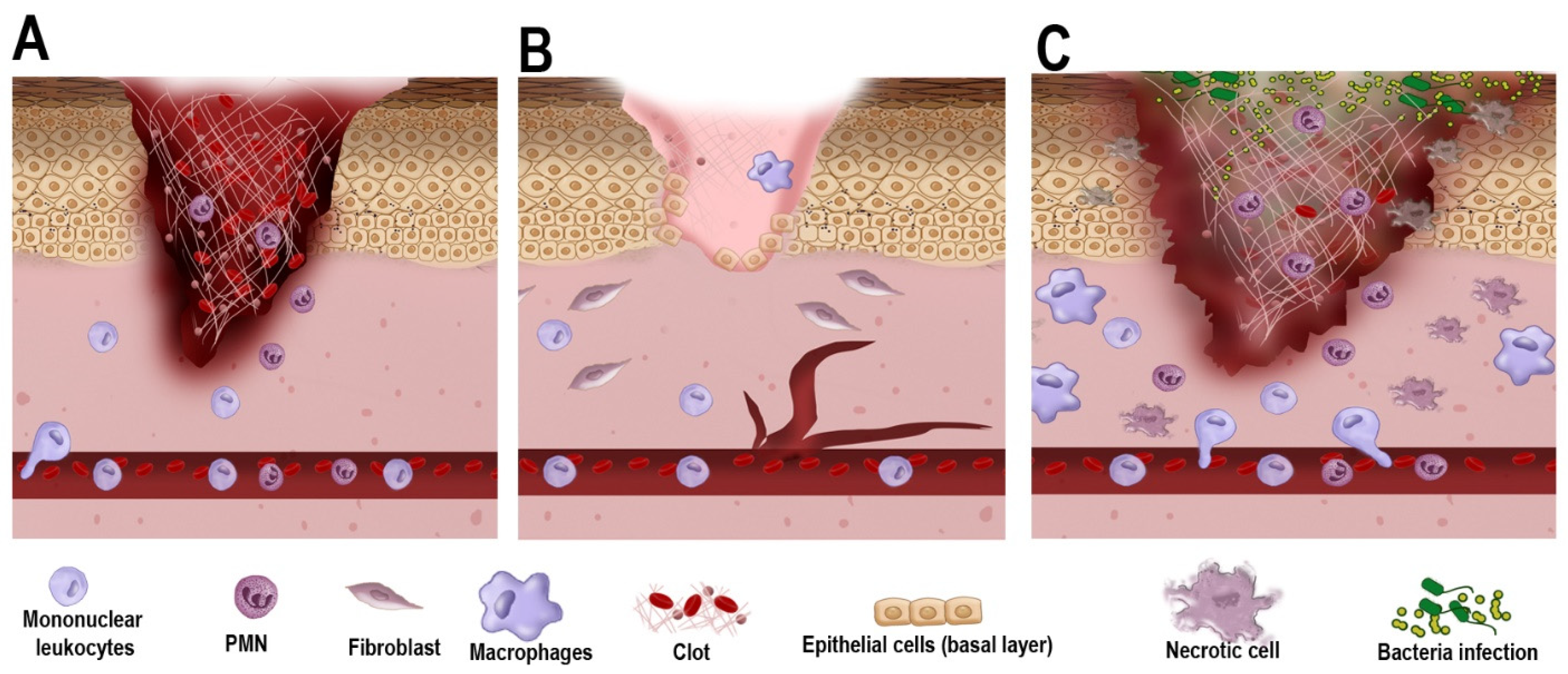
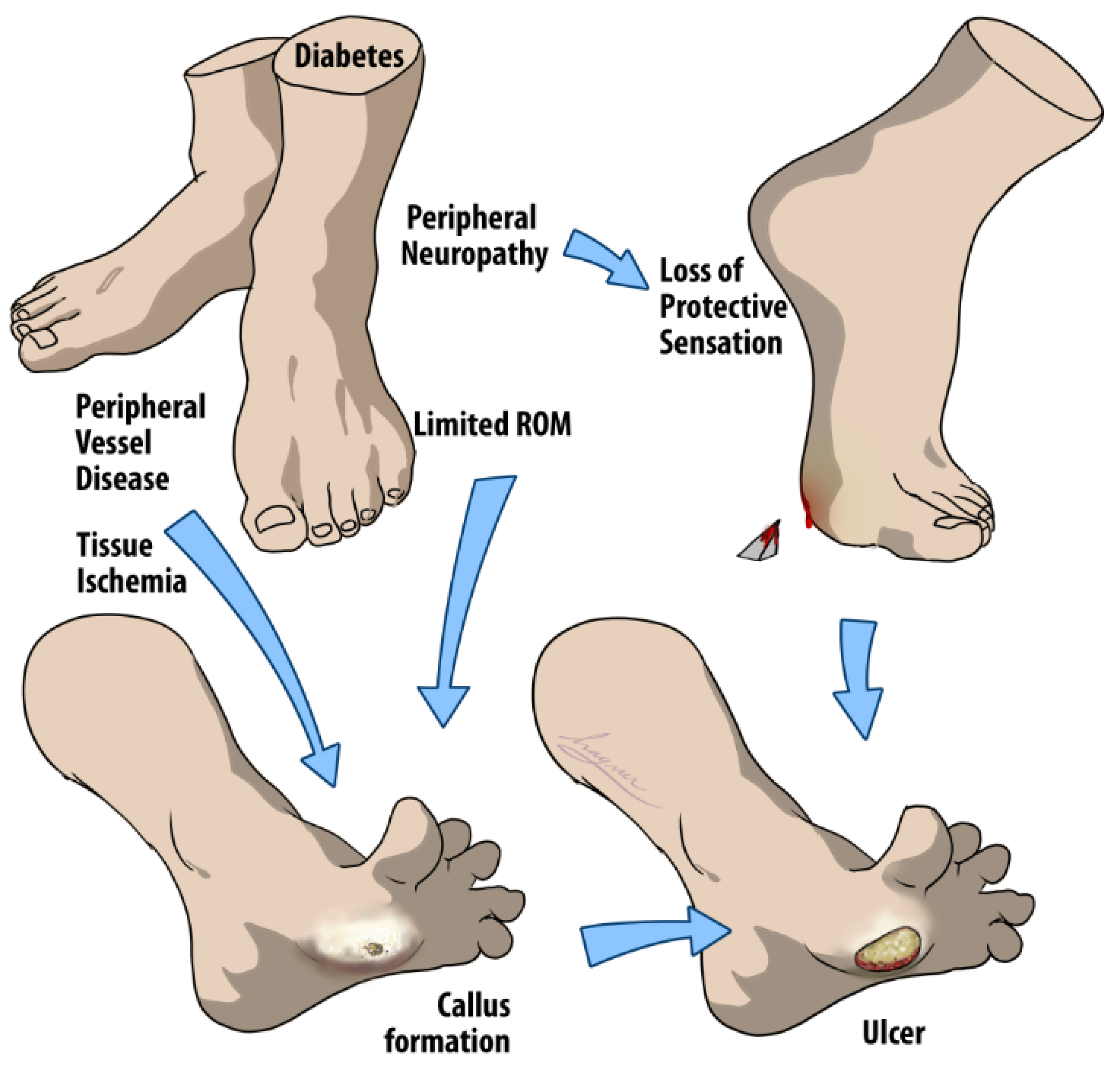
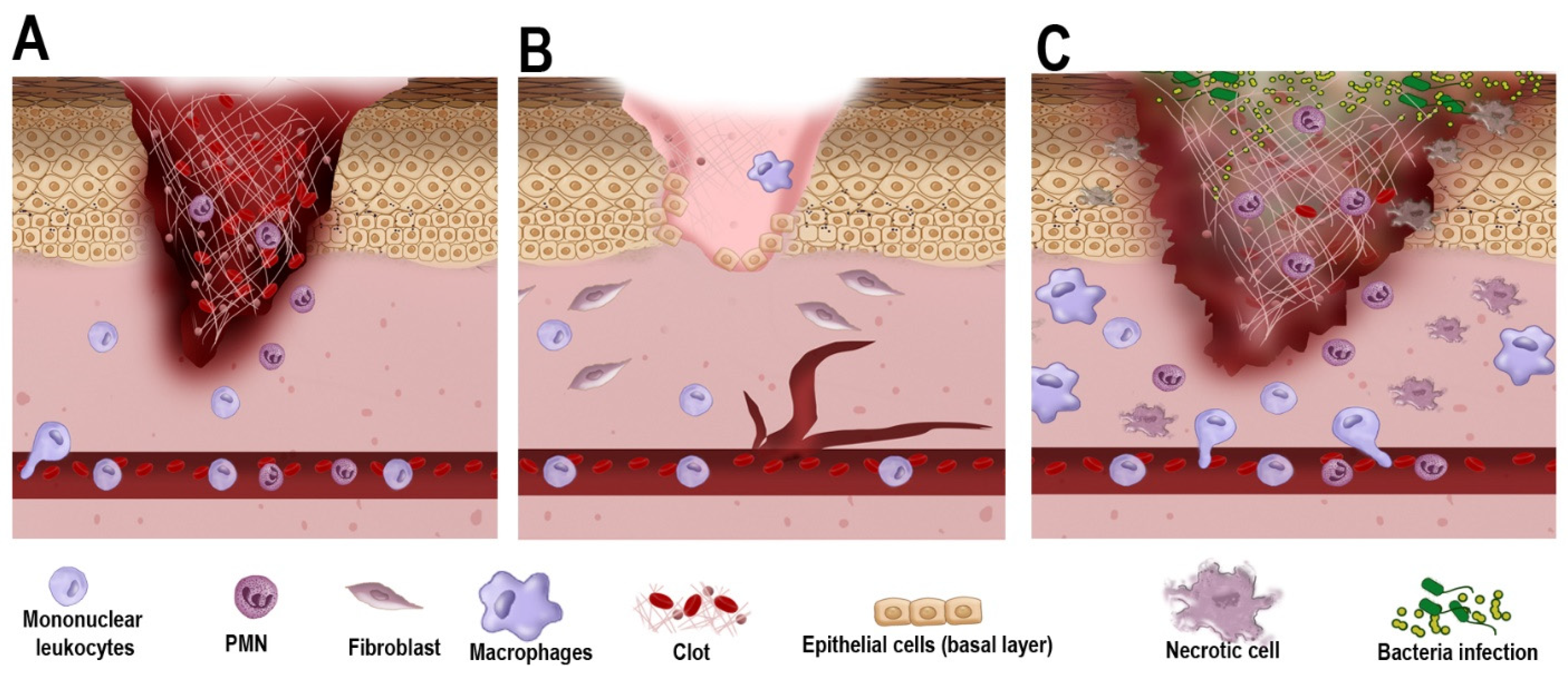
2.1. Overview of the Current Understanding of DFU Pathophysiology
2.2. Types of Treatment of DFUs
3. Materials and Methods
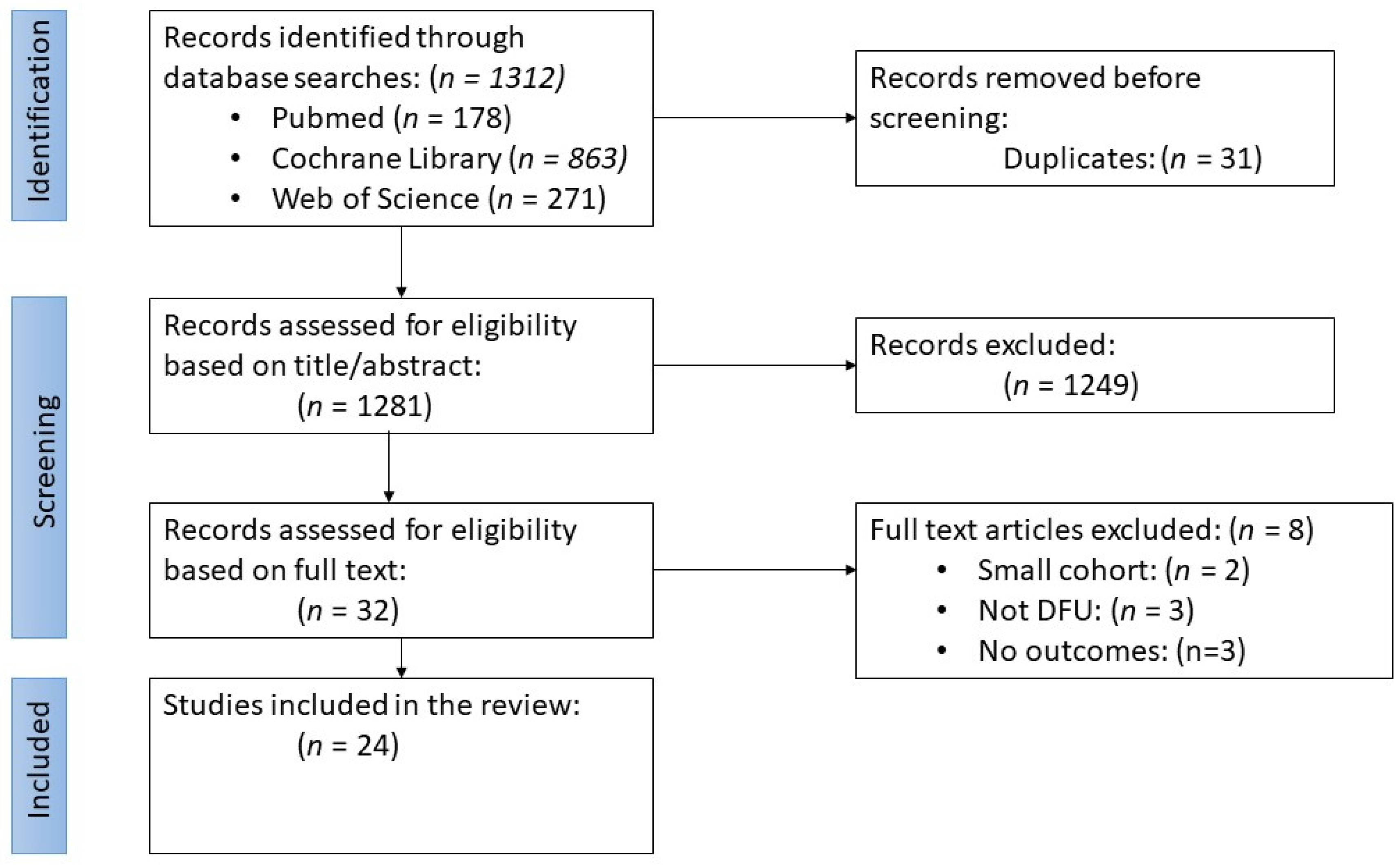
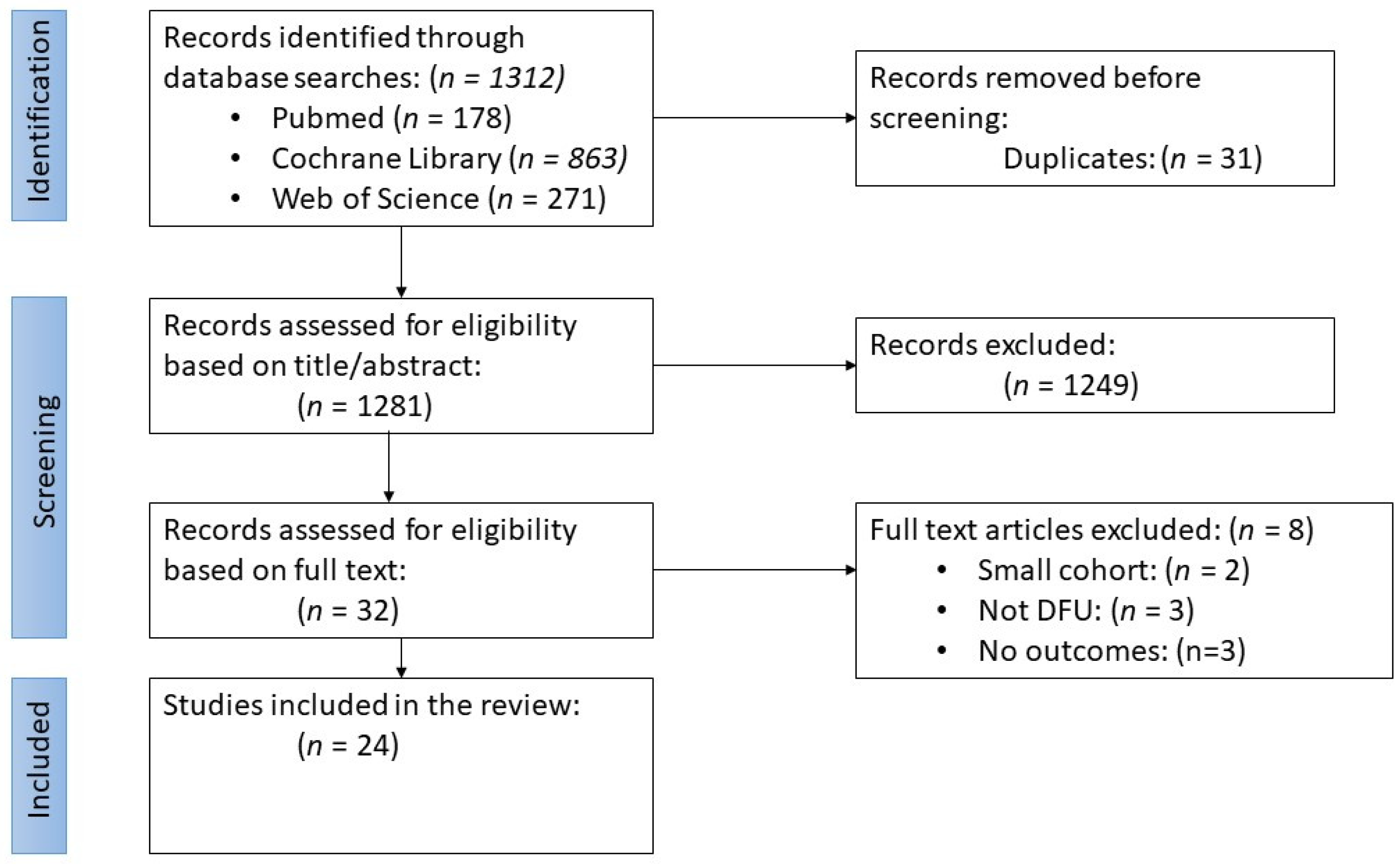
3.1. Literature Search
3.2. Study Selection and Eligibility Criteria
- Population: a sample size of 10 or more adult diabetic patients who received bioengineered skin substitutes compared to human skin allografts or standard wound care (SWC) in treating DFUs. No exclusionary or inclusionary criteria were set for patients’ sex or the presence and severity of DFU infection.
- Intervention: Application of bioengineered tissues for treatment of DFUs following wound debridement.
- Comparison: other alternate skin substitutes or SWC methods.
- Outcomes: sum and percentage of wounds achieving closure, time to wound closure (median and mean), incidence of amputation (post-treatment), and adverse events related to therapy.
3.3. Data Extraction and Synthesis
4. Results and Discussion
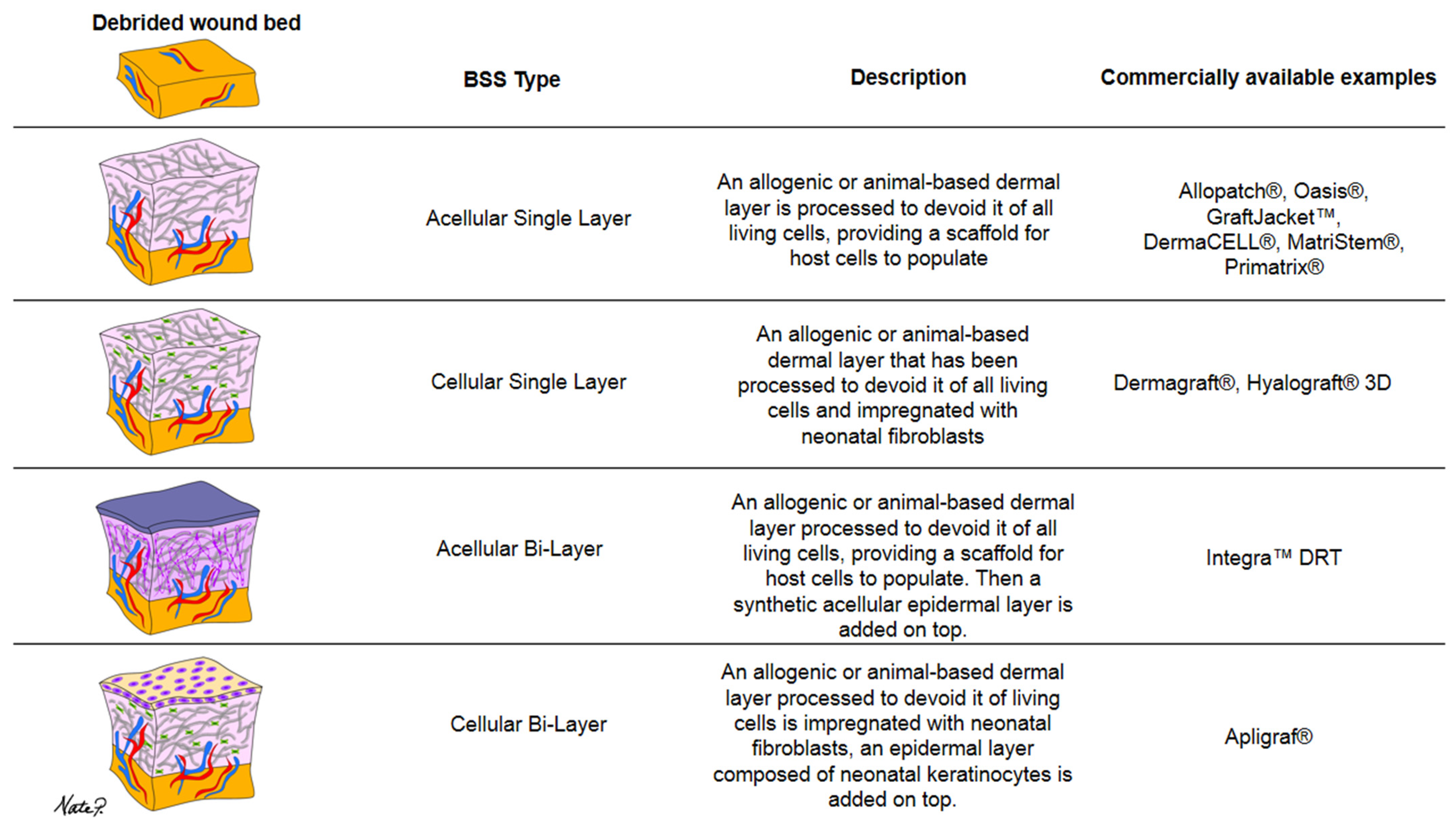
4.1. Types of BSS Found in this Scoping Review
4.2. Subject Characteristics and Investigated Outcomes
4.3. Effectiveness of BSSs in Promoting Wound Closure and Improving Patient Outcomes
4.4. Cost Effectiveness
5. Limitations
6. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Jupiter, D.C.; Thorud, J.C.; Buckley, C.J.; Shibuya, N. The impact of foot ulceration and amputation on mortality in diabetic patients. I: From ulceration to death, a systematic review. Int. Wound J. 2016, 13, 892–903. [Google Scholar] [CrossRef]
- Lavery, L.A.; Armstrong, D.G.; Wunderlich, R.P.; Mohler, M.J.; Wendel, C.S.; Lipsky, B.A. Risk Factors for Foot Infections in Individuals With Diabetes. Diabetes Care 2006, 29, 1288–1293. [Google Scholar] [CrossRef]
- Jeffcoate, W.J.; Harding, K.G. Diabetic foot ulcers. Lancet 2003, 361, 1545–1551. [Google Scholar] [CrossRef]
- Barshes, N.R.; Barshes, N.R.; Sigireddi, M.; Wrobel, J.S.; Mahankali, A.; Robbins, J.M.; Kougias, P.; Armstrong, D.G. The system of care for the diabetic foot: Objectives, outcomes, and opportunities. Diabet. Foot Ankle 2013, 4, 21847. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, L.; Nasiri, M.; Adarvishi, S. Literature review on the management of diabetic foot ulcer. World J. Diabetes 2015, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Sohail, M.; Khan, S.; Minhas, M.U.; de Matas, M.; Sikstone, V.; Hussain, Z.; Abbasi, M.; Kousar, M. Biopolymer-based biomaterials for accelerated diabetic wound healing: A critical review. Int. J. Biol. Macromol. 2019, 139, 975–993. [Google Scholar] [CrossRef] [PubMed]
- Mir, M.; Ali, M.N.; Barakullah, A.; Gulzar, A.; Arshad, M.; Fatima, S.; Asad, M. Synthetic polymeric biomaterials for wound healing: A review. Prog. Biomater. 2018, 7, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Bardill, J.R.; Laughter, M.R.; Stager, M.; Liechty, K.W.; Krebs, M.D.; Zgheib, C. Topical gel-based biomaterials for the treatment of diabetic foot ulcers. Acta Biomater. 2022, 138, 73. [Google Scholar] [CrossRef]
- Gao, D.; Zhang, Y.; Bowers, D.T.; Liu, W.; Ma, M. Functional hydrogels for diabetic wound management. APL Bioeng. 2021, 5, 31503. [Google Scholar] [CrossRef]
- Baltzis, D.; Eleftheriadou, I.; Veves, A. Pathogenesis and Treatment of Impaired Wound Healing in Diabetes Mellitus: New Insights. Adv. Ther. 2014, 31, 817–836. [Google Scholar] [CrossRef]
- Louiselle, A.E.; Niemiec, S.M.; Zgheib, C.; Liechty, K.W. Macrophage polarization and diabetic wound healing. Transl. Res. 2021, 236, 109–116. [Google Scholar] [CrossRef]
- Zarei, F.; Negahdari, B.; Eatemadi, A. Diabetic ulcer regeneration: Stem cells, biomaterials, growth factors. Artif. Cells Nanomed. Biotechnol. 2018, 46, 26–32. [Google Scholar] [CrossRef]
- Dovi, J.V.; Szpaderska, A.M.; DiPietro, L.A. Neutrophil function in the healing wound: Adding insult to injury? Thromb. Haemost. 2004, 92, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Everett, E.; Mathioudakis, N. Update on management of diabetic foot ulcers. Ann. N. Y. Acad. Sci. 2018, 1411, 153–165. [Google Scholar] [CrossRef]
- Crisologo, P.A.; Lavery, L.A.; La Fontaine, J. Conservative Offloading. Clin. Podiatr. Med. Surg. 2019, 36, 371–379. [Google Scholar] [CrossRef]
- Thomas, D.C.; Tsu, C.L.; Nain, R.A.; Arsat, N.; Fun, S.S.; Lah, N.A.S.N. The role of debridement in wound bed preparation in chronic wound: A narrative review. Ann. Med. Surg. 2021, 71, 102876. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, J.R.; Carter, M.J.; Covington, S. Frequency of Debridements and Time to Heal. JAMA Dermatol. 2013, 149, 1050. [Google Scholar] [CrossRef]
- Debridement Procedures for Managing Diabetic Foot Ulcers: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. September 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK253769/ (accessed on 3 January 2024).
- Dayya, D.; O’Neill, O.J.; Huedo-Medina, T.B.; Habib, N.; Moore, J.; Iyer, K. Debridement of Diabetic Foot Ulcers. Adv. Wound Care 2022, 11, 666. [Google Scholar] [CrossRef]
- Atkin, L. Understanding methods of wound debridement. Br J Nurs. 2014, 23, S10–S15. [Google Scholar] [CrossRef] [PubMed]
- Madhok, B.M.; Vowden, K.; Vowden, P. New techniques for wound debridement. Int. Wound J. 2013, 10, 247–251. [Google Scholar] [CrossRef]
- Rayman, G.; Vas, P.; Dhatariya, K.; Driver, V.; Hartemann, A.; Londahl, M.; Piaggesi, A.; Driver, V.; Apelqvist, J.; Attinger, C.; et al. Guidelines on use of interventions to enhance healing of chronic foot ulcers in diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1), e3283. [Google Scholar] [CrossRef]
- Anghel, E.L.; DeFazio, M.V.; Barker, J.C.; Janis, J.E.; Attinger, C.E. Current Concepts in Debridement. Plast. Reconstr. Surg. 2016, 138, 82S–93S. [Google Scholar] [CrossRef]
- Tombulturk, F.K.; Kanigur-Sultuybek, G. A molecular approach to maggot debridement therapy with Lucilia sericata and its excretions/secretions in wound healing. Wound Repair Regen. 2021, 29, 1051–1061. [Google Scholar] [CrossRef]
- Smith, F.; Dryburgh, N.; Donaldson, J.; Mitchell, M. Debridement for surgical wounds. Cochrane Database Syst. Rev. 2013, 2013, CD006214. [Google Scholar] [CrossRef]
- Santema, T.B.; Poyck, P.P.C.; Ubbink, D.T. Skin grafting and tissue replacement for treating foot ulcers in people with diabetes. Cochrane Database Syst. Rev. 2016, 2016, CD011255. [Google Scholar] [CrossRef]
- Kohlhauser, M.; Luze, H.; Nischwitz, S.P.; Kamolz, L.P. Historical Evolution of Skin Grafting—A Journey through Time. Medicina 2021, 57, 348. [Google Scholar] [CrossRef]
- Ramanujam, C.L.; Zgonis, T. An Overview of Autologous Skin Grafts and Advanced Biologics for the Diabetic Foot. Clin. Podiatr. Med. Surg. 2012, 29, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Serra, R.; Rizzuto, A.; Rossi, A.; Perri, P.; Barbetta, A.; Abdalla, K.; Caroleo, S.; Longo, C.; Amantea, B.; Sammarco, G.; et al. Skin grafting for the treatment of chronic leg ulcers—A systematic review in evidence-based medicine. Int. Wound J. 2017, 14, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Goverman, J.; Kraft, C.T.; Fagan, S.; Levi, B. Back Grafting the Split-Thickness Skin Graft Donor Site. J. Burn. Care Res. 2017, 38, e443–e449. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Mohapatra, D.P.; Chittoria, R.K.; Subbarayan, E.; Reddy, S.K.; Chavan, V.; Aggarwal, A.; Reddy, L.C. Human skin allograft: Is it a viable option in management of burn patients? J. Cutan. Aesthetic Surg. 2019, 12, 132. [Google Scholar] [CrossRef]
- Kearney, J.N. Guidelines on processing and clinical use of skin allografts. Clin. Dermatol. 2005, 23, 357–364. [Google Scholar] [CrossRef]
- Roy, A.; Griffiths, S. Intermediate layer contribution in placental membrane allografts. J. Tissue Eng. Regen. Med. 2020, 14, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S.; Baganizi, D.R.; Sahu, R.; Dosunmu, E.; Chaudhari, A.; Vig, K.; Pillai, S.R.; Singh, S.R.; Dennis, V.A. Immunological challenges associated with artificial skin grafts: Available solutions and stem cells in future design of synthetic skin. J. Biol. Eng. 2017, 11, 49. [Google Scholar] [CrossRef]
- Yamamoto, T.; Iwase, H.; King, T.W.; Hara, H.; Cooper, D.K.C. Skin xenotransplantation: Historical review and clinical potential. Burns 2018, 44, 1738–1749. [Google Scholar] [CrossRef]
- Cooper, D.K.; Ezzelarab, M.B.; Hara, H.; Iwase, H.; Lee, W.; Wijkstrom, M.; Bottino, R. The pathobiology of pig-to-primate xenotransplantation: A historical review. Xenotransplantation 2016, 23, 83–105. [Google Scholar] [CrossRef] [PubMed]
- Rijal, N.P.; Narmoneva, D.A. Biomaterials for diabetic wound-healing therapies. In Wound Healing, Tissue Repair, and Regeneration in Diabetes; Elsevier: Amsterdam, The Netherlands, 2020; pp. 273–304. [Google Scholar] [CrossRef]
- Oualla-Bachiri, W.; Fernández-González, A.; Quiñones-Vico, M.I.; Arias-Santiago, S. From Grafts to Human Bioengineered Vascularized Skin Substitutes. Int. J. Mol. Sci. 2020, 21, 8197. [Google Scholar] [CrossRef] [PubMed]
- Alrubaiy, L. Skin Substitutes: A Brief Review of Types and Clinical Applications. Oman Med. J. 2009, 24, 4–6. [Google Scholar] [CrossRef]
- Tchanque-Fossuo, C.N.; Dahle, S.E.; Lev-Tov, H.; West, K.I.M.; Li, C.S.; Rocke, D.M.; Isseroff, R.R. Cellular versus acellular matrix devices in the treatment of diabetic foot ulcers: Interim results of a comparative efficacy randomized controlled trial. J. Tissue Eng. Regen. Med. 2019, 13, 1430–1437. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Sabolinski, M.L.; Gibbons, G. Comparative effectiveness of a bilayered living cellular construct and an acellular fetal bovine collagen dressing in the treatment of venous leg ulcers. J. Comp. Eff. Res. 2018, 7, 797–805. [Google Scholar] [CrossRef]
- Nilforoushzadeh, M.A.; Sisakht, M.M.; Amirkhani, M.A.; Seifalian, A.M.; Banafshe, H.R.; Verdi, J.; Nouradini, M. Engineered skin graft with stromal vascular fraction cells encapsulated in fibrin–collagen hydrogel: A clinical study for diabetic wound healing. J. Tissue Eng. Regen. Med. 2020, 14, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Orgill, D.P.; Galiano, R.D.; Glat, P.M.; Kaufman, J.P.; Carter, M.J.; DiDomenico, L.A.; Zelen, C.M. Use of a purified reconstituted bilayer matrix in the management of chronic diabetic foot ulcers improves patient outcomes vs standard of care: Results of a prospective randomised controlled multi-centre clinical trial. Int. Wound J. 2022, 19, 1197–1209. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Tettelbach, W.H.; Chang, T.J.; De Jong, J.L.; Glat, P.M.; Hsu, J.H.; Kelso, M.R.; Niezgoda, J.A.; Tucker, T.L.; Labovitz, J.M. Observed impact of skin substitutes in lower extremity diabetic ulcers: Lessons from the Medicare Database (2015–2018). J. Wound Care 2021, 30 (Suppl. S7), S5–S16. [Google Scholar] [CrossRef]
- Campitiello, F.; Mancone, M.; Della Corte, A.; Guerniero, R.; Canonico, S. To evaluate the efficacy of an acellular Flowable matrix in comparison with a wet dressing for the treatment of patients with diabetic foot ulcers: A randomized clinical trial. Updates Surg. 2017, 69, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Djavid, G.E.; Tabaie, S.M.; Tajali, S.B.; Totounchi, M.; Farhoud, A.; Fateh, M.; Taghizadeh, S. Application of a collagen matrix dressing on a neuropathic diabetic foot ulcer: A randomised control trial. J. Wound Care 2020, 29 (Suppl. S3), S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Cazzell, S.M.; Lange, D.L.; Dickerson, J.E.; Slade, H.B. The Management of Diabetic Foot Ulcers with Porcine Small Intestine Submucosa Tri-Layer Matrix: A Randomized Controlled Trial. Adv. Wound Care 2015, 4, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Driver, V.R.; Lavery, L.A.; Reyzelman, A.M.; Dutra, T.G.; Dove, C.R.; Kotsis, S.V.; Chung, K.C. A clinical trial of Integra Template for diabetic foot ulcer treatment. Wound Repair Regen. 2015, 23, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Frykberg, R.G.; Cazzell, S.M.; Arroyo-Rivera, J.; Tallis, A.; Reyzelman, A.M.; Saba, F.; Gilbert, T.W. Evaluation of tissue engineering products for the management of neuropathic diabetic foot ulcers: An interim analysis. J. Wound Care 2016, 25 (Suppl. S7), S18–S25. [Google Scholar] [CrossRef]
- Rosa, S.S.R.F.; Rosa, M.F.F.; Marques, M.P.; Guimarães, G.A.; Motta, B.C.; Macedo, Y.C.L.; Inazawa, P.; Dominguez, A.; Macedo, F.S.; Lopes, C.A.P.; et al. Regeneration of Diabetic Foot Ulcers Based on Therapy with Red LED Light and a Natural Latex Biomembrane. Ann. Biomed. Eng. 2019, 47, 1153–1164. [Google Scholar] [CrossRef]
- You, H.J.; Han, S.K.; Rhie, J.W. Randomised controlled clinical trial for autologous fibroblast-hyaluronic acid complex in treating diabetic foot ulcers. J. Wound Care 2014, 23, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Zelen, C.M.; Serena, T.E.; Snyder, R.J. A prospective, randomised comparative study of weekly versus biweekly application of dehydrated human amnion/chorion membrane allograft in the management of diabetic foot ulcers. Int. Wound J. 2014, 11, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Zelen, C.M.; Gould, L.; Serena, T.E.; Carter, M.J.; Keller, J.; Li, W.W. A prospective, randomised, controlled, multi-centre comparative effectiveness study of healing using dehydrated human amnion/chorion membrane allograft, bioengineered skin substitute or standard of care for treatment of chronic lower extremity diabetic ulcers. Int. Wound J. 2015, 12, 724–732. [Google Scholar] [CrossRef]
- Zelen, C.M.; Serena, T.E.; Gould, L.; Le, L.; Carter, M.J.; Keller, J.; Li, W.W. Treatment of chronic diabetic lower extremity ulcers with advanced therapies: A prospective, randomised, controlled, multi-centre comparative study examining clinical efficacy and cost. Int. Wound J. 2016, 13, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Zelen, C.M.; Orgill, D.P.; Serena, T.; Galiano, R.; Carter, M.J.; DiDomenico, L.A.; Keller, J.; Kaufman, J.; Li, W.W. A prospective, randomised, controlled, multicentre clinical trial examining healing rates, safety and cost to closure of an acellular reticular allogenic human dermis versus standard of care in the treatment of chronic diabetic foot ulcers. Int. Wound J. 2017, 14, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Cazzell, S.; Vayser, D.; Pham, H.; Walters, J.; Reyzelman, A.; Samsell, B.; Moore, M. A randomized clinical trial of a human acellular dermal matrix demonstrated superior healing rates for chronic diabetic foot ulcers over conventional care and an active acellular dermal matrix comparator. Wound Repair Regen. 2017, 25, 483–497. [Google Scholar] [CrossRef]
- Glat, P.; Orgill, D.P.; Galiano, R.; Armstrong, D.; Serena, T.; DiDomenico, L.A.; Kaufman, J.; Carter, M.J.; Jacobs, A.M.; Zelen, C.M. Placental Membrane Provides Improved Healing Efficacy and Lower Cost Versus a Tissue-Engineered Human Skin in the Treatment of Diabetic Foot Ulcerations. Plast. Reconstr. Surg. Glob. Open 2019, 7, 2371. [Google Scholar] [CrossRef]
- Sanders, L.; Landsman, A.S.; Landsman, A.; Keller, N.; Cook, J.; Cook, E.; Hopson, M. Prospective, multicenter, randomized, controlled clinical trial comparing a bioengineered skin substitute to a human skin allograft. Ostomy/Wound Manag. 2014, 60, 26–38. [Google Scholar]
- Kirsner, R.S.; Sabolinski, M.L.; Parsons, N.B.; Skornicki, M.; Marston, W.A. Comparative effectiveness of a bioengineered living cellular construct vs. a dehydrated human amniotic membrane allograft for the treatment of diabetic foot ulcers in a real-world setting. Wound Repair Regen. 2015, 23, 737–744. [Google Scholar] [CrossRef]
- Kraus, I.; Sabolinski, M.L.; Skornicki, M.; Parsons, N.B. The Comparative Effectiveness of a Human Fibroblast Dermal Substitute versus a Dehydrated Human Amnion/Chorion Membrane Allograft for the Treatment of Diabetic Foot Ulcers in a Real-world Setting. Wounds A Compend. Clin. Res. Pract. 2017, 29, 125–132. [Google Scholar]
- Fitzgerald, R.H.; Sabolinski, M.L.; Skornicki, M. Evaluation of Wound Closure Rates Using a Human Fibroblast-derived Dermal Substitute Versus a Fetal Bovine Collagen Dressing: A Retrospective Study. Wound Manag. Prev. 2019, 65, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, A.M.; Waycaster, C.R.; Landsman, A.L. Wound closure in patients with DFU: A cost-effectiveness analysis of two cellular/tissue-derived products. J. Wound Care 2015, 24, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Ananian, C.E.; Dhillon, Y.S.; Van Gils, C.C.; Lindsey, D.C.; Otto, R.J.; Dove, C.R.; Pierce, J.T.; Saunders, M.C. A multicenter, randomized, single-blind trial comparing the efficacy of viable cryopreserved placental membrane to human fibroblast-derived dermal substitute for the treatment of chronic diabetic foot ulcers. Wound Repair Regen. 2018, 26, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Snyder, R. A Comparative Analysis of the Cost Effectiveness of Five Advanced Skin Substitutes in the Treatment of Foot Ulcers in Patients with Diabetes. Ann. Rev. Res. 2020, 6, 1–14. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Product Name | Company | Product Description |
|---|---|---|---|
| Armstrong et al., 2022 | Derma-Gide® | Geistlich Pharma North America, Inc., Princeton, NJ, USA | Bi-layered acellular matrix derived from porcine material |
| Campitiello et al., 2017 | Integra Flowable Wound Matrix® | Integra LifeScience, Corp., Princeton, NJ, USA | Bi-layered acellular matrix from bovine tendon collagen and glycosaminoglycan (chondroitin-6-sulfate) |
| Cazzell et al., 2015, Gilligan et al., 2015, Tchangque Fossuo et al., 2019 | OASIS® Extracellular Matrix | Cook Biotech Inc., West Lafayette, IN, USA; exclusively marketed by Smith and Nephew, Inc., Memphis, TN, USA | Tri-layer porcine small intestine submucosa, acellular, collagen-based extracellular matrix |
| Djavid et al., 2020 | Tebaderm® Collagen Matrix | Tebaderm manufacturer, Treetta Advanced Wound Care Products., Mashhad, Iran | Collagen matrix dressing including chitosan/collagen hydrogel |
| Driver et al., 2015 | Omnigraft® Dermal Regeneration Matrix | Integra LifeScience, Corp., Princeton, NJ, USA | Bi-layered with bioengineered Silicone and Collagen/Chondroitin-6-sulfate matrix |
| Rosa et al., 2019 | RAPHA® System–Latex biomembrane | Department of the Industrial Complex and Innovation in Health (DECIIS) and the Engineering and Innovation Laboratory (LEI/UnB)., Brasilia, Federal District, Brazil | Natural latex biomembrane originating from Hevea brasiliensis |
| You et al., 2014 | Hyalograft 3D | CHA BIO&DIOSTECH CO LTD, Seongnam, South Korea | Autologous skin fibroblasts in 3D scaffolds formed of hyaluronic acid derivatives |
| Zelen et al., 2014, Zelen et al., 2015, Kisner et al., 2015, Kraus et al., 2017, Glat et al., 2019 | Apligraf® | Organogenesis, Inc., Canton, MA, USA | Bi-layered cellular skin substitute composed of human neonatal fibroblasts cultured in a bovine type I collagen matrix over human neonatal epidermal keratinocytes. |
| Zelen et al., 2014, Zelen et al., 2015, Kisner et al., 2015, Kraus et al., 2017 | EpiFix® | MIMEDX Group, Inc., Marietta, GA, USA | Composed by placental tissue allograft containing human amnion/chorion membrane |
| Zelen et al., 2016, Zelen et al., 2018 | AlloPatch® Pliable | MTF Biologics, Corp., Edison, NJ, USA | Human acellular dermal matrix |
| Ananian et al., 2018, Sabolinski et al., 2019 | Grafix Prime® | Osiris Therapeutics, Inc., Columbia, MD, USA | Viable cryopreserved human placental membrane |
| Glat et al., 2019 | AmnioBand® Membrane | MTF Biologics, Corp., Edison, NJ, USA | Human acellular placental matrix |
| Sanders et al., 2014, Gilligan et al., 2015, Frykberg et al., 2015, Ananian et al., 2018, Sabolinski et al., 2019, Fitzgerald et al., 2019, Tchangque Fossuo et al., 2019 | Dermagraft® | Organogenesis, Inc., Canton, MA, USA | Three-dimensional polyglactin mesh substrate containing human neonatal dermal fibroblasts |
| Sanders et al., 2014 | TheraSkin® | LifeNet Health, Virginia Beach, VA, USA | Human extracellular matrix containing viable human fibroblasts and keratinocytes |
| Cazzell et al., 2017 | DermACELL® | MATRACELL® technology from LifeNet Health., Virginia Beach, VA, USA | Human acellular tissue matrix allograft |
| GraftJacket® | LifeCell, Corp., Branchburg, NJ, USA | Human acellular dermal matrix | |
| Fitzgerald et al., 2019 | Primatrix® | Integra LifeScience, Corp., Princeton, NJ, USA | Fetal bovine acellular dermal matrix |
| Frykberg et al., 2016 | MatriStem® | Acell, Inc., Columbia, MD, USA | Urinary Bladder Matrix |
| Study | Group Distribution per Type of Treatment Modality | Number of DFUs | Wound Closure (n, %) | Time to Wound Closure | Cost Per-Patient | Amputation, n (%) | Treatment Related Adverse Events (n, %) |
|---|---|---|---|---|---|---|---|
| Armstrong et al., 2021 | Group 1 Adv | 12,676 | NR | NR | NR | Minor: 490 (3.9%) Major: 197 (1.6%) | NR |
| Group 2 Adv FPFU Group 2 Adv No FPFU | 1131 1131 | Minor: 22 (1.9%) Major: <11 (<1%) Minor: 51 (4.5%) Major: 18 (1.6%) | |||||
| SWC Group 1 | 12,676 | NR | NR | NR | Minor: 551 (4.3%) Major: 402 (3.2%) | NR | |
| SWC Group 2 | 1131 | Minor: 47 (4.2%) Major: 30 (2.7%) | |||||
| Armstrong et al., 2022 | Derma-Gide® | 20 | 17 (85%) | Mean: 37 days | $1731 | NR | NR |
| SWC | 20 | 6 (30%) | Mean: 67 days | SWC: NR | NR | NR | |
| Campitiello et al., 2017 | Integra | 23 | 20 (86.95%) | Mean: 29.73 days | NR | 10 (43.48%) | 10 (43.48%) |
| SWC | 23 | 12 (53.17%) | Mean: 42.78 days | NR | 15 (65.2%) | 15 (65.2%) | |
| Cazzell et al., 2015 | OASIS® Extracellular Matrix | 41 | 22 (54%) | Median: 9 weeks | NR | NR | 1 (2.4%) |
| SWC | 41 | 13 (32%) | Median: 11 weeks | NR | NR | 0 (0%) | |
| Djavid et al., 2020 | Tebaderm® Collagen Matrix | 30 | 18 (60%) | Median: 11.8 weeks | NR | NR | 2 (6.67%) |
| SWC | 31 | 11 (35.5%) | Median: 21.4 weeks | NR | NR | 3 (9.68%) | |
| Driver et al., 2015 | Omnigraft® Dermal Regeneration Matrix | 154 | 79 (51%) | Median: 43 days | NR | NR | 7 (4.55%) |
| SWC | 153 | 49 (32%) | Median: 78 days | 8 (5.23%) | |||
| Frykberg et al., 2015 | Dermagraft® | 163 | NR | NR | NR | 9 (5.5%) | 9 (5.5%) |
| SWC | 151 | 19 (12.6%) | 19 (12.6%) | ||||
| Rosa et al., 2019 | RAPHA® System–Latex biomembrane with HCP | 12 | 4 (66.6%) | NR | NR | NR | NR |
| RAPHA® System–Latex biomembrane without HCP | 8 | 2 (25%) | |||||
| SWC | 5 | 1 (20%) | |||||
| You et al., 2014 | Hyalograft 3D | 31 | 26 (84%) | Mean: 36.4 days | NR | NR | No adverse events related to the study dressings |
| SWC | 32 | 11 (34%) | Median: 48.4 days | ||||
| Zelen et al., 2014 | Apligraf® | 20 | 9 (45%) | Median: 49 days | Mean: $9216.00 | NR | No adverse events related to the study dressings |
| EpiFix® | 20 | 19 (95%) | Median: 49 days | Mean: $1669.00 | |||
| SWC | 20 | 7 (35%) | Median: 49 days | NR | |||
| Zelen et al., 2015 | Apligraf® | 33 | 24 (73%) | Mean: 47.9 days, Median:NR | Mean: $8918 | NR | No adverse events related to the study dressings |
| EpiFix® | 32 | 31 (97%) | Mean:NR, Median: 23.6 days | Mean: $2798 | |||
| SWC | 35 | 18 (51%) | Mean: 57.4 days, Median: NR | NR | |||
| Zelen et al., 2016 | AlloPatch® Pliable | 20 | 13 (65%) | Mean: 40 days | Mean: $1475 | NR | No adverse events related to the study dressings |
| SWC | 20 | 1 (5%) | Mean: 77 days | Median: $963 | |||
| Zelen et al., 2018 | AlloPatch® Pliable | 40 | AlloPatch: 34 (68%) | Mean: 38 days | Mean: $1200 | NR | No adverse events related to the study dressings |
| SWC | 40 | SWC: 12 (30%) | Mean: 72 days | Median: $680 | |||
| Ananian et al., 2018 | Grafix Prime® | 31 | 15 (48.4%) | Mean: 38 days | $3846.25 | NR | 3 (9.7%) |
| Dermagraft® | 31 | 12 (38.7%) | Mean: 31 days | $7968.75 | 10 (32.26%) | ||
| Glat et al., 2019 | AmnioBand® Membrane | 30 | 27 (90%) | Mean: 32 days | Mean: $2900.00 | NR | No adverse events related to the study dressings |
| Apligraf® | 30 | 12 (40%) | Mean: 63 days | Mean: $9700.00 | |||
| Kirsner et al., 2015 | Apligraf® | 163 | 72% | Median: 13.3 weeks | NR | NR | NR |
| EpiFix® | 63 | 47% | Median: 26 weeks | ||||
| Kraus et al., 2017 | Apligraf® | 59 | 76% | Median: 12 weeks | NR | 8.9% of all patients enrolled in the study underwent amputation or bone resection | NR |
| EpiFix® | 63 | 50% | Median: 19.4 weeks | ||||
| Sabolinski et al., 2019 | Dermagraft® | 1444 | 61% | Median: 20 weeks | NR | NR | No significant differences between groups in adverse events |
| Grafix Prime® | 178 | 46% | Median: 36 weeks | ||||
| Sanders et al., 2014 | Dermagraft® | 12 | 4 (33.3%) | Mean: 12.5 weeks | NR | N/A | No adverse ulcer related events were observed |
| TheraSkin® | 11 | 7 (63.6%) | Mean: 8.9 weeks | ||||
| Cazzell et al., 2017 | DermACELL® | 53 | 29 (54.7%) | NR | NR | Subjects with amputations due to infection were excluded from the protocol | Not speficic adverse events repored |
| GraftJacket® | 23 | 9 (39.13%) | |||||
| SWC | 56 | 30 (53.57%) | |||||
| Fitzgerald et al., 2019 | Dermagraft® | 108 | 69 (64%) | Median: 14.6 weeks | NR | NR | NR |
| Primatrix® | 100 | 43 (43%) | Median: 25 weeks | ||||
| Frykberg et al., 2016 | MatriStem® | 27 | 7 (25.9%) | Mean: 69.8 days | $1780.63 | 9 (33.3%) | No adverse events were observed with procedure or product related |
| Dermagraft® | 29 | 9 (31.0%) | Mean: 65.7 days | $11,371.43 | 19 (65.5%) | ||
| Gilligan et al., 2015 | OASIS® Extracellular Matrix | 13 | 10 (77%) | Mean: 36 days | $2522 | NR | NR |
| Dermagraft® | 13 | 11 (85%) | Mean: 41 days | $3889 | |||
| Tchangque Fossuo et al., 2019 | Dermagraft® | 17 | 8 (47.1%) | NR | NR | NR | None of the adverse events were related to the procedures and products |
| OASIS® Extracellular Matrix | 19 | 14 (73.7%) | |||||
| SWC | 19 | 11 (57.9%) |
| Study | Treatment Modality | Age, Mean (SD) | Race: n (%) | Ethnicity: n (%) | Sex: n (%) | Wound Duration | Area of Ulcer (cm2) |
|---|---|---|---|---|---|---|---|
| Ananian et al., 2018 | Grafix Prime® | 55.13 (12.09) | White: 32 (84.2%) | Hispanic: 22 (57.9%) | Male: 28 (73.7%) | Mean: 199.32, Median: 191 days | Mean: 7.15, Median: 5.0 |
| Black/African American: 3 (7.9%) | |||||||
| American Indian/ Alaskan Native: 1 (2.6%) | Non-Hispanic: 16 (42.9%) | Female: 10 (6.3%) | |||||
| Other: 2 (5.3%) | |||||||
| Dermagraft® | 58.1 (11.89) | White: 34 (91.9%) | Hispanic: 21 (56.8%) | Male: 32 (86.5%) | Mean: 146.32, Median: 125 days | Mean: 5.7, Median: 5.0 | |
| Black/African American: 1 (2.7%) | |||||||
| American Indian/ Alaskan Native: 0 (0%) | Non-Hispanic: 16 (43.2%) | Female: 5 (13.5%) | |||||
| Other: 2 (5.4%) | |||||||
| Armstrong et al., 2021 * | Group 1 SWC | 70.8 (11.7) | White: 10,226 (81.7%) | NR | Male: 7296 (58.3%) | NR | NR |
| Black: 1589 (12.7%) | |||||||
| Hispanic: 273 (2.2%) | |||||||
| Native American: 122 (1.0%) | Female: 5214 (41.7%) | ||||||
| Asian: 72 (0.6%) | |||||||
| Other: 123 (1.0%) | |||||||
| Unknown: 105 (0.8%) | |||||||
| Group 1 Adv | 70.7 (11.5) | White: 10,122 (82.2%) | NR | Male: 7268 (59.0%) | NR | NR | |
| Black: 1342 (10.9%) | |||||||
| Hispanic: 373 (3.0%) | |||||||
| Native American: 122 (1.0%) | |||||||
| Asian: 84 (0.7%) | Female: 5045 (41.0%) | ||||||
| Other: 137 (1.1%) | |||||||
| Unknown: 133 (1.1%) | |||||||
| Group 2 SWC | 71.4 (11.4) | White: 933 (82.0%) | NR | Male: 661 (58.0%) | NR | NR | |
| Black: 142 (13.0%) | |||||||
| Hispanic: 22 (2.0%) | |||||||
| Native American: 34 (3.0%) | |||||||
| Asian: 34 (3.0%) | Female: 470 (42.0%) | ||||||
| Other: 34 (3.0%) | |||||||
| Unkown: 34 (3.0%) | |||||||
| Group 2 Adv FPFU | 71.9 (11.2) | White: 954 (84.0%) | NR | Male: 643 (58.0%) | NR | NR | |
| Black: 109 (10.0%) | |||||||
| Hispanic: 36 (3.0%) | |||||||
| Native American: 32 (3.0%) | |||||||
| Asian: 32 (3.0%) | Female: 488 (44.0%) | ||||||
| Other: 32 (3.0%) | |||||||
| Unkown: 32 (3.0%) | |||||||
| Group 2 Adv No FPFU | 70.8 (11.6) | White: 929 (82.4%) | NR | Male: 678 (60.1%) | NR | NR | |
| Black: 126 (11.2%) | |||||||
| Hispanic: 39 (3.5%) | |||||||
| Native American: 34 (3.0%) | Female: 450 (49.9%) | ||||||
| Asian: 34 (3.0%) | |||||||
| Other: 34 (3.0%) | |||||||
| Unkown: 34 (3.0%) | |||||||
| Armstrong et al., 2022 | Derma-Gide® | 59.3 (13.35) | Caucasian: 20 (100%) | NR | Male: 13 (65%) | Mean SD: 12.1 (8.21) weeks | Mean SD: 2.5 (2.16) |
| African American: 0 (0%) | Female: 7 (35%) | Median (IQR): 9 (8) weeks | Median (IQR): 1.7 (1.4) | ||||
| SWC | 66.5 (11.26) | Caucasian: 19 (95%) | NR | Male: 12 (60%) | Mean SD: 15.6 (12.96) weeks | Mean SD: 3.5 (2.85) | |
| African American: 1 (5%) | Female: 8 (40%) | Median (IQR): 8 (17) weeks | Median (IQR): 3.0 (3.8) | ||||
| Campitello et al., 2017 | Integra Flowable Wound Matrix® | 64.04 ± 8.94 | NR | NR | Male: 15 (65.22%) | Mean: 38.56 (12.61) weeks | NR |
| Female: 8 (34.78%) | |||||||
| SWC | 62.08 ± 7.71 | NR | NR | Male: 13 (56.53%) | Mean: 39.5 (9.90) weeks | NR | |
| Female: 10 (43.47%) | |||||||
| Cazzell et al., 2015 | OASIS® Extracellular Matrix | 57.1 (10.9) | White: 33 (81%) | Hispanic/Latio: 10 (24%) | Male: 32 (78%) | Mean (SD): 21.3 (12.3) weeks | Mean (SD): 2.1 (2.3) |
| Non-white: 8 (20%) | Non-Hispanic/Latino: 31 (76%) | Female: 9 (22%) | Median (Min–Max): 19.0 (7.0–49.0) weeks | Median (Min–Max): 1.2 (0.3–10.5) | |||
| SWC | 56.6 (10.8) | White: 33(81%) | Hispanic/Latio: 16 (39%) | Male: 30 (73%) | Mean (SD): 22.2 (13.5) | Mean (SD): 2.6 (7.5) | |
| Non-white: 8 (20%) | Non-Hispanic/Latino: 25 (61%) | Female: 11 (27%) | Median (Min–Max): 18.0 (7.0–49.0) | Median (Min–Max): 1.0 (0.4–48.4) | |||
| Cazzell et al., 2017 | DermACELL® | 59.1 (12.176) | NR | NR | Male: 57 (80.3%) | Mean (SD): 40.0 (71.56) weeks | Mean (SD): 3.9 (4.15) |
| Female: 14 (19.7%) | Median: 20.1 (6.0–479.0) weeks | Median: 1.9 (1.0–21.0) | |||||
| SWC | 56.9 (10.86) | NR | NR | Male: 51 (73.9%) | Mean (SD): 36.4 (38.84) weeks | Mean (SD): 3.6 (3.61) | |
| Female: 18 (26.1%) | Median: 15.3 (2.0–167.0) weeks | Median: 2.30 (1.0–20.0) | |||||
| GraftJacket® | 58.5 (9.83) | NR | NR | Male: 20 (71.4%) | Mean (SD): 36.8 (53.60) weeks | Mean (SD): 3.3 (2.69) | |
| Female: 8 (28.6%) | Median: 13.5 (2.0–226.0) weeks | Median: 2.00 (1.0–11.0) | |||||
| Djavid et al., 2020 | SWC | 57.3 (13.2) | NR | NR | Male: 22 (71%) | NR | Mean: 3.5 (4.2) |
| Female: 9 (29%) | Median (range): 2.0 (0.5–22) | ||||||
| Tebaderm® Collagen Matrix | 54.2 (13.2) | NR | NR | Male: 18 (60%) | NR | Mean: 3.09 (2.5) | |
| Female: 12 (40%) | Median (range): 2.5 (0.5–12) | ||||||
| Driver et al., 2015 | Omnigraft® Dermal Regeneration Matrix | 55.8 ± 10.6 | White: 118 (76.6%) | Male: 118 (76.6%) | Omnigraft: Days | Omnigraft: cm2 | |
| African American: 28 (18.2%) | NR | Mean (SD): 308 (491) | Mean (SD): 3.53 (2.5) | ||||
| Hispanic: 46 (29.9%) | Median (IQR): 126 (288) | ||||||
| SWC | 57.3 ± 9.7 | White: 111 (72.5%) | Male: 114 (74.5%) | SWC: Days | SWC: cm2 | ||
| African American: 34 (22.2%) | NR | Mean (SD): 303 (481) | Mean (SD): 3.65 (2.7) | ||||
| Hispanic: 83 (27.0%) | Median (IQR): 152 (224) | ||||||
| Fitzgerald et al., 2019 | Dermagraft® | 60.2 | NR | NR | Male: 78/106 (74.3%) | Mean (SD): 8.8 (11.7) months | Mean (SD): 4 (3.6) |
| Primatrix® | 65.2 | NR | NR | Male: 66/100 (66.0%) | Mean (SD): 12.8 (48.3) weeks | Mean (SD): 5.8 (4.6) | |
| Frykberg et al., 2016 | MatriStem® | 57.0 (9.8) | Caucasian: 22 (81.5%) | Hispanic or Latino: 10 (37%) | Male: 21 (77.8%) | NR | 4.3 (5.7) |
| Non-Caucasian: 5 (18.5%) | Non-Hispanic or Latino: 17 (63%) | Female: 6 (22.2%) | |||||
| Dermagraft® | 58.5 (11.4) | Caucasian: 25 (86.2%) | Hispanic or Latino: 25 (82.2) | Male: 22 (75.9) | NR | 3.2 (4.5) | |
| Non-Caucasian: 4 (13.8%) | Non-Hispanic or Latino: 4 (13.8) | Female: 7 (24.1) | |||||
| Gilligan et al., 2015 | OASIS® Extracellular Matrix | 62.2 (12.2) | NR | NR | Male (%): 76.9% | Minimum of 4 weeks | 1.9 (1.8) |
| Dermagraft® | 63.4 (9.8) | NR | NR | Male (%): 61.5% | 1.9 (1.4) | ||
| Glat et al., 2019 | AmnioBand® Membrane | 62 (13.2) | Caucasian: 28 (93%) | NR | Male: 16 (53%) | Mean (SD): 12.3 (14.25) | Mean (SD): 2.4 (1.88) |
| African American: 2 (7%) | Female: 14 (47%) | Median: 7.5 weeks | Median: 1.4 | ||||
| Apligraf® | 62 (15.28) | Caucasian: 27 (90%) | NR | Male: 23 (77%) | Mean (SD): 14.5 (14.7) | Mean (SD): 3.1 (2.29) | |
| African American: 3 (10%) | Female: 7 (23%) | Median: 8 weeks | Median: 2.1 | ||||
| Kirsner et al., 2015 | Apligraf® | Mean (SD): 60.1 (12.5) | NR | NR | Male: 104 (68%) | Mean (SD): 4.4 (2.6) | Mean (SD): 6.0 (5.5) |
| Median: 60 | Female: 49 (32%) | Median: 3.8 months | Median: 3.9 | ||||
| EpiFix® | Mean (SD): 61.1 (12.2) | NR | NR | Male: 48 (76.2%) | Mean (SD): 4.6 (3.0) | Mean (SD): 5.2 (5.0) | |
| Median: 62 | Female: 15 (23.8%) | Median: 3.5 months | Median: 3.0 | ||||
| Kraus et al., 2017 | Apligraf® | 61 | NR | NR | Male: 13 | Mean (SD): 4.2 (2.5) | Mean (SD): 4.8 (5.1) |
| Female: 46 | Median: 3.7 months | Median: 2.7 | |||||
| EpiFix® | NR | NR | Male: 15 | Mean (SD): 4.6 (3.0) | Mean (SD): 5.2 (5.0) | ||
| Female: 48 | Median: 3.5 months | Median: 3.0 | |||||
| Sabolinski et al., 2019 | Dermagraft® | 62 (12.4) | NR | NR | Male: 472 (32.7%) | Mean (SD): 8.97 (14.96) | Mean (SD): 7.23 (7.74) |
| Female: 878 (68.3%) | Median: 4.63 months | Median: 4.0 | |||||
| Grafix Prime® | 62 (12) | NR | NR | Male: 45 (25.4%) | Mean (SD): 11.54 (19.30) | Mean (SD): 6.43 (6.73) | |
| Female: 131 (75.6%) | Median: 6.13 months | Median: 3.6 | |||||
| Tchangque Fossuo et al., 2019 | Dermagraft® | 62.83 (9.03) | Caucasian: 17 (100%) | Hispanic: 2 (11.8%) | Male: 17 (100%) | Mean (SD): 37.61 (96.07) weeks | Week1: 1.60 (1.79) |
| Non-Caucasian: 0 (0%) | Non-Hispanic: 15 (88.2%) | Female: 0 (0%) | Week 12: 0.33 (0.57) | ||||
| Week 28: 0.29 (0.69) | |||||||
| OASIS® Extracellular Matrix | 61.88 (8.64) | Caucasian: 16 (84.2%) | Hispanic: 2 (10.5%) | Male: 18 (94.7%) | Mean (SD): 10.91 (7.56) weeks | Week 1: 3.08 (3.79) | |
| Non-Caucasian: 3 (15.8%) | Non-Hispanic: 17 (89.5%) | Female: 1 (5.3%) | Week 12:0.31 (0.76) | ||||
| Week 28:0.08 (0.36) | |||||||
| SWC | 63.31 (9.09) | Caucasian: 18 (94.7%) | Hispanic: 0 (0%) | Male: 17 (89.5%) | Mean (SD): 21.68 (36.06) weeks | Week 1:1.29 (0.90) | |
| Non-Caucasian: 1 (5.3%) | Non-Hispanic: 19 (100%) | Female: 2 (10.5%) | Week 12:0.20 (0.38) | ||||
| Week 28:0.05 (0.10) | |||||||
| You et al., 2014 | Hyalograft 3D | 61.2 (11.4) | NR | NR | Male: 21 (68%) | Mean (SD): 6.1 (16.4) | Mean (SD): 3.5 (3.7) |
| Female:10 (32%) | Median (Min–Max): 4.4 (1.5–84.0) months | Median (Min–Max): 1.7 (1.0–15.6) | |||||
| SWC | 63.8 (10.7) | NR | NR | Male: 22 (69) | Mean (SD): 6.2 (19.7) | Mean (SD): 2.9(2.7) | |
| Female: 10 (31) | Median (Min–Max): 3.9 (1.5–108.0) months | Median (Min–Max): 2.1 (1.0–14.3) | |||||
| Zelen et al., 2014 | Apligraf® | 65.2 (11.7) | Caucasian: 18 (90%) | NR | Male: 9 (45%) | Mean: 18.5 (13.8) | Mean: 2.6 (1.8) |
| African American: 2 (10%) | Female: 11 (55%) | Median (min, max): 13 (6, 54) weeks | Median (min–max): 2.1 (1.0–6.8) | ||||
| EpiFix® | 63.2 (13.0) | Caucasian: 19 (95%) | NR | Male: 10 (50%) | Mean: 15.6 (12.7) | Mean: 2.7 (2.4) | |
| African American: 1 (5%) | Female: 10 (50%) | Median (min, max): 11 (5, 54) weeks | Median (min, max): 2.0 (1.0, 9.0) | ||||
| SWC | 62.2 (12.8) | Caucasian: 17 (85%) | NR | Male: 9 (45%) | Mean: 16.2 (13.5) | Mean: 3.3 (2.7) | |
| African American: 3 (15%) | Female: 10 (45%) | Median (min, max): 9 (6, 52) weeks | Median (min, max): 2.0 (1.0, 9.0) | ||||
| Zelen et al., 2015 | Apligraf® | 63.8 (11.86) | Caucasian: 30 (29.7%) | NR | Male: 14 (13.9%) | Mean: 19.0 (14.78) | Mean: 2.7 (2.75) |
| African American: 3 (30%) | Female: 19 | Median: 16 (4,52) | Median: 1.7 (1.0–14.7) | ||||
| EpiFix® | 63.3 (12.25) | Caucasian: 31 (30.7%) | NR | Male: 19 (18.3%) | Mean: 17.3 (15.3) | Mean: 2.6 (2.97) | |
| African American: 2 (2.0%) | Female: 13 | Median (min, max): 12 (3, 52) | Median: 1.7 (1.0, 16.9) | ||||
| SWC | 60.6 (11.55) | Caucasian: 31 (30.7%) | NR | Male: 22 (21.8%) | Mean: 14.1 (12.9) | Mean: 3.1 (3.17) | |
| African American: 3 (3%) | Female: 13 | Median (min, max): 8 (2, 50) | Median: 1.8 (1.0, 15.5) | ||||
| Zelen et al., 2016 | AlloPatch® Pliable | 61.5 (10.85) | Caucasian: 20 (100%) | NR | Male: 16 (80%) | NR | Mean (SD):4.7 (5.24) |
| African American: 0 (0%) | Female: 4 (20%) | ||||||
| SWC | 57.1 (10.65) | Caucasian: 19 (95%) | NR | Male: 12 (60%) | NR | Mean (SD):2.7 (2.26) | |
| African American: 1 (5%) | Female: 8 (40%) | ||||||
| Zelen et al., 2018 | 1st AlloPatch® Pliable | 62(11) | White: 20 (100%) | NR | Male: 16 (80%) | Mean Healing Time: 6–12 weeks | 4.7 (5.3) |
| African Americans: 0 (0%) | Female: 4 (20%) | ||||||
| 2nd AlloPatch® Pliable | 55 (13) | White: 16 (80%) | NR | Male: 12 (60%) | 1.7 (0.61)) | ||
| African Americans: 4 (20%) | Female: 8 (40%) | ||||||
| 1st SWC | 57 (11) | White: 19 (95%) | NR | Male: 12 (60%) | 2.7 (2.3) | ||
| African Americans: 1 (5%) | Female: 8 (40%) | ||||||
| 2nd SWC | 67 (14) | White: 19 (95) | NR | Male: 12 (60%) | 2.6 (2.7) | ||
| African Americans: 1 (5%) | Female: 8 (40%) | ||||||
| Frykberg et al., 2015 | Dermagraft® SWC | NR | NR | NR | NR | Greater than 6 week duration | NR |
| Sanders et al., 2014 | Dermagraft® | 56.58 (14.96) | White Non-hispanic: 66.67% Black: 33.33% | NR | Male: 6 (50%) Female: 6 (50%) | Mean: 11.71 (8.02) weeks | 4.78 (3.95) |
| TheraSkin® | 60 (15.74) | White Non-hispanic: 54.55% Black: 45.45% | NR | Male: 5 (45.45%) Female: 6 (54.55%) | Mean: 43.58 (78.08) weeks | 5.45 (5.58) | |
| Rosa et al., 2019 | RAPHA® System–Latex biomembrane with HCP RAPHA® System–Latex without HCP | NR | NR | NR | NR | Wound Advent Period: 2 months–10 years | Wound size: 1.5–299.14 cm2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Primous, N.R.; Elvin, P.T.; Carter, K.V.; Andrade, H.L.; La Fontaine, J.; Shibuya, N.; Biguetti, C.C. Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review. J. Clin. Med. 2024, 13, 1221. https://doi.org/10.3390/jcm13051221
Primous NR, Elvin PT, Carter KV, Andrade HL, La Fontaine J, Shibuya N, Biguetti CC. Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review. Journal of Clinical Medicine. 2024; 13(5):1221. https://doi.org/10.3390/jcm13051221
Chicago/Turabian StylePrimous, Nathaniel R., Peter T. Elvin, Kathleen V. Carter, Hagner L. Andrade, Javier La Fontaine, Naohiro Shibuya, and Claudia C. Biguetti. 2024. "Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review" Journal of Clinical Medicine 13, no. 5: 1221. https://doi.org/10.3390/jcm13051221
APA StylePrimous, N. R., Elvin, P. T., Carter, K. V., Andrade, H. L., La Fontaine, J., Shibuya, N., & Biguetti, C. C. (2024). Bioengineered Skin for Diabetic Foot Ulcers: A Scoping Review. Journal of Clinical Medicine, 13(5), 1221. https://doi.org/10.3390/jcm13051221