

Association between Preoperative Glucose Dysregulation and Delirium after Non-Cardiac Surgery
 , , and
, , and 
Abstract
1. Introduction
2. Methods
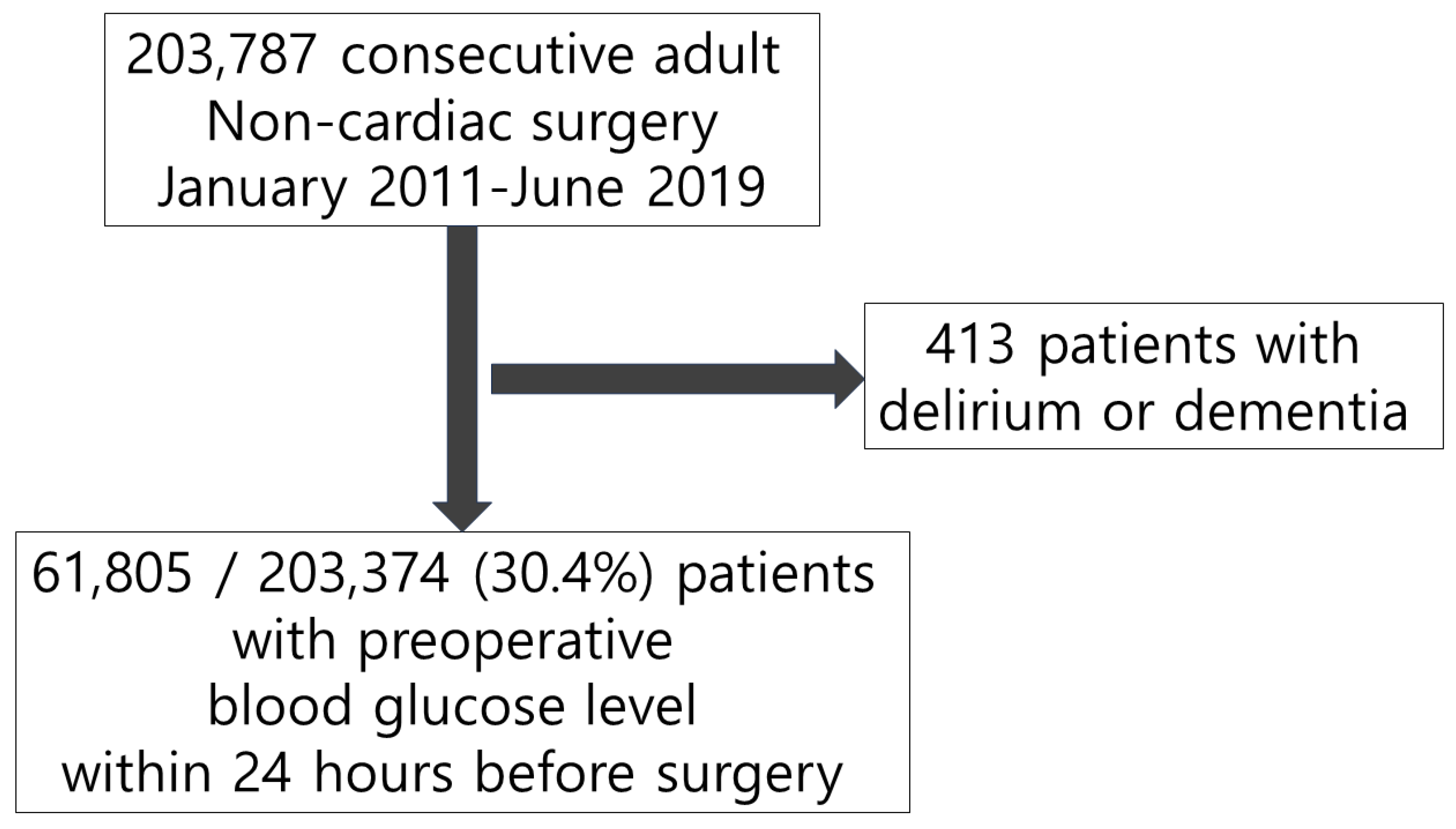
2.1. Study Population and Data Sources
2.2. Exposure
2.3. Outcome
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swarbrick, C.J.; Partridge, J.S.L. Evidence-based strategies to reduce the incidence of postoperative delirium: A narrative review. Anaesthesia 2022, 77 (Suppl. S1), 92–101. [Google Scholar] [CrossRef]
- Inouye, S.K.; Westendorp, R.G.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef]
- McCusker, J.; Cole, M.G.; Dendukuri, N.; Belzile, E. Does delirium increase hospital stay? J. Am. Geriatr. Soc. 2003, 51, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.; Schurch, R.; Boettger, S.; Garcia Nunez, D.; Schwarz, U.; Bettex, D.; Jenewein, J.; Bogdanovic, J.; Staehli, M.L.; Spirig, R.; et al. A hospital-wide evaluation of delirium prevalence and outcomes in acute care patients—A cohort study. BMC Health Serv. Res. 2018, 18, 550. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Yue, J.R.; Xie, D.M.; Carter, P.; Li, Q.L.; Gartaganis, S.L.; Chen, J.; Inouye, S.K. Effect of the Tailored, Family-Involved Hospital Elder Life Program on Postoperative Delirium and Function in Older Adults: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Janssen, T.L.; Alberts, A.R.; Hooft, L.; Mattace-Raso, F.; Mosk, C.A.; van der Laan, L. Prevention of postoperative delirium in elderly patients planned for elective surgery: Systematic review and meta-analysis. Clin. Interv. Aging 2019, 14, 1095–1117. [Google Scholar] [CrossRef] [PubMed]
- Rom, S.; Zuluaga-Ramirez, V.; Gajghate, S.; Seliga, A.; Winfield, M.; Heldt, N.A.; Kolpakov, M.A.; Bashkirova, Y.V.; Sabri, A.K.; Persidsky, Y. Hyperglycemia-Driven Neuroinflammation Compromises BBB Leading to Memory Loss in Both Diabetes Mellitus (DM) Type 1 and Type 2 Mouse Models. Mol. Neurobiol. 2019, 56, 1883–1896. [Google Scholar] [CrossRef] [PubMed]
- van Keulen, K.; Knol, W.; Belitser, S.V.; van der Linden, P.D.; Heerdink, E.R.; Egberts, T.C.G.; Slooter, A.J.C. Diabetes and Glucose Dysregulation and Transition to Delirium in ICU Patients. Crit. Care Med. 2018, 46, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Frisch, A.; Chandra, P.; Smiley, D.; Peng, L.; Rizzo, M.; Gatcliffe, C.; Hudson, M.; Mendoza, J.; Johnson, R.; Lin, E.; et al. Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care 2010, 33, 1783–1788. [Google Scholar] [CrossRef] [PubMed]
- Moghissi, E.S.; Korytkowski, M.T.; DiNardo, M.; Einhorn, D.; Hellman, R.; Hirsch, I.B.; Inzucchi, S.E.; Ismail-Beigi, F.; Kirkman, M.S.; Umpierrez, G.E. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care 2009, 32, 1119–1131. [Google Scholar] [CrossRef]
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.; Botker, H.E.; Hert, S.D.; Ford, I.; Gonzalez-Juanatey, J.R.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: Cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur. Heart J. 2014, 35, 2383–2431. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Krzych, L.J.; Wybraniec, M.T.; Krupka-Matuszczyk, I.; Skrzypek, M.; Bochenek, A.A. Delirium Screening in Cardiac Surgery (DESCARD): A useful tool for nonpsychiatrists. Can. J. Cardiol. 2014, 30, 932–939. [Google Scholar] [CrossRef]
- Krzych, L.J.; Wybraniec, M.T.; Krupka-Matuszczyk, I.; Skrzypek, M.; Bolkowska, A.; Wilczynski, M.; Bochenek, A.A. Complex assessment of the incidence and risk factors of delirium in a large cohort of cardiac surgery patients: A single-center 6-year experience. BioMed Res. Int. 2013, 2013, 835850. [Google Scholar] [CrossRef]
- Adamis, D.; Treloar, A.; Martin, F.C.; Gregson, N.; Hamilton, G.; Macdonald, A.J. APOE and cytokines as biological markers for recovery of prevalent delirium in elderly medical inpatients. Int. J. Geriatr. Psychiatry 2007, 22, 688–694. [Google Scholar] [CrossRef]
- He, R.; Wang, F.; Shen, H.; Zeng, Y.; Zhang, L. Association between increased neutrophil-to-lymphocyte ratio and postoperative delirium in elderly patients with total hip arthroplasty for hip fracture. BMC Psychiatry 2020, 20, 496. [Google Scholar] [CrossRef]
- Song, Q.; Dai, M.; Zhao, Y.; Lin, T.; Huang, L.; Yue, J. Association between stress hyperglycemia ratio and delirium in older hospitalized patients: A cohort study. BMC Geriatr. 2022, 22, 277. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, A.; Hrnjakovic, L. Hypoglycemia—A delirious state with vestibular hallucinations. Med. Pregl. 1991, 44, 231–232. [Google Scholar] [PubMed]
- Fishbain, D.A.; Rotundo, D. Frequency of hypoglycemic delirium in a psychiatric emergency service. Psychosomatics 1988, 29, 346–348. [Google Scholar] [CrossRef] [PubMed]
- Shehadeh, N.; Kassem, J.; Tchaban, I.; Ravid, S.; Shahar, E.; Naveh, T.; Etzioni, A. High incidence of hypoglycemic episodes with neurologic manifestations in children with insulin dependent diabetes mellitus. J. Pediatr. Endocrinol. Metab. 1998, 11 (Suppl. S1), 183–187. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, A. Hypoglycemia and states of confusion. Med. Pregl. 1990, 43, 221–223. [Google Scholar] [PubMed]
- Sejling, A.S.; Kjaer, T.W.; Pedersen-Bjergaard, U.; Diemar, S.S.; Frandsen, C.S.; Hilsted, L.; Faber, J.; Holst, J.J.; Tarnow, L.; Nielsen, M.N.; et al. Hypoglycemia-associated changes in the electroencephalogram in patients with type 1 diabetes and normal hypoglycemia awareness or unawareness. Diabetes 2015, 64, 1760–1769. [Google Scholar] [CrossRef]
- Zhao, H.; Ying, H.L.; Zhang, C.; Zhang, S. Relative Hypoglycemia is Associated with Delirium in Critically Ill Patients with Diabetes: A Cohort Study. Diabetes Metab. Syndr. Obes. 2022, 15, 3339–3346. [Google Scholar] [CrossRef]
- Noordzij, P.G.; Boersma, E.; Schreiner, F.; Kertai, M.D.; Feringa, H.H.; Dunkelgrun, M.; Bax, J.J.; Klein, J.; Poldermans, D. Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery. Eur. J. Endocrinol. 2007, 156, 137–142. [Google Scholar] [CrossRef]
- Abdelmalak, B.B.; Knittel, J.; Abdelmalak, J.B.; Dalton, J.E.; Christiansen, E.; Foss, J.; Argalious, M.; Zimmerman, R.; Van den Berghe, G. Preoperative blood glucose concentrations and postoperative outcomes after elective non-cardiac surgery: An observational study. Br. J. Anaesth. 2014, 112, 79–88. [Google Scholar] [CrossRef]
- Farrokhi, F.; Smiley, D.; Umpierrez, G.E. Glycemic control in non-diabetic critically ill patients. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Quagliaro, L.; Piconi, L.; Assaloni, R.; Martinelli, L.; Motz, E.; Ceriello, A. Intermittent high glucose enhances apoptosis related to oxidative stress in human umbilical vein endothelial cells: The role of protein kinase C and NAD(P)H-oxidase activation. Diabetes 2003, 52, 2795–2804. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S. Glycemic variability and mortality in critically ill patients: The impact of diabetes. J. Diabetes Sci. Technol. 2009, 3, 1292–1301. [Google Scholar] [CrossRef]
- Umpierrez, G.; Cardona, S.; Pasquel, F.; Jacobs, S.; Peng, L.; Unigwe, M.; Newton, C.A.; Smiley-Byrd, D.; Vellanki, P.; Halkos, M.; et al. Randomized Controlled Trial of Intensive Versus Conservative Glucose Control in Patients Undergoing Coronary Artery Bypass Graft Surgery: GLUCO-CABG Trial. Diabetes Care 2015, 38, 1665–1672. [Google Scholar] [CrossRef]
- Macisaac, R.J.; Jerums, G. Intensive glucose control and cardiovascular outcomes in type 2 diabetes. Heart Lung Circ. 2011, 20, 647–654. [Google Scholar] [CrossRef]
- Wiener, R.S.; Wiener, D.C.; Larson, R.J. Benefits and risks of tight glucose control in critically ill adults: A meta-analysis. JAMA 2008, 300, 933–944. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| No Delirium (n = 59,869) | Delirium (n = 1936) | p Value | |
|---|---|---|---|
| Hyperglycemia | 5456 (9.1) | 395 (20.4) | <0.001 |
| Hypoglycemia | 1367 (2.3) | 85 (4.4) | <0.001 |
| Glycemic dysregulation | 129 (0.2) | 16 (0.8) | <0.001 |
| Male | 31,508 (52.6) | 1297 (67.0) | <0.001 |
| Age | 57.5 (±14.6) | 64.7 (±14.6) | <0.001 |
| Body mass index | 24.4 (±3.7) | 23.6 (±3.8) | <0.001 |
| Psychiatric disorder, any | 2628 (4.4) | 243 (12.6) | <0.001 |
| Mood disorder | 1133 (1.9) | 114 (5.9) | <0.001 |
| Schizophrenia | 63 (0.1) | 21 (1.1) | <0.001 |
| Alcoholic use disorder | 65 (0.1) | 10 (0.5) | <0.001 |
| Other substance abuse | 15 (0.0) | 3 (0.2) | 0.01 |
| Sleep disorder | 893 (1.5) | 56 (2.9) | <0.001 |
| Personality disorder | 20 (0.0) | 2 (0.1) | 0.32 |
| Current alcohol | 11,119 (18.6) | 288 (14.9) | <0.001 |
| Current smoking | 5160 (8.6) | 229 (11.8) | <0.001 |
| Previous disease | |||
| Hypertension | 23,009 (38.4) | 912 (47.1) | <0.001 |
| Diabetes | 20,908 (34.9) | 677 (35.0) | 0.99 |
| Chronic kidney disease | 2208 (3.7) | 155 (8.0) | <0.001 |
| Dialysis | 702 (1.2) | 93 (4.8) | <0.001 |
| Stroke | 2262 (3.8) | 172 (8.9) | <0.001 |
| Coronary artery disease | 2144 (3.6) | 124 (6.4) | <0.001 |
| Heart failure | 404 (0.7) | 35 (1.8) | <0.001 |
| Arrhythmia | 1470 (2.5) | 118 (6.1) | <0.001 |
| Peripheral artery disease | 367 (0.6) | 35 (1.8) | <0.001 |
| Aortic disease | 357 (0.6) | 43 (2.2) | <0.001 |
| Valvular heart disease | 134 (0.2) | 11 (0.6) | <0.001 |
| Chronic obstructive pulmonary disease | 1459 (2.4) | 98 (5.1) | <0.001 |
| Preoperative blood laboratory tests | |||
| Hemoglobin, g/dL | 13.1 (±1.9) | 11.9 (±2.3) | <0.001 |
| Creatinine, mg/dL | 1.0 (±1.3) | 1.4 (±2.0) | <0.001 |
| Preoperative electrolytes | |||
| Hyponatremia | 3323 (5.6) | 375 (19.4) | <0.001 |
| Hypernatremia | 594 (1.0) | 25 (1.3) | 0.24 |
| Hypokalemia | 1308 (2.2) | 127 (6.6) | <0.001 |
| Hyperkalemia | 787 (1.3) | 61 (3.2) | <0.001 |
| Hypophosphatemia | 2010 (3.4) | 168 (8.7) | <0.001 |
| Hyperphosphatemia | 2426 (4.1) | 134 (6.9) | <0.001 |
| Hypochloremia | 2056 (3.4) | 201 (10.4) | <0.001 |
| Hyperchloremia | 9906 (16.5) | 493 (25.5) | <0.001 |
| Operative variables | |||
| General anesthesia | 53,625 (89.6) | 1795 (92.7) | <0.001 |
| Emergency operation | 8148 (13.6) | 584 (30.2) | <0.001 |
| Operation duration, min | 165.6 (±121.0) | 250.4 (±180.4) | <0.001 |
| Intraoperative transfusion | 4354 (7.3) | 585 (30.2) | <0.001 |
| Intraoperative inotropic infusion | 8153 (13.6) | 870 (44.9) | <0.001 |
| Surgical risk | |||
| Mild | 12,713 (21.2) | 218 (11.3) | <0.001 |
| Intermediate | 39,331 (65.7) | 1161 (60.0) | <0.001 |
| High | 7825 (13.1) | 557 (28.8) | <0.001 |
| Surgery types | <0.001 | ||
| Neuroendocrine | 1320 (2.2) | 5 (0.3) | |
| Lung | 3179 (5.3) | 113 (5.8) | |
| Head and neck | 12,949 (21.6) | 417 (21.5) | |
| Breast | 1395 (2.3) | 7 (0.4) | |
| Stomach | 2881 (4.8) | 52 (2.7) | |
| Hepatobiliary | 8803 (14.7) | 427 (22.1) | |
| Colorectal | 4717 (7.9) | 206 (10.6) | |
| Urology | 6110 (10.2) | 116 (6.0) | |
| Gynecology | 3873 (6.5) | 19 (1.0) | |
| Bone, skin, etc. | 14,642 (24.5) | 574 (29.6) | |
| Outcomes | |||
| One-year mortality | 3039 (5.1) | 406 (21.0) | <0.001 |
| Three-year mortality | 5891 (9.8) | 569 (29.4) | <0.001 |
| Outcome | Unexposed Group | Exposed Group | ||||
|---|---|---|---|---|---|---|
| No. with Outcome/Total No. (%) | Incidence Rate per 100 Person-Months (95% CI) | No. with Outcome/Total No. (%) | Incidence Rate per 100 Person-Months (95% CI) | Crude HR (95% CI) | IPTW-Adjusted HR (95% CI) | |
| Primary analysis | ||||||
| Hyperglycemia | 1541/55,954 (2.8) | 2.82 (2.68–2.96) | 395/5851 (6.8) | 7.13 (6.45–7.87) | 2.50 (2.24–2.80) | 1.35 (1.18–1.56) |
| Hypoglycemia | 1851/60,353 (3.1) | 3.15 (3.01–3.29) | 85/1452 (5.9) | 6.14 (4.91–7.59) | 2.50 (2.24–2.80) | 1.36 (1.06–1.75) |
| Both | 1920/61,660 (3.1) | 3.20 (3.05–3.34) | 16/145 (11.0) | 12.12 (6.93–19.68) | 3.72 (2.27–6.08) | 3.14 (1.27–7.77) |
| Subgroup analysis | ||||||
| With diabetes | ||||||
| Hyperglycemia | 482/18,452 (2.6) | 2.67 (2.44–2.92) | 195/3133 (6.2) | 6.56 (5.67–7.55) | 2.43 (2.06–2.87) | 1.33 (1.10–1.62) |
| Hypoglycemia | 637/20,759 (3.1) | 3.15 (2.91–3.40) | 40/826 (4.8) | 5.05 (3.61–6.88) | 1.59 (1.16–2.19) | 1.25 (0.86–1.836) |
| Both | 667/21,469 (3.1) | 3.19 (2.95–3.44) | 10/116 (8.6) | 9.35 (4.48–17.2) | 1.59 (1.16–2.19) | 1.99 (0.52–7.65) |
| Without diabetes | ||||||
| Hyperglycemia | 1059/37,502 (2.8) | 2.89 (2.72–3.07) | 200/2718 (7.4) | 7.80 (6.76–8.96) | 2.67 (2.30–3.10) | 1.32 (1.06–1.65) |
| Hypoglycemia | 1214/39,594 (3.1) | 3.14 (2.97–3.33) | 45/626 (7.2) | 7.61 (5.56–10.19) | 2.39 (1.78–3.22) | 1.77 (1.21–2.59) |
| Both | 1253/40,191 (3.1) | 3.20 (3.03–3.38) | 6/29 (20.7) | 25.00 (9.17–54.41) | 7.37 (3.30–16.43) | 1.22 (0.18–3.85) |
| Outcome | Unexposed Group | Exposed Group | ||||
|---|---|---|---|---|---|---|
| No. with Outcome /Total No. (%) | Incidence Rate per 100 Person-Months (95% CI) | No. with Outcome /Total No. (%) | Incidence Rate per 100 Person-Months (95% CI) | Crude HR (95% CI) | IPTW-Adjusted HR (95% CI) | |
| One-year follow-up | ||||||
| Primary analysis | ||||||
| Hyperglycemia | 2747/55,954 (4.9) | 0.41 (0.40–0.43) | 698/5851 (11.9) | 1.07 (0.99–1.15) | 2.63 (2.42–2.85) | 1.32 (1.18–1.47) |
| Hypoglycemia | 3332/60,353 (5.5) | 0.47 (0.45–0.48) | 113/1452 (7.8) | 0.68 (0.56–0.81) | 1.43 (1.19–1.73) | 1.03 (0.73–1.28) |
| Both | 3426/61,660 (5.6) | 0.47 (0.46–0.49) | 19/145 (13.1) | 1.20 (0.72–1.88) | 2.48 (1.58–3.90) | 1.22 (0.52–2.84) |
| Subgroup analysis | ||||||
| With diabetes | ||||||
| Hyperglycemia | 805/18,452 (4.4) | 0.37 (0.34–0.39) | 316/3133 (10.1) | 0.89 (0.79–0.99) | 2.41 (2.12–2.75) | 1.37 (1.17–1.59) |
| Hypoglycemia | 1067/20,759 (5.1) | 0.43 (0.41–0.46) | 54/826 (6.5) | 0.56 (0.42–0.73) | 1.30 (0.99–1.70) | 1.15 (0.84–1.56) |
| Both | 1110/21,469 (5.2) | 0.44 (0.41–0.46) | 11/116 (9.5) | 0.83 (0.42–1.49) | 1.85 (1.02–3.35) | 1.64 (0.60–4.51) |
| Without diabetes | ||||||
| Hyperglycemia | 1942/37,502 (5.2) | 0.44 (0.42–0.46) | 382/2718 (14.1) | 1.30 (1.17–1.43) | 3.09 (2.77–3.45) | 1.32 (1.09–1.60) |
| Hypoglycemia | 2265/39,594 (5.7) | 0.49 (0.47–0.51) | 59/626 (9.4) | 0.84 (0.64–1.08) | 1.69 (1.31–2.19) | 0.99 (0.69–1.44) |
| Both | 2316/40,191 (5.8) | 0.49 (0.47–0.51) | 8/29 (27.6) | 3.10 (1.34–6.11) | 6.45 (3.22–12.91) | 0.77 (0.57–1.05) |
| Three-year follow-up | ||||||
| Primary analysis | ||||||
| Hyperglycemia | 5396/55,954 (9.6) | 0.28 (0.27–0.29) | 1064/5851 (18.2) | 0.58 (0.54–0.61) | 2.07 (1.94–2.21) | 1.32 (1.21–1.44) |
| Hypoglycemia | 6290/60,353 (10.4) | 0.31 (0.30–0.31) | 170/1452 (11.7) | 0.35 (0.30–0.41) | 1.14 (0.98–1.32) | 0.88 (0.73–1.05) |
| Both | 6426/61,660 (10.4) | 0.31 (0.30–0.31) | 34/145 (23.4) | 0.77 (0.54–1.08) | 2.34 (1.67–3.28) | 3.89 (1.02–14.73) |
| Subgroup analysis | ||||||
| With diabetes | ||||||
| Hyperglycemia | 1671/18,452 (9.1) | 0.26 (0.25–0.28) | 554/3133 (17.7) | 0.55 (0.51–0.60) | 2.07 (1.88–2.27) | 1.40 (1.25–1.56) |
| Hypoglycemia | 2132/20,759 (10.3) | 0.30 (0.29–0.31) | 93/826 (11.3) | 0.33 (0.27–0.41) | 1.12 (0.91–1.37) | 0.99 (0.78–1.27) |
| Both | 2199/21,469 (10.2) | 0.30 (0.29–0.31) | 26/116 (22.4) | 0.72 (0.47–1.05) | 2.23 (1.51–3.28) | 1.79 (0.96–3.34) |
| Without diabetes | ||||||
| Hyperglycemia | 3725/37,502 (9.9) | 0.29 (0.28–0.30) | 510/2718 (18.8) | 0.61 (0.55–0.66) | 2.19 (2.00–2.41) | 1.24 (1.07–1.45) |
| Hypoglycemia | 4158/39,594 (10.5) | 0.31 (0.30–0.32) | 77/626 (12.3) | 0.37 (0.30–0.47) | 1.19 (0.95–1.49) | 0.95 (0.49–1.87) |
| Both | 4227/40,191 (10.5) | 0.31 (0.30–0.32) | 8/29 (27.6) | 1.04 (0.45–2.05) | 3.23 (1.61–6.46) | 8.07 (2.10–31.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, A.R.; Lee, D.Y.; Lee, S.; Lee, J.-H.; Yang, K.; Choi, B.; Park, J. Association between Preoperative Glucose Dysregulation and Delirium after Non-Cardiac Surgery. J. Clin. Med. 2024, 13, 932. https://doi.org/10.3390/jcm13040932
Oh AR, Lee DY, Lee S, Lee J-H, Yang K, Choi B, Park J. Association between Preoperative Glucose Dysregulation and Delirium after Non-Cardiac Surgery. Journal of Clinical Medicine. 2024; 13(4):932. https://doi.org/10.3390/jcm13040932
Chicago/Turabian StyleOh, Ah Ran, Dong Yun Lee, Seunghwa Lee, Jong-Hwan Lee, Kwangmo Yang, Byungjin Choi, and Jungchan Park. 2024. "Association between Preoperative Glucose Dysregulation and Delirium after Non-Cardiac Surgery" Journal of Clinical Medicine 13, no. 4: 932. https://doi.org/10.3390/jcm13040932
APA StyleOh, A. R., Lee, D. Y., Lee, S., Lee, J.-H., Yang, K., Choi, B., & Park, J. (2024). Association between Preoperative Glucose Dysregulation and Delirium after Non-Cardiac Surgery. Journal of Clinical Medicine, 13(4), 932. https://doi.org/10.3390/jcm13040932