
Incidence and Course of Joint Inflammation Associated with Inflammatory Bowel Disease in Patients Undergoing Treatment with Vedolizumab/Ustekinumab: The VEDUSTAR Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
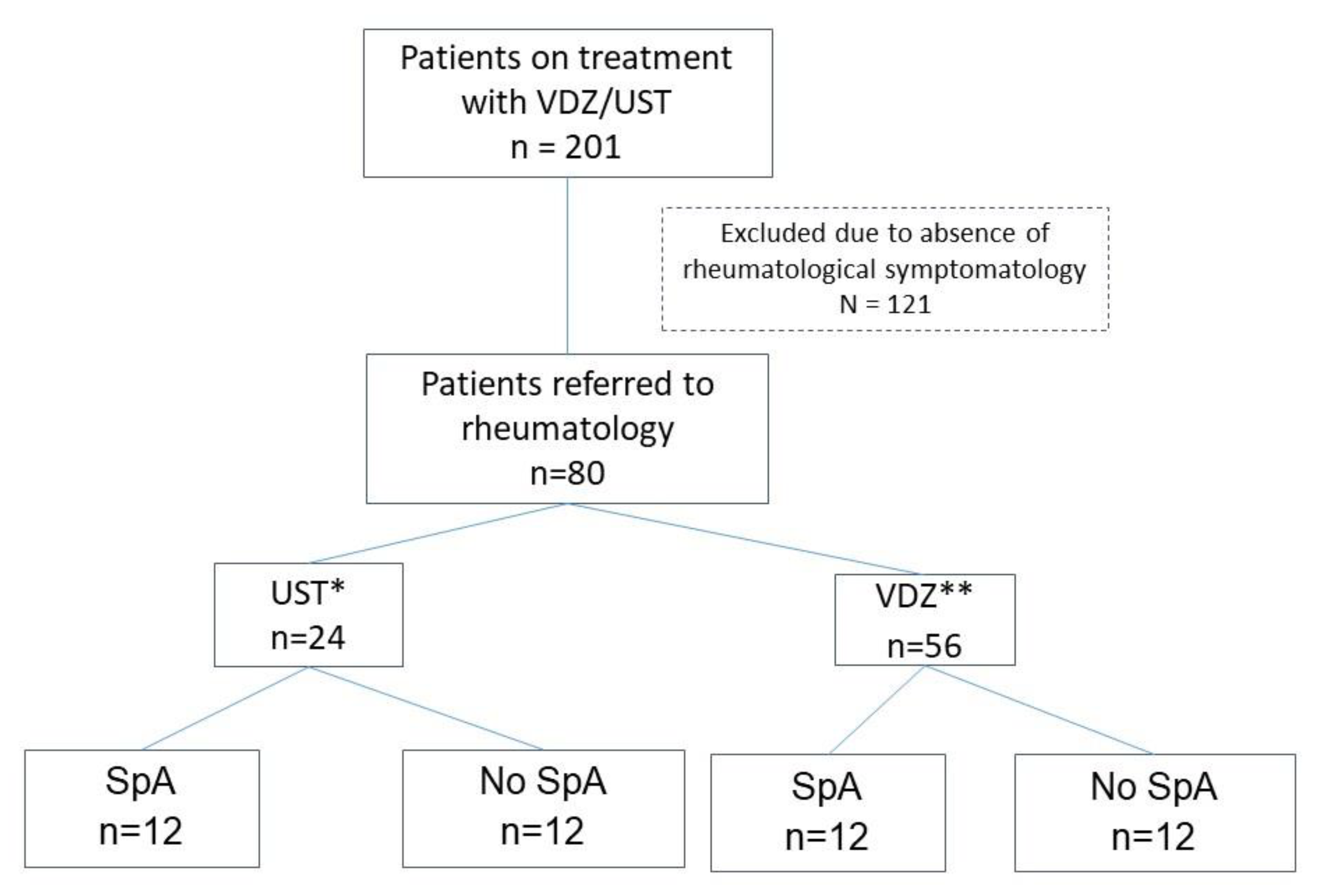
2.2. Patients and Variables
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Gastrointestinal Activity of Referred Patients
3.3. Rheumatologic Activity of Referred Patients
3.4. Discontinuation of UST or VDZ
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orchard, T.R.; Wordsworth, B.P.; Jewell, D.P. Peripheral Arthropathies in Inflammatory Bowel Disease: Their Articular Distribution and Natural History. Gut 1998, 42, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Palm, Ø.; Moum, B.; Ongre, A.; Gran, J.T. Prevalence of Ankylosing Spondylitis and Other Spondyloarthropathies Among Patients with Inflammatory Bowel Disease: A Population Study (The IBSEN Study). J. Rheumatol. 2002, 29, 511–515. [Google Scholar] [PubMed]
- Paredes, J.M.; Barrachina, M.M.; Román, J.; Moreno-Osset, E. Patología articular en la enfermedad inflamatoria intestinal. Gastroenterol. Hepatol. 2005, 28, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, A.B.; Armstrong, A.W.; FitzGerald, O.; Gladman, D.D. Prologue: Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) 2022 Annual Meeting. J. Rheumatol. 2023, 50 (Suppl. S2), 1–3. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Schoepfer, A.; Scharl, M.; Lakatos, P.L.; Navarini, A.; Rogler, G. Extraintestinal Manifestations of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1982–1992. [Google Scholar] [CrossRef]
- Arvikar, S.L.; Fisher, M.C. Inflammatory Bowel Disease Associated Arthropathy. Curr. Rev. Musculoskelet. Med. 2011, 4, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Herfarth, H.; Obermeier, F.; Andus, T.; Rogler, G.; Nikolaus, S.; Kuehbacher, T.; Schreiber, S. Improvement of arthritis and arthralgia after treatment with infliximab (Remicade) in a German prospective, open-label, multicenter trial in refractory Crohn’s disease. Am. J. Gastroenterol. 2002, 97, 2688–2690. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.T.; Rowbotham, D.S.; Danese, S.; Sandborn, W.J.; Miao, Y.; Zhang, H.; Tikhonov, I.; Panaccione, R.; Hisamatsu, T.; Scherl, E.J.; et al. Efficacy and Safety of Maintenance Ustekinumab for Ulcerative Colitis Through 3 Years: UNIFI Long-Term Extension. J. Crohns Colitis 2022, 16, 1222–1234. [Google Scholar] [CrossRef]
- Generini, S. Infliximab in Spondyloarthropathy Associated with Crohn’s Disease: An Open Study on the Efficacy of Inducing and Maintaining Remission of Musculoskeletal and Gut Manifestations. Ann. Rheum. Dis. 2004, 63, 1664–1669. [Google Scholar] [CrossRef]
- Barreiro-de-Acosta, M.; Lorenzo, A.; Domínguez-Muñoz, J.E. Efficacy of Adalimumab for the Treatment of Extraintestinal Manifestations of Crohn’s Disease. Rev. Esp. Enfermedades Dig. 2012, 104, 468–472. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sandborn, W.J.; Colombel, J.-F.; Byrne, S.O.; Khalid, J.M.; Kempf, C.; Geransar, P.; Bhayat, F.; Rubin, D.T. Incidence of Arthritis/Arthralgia in Inflammatory Bowel Disease with Long-Term Vedolizumab Treatment: Post Hoc Analyses of the GEMINI Trials. J. Crohns Colitis 2019, 13, 50–57. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.-F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Orlando, R.; Fries, W.; Scolaro, M.; Magnano, A.; Pluchino, D.; Cappello, M.; Morreale, G.C.; Siringo, S.; Privitera, A.C.; et al. The Real-World Effectiveness of Vedolizumab on Intestinal and Articular Outcomes in Inflammatory Bowel Diseases. Dig. Liver Dis. 2018, 50, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Tadbiri, S.; Peyrin-Biroulet, L.; Serrero, M.; Filippi, J.; Pariente, B.; Roblin, X.; Buisson, A.; Stefanescu, C.; Trang-Poisson, C.; Altwegg, R.; et al. Impact of Vedolizumab Therapy on Extra-intestinal Manifestations in Patients with Inflammatory Bowel Disease: A Multicentre Cohort Study Nested in the OBSERV—IBD Cohort. Aliment. Pharmacol. Ther. 2018, 47, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Ramos, G.P.; Dimopoulos, C.; McDonald, N.M.; Janssens, L.P.; Hung, K.W.; Proctor, D.; Ruggiero, E.; Kane, S.; Bruining, D.H.; Faubion, W.A.; et al. The Impact of Vedolizumab on Pre-Existing Extraintestinal Manifestations of Inflammatory Bowel Disease: A Multicenter Study. Inflamm. Bowel Dis. 2021, 27, 1270–1276. [Google Scholar] [CrossRef]
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.-F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.-J.; Danese, S.; et al. Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O’Brien, C.D.; Zhang, H.; Johanns, J.; Adedokun, O.J.; Li, K.; Peyrin-Biroulet, L.; Van Assche, G.; et al. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1201–1214. [Google Scholar] [CrossRef] [PubMed]
- Appel, H.; Maier, R.; Bleil, J.; Hempfing, A.; Loddenkemper, C.; Schlichting, U.; Syrbe, U.; Sieper, J. In Situ Analysis of Interleukin–23– and Interleukin-12–Positive Cells in the Spine of Patients With Ankylosing Spondylitis. Arthritis Rheum. 2013, 65, 1522–1529. [Google Scholar] [CrossRef]
- Rahman, P.; Inman, R.D.; Gladman, D.D.; Reeve, J.P.; Peddle, L.; Maksymowych, W.P. Association of Interleukin-23 Receptor Variants with Ankylosing Spondylitis. Arthritis Rheum. 2008, 58, 1020–1025. [Google Scholar] [CrossRef]
- Nair, R.P.; Duffin, K.C.; Helms, C.; Ding, J.; Stuart, P.E.; Goldgar, D.; Gudjonsson, J.E.; Li, Y.; Tejasvi, T.; Feng, B.-J.; et al. Genome-Wide Scan Reveals Association of Psoriasis with IL-23 and NF-κB Pathways. Nat. Genet. 2009, 41, 199–204. [Google Scholar] [CrossRef]
- Duerr, R.H.; Taylor, K.D.; Brant, S.R.; Rioux, J.D.; Silverberg, M.S.; Daly, M.J.; Steinhart, A.H.; Abraham, C.; Regueiro, M.; Griffiths, A.; et al. A Genome-Wide Association Study Identifies IL23R as an Inflammatory Bowel Disease Gene. Science 2006, 314, 1461–1463. [Google Scholar] [CrossRef]
- Matsumoto, S.; Mashima, H. Efficacy of Ustekinumab against Infliximab-Induced Psoriasis and Arthritis Associated with Crohn’s Disease. Biol. Targets Ther. 2018, 12, 69–73. [Google Scholar] [CrossRef]
- Matsumoto, S.; Matsumoto, K.; Takaya, H.; Otake, H.; Mashima, H. Efficacy of Ustekinumab Against Spondyloarthritis As-sociated with Crohn’s Disease: A Case Report and Review of the Literature. Open Access Rheumatol. Res. Rev. 2020, 12, 133–137. [Google Scholar] [CrossRef]
- Ghosh, S.; Gensler, L.S.; Yang, Z.; Gasink, C.; Chakravarty, S.D.; Farahi, K.; Ramachandran, P.; Ott, E.; Strober, B.E. Ustekinumab Safety in Psoriasis, Psoriatic Arthritis, and Crohn’s Disease: An Integrated Analysis of Phase II/III Clinical Development Programs. Drug Saf. 2019, 42, 751–768. [Google Scholar] [CrossRef] [PubMed]
- McInnes, I.B.; Chakravarty, S.D.; Apaolaza, I.; Kafka, S.; Hsia, E.C.; You, Y.; Kavanaugh, A. Efficacy of Ustekinumab in Biologic-Naïve Patients with Psoriatic Arthritis by Prior Treatment Exposure and Disease Duration: Data from PSUMMIT 1 and PSUMMIT 2. RMD Open 2019, 5, e000990. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Puig, L.; Gottlieb, A.B.; Ritchlin, C.; Li, S.; Wang, Y.; Mendelsohn, A.M.; Song, M.; Zhu, Y.; Rahman, P.; et al. Maintenance of Clinical Efficacy and Radiographic Benefit Through Two Years of Ustekinumab Therapy in Patients with Active Psoriatic Arthritis: Results From a Randomized, Place-bo-Controlled Phase III Trial. Arthritis Care Res. 2015, 67, 1739–1749. [Google Scholar] [CrossRef] [PubMed]
- Poddubnyy, D.; Hermann, K.-G.A.; Callhoff, J.; Listing, J.; Sieper, J. Ustekinumab for the Treatment of Patients with Active Ankylosing Spondylitis: Results of a 28-Week, Prospective, Open-Label, Proof-of-Concept Study (TOPAS). Ann. Rheum. Dis. 2014, 73, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Romero-Sánchez, C.; Jaimes, D.A.; Londoño, J.; Avila, J.D.; Castellanos, J.E.; Bello, J.M.; Bautista, W.; Valle-Oñate, R. Association between Th-17 Cytokine Profile and Clinical Features in Patients with Spondyloarthritis. Clin. Exp. Rheumatol. Incl Suppl. 2011, 29, 828. [Google Scholar]
- Sandborn, W.J.; Gasink, C.; Gao, L.-L.; Blank, M.A.; Johanns, J.; Guzzo, C.; Sands, B.E.; Hanauer, S.B.; Targan, S.; Rut-geerts, P.; et al. Ustekinumab Induction and Maintenance Therapy in Refractory Crohn’s Disease. N. Engl. J. Med. 2012, 367, 1519–1528. [Google Scholar] [CrossRef]
- Deodhar, A.; Gensler, L.S.; Sieper, J.; Clark, M.; Calderon, C.; Wang, Y.; Zhou, Y.; Leu, J.H.; Campbell, K.; Sweet, K.; et al. Three Multicenter, Randomized, Double-Blind, Placebo-Controlled Studies Evalu-ating the Efficacy and Safety of Ustekinumab in Axial Spondyloarthritis. Arthritis Rheumatol. 2019, 71, 258–270. [Google Scholar] [CrossRef]
- Ferretti, F.; Monico, M.C.; Cannatelli, R.; Carmagnola, S.; Lenti, M.V.; Di Sabatino, A.; Conforti, F.; Pastorelli, L.; Caprioli, F.; Bezzio, C.; et al. The Impact of Biologic Therapies on Extra-Intestinal Manifestations in Inflammatory Bowel Disease: A Multicenter Study. Front. Med. 2022, 9, 933357. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Burisch, J.; Ben-Horin, S.; Braegger, F.; Fernández-Nistal, A.; Lara, N.; Heinrich, H.S.; Vavricka, S.R. Impact of Vedolizumab on Extraintestinal Manifestations in Inflammatory Bowel Disease: Results from a Descriptive, Retrospective, Real-World Study. Inflamm. Bowel Dis. 2023, 29, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Varkas, G.; Thevissen, K.; De Brabanter, G.; Van Praet, L.; Czul-gurdian, F.; Cypers, H.; De Kock, J.; Carron, P.; De Vos, M.; Hindryckx, P.; et al. An Induction or Flare of Arthritis and/or Sacroiliitis by Vedolizumab in Inflammatory Bowel Disease: A Case Series. Ann. Rheum. Dis. 2017, 76, 878–881. [Google Scholar] [CrossRef] [PubMed]
- Wendling, D.; Sondag, M.; Verhoeven, F.; Vuitton, L.; Koch, S.; Prati, C. Arthritis Occurrence or Reactivation under Vedolizumab Treatment for Inflammatory Bowel Disease. A Four Cases Report. Jt. Bone Spine 2018, 85, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Dubash, S.; Marianayagam, T.; Tinazzi, I.; Al-Araimi, T.; Pagnoux, C.; Weizman, A.V.; Richette, P.; Tran Minh, M.-L.; Allez, M.; Singh, A.; et al. Emergence of Severe Spondyloarthropathy-Related Entheseal Pathology Following Successful Vedolizumab Therapy for Inflammatory Bowel Disease. Rheumatology 2019, 58, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Orlando, A.; Orlando, R.; Ciccia, F.; Renna, S.; Rizzo, A.; Cottone, M.; Macaluso, F.S. Clinical Benefit of Vedolizumab on Articular Manifestations in Patients with Active Spondyloarthritis Associated with Inflammatory Bowel Disease. Ann. Rheum. Dis. 2017, 76, e31. [Google Scholar] [CrossRef] [PubMed]
- Pérez Galindo, P.; Gisbert, J.P.; Carrillo-Palau, M.; Bertoletti, F.; González-Vivó, M.; Ferrer, J.A.; Pajares, R.; Merino, O.; Castano, A.; Chaparro, M.; et al. P276 Influence of vedolizumab on extraintestinal manifestations in Inflammatory Bowel Disease: A nationwide multicenter study of the GETECCU Eneida registry. J. Crohns Colitis 2021, 15 (Suppl. S1), S308–S309. [Google Scholar] [CrossRef]
- Hanzel, J.; Ma, C.; Casteele, N.V.; Khanna, R.; Jairath, V.; Feagan, B.G. Vedolizumab and Extraintestinal Manifestations in Inflammatory Bowel Disease. Drugs 2021, 81, 333–347. [Google Scholar] [CrossRef]
- Sange, A.H.; Srinivas, N.; Sarnaik, M.K.; Modi, S.; Pisipati, Y.; Vaidya, S.; Syed Gaggatur, N.; Sange, I. Extra-Intestinal Manifestations of Inflammatory Bowel Disease. Cureus 2021, 13, e17187. [Google Scholar] [CrossRef]
- Helliwell, P.S.; Gladman, D.D.; Chakravarty, S.D.; Kafka, S.; Karyekar, C.S.; You, Y.; Campbell, K.; Sweet, K.; Kavanaugh, A.; Gensler, L.S. Effects of Ustekinumab on Spondylitis-Associated Endpoints in TNFi-Naïve Active Psoriatic Arthritis Patients with Physician-Reported Spondylitis: Pooled Results from Two Phase 3, Randomised, Controlled Trials. RMD Open 2020, 6, e001149. [Google Scholar] [CrossRef]
- Cuthbert, R.J.; Fragkakis, E.M.; Dunsmuir, R.; Li, Z.; Coles, M.; Marzo-Ortega, H.; Giannoudis, P.V.; Jones, E.; El-Sherbiny, Y.M.; McGonagle, D. Brief Report: Group 3 Innate Lymphoid Cells in Human Enthesis. Arthritis Rheumatol. 2017, 69, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Yawalkar, N.; Karlen, S.; Hunger, R.; Brand, C.U.; Braathen, L.R. Expression of Interleukin-12 Is Increased in Psoriatic Skin. J. Investig. Dermatol. 1998, 111, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Guillo, L.; D’Amico, F.; Danese, S.; Peyrin-Biroulet, L. Ustekinumab for Extra-Intestinal Manifestations of Inflammatory Bowel Disease: A Systematic Literature Review. J. Crohns Colitis 2021, 15, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Mocci, G.; Maconi, G. Effect of Ustekinumab on Extraintestinal Diseases in Refractory Crohn’s Disease. J. Crohns Colitis 2021, 15, 1399–1400. [Google Scholar] [CrossRef] [PubMed]
- Dupré, A.; Collins, M.; Nocturne, G.; Carbonnel, F.; Mariette, X.; Seror, R. Articular Manifestations in Patients with Inflammatory Bowel Disease Treated with Vedolizumab. Rheumatology 2020, 59, 3275–3283. [Google Scholar] [CrossRef] [PubMed]
- Mader, O.; Juillerat, P.; Biedermann, L.; Michetti, P.; Hruz, P.; Pittet, V.; Rogler, G.; Zahnd-Straumann, N.; Seibold, F. Factors Influencing the Outcome of Vedolizumab Treatment: Real-life Data with Objective Outcome Measurements. United Eur. Gastroenterol. J. 2021, 9, 398–406. [Google Scholar] [CrossRef] [PubMed]
- De Galan, C.; Truyens, M.; Peeters, H.; Mesonero Gismero, F.; Elorza, A.; Torres, P.; Vandermeulen, L.; Jauregui Amezaga, A.; Ferreiro-Iglesias, R.; Holvoet, T.; et al. The Impact of Vedolizumab and Ustekinumab on Articular Extra-Intestinal Manifestations in Inflammatory Bowel Disease Patients: A Real-Life Multicentre Cohort Study. J. Crohns Colitis 2022, 16, 1676–1686. [Google Scholar] [CrossRef]
- Liefferinckx, C.; Verstockt, B.; Gils, A.; Noman, M.; Van, C.; Macken, E.; Vos, M.D.; Moerkercke, W.V.; Rahier, F.; Bossuyt, P.; et al. Long-Term Clinical Effectiveness of Ustekinumab in Patients with Crohn’s Disease Who Failed Biological Therapies: A National Cohort Study. J. Crohn’s Colitis 2019, 13, 1401–1409. [Google Scholar] [CrossRef]
- Biemans, V.B.C.; Van Der Meulen - De Jong, A.E.; Van Der Woude, C.J.; Löwenberg, M.; Dijkstra, G.; Oldenburg, B.; De Boer, N.K.H.; Van Der Marel, S.; Bodelier, A.G.L.; Jansen, J.M.; et al. Ustekinumab for Crohn’s Disease: Results of the ICC Registry, a Nationwide Prospective Observational Cohort Study. J. Crohns Colitis 2020, 14, 33–45. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Jiang, X.; Peerani, F.; Narula, N.; Chaudrey, K.; Whitehead, D.; Hudesman, D.; Lukin, D.; Swaminath, A.; et al. The Real-World Effectiveness and Safety of Vedolizumab for Moderate–Severe Crohn’s Disease: Results from the US VICTORY Consortium. Am. J. Gastroenterol. 2016, 111, 1147–1155. [Google Scholar] [CrossRef]
- Meserve, J.; Aniwan, S.; Koliani-Pace, J.L.; Shashi, P.; Weiss, A.; Faleck, D.; Winters, A.; Chablaney, S.; Kochhar, G.; Boland, B.S.; et al. Retrospective Analysis of Safety of Vedolizumab in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2019, 17, 1533–1540.e2. [Google Scholar] [CrossRef]
- Vavricka, S.R.; Brun, L.; Ballabeni, P.; Pittet, V.; Vavricka, B.M.P.; Zeitz, J.; Rogler, G.; Schoepfer, A.M. Frequency and Risk Factors for Extraintestinal Manifestations in the Swiss Inflammatory Bowel Disease Cohort. Am. J. Gastroenterol. 2011, 106, 110–119. [Google Scholar] [CrossRef]
- Yeo, M.-K.; Park, J.H.; Kang, S.H.; Moon, H.S.; Sung, J.K.; Jeong, H.Y.; Kim, J.S. What Are the Risk Factors for Extraintestinal Manifestations in Inflammatory Bowel Diseases? Medicine 2023, 102, e33031. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total (n = 80) | SpA (n = 24) | Non-SpA (n = 56) | p-Value | |
|---|---|---|---|---|
| Sociodemographic Variables | ||||
| Mean age (years) * | 52.16 ± 14.3 | 54.9 ± 13.1 | 36.93 ± 18.76 | 0.4 |
| Disease duration * | 14.28 ± 9.4 | 13.29 ± 7.35 | 14 ± 10.18 | 0.2 |
| Sex | ||||
| Male | 36 (45%) | 10 (42%) | 26 (46%) | 0.695 |
| Female | 44 (55%) | 14 (58%) | 30 (54%) | |
| IBD type | ||||
| UC | 27 (34%) | 7 (29%) | 20 (36%) | 0.278 |
| CD | 52 (65%) | 16 (67%) | 36 (64%) | |
| Indeterminate colitis | 1 (1%) | 1 (4%) | 0 (0%) | |
| Smoking status | ||||
| Never | 38 (47.5%) | 10 (42%) | 28 (50%) | 0.519 |
| Former smoker | 30 (37.5%) | 11 (46%) | 19 (34%) | |
| Active smoker | 12 (15%) | 3 (13%) | 9 (16%) | |
| Specific Characteristics of IBD | ||||
| Type of CD | ||||
| Ileitis | 24 (30%) | 6 (25%) | 18 (32%) | 0.823 |
| Ileocolitis | 19 (24%) | 6 (25%) | 13 (23%) | |
| Colitis | 2 (3%) | 1 (4%) | 1 (2%) | |
| Jejunoileitis | 7 (9%) | 2 (8,3%) | 5 (9%) | |
| Type of UC | ||||
| Left-sided | 9 (11%) | 2 (8%) | 7 (12.5%) | 0.940 |
| Pancolitis | 18 (23%) | 4 (17%) | 14 (25%) | |
| CD phenotype | ||||
| Inflammatory | 16 (20%) | 5 (33%) | 11 (20%) | 0.577 |
| Stricturing | 17 (21%) | 6 (40%) | 11 (20%) | |
| Fistulizing | 18 (22.5%) | 4 (27%) | 14 (25%) | |
| Immune-mediated inflammatory diseases | 19 (24%) | 11 (46%) | 8 (14%) | 0.001 |
| Perianal disease (PD) | 15 (19%) | 3 (10.3%) | 12 (21%) | 0.461 |
| VDZ/UST Treatment | ||||
| VDZ | 56 (70%) | 12 (50%) | 44 (79%) | 0.011 |
| UST | 24 (30%) | 12 (50%) | 12 (21%) | |
| HLA-B27 known status | 48 (60%) | |||
| Positive | 5 (6%) | 4 (17%) | 1 (2%) | 0.156 |
| Negative | 43 (54%) | 20 (83%) | 23 (41%) | |
| HLA-B27 unknown status | 32 (40%) | 0 (0%) | 32 (57%) | |
| Previous Biological Treatment | ||||
| 1 biologic | 24 (30%) | 5 (21%) | 19 (34%) | 0.086 |
| 2 biologics | 34 (43%) | 8 (33%) | 26 (46%) | |
| ≥3 biologics | 15 (19%) | 9 (38%) | 6 (11%) | |
| Biologic-naïve | 7 (8%) | 2 (8%) | 5 (9%) | |
| Concomitant DMARDs | ||||
| Thiopurines | 30 (37%) | 5 (21%) | 25 (45%) | 0.006 |
| Methotrexate | 4 (5%) | 1 (4%) | 3 (5%) | |
| Sulfasalazine | 4 (5%) | 4 (17%) | 0 (0%) | |
| Mesalazine | 4 (5%) | 1 (4%) | 3 (5%) | |
| Monotherapy | 38 (48%) | 13 (54%) | 25 (45%) | |
| Corticosteroid use | 3 (4%) | 1 (4%) | 2 (4%) | 0.441 |
| Combined Biological Therapy | ||||
| VDZ + anti-TNF | 1 (1%) | 1 (4%) | 0 (0%) | - |
| UST + anti-TNF | 1 (1%) | 1 (4%) | 0 (0%) | |
| Type | Frequency |
|---|---|
| Spondyloarthritis (SpA) (n = 24) | |
| Previous SpA (n = 22): | |
| Axial | 7 (32%) |
| Peripheral | 11 (50%) |
| Mixed: axial and peripheral | 4 (18%) |
| Onset of SpA(n = 2): | |
| Axial | 0 (0%) |
| Peripheral | 0 (0%) |
| Mixed | 2 (100%) |
| Non-SpA (n = 56) | |
| Osteoarthritis | 8 (14%) |
| Microcrystalline arthritis | 2 (3%) |
| Connective tissue diseases | 3 (6%) |
| Non-inflammatory low back pain | 4 (7%) |
| Non-inflammatory joint pain | 39 (70%) |
| Total (n = 22) | UST (n = 12) | VDZ (n = 10) | |
|---|---|---|---|
| Improvement | 5 (23%) | 5 (42%) | 0 (0%) |
| Stability | 15 (68%) | 6 (50%) | 9 (90%) |
| Flare-up | 2 (9%) | 1 (8%) | 1 (10%) |
| Odds Ratio | Std. Error | p-Value | 95% Confidence Interval | |
|---|---|---|---|---|
| Active smoker | 1.9 | 0.73 | 0.10 | [0.87–4.13] |
| HLA-B27 | 1.9 | 2.66 | 0.64 | [0.12–29.26] |
| Number of biologic treatments | 2.3 | 1.26 | 0.12 | [0.80–6.73] |
| VDZ | 1.6 | 3.35 | 0.82 | [0.03–96.48] |
| UST | 0.6 | 0.58 | 0.57 | [0.14–2.98] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez Diaz, I.; Gutierrez Riart, M.; Martin-Arranz, M.D.; Plasencia Rodriguez, C.; Suarez Ferrer, C.; on behalf of VEDUSTAR Research Team. Incidence and Course of Joint Inflammation Associated with Inflammatory Bowel Disease in Patients Undergoing Treatment with Vedolizumab/Ustekinumab: The VEDUSTAR Study. J. Clin. Med. 2024, 13, 1076. https://doi.org/10.3390/jcm13041076
Gonzalez Diaz I, Gutierrez Riart M, Martin-Arranz MD, Plasencia Rodriguez C, Suarez Ferrer C, on behalf of VEDUSTAR Research Team. Incidence and Course of Joint Inflammation Associated with Inflammatory Bowel Disease in Patients Undergoing Treatment with Vedolizumab/Ustekinumab: The VEDUSTAR Study. Journal of Clinical Medicine. 2024; 13(4):1076. https://doi.org/10.3390/jcm13041076
Chicago/Turabian StyleGonzalez Diaz, Irene, Mariana Gutierrez Riart, Maria Dolores Martin-Arranz, Chamaida Plasencia Rodriguez, Cristina Suarez Ferrer, and on behalf of VEDUSTAR Research Team. 2024. "Incidence and Course of Joint Inflammation Associated with Inflammatory Bowel Disease in Patients Undergoing Treatment with Vedolizumab/Ustekinumab: The VEDUSTAR Study" Journal of Clinical Medicine 13, no. 4: 1076. https://doi.org/10.3390/jcm13041076
APA StyleGonzalez Diaz, I., Gutierrez Riart, M., Martin-Arranz, M. D., Plasencia Rodriguez, C., Suarez Ferrer, C., & on behalf of VEDUSTAR Research Team. (2024). Incidence and Course of Joint Inflammation Associated with Inflammatory Bowel Disease in Patients Undergoing Treatment with Vedolizumab/Ustekinumab: The VEDUSTAR Study. Journal of Clinical Medicine, 13(4), 1076. https://doi.org/10.3390/jcm13041076