
The Impact of Thermal Water in Asthma and COPD: A Systematic Review According to the PRISMA Statement

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Review Question
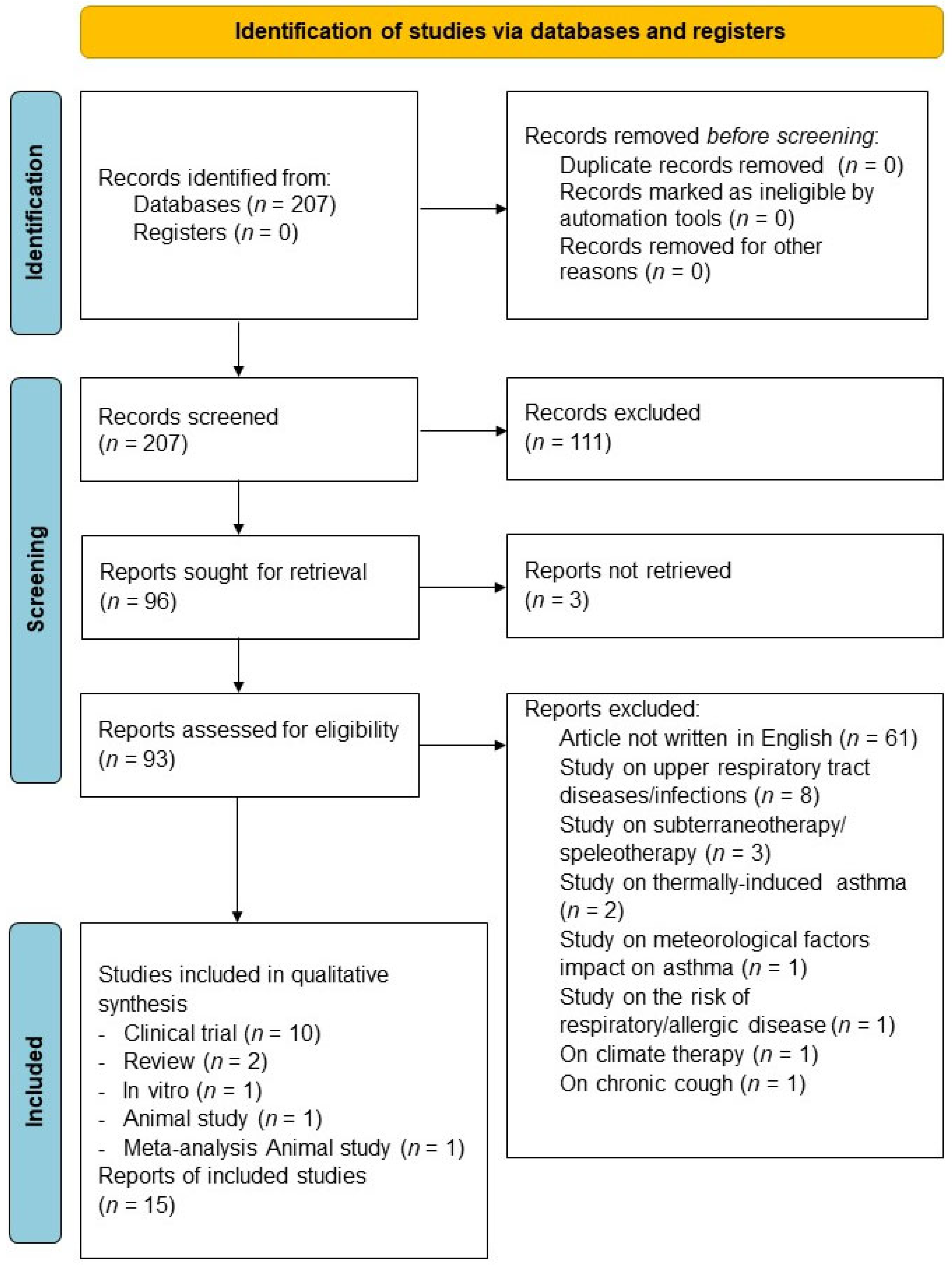
2.2. Search Strategy and Study Eligibility
2.3. Data Extraction
2.4. Endpoint
2.5. Strategy for Data Synthesis
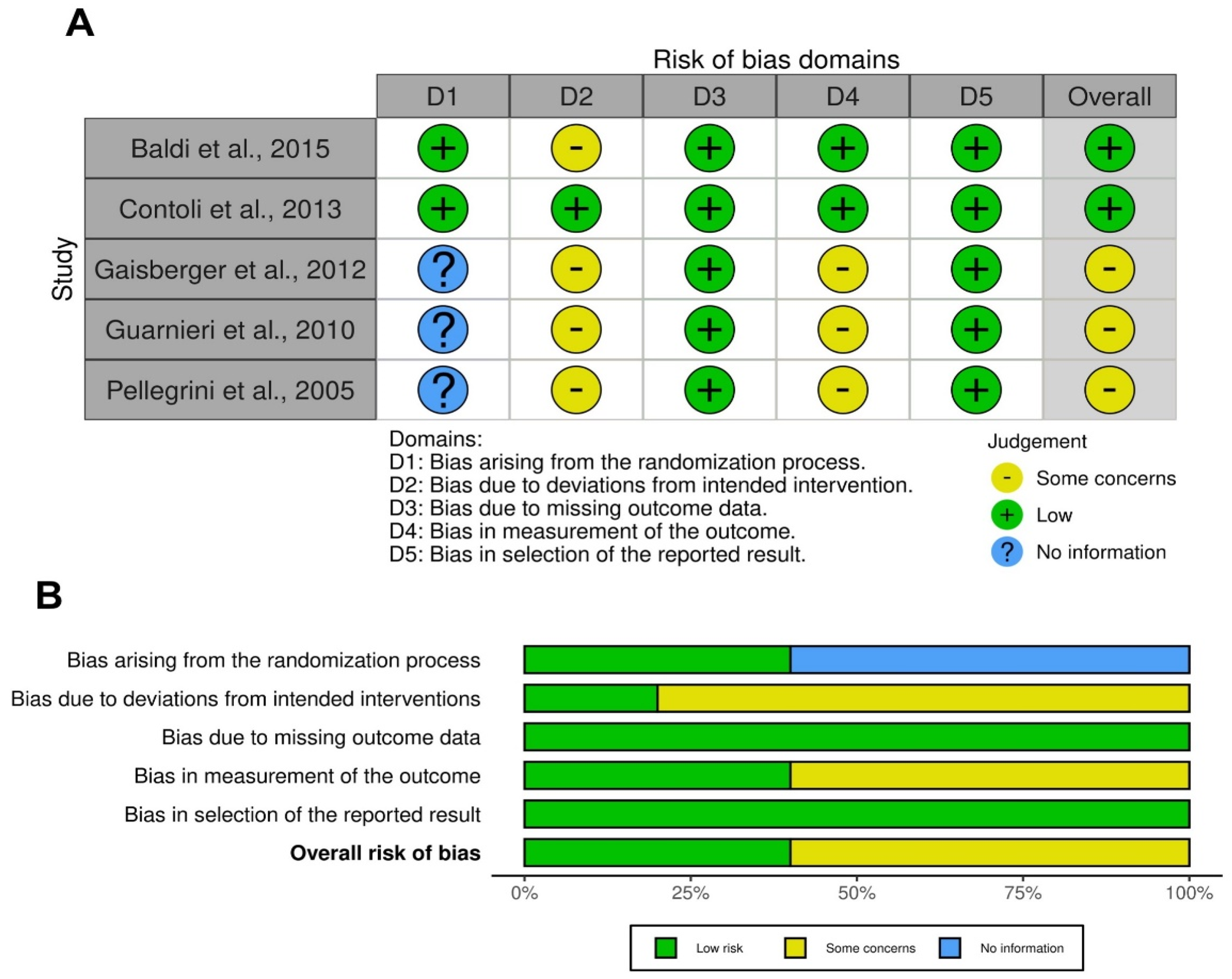
2.6. Quality of Studies and Risk Bias
3. Results
3.1. Study Characteristics
3.2. Studies In Vitro
3.3. Studies in Experimental Animals
3.4. RCTs
3.5. Non-RCTs
3.6. Observational Studies
4. Quality of Evidence and Risk of Bias
5. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur. Respir. J. 2023, 61, 2300239. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.L.; Bacharier, L.B.; Bateman, E.; Boulet, L.-P.; Brightling, C.; Buhl, R.; Brusselle, G.; Cruz, A.A.; Drazen, J.M.; Duijts, L.; et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. Prim. Care Respir. Med. 2023, 33, 7. [Google Scholar] [CrossRef] [PubMed]
- Tamondong-Lachica, D.R.; Skolnik, N.; Hurst, J.R.; Marchetti, N.; Rabe, A.P.J.; de Oca, M.M.; Celli, B.R. GOLD 2023 Update: Implications for Clinical Practice. SSRN Electron. J. 2023, 18, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, G.; Ferrazzoni, S.; Scarpa, M.C.; Lalli, A.; Maestrelli, P. Effects of Inhalation of Thermal Water on Exhaled Breath Condensate in Chronic Obstructive Pulmonary Disease. Respiration 2010, 79, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Viegas, J.; Esteves, A.F.; Cardoso, E.M.; Arosa, F.A.; Vitale, M.; Taborda-Barata, L. Biological Effects of Thermal Water-Associated Hydrogen Sulfide on Human Airways and Associated Immune Cells: Implications for Respiratory Diseases. Front. Public Health 2019, 7, 128. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Lobanov, A.A.; Fesyun, A.D.; Voronenko, A.G.; Andronov, S.V.; Yakovlev, M.Y.; Rachin, A.P.; Solimene, U.; Nikitina, A.M.; Zaitsev, A.R.; Kochetkova, V.; et al. The application of mineral water in the treatment of chronic obstructive pulmonary disease: A meta-analysis. Minerva Respir. Med. 2021, 60, 100–113. [Google Scholar] [CrossRef]
- Zajac, D. Inhalations with thermal waters in respiratory diseases. J. Ethnopharmacol. 2021, 281, 114505. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing Risk of Bias in a Randomized Trial. Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). 2019, pp. 205–228. Available online: www.training.cochrane.org/handbook (accessed on 7 February 2024).
- Pedder, H.; Sarri, G.; Keeney, E.; Nunes, V.; Dias, S. Data extraction for complex meta-analysis (DECiMAL) guide. Syst. Rev. 2016, 5, 212. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and web application for visualising risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Baldi, S.; Pinna, G.D.; Bruschi, C.; Caldara, F.; Dacosto, E.; Crotti, P.; Popovich, E.; Bellinzona, E.; Montemartini, S.; Fracchia, C.; et al. Medicinal clays improve the endurance of loaded inspiratory muscles in COPD: A randomized clinical trial of nonpharmacological treatment. SSRN Electron. J. 2015, 10, 2235–2248. [Google Scholar] [CrossRef]
- Contoli, M.; Gnesini, G.; Forini, G.; Marku, B.; Pauletti, A.; Padovani, A.; Casolari, P.; Taurino, L.; Ferraro, A.; Chicca, M.; et al. Reducing Agents Decrease the Oxidative Burst and Improve Clinical Outcomes in COPD Patients: A Randomised Controlled Trial on the Effects of Sulphurous Thermal Water Inhalation. Sci. World J. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Gaisberger, M.; Šanović, R.; Dobias, H.; Kolarž, P.; Moder, A.; Thalhamer, J.; Selimović, A.; Huttegger, I.; Ritter, M.; Hartl, A.; et al. Effects of Ionized Waterfall Aerosol on Pediatric Allergic Asthma. J. Asthma 2012, 49, 830–838. [Google Scholar] [CrossRef]
- Pellegrini, M.; Fanin, D.; Nowicki, Y.; Guarnieri, G.; Bordin, A.; Faggian, D.; Plebani, M.; Saetta, M.; Maestrelli, P. Effect of inhalation of thermal water on airway inflammation in chronic obstructive pulmonary disease. Respir. Med. 2005, 99, 748–754. [Google Scholar] [CrossRef]
- Mitsunobu, F.; Yamaoka, K.; Hanamoto, K.; Kojima, S.; Hosaki, Y.; Ashida, K.; Sugita, K.; Tanizaki, Y. Elevation of Antioxidant Enzymes in the Clinical Effects of Radon and Thermal Therapy for Bronchial Asthma. J. Radiat. Res. 2003, 44, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Tanizaki, Y.; Kitani, H.; Okazaki, M.; Mifune, T.; Mitsunobu, F.; Honke, N. Clinical effects of complex spa therapy on patients with steroid-dependent intractable asthma (SDIA). Jpn. J. Allergol. 1993, 42, 219–227. [Google Scholar]
- Carubbi, C.; Masselli, E.; Calabrò, E.; Bonati, E.; Galeone, C.; Andreoli, R.; Goldoni, M.; Corradi, M.; Sverzellati, N.; Pozzi, G.; et al. Sulphurous thermal water inhalation impacts respiratory metabolic parameters in heavy smokers. Int. J. Biometeorol. 2019, 63, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Takata, K.; Ashida, A.; Hosaki, Y.; Iwagaki, N.; Kikuchi, H.; Mitsunobu, F. Effect of spa therapy on the six-minute walk test in patients with chronic obstructive pulmonary disease. J. Jpn. Soc. Balneol. Climatol. Phys. Med. 2008, 71, 241–249. [Google Scholar]
- Pironti, C.; Ricciardi, M.; Motta, O.; Venier, M.; Faggiano, A.; Cucciniello, R.; Proto, A. Sulphurous air pollutants and exposure events of workers in thermal-mineral springs: A case study of Contursi Terme (Salerno, Italy). Environ. Sci. Pollut. Res. 2022, 30, 3112–3120. [Google Scholar] [CrossRef] [PubMed]
- Melgar-Sánchez, L.M.; García-Ruiz, I.; Pardo-Marqués, V.; Agulló-Ortuño, M.T.; Martínez-Galán, I. Influence of mineral waters on in vitro proliferation, antioxidant response and cytokine production in a human lung fibroblasts cell line. Int. J. Biometeorol. 2019, 63, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Zając, D.; Russjan, E.; Kostrzon, M.; Kaczyńska, K. Inhalations with Brine Solution from the ‘Wieliczka’ Salt Mine Diminish Airway Hyperreactivity and Inflammation in a Murine Model of Non-Atopic Asthma. Int. J. Mol. Sci. 2020, 21, 4798. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]
- Selroos, O.; Kupczyk, M.; Kuna, P.; Łacwik, P.; Bousquet, J.; Brennan, D.; Palkonen, S.; Contreras, J.; FitzGerald, M.; Hedlin, G.; et al. National and regional asthma programmes in Europe. Eur. Respir. Rev. 2015, 24, 474–483. [Google Scholar] [CrossRef]
- Cazzola, M.; Puxeddu, E.; Bettoncelli, G.; Novelli, L.; Segreti, A.; Cricelli, C.; Calzetta, L. The prevalence of asthma and COPD in Italy: A practice-based study. Respir. Med. 2011, 105, 386–391. [Google Scholar] [CrossRef]
- Bates, M.N.; Garrett, N.; Crane, J.; Balmes, J.R. Associations of ambient hydrogen sulfide exposure with self-reported asthma and asthma symptoms. Environ. Res. 2013, 122, 81–87. [Google Scholar] [CrossRef]
- Yan, M.; Li, C.; Zhang, L.; Chen, X.; Yang, X.; Shan, A.; Li, X.; Wu, H.; Ma, Z.; Zhang, Y.; et al. Association between long-term exposure to Sulfur dioxide pollution and hypertension incidence in northern China: A 12-year cohort study. Environ. Sci. Pollut. Res. 2020, 27, 21826–21835. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Study, Year and Reference | Type of Study (Characteristics) | Treatment Duration | Type of Cells, Animals, Donors, or Analyzed Patients | Number of Cell Donors, Animals, or Analyzed Patients | Type of Exposure and/or Treatment with TW | Route of Administration and Temperature | Age (Years) | Male (%) | Current Smokers (%) | Post Bronchodilator FEV1 (% Predicted) | Comparator | Evaluated Outcomes | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pironti et al., 2022 [24] | Clinical trial (case study) | 4 months | Workers in thermal-mineral springs | NA | Bicarbonate sulfurous TW from Contursi Terme in Salerno, Italy | NA,” hot” | NA | NA | NA | NA | NA | Physicochemical analysis of TW and monitoring of air concentrations of H2S and SO2 in the thermal springs | NA |
| Zajac et al., 2020 [26] | In vivo study (murine model of non-atopic asthma) | NA | BALB/c mice intratracheally sensitized with 0.5% DNFB and challenged with cognate hapten-50 μL of 0.6% DNS | 50 | Brine solution containing sodium chloride TW from the “Wieliczka” Salt Mine | Inhalation, NA | 7–8 wks | 100.0 | NA | NA | Sensitized mice inhaled with pure water or 0.9% NaCl or untreated | AHR, inflammation, and oxidative stress | NA |
| Carubbi et al., 2019 [22] | Clinical trial (observational, cohort study) | 10 days | Heavy current and former smokers with ≥20 pack-years of smoking history | 419 | Sulfurous TW | Inhalation, NA | 63.2 | 58.9 | 49.2 | 87.4 | Baseline | Pulmonary function and EBC metabolic analysis | NA |
| Melgar-Sánchez et al., 2019 [25] | In vitro study | NA | Human lung embryonic fibroblast LC5 cells | NA | Sulfurous MW from Spanish health resorts of Baños de Ledesma, Paracuellos de Jiloca, and Archena | Incubation, NA | NA | NA | NA | NA | Untreated cells | Cell proliferation, oxidative stress, and inflammation | NA |
| Baldi et al., 2015, NCT01253941 [16] | Clinical trial (single-center, randomized, unblinded, parallel-group study) | 2 wks (12 sessions) | Mild to severe COPD patients (FEV1/FVC ≤ 70%, change in post-bronchodilator FEV1 < 12% and 200 mL defined the presence of chronic airflow obstruction) | 42 | Sulfurous TW from Colli Euganei mineral-water field | Exposure to TW by unsupervised leisure activity in thermal pools, 38–42 °C | 64.6 | 78.6 | 40.5 | 68.3 | Mud bath therapy | Pulmonary function, endurance time and O2 expenditure, and plasma IL-6 concentration level following an IRB challenge | 3 |
| Contoli et al., 2013, NCT01664767 [17] | Clinical trial (single-center, randomized, controlled, double-blind, parallel-group study) | 12 days | COPD patients (FEV1/FVC < 70%, post-bronchodilator FEV1 > 30% and < 80% of predicted; at GOLD stages 2 and 3) | 40 | Sulfurous TW from Terme di Riolo in Ravenna, Italy | Inhalation, “warm” | 69.9 | 72.5 | 5.0 | 58.1 | Inhalation of isotonic saline solution | Pulmonary function, health status, oxidative stress, and airway inflammation | 5 |
| Gaisberger et al., 2012, ISRCTN04002573 [18] | Clinical trial (single-center, randomized controlled, unblinded, parallel-group study) | 3 wks, 1 h per day | Children affected by asthma | 54 | Exposure to waterfall environment by inhaling of ions and aerosols generated by splashing of water termed “ionosols” combined with high-altitude climate therapy | TW aerosol by exposure to waterfall, NA | 11.0 | 69.2 | 0.0 | 81.8 | High-altitude climate therapy | Pulmonary function, symptoms control, airway inflammation (including FeNO) | 2 |
| Guarnieri et al., 2010 [4] | Clinical trial (single-center, randomized, controlled, single-blind, crossover study | 2 wks | COPD patients (FEV1/FVC < 70%, post-bronchodilator reversibility < 12% and 200 mL of initial FEV1; at GOLD stages 1–3) | 13 | Salt-bromide-iodine TW | Inhalation, 80 °C | 69.0 | 76.9 | 38.5 | 66.6 | Inhalation of normal saline and baseline | Airway-lining fluid by analysis of EBC pH and LTB4 level, pulmonary function, and dyspnea | 2 |
| Takata et al., 2008 [23] | Clinical trial (observational study) | 4 wks | Hospitalized COPD patients (GOLD stages 1–3) | 25 | Spa therapy including swimming training and exercise in a hot spring pool, inhalation of iodine salt solution and fango therapy | Exposure to environment with TW and inhalation, “hot” | 73.3 | 88.0 | 0.0 | NA | Baseline | Pulmonary function, 6 MWT, and O2 saturation | NA |
| Pellegrini et al., 2005 [19] | Clinical trial (single-center, randomized, controlled, single-blind, parallel-group study) | 2 wks | Stable COPD (FEV1/FVC < 70%, post-bronchodilator reversibility < 15% or 200 mL of initial FEV1; patients with smoking history of ≥10 pack/year and chronic bronchitis) | 39 | Salt-bromide-iodine TW | Inhalation, 37 °C | 64.0 | 89.7 | 100.0 | 72.0 | Inhalation of normal saline and baseline | Inflammation, SGRQ, dyspnea, and 6 MWT | 2 |
| Mistunobu et al., 2003 [20] | Clinical trial (pilot interventional study, not randomized, not controlled) | 4 wks | Atopic asthma | 9 | Radon and TW therapy | Inhalation, 48 °C | 59.0 | 55.6 | 0.0 | NA | Baseline | Pulmonary function and oxidative stress | NA |
| Tanizaki et al., 1993 [21] | Clinical trial (interventional study, not randomized, not controlled) | 1–3 months | Steroid-dependent intractable asthma | 52 | Exposure to TW by spa therapy including swimming training in a hot spring pool, iodine salt solution inhalation twice daily, and fango therapy | Exposure to environment with TW and inhalation, 70–80 °C | 57.7 | 44.2 | 0.0 | NA | Baseline | AHR, pulmonary function and inflammation | NA |
| Type of MW | Outcomes | |||
|---|---|---|---|---|
| Cell Proliferation (Fibroblasts) | Oxidant Activity (ROS-RNS) | GSH | Cytokines Profiling (MIF, IL-6, CL-1, CCL-5, ICAM-1) | |
| Ledesma | ↑ [25] | ≈ [25] | NA | ↑ [25] |
| Paracuellos | ↑ [25] | ↑ in autumn ↓ in spring [25] | ↑ in autumn and spring [25] | ↑ [25] |
| Archena | ↑ [25] | ↑ in spring ↓ in autumn [25] | ↑ in autumn [25] | ↑ [25] |
| Type of TW | Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|
| AHR to MCh | Inflammatory Cells | Neutrophil | IL-1α | IL-6 | IL-10 | IL-1β | GSH | |
| Wieliczka Salt Mine (inhalation of brine solution) | ↓ [26] | ↓ [26] | ↓ [26] | ↓ [26] | ↓ [26] | ≈ [26] | ≈ [26] | ↓ [26] |
| Polish health resort (inhalation of brine solution) | ↓ [26] | ↓ [26] | ↓ [26] | ↓ [26] | ↓ [26] | ≈ [26] | ≈ [26] | ↓ [26] |
| Type of Mineral Water | Outcomes | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LTB 4 in EBC | pH in EBC | FEV1 | O2− Production | CAT | ACT | Dyspnea | SGRQ | ECP | T Cell | ET | Sputum | Sputum Neutrophils | Macrophage | IRB | IL-6 | VO2Endur | FeNO | IL-5-, IL-10, IL-13 | |
| Salt-bromide-iodine (inhalation) | ≈ [4] | ↓ [4] | ≈ [4,19] | NA | NA | NA | ≈ [4,19] | ↓ [19] | NA | NA | NA | ↓ [19] | ↓ [19] | ↑ [19] | NA | NA | NA | NA | NA |
| Sulfurous (inhalation) | NA | NA | ≈ [17] | ↓ [17] | ↓ [17] | NA | NA | NA | NA | NA | NA | ≈ [17] | NA | NA | NA | NA | NA | NA | NA |
| Mud bath water natural clay sulfur-rich mineral | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | ↑ [16] | NA | NA | NA | ↑ [16] | ≈ [16] | ↑ [16] | NA | NA |
| Alpine waterfall | NA | NA | ↑ [18] | NA | NA | ↑ [18] | NA | NA | ≈ [18] | ↑ [18] | NA | NA | NA | NA | NA | NA | NA | ↓ [18] | ↓ [18] |
| Type of TW | Outcomes | ||||
|---|---|---|---|---|---|
| FEV1/FVC | Blood Catalase and SOD | Lipid Peroxide | Neutrophil—Eosinophil | AHR | |
| Radon and TW (inhalation) | ↑ [20] | ↑ [20] | ↓ [20] | NA | NA |
| Iodine salt solution (inhalation) | NA | NA | NA | ↑ [21] | ↓ [21] |
| Type of TW | Outcomes | ||||||
|---|---|---|---|---|---|---|---|
| Citrulline | Ornithine | NO | FEV1 | Maximum Borg Scale Values | SO2 | H2S | |
| Sulfurous (inhalation) | ↑ [22] | ↓ [22] | ↓ [22] | NA | NA | ↑ [24] | ≈ indoor; ↑ outdoor [24] |
| Spa therapy | NA | NA | NA | ≈ [23] | ↓ [23] | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calzetta, L.; Di Daniele, N.; Chetta, A.; Vitale, M.; Gholamalishahi, S.; Cazzola, M.; Rogliani, P. The Impact of Thermal Water in Asthma and COPD: A Systematic Review According to the PRISMA Statement. J. Clin. Med. 2024, 13, 1071. https://doi.org/10.3390/jcm13041071
Calzetta L, Di Daniele N, Chetta A, Vitale M, Gholamalishahi S, Cazzola M, Rogliani P. The Impact of Thermal Water in Asthma and COPD: A Systematic Review According to the PRISMA Statement. Journal of Clinical Medicine. 2024; 13(4):1071. https://doi.org/10.3390/jcm13041071
Chicago/Turabian StyleCalzetta, Luigino, Nicola Di Daniele, Alfredo Chetta, Marco Vitale, Shima Gholamalishahi, Mario Cazzola, and Paola Rogliani. 2024. "The Impact of Thermal Water in Asthma and COPD: A Systematic Review According to the PRISMA Statement" Journal of Clinical Medicine 13, no. 4: 1071. https://doi.org/10.3390/jcm13041071
APA StyleCalzetta, L., Di Daniele, N., Chetta, A., Vitale, M., Gholamalishahi, S., Cazzola, M., & Rogliani, P. (2024). The Impact of Thermal Water in Asthma and COPD: A Systematic Review According to the PRISMA Statement. Journal of Clinical Medicine, 13(4), 1071. https://doi.org/10.3390/jcm13041071