
Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy in Children—A Literature Review
 , , ,
, , ,
Abstract
1. Introduction
2. VNS Therapy Device
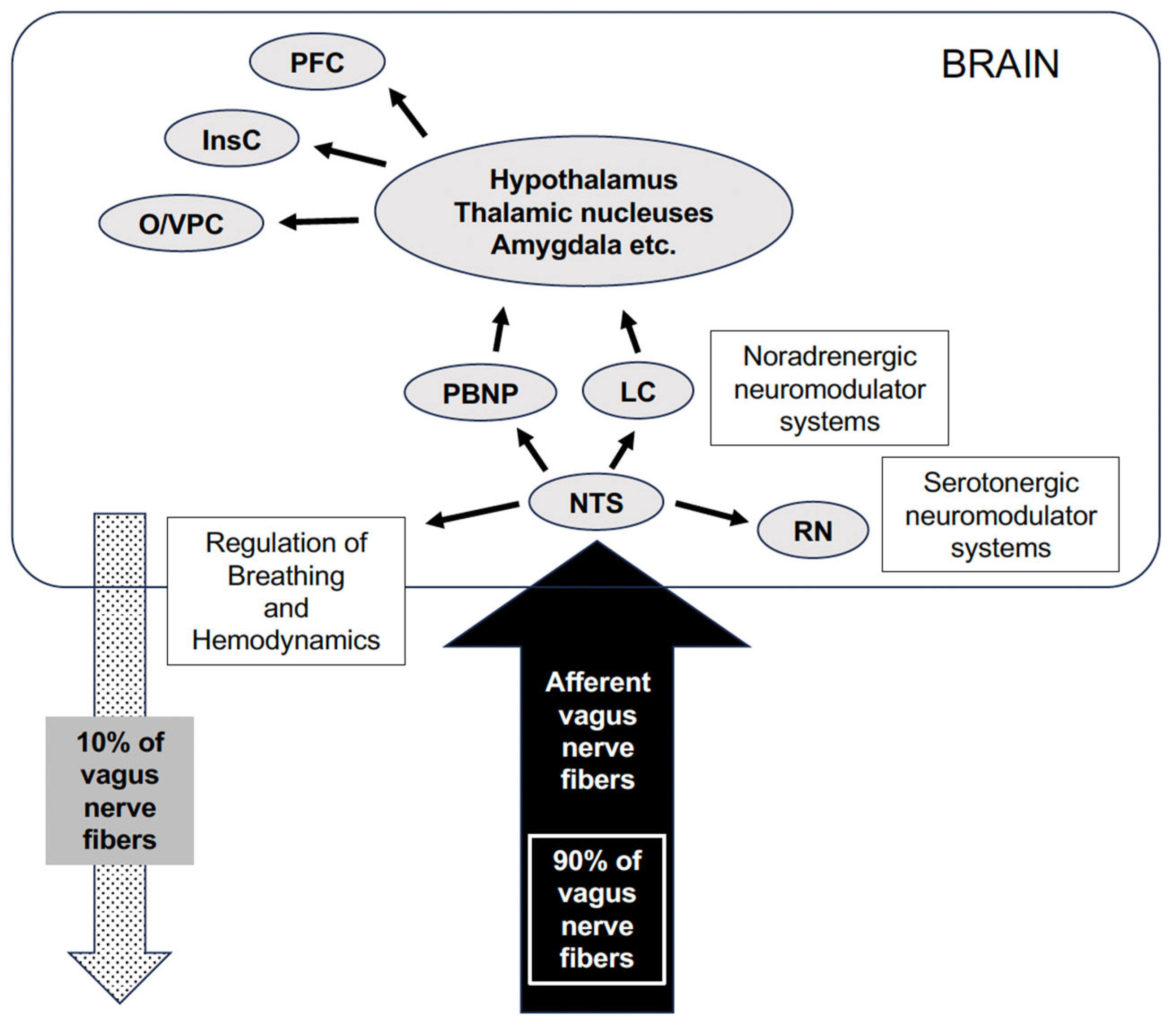
3. Anatomy of the Vagus Nerve and Mechanism of Antiepileptic Action of VNS
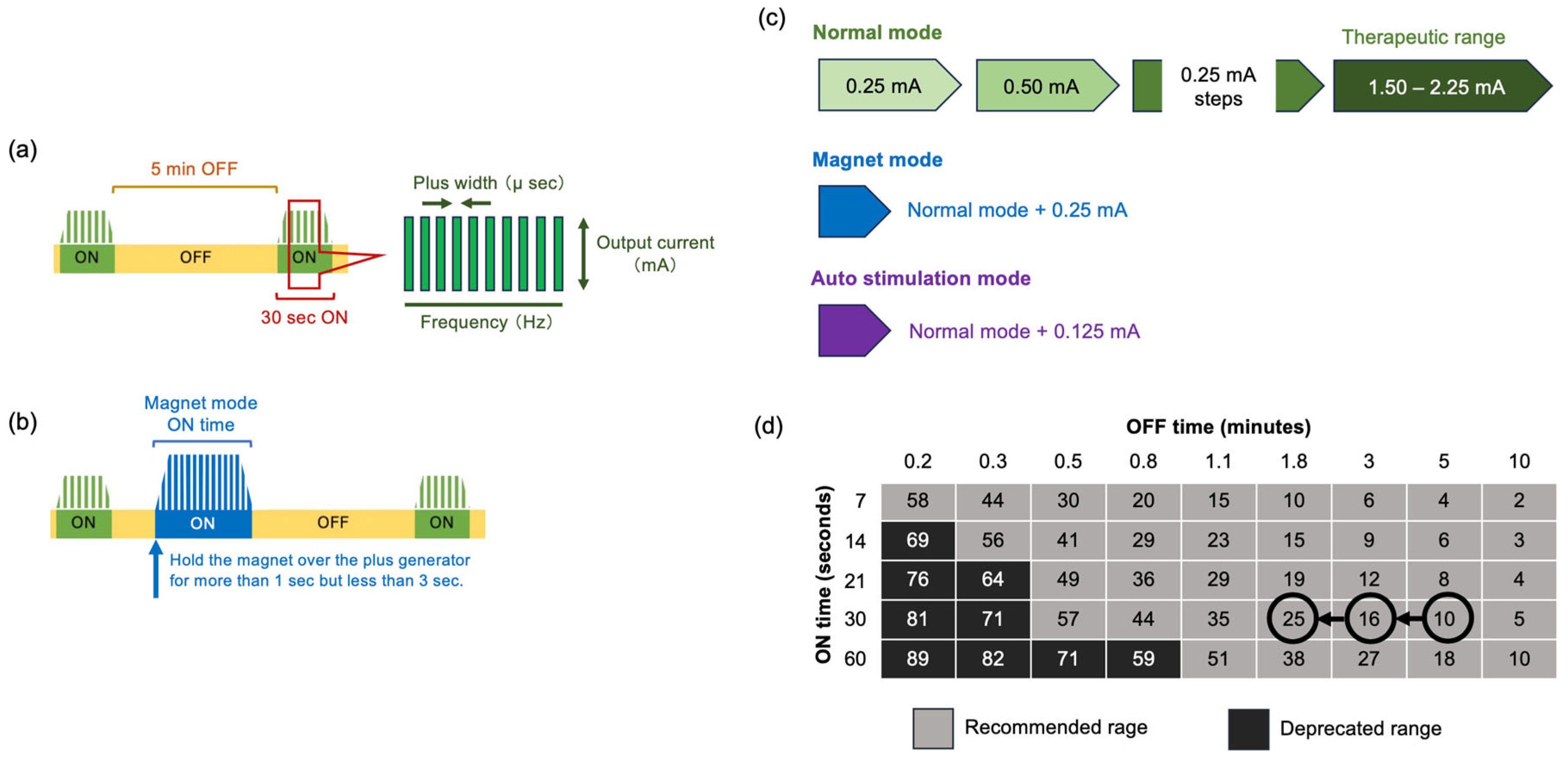
4. Specific Basic Stimulus Adjustment of VNS
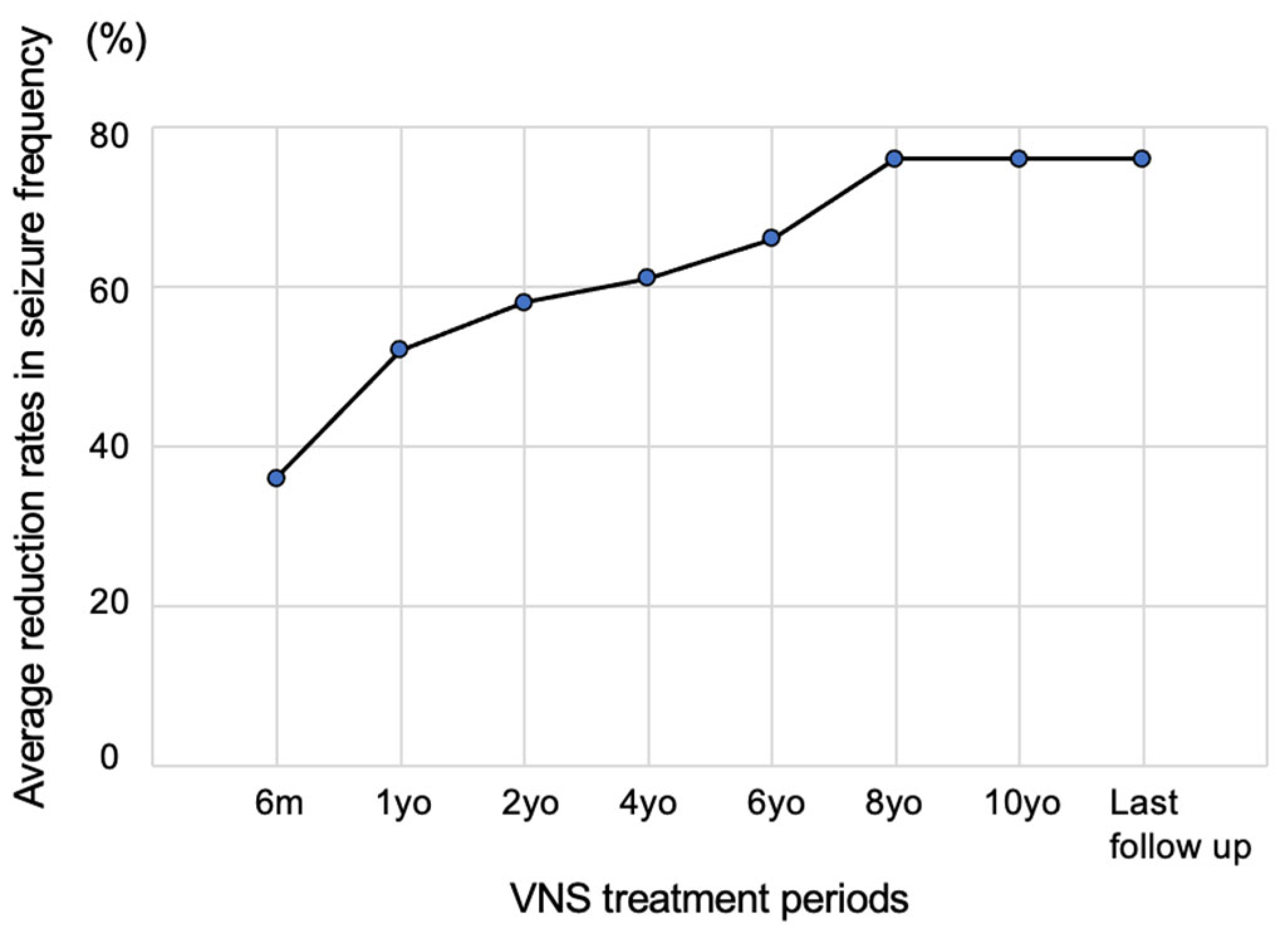
5. Seizure Suppression Effect
6. VNS Device with an Automatic Seizure Control System Based on Heart Rate Fluctuations
7. Clinical Effects and Benefits Other Than Seizures
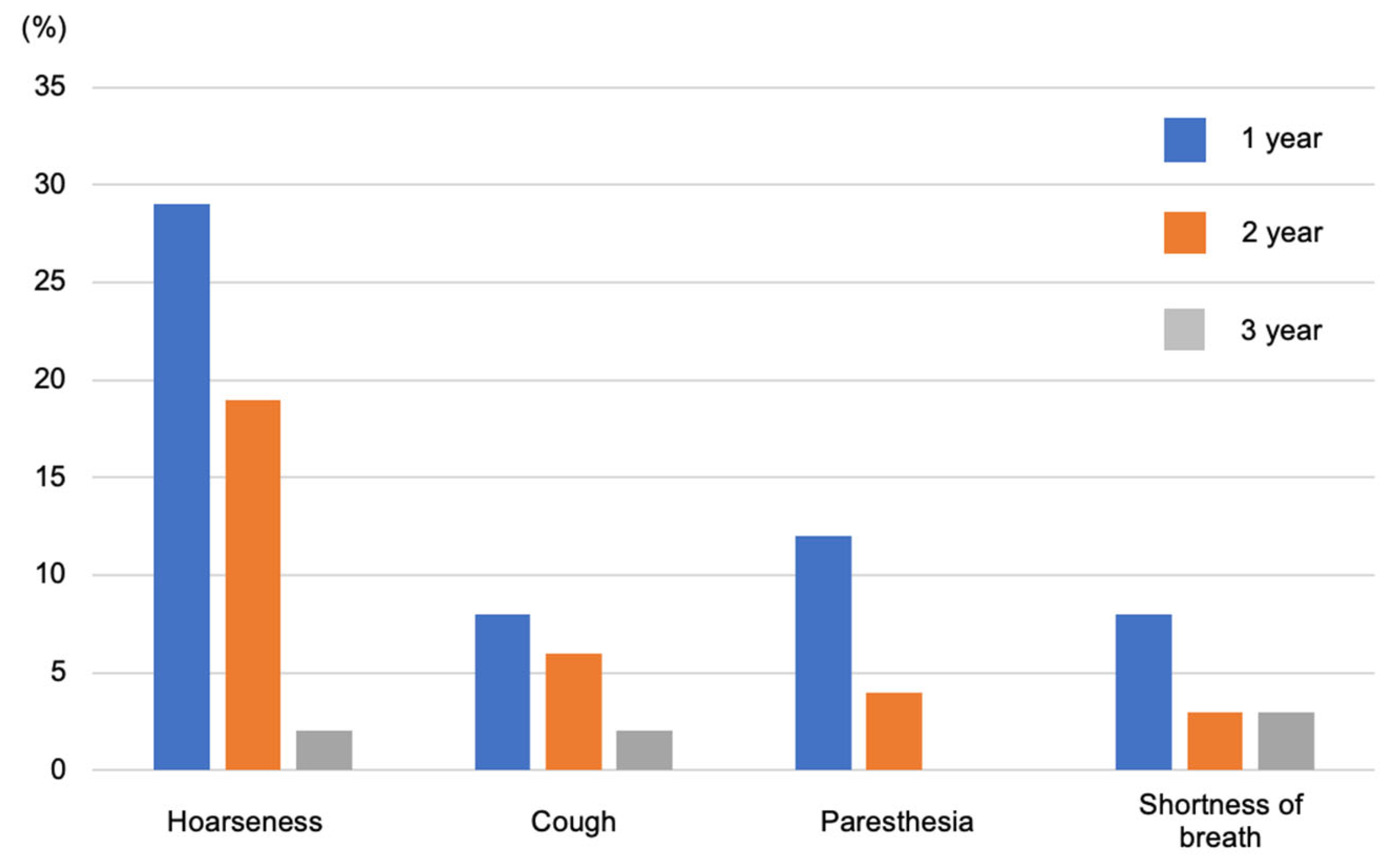
8. Side Effects
9. Effect on Pediatric Drug-Resistant Epilepsy
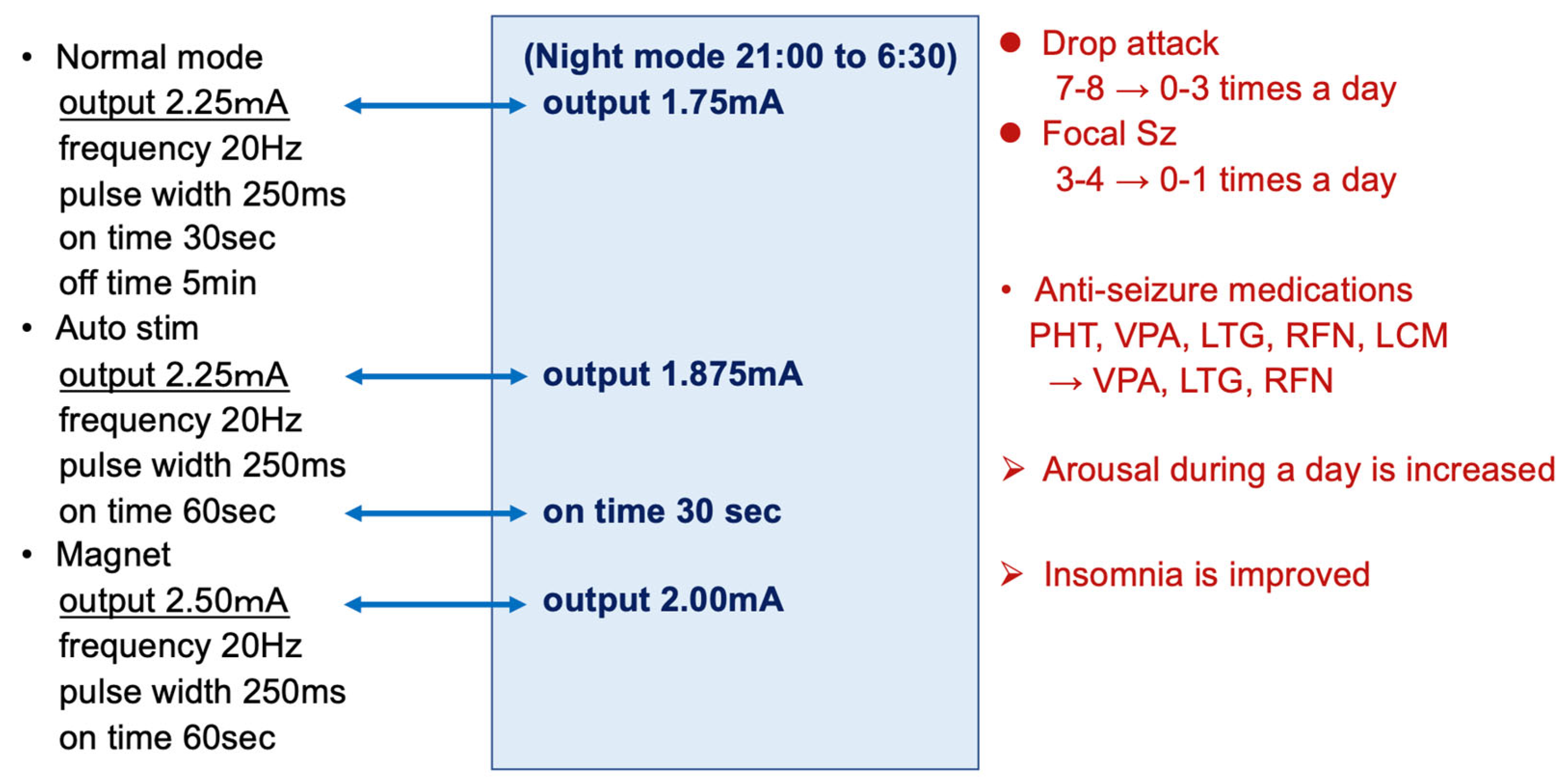
10. Clinical Efficacy of the Latest Model SentTiva: An Illustrative Report
11. Future Perspectives
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- What Is VNS Therapy™ and How Does It Work? Available online: https://www.livanova.com/epilepsy-vnstherapy/en-us (accessed on 6 December 2023).
- Capilupi, M.J.; Kerath, S.M.; Becker, L.B. Vagus nerve stimulation and the cardiovascular system. Cold Spring Harb. Perspect. Med. 2020, 10, a034173. [Google Scholar] [CrossRef]
- Binnie, C.D. Vagus nerve stimulation for epilepsy: A review. Seizure 2000, 9, 161–169. [Google Scholar] [CrossRef]
- Berthoud, H.R.; Neuhuber, W.L. Functional and chemical anatomy of the afferent vagal system. Auton. Neurosci. 2000, 85, 1–17. [Google Scholar] [CrossRef]
- Breit, S.; Kupferberg, A.; Rogler, G.; Hasler, G. Vagus nerve as modulator of the brain–gut axis in psychiatric and inflammatory Disorders. Front. Psychiatry 2018, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Olejniczak, P.W.; Fisch, B.J.; Carey, M.; Butterbaugh, G.; Happel, L.; Tardo, C. The effect of vagus nerve stimulation on epileptiform activity recorded from hippocampal depth electrodes. Epilepsia 2001, 42, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.R.; Bakay, R.A.; Pennell, P.B.; Epstein, C.M.; Votaw, J.R. Brain blood-flow alterations induced by therapeutic vagus nerve stimulation in partial epilepsy: II. prolonged effects at high and low levels of stimulation. Epilepsia 2004, 45, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Dolphin, H.; Dukelow, T.; Finucane, C.; Commins, S.; McDlwaine, P.; Kennelly, S.P. The wandering nerve linking heart and mind”—The complementary role of transcutaneous vagus nerve stimulation in modulating neuro cardiovascular and cognitive performance. Front. Neurosci. 2022, 16, 897303. [Google Scholar] [CrossRef] [PubMed]
- Roosevelt, R.W.; Smith, D.C.; Clough, R.W.; Jensen, R.A.; Browning, R.A. Increased extracellular concentrations of norepinephrine in cortex and hippocampus following vagus nerve stimulation in the rat. Brain Res. 2006, 1119, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Ben-Menachem, E.; Hamberger, A.; Hedner, T.; Hammond, E.J.; Uthman, B.M.; Slater, J.; Treig, T.; Stefan, H.; Ramsay, R.E.; Wernicke, J.F.; et al. Effects of vagus nerve stimulation on amino acids and other metabolites in the CSF of patients with partial seizures. Epilepsy Res. 1995, 20, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Majoie, H.J.; Rijkers, K.; Berfelo, M.W.; Hulsman, J.A.; Myint, A.; Schwarz, M.; Vles, J.S. Vagus nerve stimulation in refractory epilepsy: Effects on pro- and anti-inflammatory cytokines in peripheral blood. Neuroimmunomodulation 2011, 18, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Selden, N.R.; Aballay, A. Anti-inflammatory effects of vagus nerve stimulation in pediatric patients with epilepsy. Front. Immunol. 2023, 14, 1093574. [Google Scholar] [CrossRef] [PubMed]
- Koo, B. EEG changes with vagus nerve stimulation. J. Clin. Neurophysiol. 2001, 18, 434–441. [Google Scholar] [CrossRef] [PubMed]
- The Vagus Nerve Stimulation Study Group. A randomized controlled trial of chronic vagus nerve stimulation for treatment of medically intractable seizures. Neurology 1995, 45, 224–230. [Google Scholar] [CrossRef]
- Handforth, A.; DeGiorgio, C.; Schachter, S.; Uthman, B.M.; Naritoku, D.K.; Tecoma, E.S.; Henry, T.R.; Collins, S.D.; Vaughn, B.V.; Gilmartin, R.C.; et al. Vagus nerve stimulation for partial onset seizures: A randomized active control trial. Neurology 1998, 51, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Dosing Guidelines SenTivaTM. Available online: https://www.livanova.com/epilepsy-vnstherapy/getmedia/65970855-63ee-4b51-adae-3c4215998c33/sentiva_dosing_guide_2022_digital_dsgdsen19u1_2.pdf (accessed on 6 December 2023).
- Fahoum, F.; Boffini, M.; Kann, L.; Faini, S.; Gordon, C.; Tzadok, M.; El Tahry, R. VNS parameters for clinical response in Epilepsy. Brain Stimul. 2022, 15, 814–821. [Google Scholar] [CrossRef]
- McHugh, J.C.; Singh, H.W.; Phillips, J.; Murphy, K.; Doherty, C.P.; Delanty, N. Outcome measurement after vagal nerve stimulation therapy: Proposal of a new classification. Epilepsia 2007, 48, 375–378. [Google Scholar] [CrossRef]
- Ben-Menachem, E. Vagus-nerve stimulation for the treatment of epilepsy. Lancet Neurol. 2002, 1, 477–482. [Google Scholar] [CrossRef]
- Elliott, R.E.; Morsi, A.; Tanweer, O.; Grobelny, B.; Geller, E.; Carlson, C.; Devinsky, O.; Doyle, W.K. Efficacy of vagus nerve stimulation over time: Review of 65 consecutive patients with treatment-resistant epilepsy treated with VNS > 10 years. Epilepsy Behav. 2011, 20, 478–483. [Google Scholar] [CrossRef]
- Skrehot, H.C.; Englot, D.J.; Haneef, Z. Neuro-stimulation in focal epilepsy: A systematic review and meta-analysis. Epilepsy Behav. 2023, 142, 109182. [Google Scholar] [CrossRef]
- Boon, P.; Vonck, K.; van Rijckevorsel, K.E.L.; Tahry, R.; Elger, C.E.; Mullatti, N.; Schulze-Bonhage, A.; Wagner, L.; Diehl, B.; Hamer, H.; et al. A prospective, multicenter study of cardiac-based seizure detection to activate vagus nerve stimulation. Seizure 2015, 32, 52–61. [Google Scholar] [CrossRef]
- Safety Information about VNS Therapy. Available online: https://www.livanova.com/epilepsy-vnstherapy/en-us/safety-information (accessed on 8 January 2024).
- Ryvlin, P.; So, E.L.; Gordon, C.M.; Hesdorffer, D.C.; Sperling, M.R.; Devinsky, O.; Bunker, M.T.; Olin, B.; Friedman, D. Long-term surveillance of SUDEP in drug-resistant epilepsy patients treated with VNS therapy. Epilepsia 2018, 59, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Ryvlin, P.; Gilliam, F.G.; Nguyen, D.K.; Colicchio, G.; Iudice, A.; Tinuper, P.; Zamponi, N.; Aguglia, U.; Wagner, L.; Minotti, L.; et al. The long-term effect of vagus nerve stimulation on quality of life in patients with pharmacoresistant focal epilepsy: The PuLsE (Open Prospective Randomized Long-term Effectiveness) trial. Epilepsia 2014, 55, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Ravan, M.; Begnaud, J. Investigating the effect of short term responsive VNS therapy on sleep quality using automatic sleep staging. IEEE Trans. Biomed. Eng. 2019, 66, 3301–3309. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, H.; Van Gompel, J.J.; Marsh, R.M.; Wharen, R.E.; Zimmerman, R.S.; Burkholder, D.B.; Lundstrom, B.N.; Britton, J.W.; Meyer, F.B. Outcomes following surgical management of vagus nerve stimulator–related infection: A retrospective multi-institutional study. J. Neurosurg. 2021, 135, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.L., 3rd; Mueller, W.M. Long-term treatment with vagus nerve stimulation in patients with refractory epilepsy. The Vagus Nerve Stimulation Study Group E01–E05. Neurology 1999, 53, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Ben-Menachem, E.; French, J.A. VNS Therapy versus the latest antiepileptic drug. Epileptic Disord. 2005, 7 (Suppl. 1), 522–526. [Google Scholar]
- Orosz, I.; McCormick, D.; Zamponi, N.; Varadkar, S.; Feucht, M.; Parain, D.; Griens, R.; Vallee, L.; Boon, P.; Rittey, P.; et al. Vagus nerve stimulation for drug-resistant epilepsy: A European long-term study up to 24 months in 347 children. Epilepsia 2014, 55, 1576–1584. [Google Scholar] [CrossRef]
- Crino, P.B.; Nathanson, K.L.; Henske, E.P. The tuberous sclerosis complex. N. Engl. J. Med. 2006, 355, 1345–1356. [Google Scholar] [CrossRef]
- Major, P.; Thiele, E.A. Vagus nerve stimulation for intractable epilepsy in tuberous sclerosis complex. Epilepsy Behav. 2008, 13, 357–360. [Google Scholar] [CrossRef]
- Parain, D.; Penniello, M.J.; Berquen, P.; Delangre, T.; Billard, C.; Murphy, J.V. Vagal nerve stimulation in tuberous sclerosis complex patients. Pediatr. Neurol. 2001, 25, 213–216. [Google Scholar] [CrossRef]
- Goldsmith, I.L.; Zupanc, M.L.; Buchhalter, J.R. Long-term seizure outcome in 74 patients with Lennox-Gastaut syndrome: Effects of incorporating MRI head imaging in defining the cryptogenic subgroup. Epilepsia 2000, 41, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Karceski, S. Vagus nerve stimulation and Lennox-Gastaut syndrome: A review of the literature and data from the VNS patient registry. CNS Spectr. 2001, 6, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Dibué, M.; Greco, T.; Spoor, J.K.H.; Tahir, Z.; Specchio, N.; Hänggi, D.; Steiger, H.J.; Kamp, M.A. Vagus nerve stimulation in patients with Lennox-Gastaut syndrome: A meta-analysis. Acta Neurol. Scand. 2021, 143, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Dravet, C. The core Dravet syndrome phenotype. Epilepsia 2011, 52 (Suppl. 2), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Dravet, C. Severe myoclonic epilepsy in infants and its related syndromes. Epilepsia 2000, 41 (Suppl. 9), 7. [Google Scholar] [CrossRef]
- Youn, S.E.; Jung, D.E.; Kang, H.C.; Kim, H.D. Long-term results of vagus nerve stimulation in children with Dravet syndrome: Time-dependent, delayed antiepileptic effect. Epilepsy Res. 2021, 174, 106665. [Google Scholar] [CrossRef] [PubMed]
- Dibué-Adjei, M.; Fischer, I.; Steiger, H.J.; Kamp, M.A. Efficacy of adjunctive vagus nerve stimulation in patients with Dravet syndrome: A meta-analysis of 68 patients. Seizure 2017, 50, 147–152. [Google Scholar] [CrossRef]
- Meins, M.; Lehmann, J.; Gerresheim, F.; Herchenbach, J.; Hagedorn, M.; Hameister, K.; Epplen, J.T. Submicroscopic duplication in Xq28 causes increased expression of the MECP2 gene in a boy with severe mental retardation and features of Rett syndrome. J. Med. Genet. 2005, 42, e12. [Google Scholar] [CrossRef]
- Vignoli, A.; Borgatti, R.; Peron, A.; Zucca, C.; Ballarati, L.; Bonaglia, C.; Bellini, M.; Giordano, L.; Romaniello, R.; Bedeschi, M.F.; et al. Electroclinical pattern in MECP2 duplication syndrome: Eight new reported cases and review of literature. Epilepsia 2012, 53, 1146–1155. [Google Scholar] [CrossRef]
- Wilfong, A.A.; Schultz, R.J. Vagus nerve stimulation for treatment of epilepsy in Rett syndrome. Dev. Med. Child. Neurol. 2006, 48, 683–686. [Google Scholar] [CrossRef]
- Morrison-Levy, N.; Go, C.; Ochi, A.; Otsubo, H.; Drake, J.; Rutka, J.; Weiss, S. Children with autism spectrum disorders and drug-resistant epilepsy can benefit from epilepsy surgery. Epilepsy Behav. 2018, 85, 200–204. [Google Scholar] [CrossRef]
- Cersósimo, R.O.; Bartuluchi, M.; De Los Santos, C.; Bonvehi, I.; Pomata, H.; Caraballo, R.H. Vagus nerve stimulation: Effectiveness and tolerability in patients with epileptic encephalopathies. Childs Nerv. Syst. 2011, 27, 787–792. [Google Scholar] [CrossRef]
- Wirrell, E.C.; Hood, V.; Knupp, K.G.; Meskis, M.A.; Nabbout, R.; Scheffer, I.E.; Wilmshurst, J.; Sullvan, J. International consensus on diagnosis and management of Dravet syndrome. Epilepsia 2022, 63, 1761–1777. [Google Scholar] [CrossRef]
- Babajani-Feremi, A.; Noorizadeh, N.; Mudigoudar, B.; Wheless, J.W. Predicting seizure outcome of vagus nerve stimulation using MEG-based network topology. Neuroimage Clin. 2018, 19, 990–999. [Google Scholar] [CrossRef]
- Ibrahim, G.M.; Sharma, P.; Hyslop, A.; Guillen, M.R.; Morgan, B.R.; Wong, S.; Abei, T.J.; Elkaim, T.J.; Cajigas, I.; Shah, A.H. Presurgical thalamocortical connectivity is associated with response to vagus nerve stimulation in children with intractable epilepsy. Neuroimage Clin. 2017, 16, 634–642. [Google Scholar] [CrossRef]
- Ravan, M. Investigating the correlation between short-term effectiveness of VNS Therapy in reducing the severity of seizures and long-term responsiveness. Epilepsy Res. 2017, 133, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Bayasgalan, B.; Matsuhashi, M.; Fumuro, T.; Nohira, H.; Nakano, N.; Iida, K.; Katagiri, M.; Shimotake, A.; Matsumoto, R.; Kikuchi, T.; et al. We could predict good responders to vagus nerve stimulation: A surrogate marker by slow cortical potential shift. Clin. Neurophysiol. 2017, 128, 1583–1598. [Google Scholar] [CrossRef]
- Hilderink, J.; Tjepkema-Cloostermans, M.C.; Geertsema, A.; Glastra-Zwiers, J.; De vos, C.C. Predicting success of vagus nerve stimulation (VNS) from EEG symmetry. Seizure 2017, 48, 69–73. [Google Scholar] [CrossRef]
- Kavčič, A.; Kajdič, N.; Rener-Primec, Z.; Krajnc, N.; Žgur, T. Efficacy and tolerability of vagus nerve stimulation therapy (VNS) in Slovenian epilepsy patients: Younger age and shorter duration of epilepsy might result in better outcome. Acta Clin. Croa 2019, 58, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Xu, C.; Zhang, X.; Qiao, L.; Wang, X.; Zhang., X.; Yan., X.; Ni, D.; Yu., T.; Zhang, G.; et al. Epilepsy duration as an independent predictor of response to vagus nerve stimulation. Epilepsy Res. 2020, 167, 106432. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Underlying Disease | Typical Age of Epilepsy Onset | 50% Responder Rate |
|---|---|---|
| Tuberous sclerosis | <1 year old [31] (1 year old on average) | 50–90% [32,33] |
| Lennox–Gastaut syndrome | Median age 4 years [34] | 50–65% [34,35,36] |
| Dravet syndrome | <1 year old [37,38] | 36–63% [39,40] |
| Rett syndrome (MECP2 genetic mutation) | 6–18 months old [41,42] | 86% [43] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukuda, M.; Matsuo, T.; Fujimoto, S.; Kashii, H.; Hoshino, A.; Ishiyama, A.; Kumada, S. Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy in Children—A Literature Review. J. Clin. Med. 2024, 13, 780. https://doi.org/10.3390/jcm13030780
Fukuda M, Matsuo T, Fujimoto S, Kashii H, Hoshino A, Ishiyama A, Kumada S. Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy in Children—A Literature Review. Journal of Clinical Medicine. 2024; 13(3):780. https://doi.org/10.3390/jcm13030780
Chicago/Turabian StyleFukuda, Mitsumasa, Takeshi Matsuo, So Fujimoto, Hirofumi Kashii, Ai Hoshino, Akihiko Ishiyama, and Satoko Kumada. 2024. "Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy in Children—A Literature Review" Journal of Clinical Medicine 13, no. 3: 780. https://doi.org/10.3390/jcm13030780
APA StyleFukuda, M., Matsuo, T., Fujimoto, S., Kashii, H., Hoshino, A., Ishiyama, A., & Kumada, S. (2024). Vagus Nerve Stimulation Therapy for Drug-Resistant Epilepsy in Children—A Literature Review. Journal of Clinical Medicine, 13(3), 780. https://doi.org/10.3390/jcm13030780