
Left Atrial Functional and Structural Characteristics in Patients After Total and Bicaval Orthotopic Heart Transplantation

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
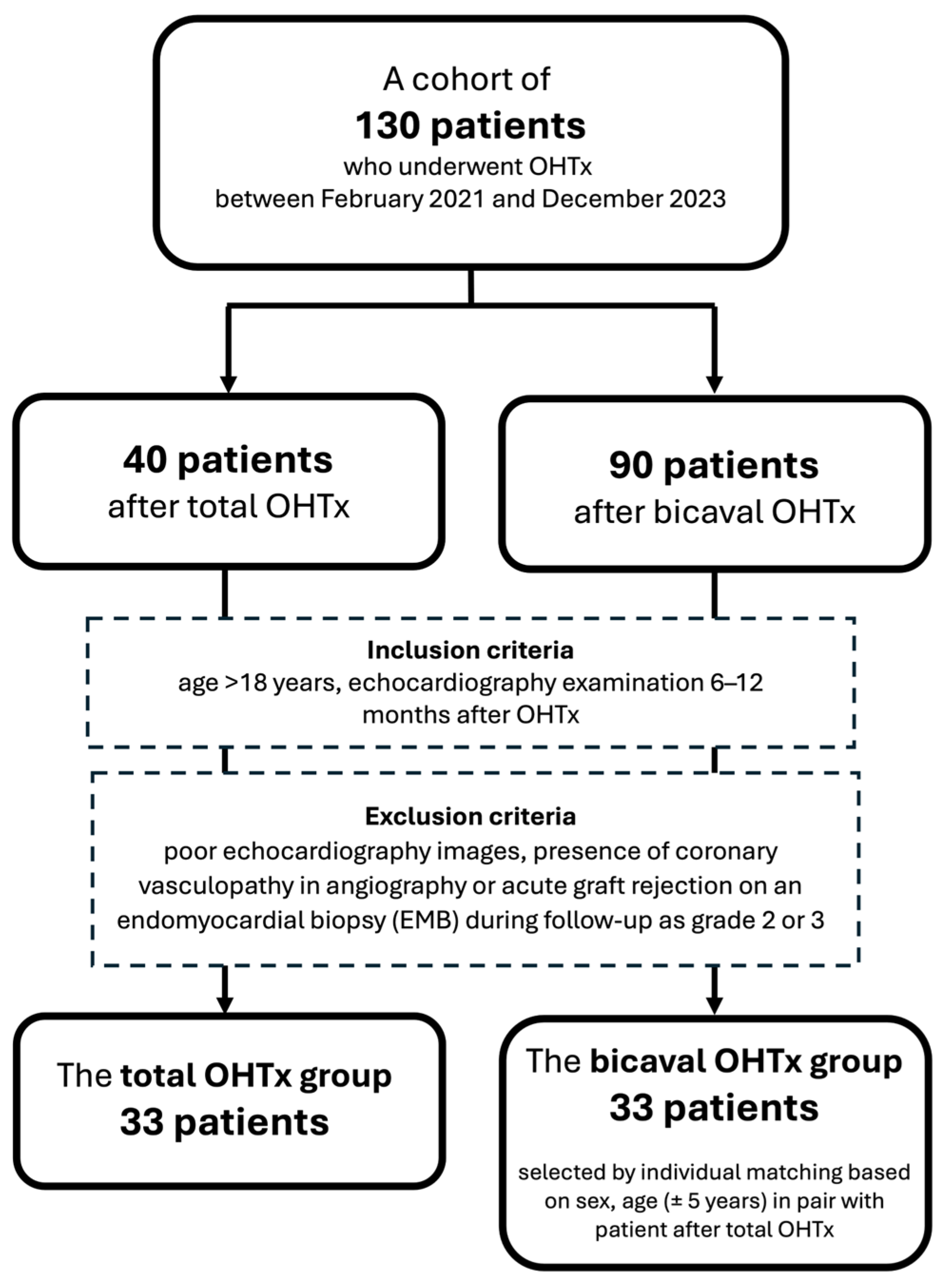
2.1. Patients and Study Design
2.2. Echocardiography Examination
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Echocardiographic Characteristics
3.3. Independent Determinants of LA Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| eGFR | estimated glomerular filtration rate |
| EMB | endomyocardial biopsy |
| GLS | global longitudinal strain |
| LA | left atrium |
| LAVI | left atrial volume index |
| LV | left ventricle |
| OHTx | orthotopic heart transplantation |
| RA | right atrium |
| PACS | peak atrial contraction strain |
| PALS | peak atrial longitudinal strain |
References
- Sievers, H.H.; Weyand, M.; Kraatz, E.G.; Bernhard, A. An alternative technique for orthotopic cardiac transplantation, with preservation of the normal anatomy of the right atrium. Thorac. Cardiovasc. Surg. 1991, 39, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus, G.; Jebara, V.; Mihaileanu, S.; Carpentier, A.F. Total orthotopic heart transplantation: An alternative to the standard technique. Ann. Thorac. Surg. 1991, 52, 1181–1184. [Google Scholar] [CrossRef] [PubMed]
- Pavri, B.B.; O‘Nunain, S.S.; Newell, J.B.; Ruskin, J.N.; William, G. Prevalence and prognostic significance of atrial arrhythmias after orthotopic cardiac transplantation. J. Am. Coll. Cardiol. 1995, 25, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Riberi, A.; Ambrosi, P.; Habib, G.; Kreitmann, B.; Yao, J.G.; Gaudart, J.; Ghez, O.; Metras, D. Systemic embolism: A serious complication after cardiac transplantation avoidable by bicaval technique. Eur. J. Cardiothorac. Surg. 2001, 19, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.A.; Edwards, N.M. Orthotopic cardiac transplantation: Comparison of outcome using biatrial, bicaval, and total techniques. J. Card. Surg. 2005, 20, 102–106. [Google Scholar] [CrossRef]
- Weiss, E.S.; Nwakanma, L.U.; Russell, S.B.; Conte, J.V.; Shah, A.S. Outcomes in bicaval versus biatrial techniques in heart transplantation: An analysis of the UNOS database. J. Heart Lung Transplant 2008, 27, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Schnoor, M.; Schäfer, T.; Lühmann, D.; Sievers, H.H. Bicaval versus standard technique in orthotopic heart transplantation: A sytematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2007, 134, 1322–1331. [Google Scholar] [CrossRef]
- Zijderhand, C.F.; Veen, K.M.; Caliskan, K.; Schoonen, T.; Mokhles, M.M.; Bekkers, J.A.; Manintveld, O.C.; Constantinescu, A.A.; Brugts, J.J.; Bogers, A.J.; et al. Biatrial Versus Bicaval Orthotopic Heart Transplantation: A Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2020, 110, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Ferretto, S.; Giuliani, I.; Sanavia, T.; Bottio, T.; Fraiese, A.P.; Gambino, A.; Tarzia, V.; Toscano, G.; Iliceto, S.; Gerosa, G.; et al. Atrial fibrillation after orthotopic heart transplantatation: Pathophysiology and clinical impact. Int. J. Cardiol. Heart Vasc. 2021, 32, 100710. [Google Scholar] [CrossRef]
- Rivinius, R.; Helmschrott, M.; Ruhparwar, A.; Erbel, C.; A Gleissner, C.; Darche, F.F.; Thomas, D.; Bruckner, T.; A Katus, H.; O Doesch, A. The influence of surgical technique on early posttransplant atrial fibrillation—Comparison of biatrial, bicaval, and total orthotopic heart transplantation. Ther. Clin. Risk Manag. 2017, 13, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Przewłocka-Kosmala, M.; Jasic-Szpak, E.; Rojek, A.; Kabaj, M.; E Sharman, J.; Kosmala, W. Association of central blood pressure with left atrial structural and functional abnormalities in hypertensive patients: Implications for atrial fibrillation prevention. Eur. J. Prev. Cardiol. 2019, 26, 1018–1027. [Google Scholar] [CrossRef]
- Jasic-Szpak, E.; Marwick, T.H.; Donal, E.; Przewlocka-Kosmala, M.; Huynh, Q.; Gozdzik, A.; Woznicka, A.K.; Jankowska, E.A.; Ponikowski, P.; Kosmala, W. Prediction of AF in heart failure with preserved ejection fraction: Incremental value of left atrial strain. JACC Cardiovasc. Imaging 2021, 14, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Kosmala, W.; Saito, M.; Kaye, G.; Negishi, K.; Linker, N.; Gammage, M.; Marwick, T.H. Protect-Pace Investigators. Incremental value of left atrial structural and functional characteristics for prediction of atrial fibrillation in patients receiving cardiac pacing. Circ. Cardiovasc. Imaging 2015, 8, e002942. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.I.; Bhattacharyya, A.; Ray, S.G. Echocardiography after cardiac transplantation. J. Am. Soc. Echocardiogr. 2002, 15, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, A.M.; Mastrobuoni, S.; Bastarrika, G.; Praschker, B.L.; Agüero, P.A.; Castaño, S.; Herreros, J.; Rabago, G. Bicaval versus standard technique in orthotopic heart transplant: Assessment of atrial performance at magnetic resonance and transthoracic echocardiography. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 457–462. [Google Scholar] [CrossRef]
- Ingvarsson, A.; Evaldsson, A.W.; Waktare, J.; Nilsson, J.; Smith, G.J.; Stagmo, M.; Roijer, A.; Rådegran, G.; Meurling, C.J. Normal Reference Ranges for Transthoracic Echocardiography Following Heart Transplantation. J. Am. Soc. Echocardiogr. 2018, 31, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Velleca, A.; A Shullo, M.; Dhital, K.; Azeka, E.; Colvin, M.; DePasquale, E.; Farrero, M.; García-Guereta, L.; Jamero, G.; Khush, K.; et al. The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2023, 42, e1–e141. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Baron, R.; Kenny, D. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 5, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Xie, Y.; Qiao, W.; Tian, F.; Sun, W.; Wang, Y.; Wu, C.; Li, H.; Yi, L.; Zhong, Y.; et al. Impaired left atrial function in clinically well heart transplant patients. Int. J. Cardiovasc. Imaging 2021, 37, 1937–1945. [Google Scholar] [CrossRef] [PubMed]
- Markowicz, E.; Duszańska, A.; Przybylski, R.; Szulik, M.; Streb, W.; Zembala, M.; Kalarus, Z.; Kukulski, T. Does the method of heart transplantation affect left ventricular filling? Kardiol. Pol. 2012, 70, 769–773. [Google Scholar]
- Gan, G.C.; Bhat, A.; Chen, H.H.; Fernandez, F.; Byth, K.; Eshoo, S.; Thomas, L. Determinants of LA reservoir strain: Independent effects of LA volume and LV global longitudinal strain. Echocardiography 2020, 37, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.R.; Sampaio, F.; Braga, J.; Ribeiro, J. Fontes-Carvalho R Left atrial strain evaluation to assess left ventricle diastolic dysfunction and heart failure with preserved ejection fraction: A guide to clinical practice: Left atrial strain and diastolic function. Int. J. Cardiovasc. Imaging 2023, 39, 1083–1096. [Google Scholar] [CrossRef]
- Barbier, P.; Solomon, S.B.; Schiller, N.B.; Glantz, S.A. Left atrial relaxation and left ventricular systolic function determine left atrial reservoir function. Circulation 1999, 100, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Hoit, B.D. Left atrial size and function: Role in prognosis. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef]
- Morris, D.A.; Belyavskiy, E.; Aravind-Kumar, R.; Kropf, M.; Frydas, A.; Braunauer, K.; Marquez, E.; Krisper, M.; Lindhorst, R.; Osmanoglou, E.; et al. Potential Usefulness and Clinical Relevance of Adding Left Atrial Strain to Left Atrial Volume Index in the Detection of Left Ventricular Diastolic Dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1405–1415. [Google Scholar] [CrossRef]
- Thomas, L.; Marwick, T.H.; Popescu, B.A.; Donal, E.; Badano, L.P. Left Atrial Structure and Function, and Left Ventricular Diastolic Dysfunction: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1961–1977. [Google Scholar] [CrossRef]
- Frydas, A.; Morris, D.A.; Belyavskiy, E.; Radhakrishnan, A.; Kropf, M.; Tadic, M.; Roessig, L.; Lam, C.S.; Shah, S.J.; Solomon, S.D.; et al. Left atrial strain as sensitive marker of left ventricular diastolic dysfunction in heart failure. ESC Heart Fail. 2020, 7, 1956–1965. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, C.; Rossi, A.; Cannata, L.; Zocco, C.; Belyavskiy, E.; Radhakrishnan, A.K.; Feuerstein, A.; Morris, D.A.; Pieske-Kraigher, E.; Pieske, B.; et al. Left atrial strain predicts exercise capacity in heart failure independently of left ventricular ejection fraction. ESC Heart Fail. 2022, 9, 842–852. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Khan, S.U. Left Atrial Strain for Assessment of Left Ventricular Diastolic Function: Focus on Populations with Normal LVEF. JACC Cardiovasc. Imaging 2023, 16, 691–707. [Google Scholar] [CrossRef]
- Sciaccaluga, C.; Fusi, C.; Landra, F.; Barilli, M.; Lisi, M.; Mandoli, G.E.; D’ascenzi, F.; Focardi, M.; Valente, S.; Cameli, M. Diastolic function in heart transplant: From physiology to echocardiographic assessment and prognosis. Front. Cardiovasc. Med. 2022, 9, 969270. [Google Scholar] [CrossRef]
- Bech-Hanssen, O.; Pergola, V.; Al-Admawi, M.; Fadel, B.M.; Di Salvo, G. function in heart transplant recipients operated with the bicaval technique. Scand. Cardiovasc. J. 2016, 50, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Telles, F.; Nanayakkara, S.; Evans, S.; Patel, H.C.; Mariani, J.A.; Vizi, D.; William, J.; Marwick, T.H.; Kaye, D.M. Impaired left atrial strain predicts abnormal exercise haemodynamics in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2019, 21, 495–505. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bicaval OHTx | Total OHTx | p-Value | |
|---|---|---|---|
| N = 33 | N = 33 | ||
| Age, years (SD) | 51.4 (10.5) | 51.0 (10.9) | 0.89 |
| Women, % | 15 | 15 | |
| BMI, kg∙m−2 (SD) | 26.7 (3.8) | 25.2 (3.8) | 0.15 |
| Heart rate, bpm (SD) | 88 (9) | 89 (10) | 0.79 |
| NT-proBNP, pg∙mL−1 (IQR) | 602 (317–1245) | 1137 (306–2026) | 0.50 |
| Troponin, (μg∙L−1) (IQR) | 7.33 (3.13–14.96) | 8.90 (4.13–12.94) | 0.54 |
| Hemoglobin, g∙dL−1 (SD) | 12.9 (1.5) | 12.4 (1.7) | 0.31 |
| CRP, mg∙L−1 (IQR) | 2.7 (1.2–11.5) | 5.7 (1.6–21.9) | 0.32 |
| Creatinine, mg∙dL−1 (SD) | 1.18 (0.39) | 1.24 (0.41) | 0.51 |
| eGFR, mL∙min−1∙1.73 m−2 (SD) | 75.1 (22.5) | 68.2 (23.7) | 0.36 |
| Age of donor, years (SD) | 41 (13) | 42 (11) | 0.81 |
| Cold ischemic time, min (SD) | 115 (52) | 132 (55) | 0.29 |
| Hypertension (%) | 48% | 33% | 0.29 |
| Diabetes mellitus (%) | 28% | 13% | 0.20 |
| Preoperative mean PAP, mmHg (SD) | 29.3 (10.4) | 27.6 (10.5) | 0.62 |
| BB (%) | 30% | 23% | 0.74 |
| ACEI or ARB (%) | 42% | 30% | 0.44 |
| CB (%) | 36% | 33% | 0.79 |
| Bicaval OHTx | Total OHTx | p-Value | |
|---|---|---|---|
| N = 33 | N = 33 | ||
| LVDd, mm (SD) | 48 (8) | 46 (8) | 0.34 |
| IVDd, mm (SD) | 12 (2) | 12 (1) | 0.59 |
| PWDd, mm (SD) | 11 (1) | 10 (1) | 0.52 |
| LV EF, % (SD) | 59 (5) | 58 (5) | 0.91 |
| LV GLS, % (SD) | 15.6 (3.0) | 16.6 (2.2) | 0.12 |
| CO, L∙min−1 (SD) | 48 (1.1) | 4.2 (1.4) | 0.23 |
| E, cm∙s−1 (SD) | 76 (18) | 65 (15) | 0.08 |
| A, cm∙s−1 (SD) | 48 (14) | 65 (19) | <0.001 |
| DT, ms (SD) | 148 (29) | 156 (44) | 0.26 |
| E/A (SD) | 1.7 (0.5) | 1.1 (0.4) | <0.001 |
| e’ lateral, cm∙s−1 (SD) | 13.0 (3.1) | 12.0 (3.4) | 0.24 |
| e’ septal, cm∙s−1 (SD) | 7.8 (2.1) | 7.4 (1.5) | 0.35 |
| E/e’ (SD) | 7.3 (2.2) | 7.0 (3.1) | 0.54 |
| LAVI, mL∙m−2 (SD) | 37.9 (7.1) | 28.6 (4.8) | <0.001 |
| LA emptying fraction, % (SD) | 50.4 (6.5) | 60.8 (6) | <0.001 |
| PALS, % (SD) | 17.4 (4.7) | 26.5 (6.9) | <0.001 |
| PACS, % (SD) | 6.0 (4.5) | 14.8 (5.8) | <0.001 |
| LA stiffness index (SD) | 0.44 (0.19) | 0.26 (0.24) | <0.001 |
| TR velocity, m∙s−1 (SD) | 2.2 (0.4) | 2.3 (0.4) | 0.46 |
| TAPSE, mm (SD) | 17 (2) | 17 (2) | 0.96 |
| RAa, cm2 (SD) | 15.0 (1) | 15.0 (1.5) | 0.98 |
| PALS | PACS | LAVI | ||||
|---|---|---|---|---|---|---|
| R | p | R | p | R | p | |
| BMI | −0.36 | <0.001 | −0.34 | 0.04 | 0.24 | 0.16 |
| Hypertension | −0.45 | 0.008 | −0.54 | 0.001 | 0.39 | 0.02 |
| Diabetes mellitus | −0.48 | 0.004 | −0.48 | 0.004 | 0.36 | 0.03 |
| Age of donor | −0.05 | 0.79 | 0.09 | 0.62 | 0.04 | 0.81 |
| Cold ischemia time | 0.23 | 0.19 | 0.17 | 0.34 | −0.23 | 0.20 |
| Total OHTx technique | 0.69 | <0.001 | 0.82 | <0.001 | −0.81 | <0.001 |
| LAVI | −0.52 | 0.002 | −0.62 | <0.001 | ||
| LV GLS | 0.39 | 0.02 | 0.33 | 0.05 | −0.16 | 0.37 |
| Model for PALS R2 = 0.53 | Model for PACS R2 = 0.58 | Model for LAVI R2 = 0.43 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | P | β | SE | p | β | SE | p | |
| Total OHTx technique | 0.50 | 0.10 | <0.001 | 0.66 | 0.09 | <0.001 | −0.56 | 0.11 | <0.001 |
| LV GLS | 0.22 | 0.10 | 0.025 | 0.02 | 0.09 | 0.84 | 0.03 | 0.11 | 0.76 |
| BMI | −0.10 | 0.10 | 0.32 | −0.07 | 0.09 | 0.46 | 0.04 | 0.11 | 0.73 |
| Diabetes mellitus | −0.24 | 0.11 | 0.026 | −0.19 | 0.10 | 0.08 | 0.12 | 0.11 | 0.29 |
| Hypertension | −0.03 | 0.11 | 0.78 | −0.12 | 0.10 | 0.24 | 0.13 | 0.12 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obremska, M.; Przybylski, R.; Sokolski, M.; Przewłocka-Kosmala, M.; Rakowski, M.; Ptak, J.; Sareło, P.; Zakliczyński, M.; Kosmala, W. Left Atrial Functional and Structural Characteristics in Patients After Total and Bicaval Orthotopic Heart Transplantation. J. Clin. Med. 2024, 13, 7643. https://doi.org/10.3390/jcm13247643
Obremska M, Przybylski R, Sokolski M, Przewłocka-Kosmala M, Rakowski M, Ptak J, Sareło P, Zakliczyński M, Kosmala W. Left Atrial Functional and Structural Characteristics in Patients After Total and Bicaval Orthotopic Heart Transplantation. Journal of Clinical Medicine. 2024; 13(24):7643. https://doi.org/10.3390/jcm13247643
Chicago/Turabian StyleObremska, Marta, Roman Przybylski, Mateusz Sokolski, Monika Przewłocka-Kosmala, Mateusz Rakowski, Jakub Ptak, Przemysław Sareło, Michał Zakliczyński, and Wojciech Kosmala. 2024. "Left Atrial Functional and Structural Characteristics in Patients After Total and Bicaval Orthotopic Heart Transplantation" Journal of Clinical Medicine 13, no. 24: 7643. https://doi.org/10.3390/jcm13247643
APA StyleObremska, M., Przybylski, R., Sokolski, M., Przewłocka-Kosmala, M., Rakowski, M., Ptak, J., Sareło, P., Zakliczyński, M., & Kosmala, W. (2024). Left Atrial Functional and Structural Characteristics in Patients After Total and Bicaval Orthotopic Heart Transplantation. Journal of Clinical Medicine, 13(24), 7643. https://doi.org/10.3390/jcm13247643