1. Introduction
According to reports from the World Health Organization (WHO), in March 2023, an estimated 1.28 billion adults aged 30–79 years worldwide had hypertension, with most (two-thirds) living in low- and middle-income countries. An estimated 46% of adults with hypertension are unaware that they have the condition, less than half of adults (42%) with hypertension are diagnosed and treated, and approximately one in five adults (21%) have it under control. Hypertension is a major cause of premature death worldwide and is a major risk factor for stroke, myocardial infarction, vascular disease, and chronic kidney disease. Dyslipidemia results in abnormal levels of lipids in the blood that can also increase the risk of cardiovascular diseases [
1]. Dyslipidemia is classified into two types: primary and secondary. Primary dyslipidemia is inherited and caused by genetic mutations that affect lipid metabolism, while secondary dyslipidemia is acquired and caused by lifestyle factors or other medical conditions that alter lipid levels. Both types are associated with hypertension. The management of dyslipidemias is an essential and integral part of cardiovascular disease prevention [
2].
Chronic high blood pressure or previous episodes of high blood pressure can affect retinal microcirculatory structure and function [
3].
There have been many previous studies on the association between hypertensive retinopathy and hypertension [
4,
5,
6,
7,
8,
9,
10].
The prevalence rate of retinopathy in patients with mild hypertension is approximately 25%, with the moderate form of the disease is 34%, and with the severe form is 84.6%. Of the patients with hypertensive retinopathy, 42.3% have a grade I, 20% a grade II, and 2.35% a grade III ocular pathology [
5].
Hypertensive retinopathy is related to blood pressure variability (BPV); the degree of BPV and retinopathy in hypertensive patients can be used to track the progression of hypertension-mediated organ damage (HOMD), and the correction of BPV may help treat or postpone the progression of HOMD. Hypertension is associated with reduced retinal vessel density and an increased foveal avascular zone (FAZ), especially in the deep venous plexus, as seen on optical coherence tomography angiography (OCTA) [
11].
Patients with hypertensive retinopathy show a reduction in the retinal vascular density, superficial and deep vascular plexus (SVP and DVP), ganglion cell–internal boundary membrane complex density (GCL-ILM), and retinal nerve fiber layer (RNFL) thickness [
12].
The classic retinal changes in chronic hypertensive retinopathy include arteriolar narrowing and tortuosity, arteriovenous crossing changes, retinal hemorrhages, cotton-wool spots, hard exudates, papilledema. The malignant stage of hypertensive retinopathy represents a medical emergency, often associated with markedly elevated blood pressure and with the risk of organ damage [
8,
13].
Compared to invasive fundus fluorescein angiography (FFA), OCTA is a new, rapid, easily performed, and non-invasive 3D imaging modality, allowing healthcare professionals to study the microvasculature of the retinal and choroidal layers in large populations of patients with dyslipidemia and hypertensive retinopathy [
14]. The retina and choroid are two distinct vascular beds. Using 3D OCTA, distinct visualizations of these two circulations can be obtained. In healthy eyes, retinal circulation is located between the internal limiting membrane (ILM) and the outer plexiform layer (OPL). The choroidal circulation is located beneath Bruch’s membrane (BM). The vitreous (anterior to the ILM) and outer retina (between OPL and Bruch’s membrane) are avascular structures [
14]. OCTA allows for quantitative assessment of the retinal microvasculature, providing metrics such as vessel density and vessel caliber. These measurements help in tracking hypertensive retinopathy progression in patients with dyslipidemia and assessing the efficacy of treatment interventions over time [
9,
15].
OCTA changes in hypertensive retinopathy include microvascular density reduction, focal capillary non-perfusion, increased FAZ, vascular tortuosity and irregularities, and choroidal thickness alterations [
3,
9,
15,
16,
17].
The aim of our current study was to measure FAZ, non-flow area (NFA), vascular flow area (VFA), retinal vascular density, and perfusion by using OCTA in patients with chronic hypertension and secondary dyslipidemia, identifying the potential OCTA parameters to be analyzed using A.I. We hypothesize that OCTA will show subclinical changes in retinal microvasculature in the superficial and deep plexi, i.e., changes related to secondary dyslipidemia and progression of hypertensive retinopathy.
2. Materials and Methods
2.1. Study Participants
The Ethics Committee approved the study in December 2022. Patients were selected for inclusion in this study by the ophthalmologist and referred to the ophthalmologist by a cardiologist, general practitioner, or internist.
We performed a prospective cohort study including 77 participants with dyslipidemia and systemic hypertension from Eastern Europe, Romania. From 2022 to 2024, 154 eyes were eligible for the final analysis presented in this study. All participants underwent ophthalmological examinations, blood testing, blood pressure monitoring, and body mass index (BMI) calculation according to protocol.
For the purpose of this study, we selected subjects diagnosed with chronic hypertension and secondary dyslipidemia (based on medical history and records) as well as undiagnosed cases by determining blood pressure, performing blood tests and fundoscopy, and by referring patients to a cardiologist and internist for an accurate diagnosis.
We selected hypertensive patients with consistently high values in all measurements, including patients using and not using antihypertensive treatments at the time of their first visit. Subjects with normalized blood pressure during follow-ups were not excluded from the study.
Patients with chronic hypertensive retinopathy were included in the study based on fundoscopic examination. We selected grade I–II of hypertensive retinopathy (mild) according to the Keith–Wagener–Barker or Mitchell–Wong classification system and no other types of retinopathy based on fundoscopy [
5,
18]. Patients with the following pathologies were excluded by using fundoscopy and by scanning the optic nerve and retina in both eyes using OCTA: hypertensive retinopathy grade III (moderate) and IV (severe) according to the Keith–Wagener–Barker or Mitchell–Wong classification system, glaucoma, diabetic retinopathy, maculopathy, central serous retinopathy, pigment epithelial detachments, epiretinal membranes, cystoid macula edema, vitreomacular traction, and other significant co-morbidities that could affect retinal vasculature.
In our study, we included participants with newly diagnosed dyslipidemia based on blood testing performed at the time of the first visit and diagnosed before referral by the internist or the cardiologist.
Systolic and diastolic blood pressure was measured twice per month. Blood pressure was taken with an automatic blood pressure monitor (Hartmann Tensoval Comfort, PAUL HARTMANN AG, 89522 Heidenheim, Germany). Three readings were taken 5 min apart, before exercise or at least 30 min after exercise. Hypertension was defined as present in participants with elevated blood pressure at the time of examination (SPB ≥ 130 mmHg or DBP ≥ 80 mmHg), according to American Heart Association criteria [
2,
16]. Undiagnosed cases were defined to be hypertensive if their systolic blood pressure was more than or equal to 140 mmHg or diastolic blood pressure more than or equal to 90 mmHg or if there was a self-reported history of self-measured blood pressure above the same values.
Height, body weight, and BMI were calculated every 3 months. Height was measured using a portable stadiometer (Seca Model 217; Seca, Hamburg, Germany). Body weight was determined using a calibrated mechanical column scale with eye-level beam (Seca 700; Seca, Hamburg, Germany). BMI was calculated by dividing body weight (kg) by the square of height (m2). The age and sex were also noted. Recording of the smoking habit was also performed. Smoking was assessed with the single categorized question: “Are you a current smoker?”.
Glycemia and HbA1c were determined in order to rule out subjects with diabetes and/or undiagnosed diabetic retinopathy. Glycemia, glycated hemoglobin (HbA1c), total cholesterol, HDL, LDL, and triglycerides were measured every 3 months using the same laboratory equipment. Non-fasting blood samples were used to assess plasma lipid profiles. Measurements were performed on all patients with or without statin use at the time of the enrollment. Patients with normalized plasma lipid values after receiving statin treatment during follow-ups were not excluded from the study.
Each participant underwent an ophthalmic examination including refraction measured with Auto Kerato-Refractometer (Topcon, Model KR-800, Tokyo, Japan) and determination of intraocular pressure with Goldmann Tonometer, fundoscopy, and OCTA. All refractive errors were included. All subjects had a normal intraocular pressure ranging from 10 to 21 mmHg. Examination of the retina using a Volk 90D and a 78D power lens (Volk, Mentor, OH, USA) was performed quarterly in order to stage hypertensive retinopathy and to include or exclude participants in our study.
OCTA was performed on both eyes, on all patients, every 3 months, with the assessment of FAZ, NFA, VFA, retinal vascular density, and perfusion on the OCTA. Eyes with poor-quality images or a poor signal strength were excluded.
2.2. Imaging Protocol
OCTA of the macula was performed using Angio-OCT Optopol Revo NX 130 (OPTOPOL Technology, Zawiercie, Poland) (Angiography module including a Retina Angiography 6 × 6 mm scan program and OCTA mosaic program to merge together 3 × 3 or 6 × 6 mm scans in order to create high-resolution mosaics of a larger area, iTracking™ technology, Motion Correction Technology™ and Projection Artefact Removal algorithm to minimize artifacts). The available vascular layers identified by the OCTA can be selected from the following list: retina, vitreous, superficial capillary plexus, superficial vascular plexus (SVC), radial peripapillary capillary plexus (RPCP), deep capillary plexus, deep vascular plexus (DVC), intermediate capillary plexus (ICP), outer retina layers, choriocapillaris, and choroidal vessels, with depth coded.
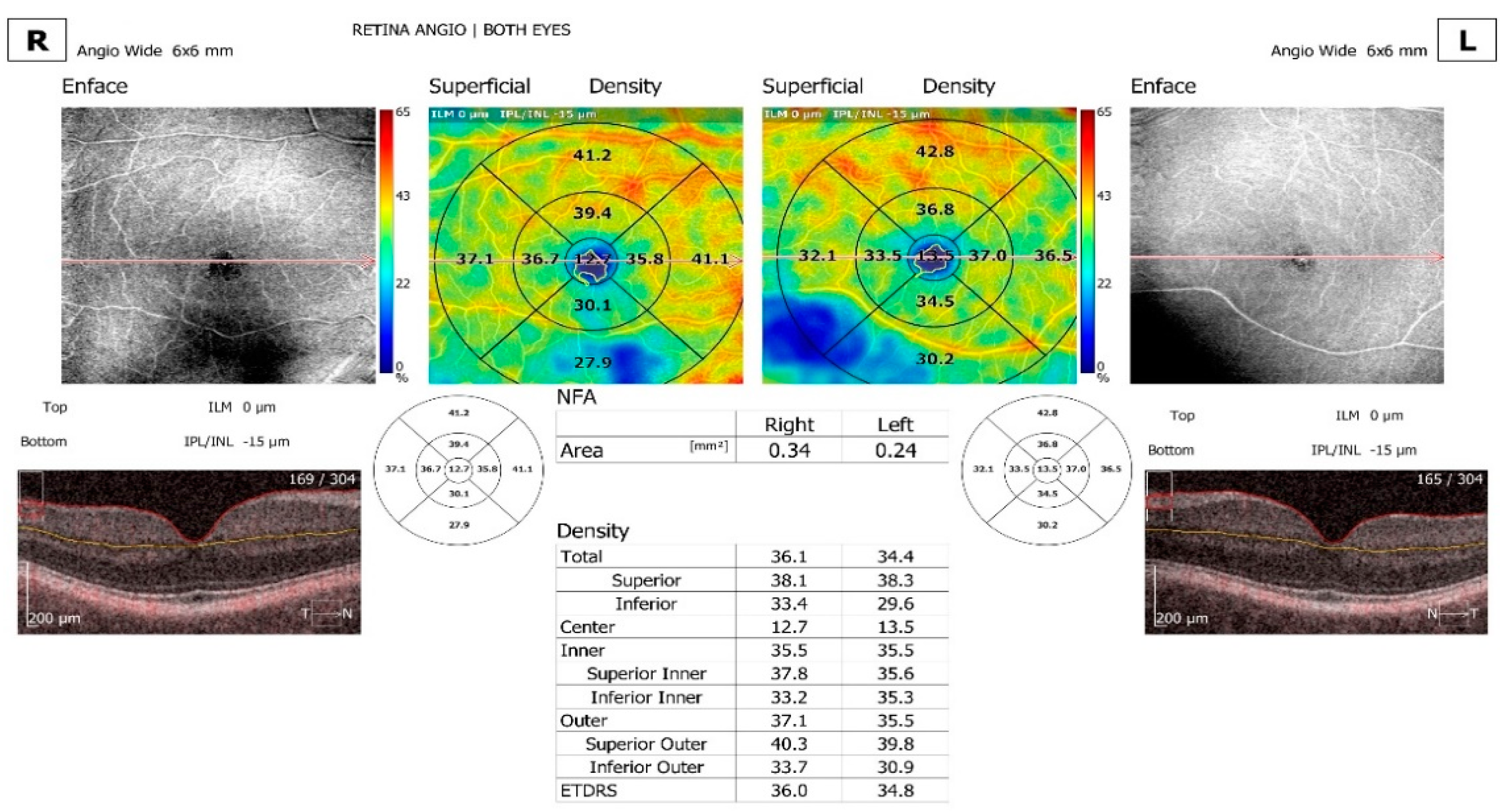
For the purpose of this study, 6.0 × 6.0 mm scans were performed, centered on the fovea of the right eye and left eye from each participant. The software (Version 11.0.4 REVO NX Device SN: 1560658/16) was used to analyze the superficial layer (with the offset of inner limiting membrane (ILM) 0 µm, inner plexiform layer/ inner nuclear layer (IPL/INL) 15 µm), the deep layer (with the offset of IPL/INL—15 µm, IPL/INL—70 µm), and the choriocapillaris (with the offset of Bruch’s membrane (BM) top BM 30 µm, bottom BM 45 µm).
The software was also used to assess the FAZ, NFA, VFA, and the retinal vascular density and skeleton. These parameters were derived from an En face angiogram. The FAZ, NFA, and VFA areas were detected and measured using the semi-auto area tool of the software. As the semi-automated measurement was noted to be inaccurate in a number of scans, manual measurements were performed. The calculated areas of the following parameters are provided: FAZ area in mm2, FAZ perimeter in mm, circularity (ratio between the measured perimeter and the perimeter of a circular area of the same size), NFA in mm2, VFA area in mm2, and VFA flow area in mm2. Quantification provided the quantification of vasculature in specific sectors and a heat map corresponding to the vasculature.
Density display is defined as the total area of perfused vasculature per unit area in a region of measurement. This metric is calculated by summing up the number of pixels that contain perfused vasculature and dividing the sum by the total number of pixels in the considered region. The result is an unitless number ranging from 0 (no perfusion) to 1 (fully perfused) (mm2/mm2).
Skeleton display is defined as the total area of skeletonized vasculature per unit area in a region of measurement. Skeletonization performs thinning of all vessels down to 1 pixel width and thus makes analysis more sensitive to small vasculature (as the large vessels lose more area than the thin ones in the skeletonization process). This metric is calculated by summing up the number of pixels that represent the skeleton of the vasculature and dividing the sum by the total number of pixels in the considered region. The result is an unitless number ranging from 0 (no perfusion) to 1 (mm2/mm2).
Both density and skeleton display can detect abnormal vasculature and provide repeatable quantitative results equally in normal and diseased eyes. Measurement zones for the available 6 mm width retina scans are total, superior, inferior, center, inner, superior inner, inferior inner, outer, superior outer, inferior outer, and the Early Treatment of Diabetic Retinopathy Study (ETDRS) grid.
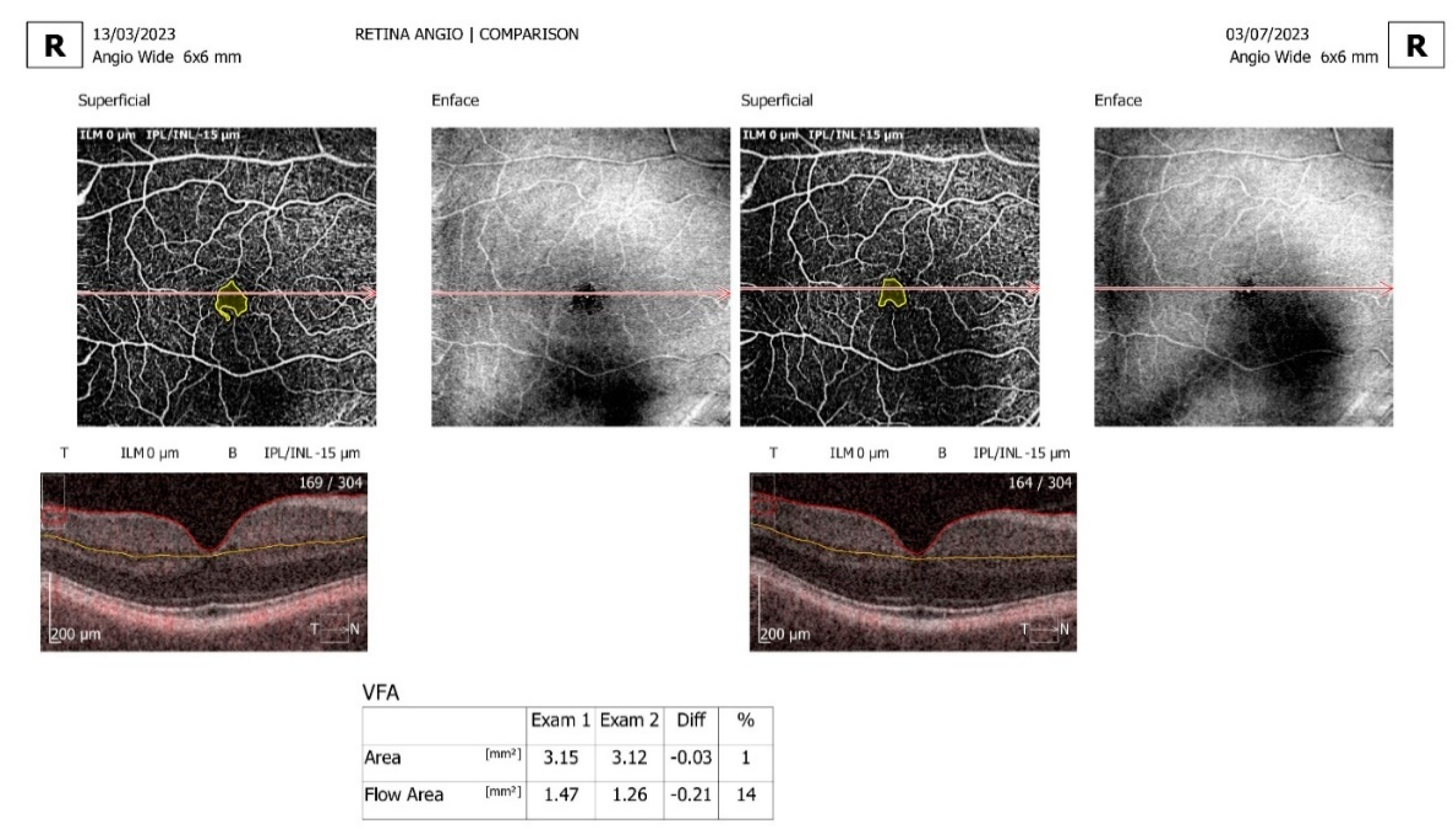
Comparison and progression view screens were used. The comparison view screen shows the analysis results, comparing two examinations of one eye on the same side in the same scan mode but from different dates. The comparison view is used to observe follow-up changes in the eye structure. The software automatically selects outermost examinations (the oldest and the newest) in order to compare them. The progression view screen shows the analysis results comparing four examinations, all performed on the same side in the same scan mode and on the same size of scanning area, arranged in a time sequence. Eyes with a significant artifact that obscured the vascular area of interest, with segmentation failure that could not be manually corrected, and with poor-quality images or a poor signal strength were excluded (
Figure 1,
Figure 2 and
Figure 3).
The current A.I. software was uploaded to the OCT machine.
The newest A.I. DeNoise™ technology improves tomogram quality powered by A.I. Advanced A.I. algorithms enhance the quality of a single tomogram to the level of an averaged tomogram obtained through multiple scans. The A.I. DeNoise™ algorithm filters out noise from the tomogram for the highest and smoothest image quality. The function is available on all tomograms. The moment a tomogram is loaded for review, the software starts denoising it. After a short moment, the original “undenoised” tomogram is replaced with a noise-free image obtaining a better visualization.
The A.I. Retina is a new layer segmentation for the posterior segment that is based on artificial intelligence, resulting in more accurate recognition of retinal layer boundaries.
The maximum intensity projection (MIP) algorithm provides better visualization of OCTA data for analysis. This MIP tool is useful for visualizing OCTA data, as it enables easier identification and tracking of high-intensity structures such as blood vessels.
The A.I. system has a direct impact on the accuracy of the clinical assessment and the assessment of the status of areas of pathology in the retina. This level of detection is more accurate and results in more detailed screening. Overall, it is a more effective way of running a pathology evaluation. A.I. segmentation is important for follow-up examinations, bringing a more accurate diagnosis when analyzing pathology over time.
2.3. Statistical Analysis
IBM Statistical Package for the Social Sciences (SPSS) V23, IBM SPSS Release 26.0.0.0, Minitab V16, JASP V 0.18.3, and Microsoft Office 2019 were used for statistical analysis.
The whole sample of 154 eyes was divided into two groups, with 77 subjects each: right eye and left eye, with each group subdivided into a hypercholesterolemia and hypertriglyceridemia group. Using descriptive statistics, the following indicators were calculated: mean, standard deviation (SD), mode, median, and 95% confidence intervals (CI). We analyzed age, sex, rural and urban areas, smoking habit, blood pressure (systolic and diastolic), cholesterol levels including total and HDL and LDL, triglycerides, BMI, glycemia, and HbA1c. For each group, the following parameters of the OCTA were determined for both eyes: FAZ area, FAZ perimeter, FAZ circularity, NFA area, VFA area, VFA flow area, density total, density ETDRS, skeleton total, and skeleton ETDRS.
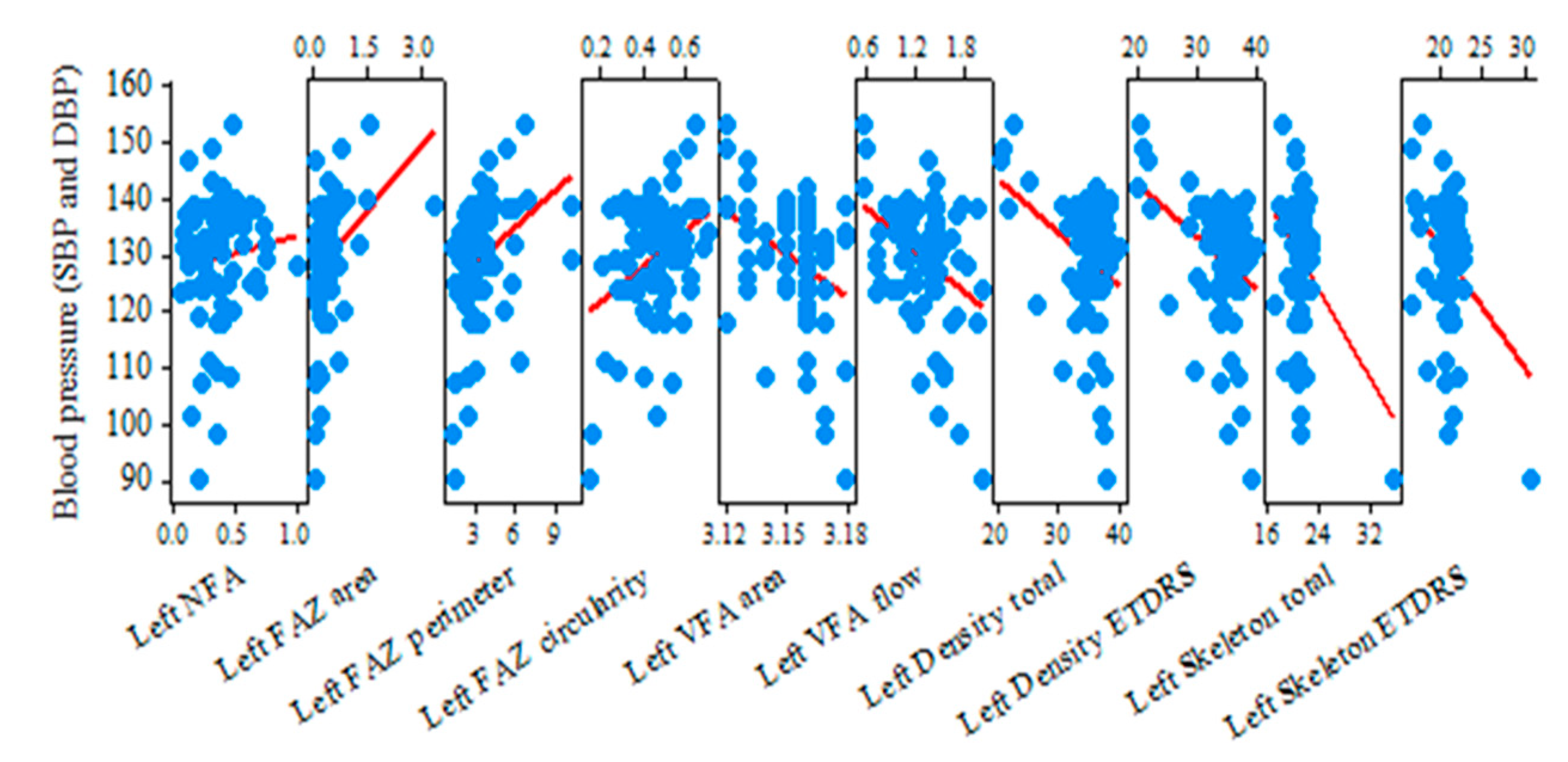
The correlation between the blood pressure and the OCTA parameters was calculated using Pearson Correlation and Sig. (2-tailed) p-value test. Correlations between blood pressure, total cholesterol, HDL, LDL, triglycerides, and OCTA parameters were determined using Pearson correlation coefficient (r) and two-tailed p-value. We divided subjects with dyslipidemia into two groups, namely a hypercholesterolemia group (we analyzed total cholesterol, HDL, and LDL) and hypertriglyceridemia group (we analyzed triglycerides), and we determined correlation with OCTA parameters for the right eye and left eye.
A dependent t-test was used to determine if there is a significant difference between OCTA parameters in the right eye and the left-eye group, analyzing t-value (t), p-value (p), and degrees of freedom (df).
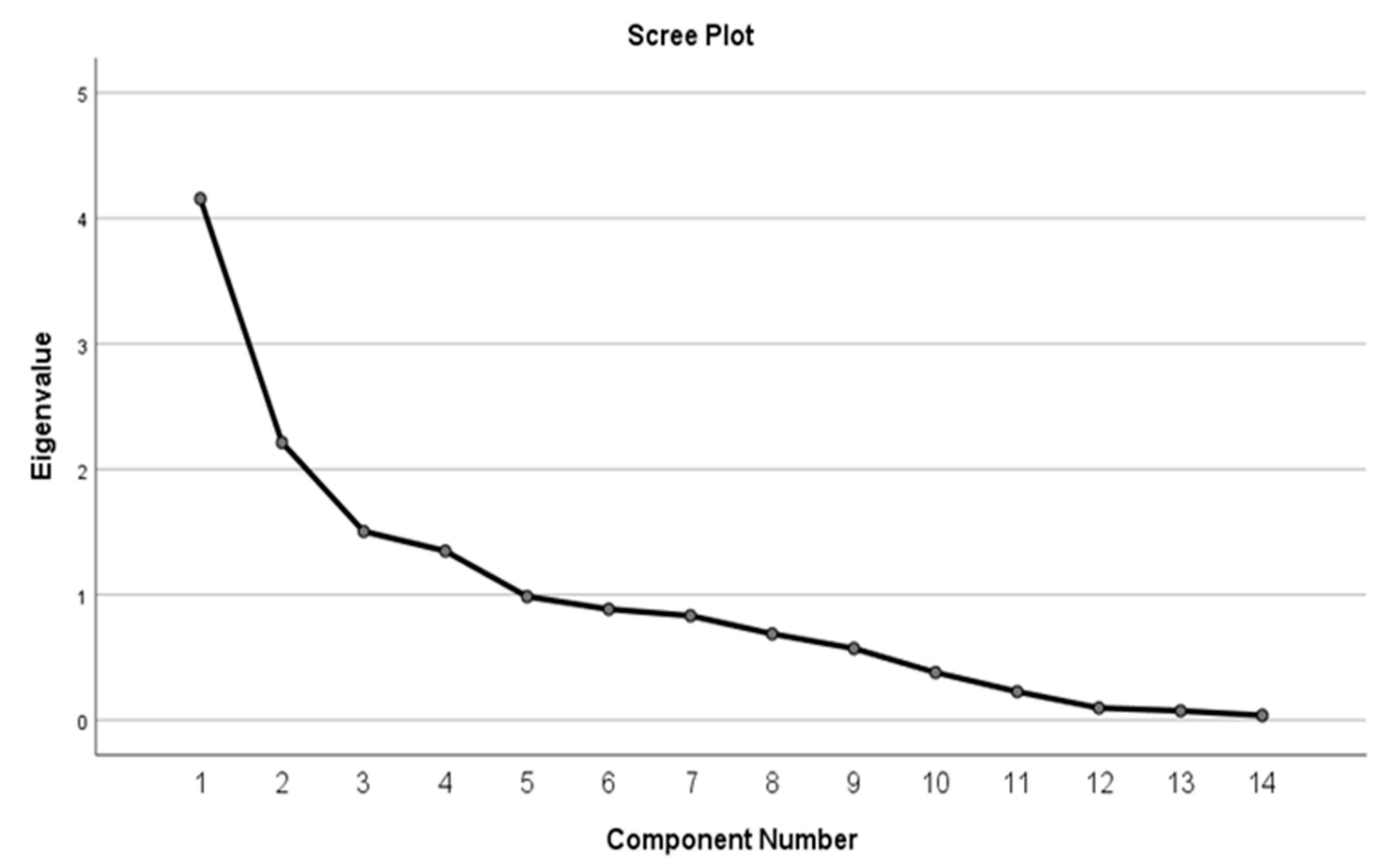
A multivariate analysis exploring how these factors interact collectively was performed. Factor analysis was performed using Principal component analysis of IBM SPSS Release 26.0.0.0. Kaiser–Meyer–Olkin test, Bartlett’s test, rotated component matrix, total variance explained, and scree plot were used.
4. Discussion
Hypertension is a very common condition worldwide and an important risk factor for cardiovascular and cerebrovascular events, renal diseases, and microvascular eye diseases [
6]. Established hypertension leads to the chronic vasoconstriction of small arteries, impairment of the organ flow reserve, and the progressive worsening of hypertensive disease.
One of the latest studies about hypertensive retinopathy was published by Lei Jiao, Chaoran Lv, and Hongling Zhang [
9]. This study concluded that hypertensive retinopathy is related to blood pressure variability (BPV), that the degree of BPV and retinopathy in hypertensive patients can be used to track the progression of hypertension-mediated organ damage (HOMD), and that the correction of BPV may help treat or postpone the progression of HOMD. Another study by Christopher Sun et al. showed that hypertension is associated with reduced retinal vessel density and an increased FAZ, especially in the deep venous plexus, as seen on OCTA [
11].
In 2022, Niro, A et al. demonstrated in their study that patients with hypertensive retinopathy show a reduction in the retinal vascular density, superficial and deep vascular plexi (SVP and DVP), ganglion cell–internal boundary membrane complex density (GCL-ILM), and retinal nerve fiber layer (RNFL) thickness [
12].
In the present study conducted on subjects with hypertension and dyslipidemia, the correlation between blood pressure (systolic and diastolic) and clinical variables showed that higher blood pressure is associated with higher total cholesterol and LDL and with lower HDL values. Triglycerides were not demonstrated to be statistically related to changes in OCTA parameters.
In our sample, participants with hypertension and a higher BMI and waist circumference had a higher blood pressure, suggesting a relationship between obesity and blood hypertension [
19].
Our subjects had no diabetes and no undiagnosed diabetic retinopathy, and no relationship between hypertension and glycemia or HbA1c was found.
The relationship between blood pressure control, retinal blood vessels, choriocapillaris, and systemic vascular risk factors in hypertension was examined in our study.
We used the OCTA to confirm the association of blood pressure variability and dyslipidemia with OCTA parameters in hypertensive patients.
The choriocapillaris is composed of a dense network of capillaries, so it may be susceptible to damage as a result of uncontrolled systemic hypertension [
6].
In the present study, we calculated the VFA (area and flow area parameters) at the level of the choriocapillaris. We reported a decrease in the capillary network in hypertensive subjects, which may contribute to flow reduction in and the impairment of oxygen delivery to different organs. The following values resulted for VFA area (r = −0.368;
p = 0.001) and VFA flow area (r = −0.364;
p = 0.001) in the right-eye group. In the left-eye group, VFA area (r = −0.373;
p = 0.001) and VFA flow area (r = −0.379;
p = 0.001) were obtained. These microvascular alterations may represent an early step in hypertension-mediated organ damage, and thus, they can be markers in monitoring the beneficial effects of antihypertensive treatment, according to Rizzoni D, Agabiti-Rosei C, Boari G.E.M., Muiesan ML, and De Ciuceis C. [
10].
In our study conducted in a hypertensive retinopathy-based sample with OCTA performed in both eyes, higher NFA area and FAZ parameters (area, perimeter, and circularity) and lower VFA (area and flow area), density, and skeleton (total and ETDRS) were observed in hypertensive subjects.
In participants with higher FAZ area and perimeter, a reduction in VFA flow area, density, and skeleton was also observed. This shows that an increase in areas with no perfusion is associated with a decrease in blood flow and a decrease in perfused blood vessels.
Subjects with higher VFA (area and flow area) showed higher density and skeleton values, meaning that subjects with an increased area of blood vessels and an increased blood flow have a larger area of perfused vasculature.
Using the Pearson Correlation and Sig. (2-tailed) test, we discovered that higher density (total and ETDRS parameters) was closely connected with higher skeleton (total and ETDRS) in hypertensive individuals.
Analyzing both eyes groups with hypercholesterolemia, in the right-eye group, we found correlation between VFA area and HDL only to be statistically significant, while in the left-eye group, statistically significant correlations were determined for total cholesterol, HLD, LDL, and multiple OCTA parameters. Our results showed that higher values of total cholesterol and LDL were associated with increasing avascular areas, reduced vascular flow, and reduced vascular density.
In our study, no statistically significant correlations between hypertriglyceridemia and OCTA parameters in the right-eye and left-eye groups were found as well as for BP and hypertriglyceridemia.
We found no statistical significance between right-eye OCTA parameters and left-eye OCTA parameters in our study. The dependent t-test determined a value of p > 0.05.
OCTA is a more suitable technique for imaging the retinal microvasculature than the conventional invasive injectable dye angiography because OCTA allows for more efficient, rapid, non-invasive, and widely available imaging. Fluorescein angiography is unsuitable for use in large cohort studies and for consecutive follow-up visits. Compared to OCTA of the retina, no other widely available imaging modality has yet been able to measure microvasculature with such good resolution, reproducibility, and short examination time [
20,
21].
Furthermore, studying changes in the microvasculature on OCTA in relation to systemic vascular disease may have the potential to detect early disease, to monitor disease progression, to potentially provide a better staging of hypertensive retinopathy, and to detect improvements in vasculature in patients with a better response to treatment.
Patients with progressive retinopathy and dyslipidemia are susceptible to coronary artery disease, peripheral vascular disease, and cerebrovascular events due to similar damage in other end-organ systems [
22].
Ong et al. noted in the Atherosclerosis Risk in Communities (ARIC) Study, which included 15,792 participants, that hypertensive retinopathy was associated with an increased risk of stroke, independent of other risk factors. They recommended the use of fundus examination to help assess the risk of stroke in these patients [
23].
Chen and co-workers studied a number of 9793 hypertensive patients within the China Stroke Primary Prevention Trial. Of these, 592 patients suffered from a stroke at the end of a 4.4-year follow-up, and a significant association was found between the presence of hypertensive retinopathy and the risk of a cerebrovascular event [
24]. Hua D, Xu Y, Zeng X, et al. noted that the microvascular structure of the retina and the cerebral and cardiac tissue have multiple similarities, so fundus examination may have an important role in the detection of end-organ damage. They suggested that the use of OCTA could increase the prediction of end-organ damage [
4].
Additional damage to the eye is also possible. The persistence of arteriolar sclerosis can potentially lead to an increased incidence of arteriolar vein occlusions within the eye, as observed by Kotruchin P, Tangpaisarn T, Mitsungnern T, et al. [
24].
Our findings were similar to the study performed by Chua et al. and by Sun et al. in that all our analyses confirmed a decrease in the deep capillary density in patients with systemic hypertension [
6,
11]. However, the difference with the study carried out by Sun et al. is that in our study did not determine intraocular pressure, visual acuity, and spherical equivalent, and our study did not compare the characteristics between groups, i.e., control and hypertensive. In addition, our study did not correlate choriocapillaris microvasculature with BP and renal parameters, which was analyzed by Chua et al. in their study. We had no control group, unlike other studies. Similar to the study performed by C Cuspidi et al. on non-diabetic hypertensive patients, retinal lesions were correlated with blood pressure, age, body mass index, smoking habit, and total serum cholesterol [
7]. The difference is that we used OCTA as a tool for monitoring retinopathy progression, and we performed correlations between OCTA parameters and dyslipidemia.
In 2022, Rebecca Zeng et al. performed an observational study on retinal microvasculature and vasoreactivity changes in hypertension using OCTA [
25]. Their study concluded that OCTA showed significant differences in the retinal vasculature of hypertensive patients, and it was also the first to demonstrate the potential of OCTA to investigate retinal vascular reactivity in patients with hypertension. Vessel density, vessel skeletonized density, and fractal dimension were calculated. A total of 23 eyes with hypertension (17 patients) and 17 control eyes (15 patients) were included, and a 6 mm × 6 mm angiogram centered on the fovea was performed. The superficial capillary plexus, vascular density, and the choriocapillaris were significantly decreased in hypertensive patients compared to control eyes. Our study had similar finding on microvascular changes, but we calculated the correlation between progressive retinopathy and microvascular changes in patients with dyslipidemia, with a larger number of subjects and without a control group. We did not study cerebral and cardiac tissue, like Hua D, Xu Y, Zeng X, et al. [
26], and over a period of 18 months of monitoring our patients, we did not record any subjects with stroke, unlike Chen and co-workers [
4].
A.I. computer systems are used extensively in medical sciences for diagnosing patients, discovering new drugs, improving communication with patients, and remotely treating patients [
27]. In 2016, Gulshan V, Peng L, Coram M, Stumpe MC, Wu D, Narayanaswamy A, et al. developed and trained A.I. using 128,175 retinal fundus images to classify images as diabetic retinopathy and macular edema for adults with diabetes [
28].
The new version of the Optopol OCT provides an A.I. algorithm for posterior-layer segmentations. By improving the current A.I. system and using OCTA findings, our research could provide new OCTA parameters for automated measurements, could help in early-stage detection of progressive hypertensive retinopathy, and could help develop screening programs, leading to increased efficiency in diagnosing patients in shorter time.
Therefore, based on our statistically significant results, we propose a few OCTA correlations to be analyzed using A.I., thus potentially resulting in new OCTA parameters: correlation between a lower VFA area and a lower HDL, a higher FAZ circularity with a higher LDL and total cholesterol, a higher LDL with a higher NFA area, and a lower skeleton total with a lower HDL.
However, there are a few limitations to this study. Firstly, we did not determine the values of apolipoprotein A1 and apolipoprotein B in correlation with OCTA parameters. Secondly, our changes in retinal vasculature were not correlated with renal function, heart function, other peripheral microvasculature parameters, or other end-organ damage measurements. Our current OCTA imaging (Angio-OCT Optopol Revo NX 130) depends on motion contrast from blood flow to visualize the retinal vasculature; hence, vessels with flow below the detectable threshold were not displayed. We acknowledge that our manual measurement performed in order to delimit FAZ, NFA, and VFA may not be as exact as the automated measurements performed by the OCTA, but this is unlikely to significantly affect our results. Also, our cohort only included 77 participants. Consecutive follow-up visits are required after our 18-month observational study.
We used the OCTA as a tool for monitoring retinopathy associated with dyslipidemia, but other complementary methods, such as fluorescein angiography, suitable for use in small cohort studies, and indocyanine green angiography (ICGA), which is another diagnostic procedure used to examine choroidal blood flow and associated pathology, should be required in order to obtain more precise results.
In our study, our primary objective was to use OCTA as a tool for analyzing the progression of hypertensive retinopathy in patients with dyslipidemia. Our secondary objective was to suggest that an improvement of the current A.I. system of the OCTA can be made.
The current A.I. system has a direct impact on the accuracy of the clinical assessment and the assessment of the status of areas of pathology in the retina. This level of detection is based on the A.I. Retina layer segmentation and MIP algorithm, thus resulting in more accurate results and more detailed screening. A.I. segmentation is important for follow-up examinations, bringing a more accurate diagnosis when analyzing pathology over time. The MIP tool enables easier identification and tracking of blood vessels. We suggest updating the current A.I system by introducing mathematic formulas in the system to show that some OCTA parameters, lipid levels, and blood pressure are directly proportional to each other, while some OCTA variables are inversely proportional to blood pressure and lipid levels, thus resulting in a more accurate evaluation and monitoring of retinal pathology in patients with dyslipidemia and hypertension.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}