
The Influence of Cryopreservation on Sperm Morphology and Its Implications in Terms of Fractions of Higher-Quality Sperm

 , ,
, , 
Abstract
1. Introduction
- -
- The patient observing a period of sexual abstinence (number of days since the last ejaculation prior to testing);
- -
- Determining the most beneficial location and method of semen collection, as well as the best sample delivery method and time from semen collection to the start of analysis;
- -
- The choice of the appropriate container;
- -
- Including any comments from the patient upon sample delivery.
- -
- Genetic defects in sperm that have not been previously considered;
- -
- Incorrect positioning relative to the liquid nitrogen mirror, which can lead to the cooling of the sperm being either too slow or too rapid;
- -
- The immersion of prepared sperm directly into liquid nitrogen without an equilibration step in nitrogen vapors;
- -
- The failure to follow freezing protocols, including freezing times;
- -
- An incorrect medium volume to sperm volume ratio;
- -
- The failure to pre-warm the freezing medium;
- -
- The incorrect method of adding cryoprotectants to the sperm;
- -
- Omitting or shortening the sperm thawing time;
- -
- Too long a delay before starting the freezing procedure (>2 h);
- -
- Too long a time spent transferring frozen sperm to the collection container;
- -
- The failure to maintain a constant temperature for frozen sperm;
- -
- A lack of experience in personnel performing the freezing process, haste, or lack of precision;
- -
- Expired reagents;
- -
- Improper storage and transport conditions for the medium;
- -
- The failure to maintain optimal conditions in the laboratory during sperm thawing.
2. Materials and Methods
- -
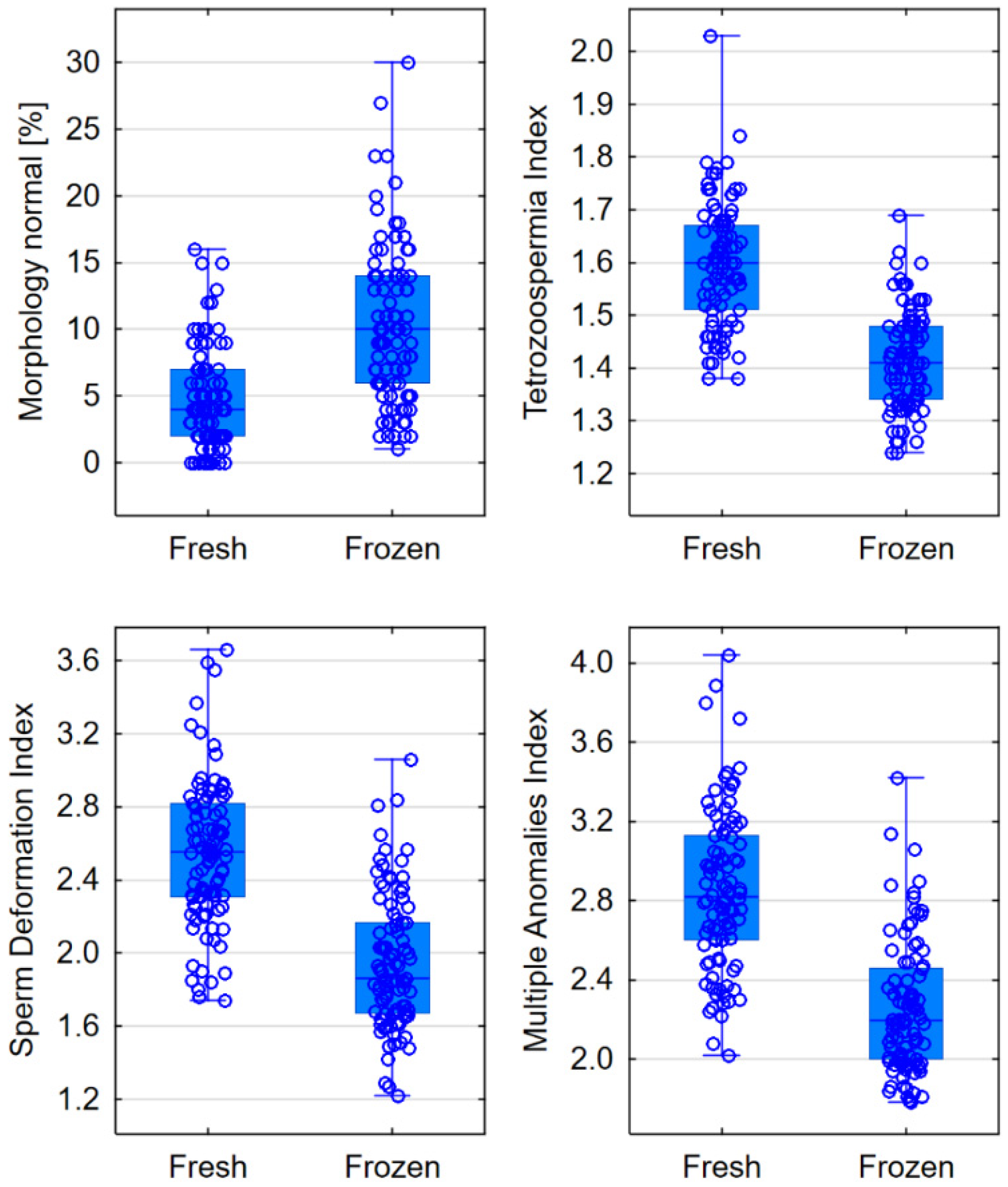
- Morphology: normal/abnormal sperm, Teratozoospermia Index, Sperm Deformation Index, and Multiple Anomalies Index;
- -
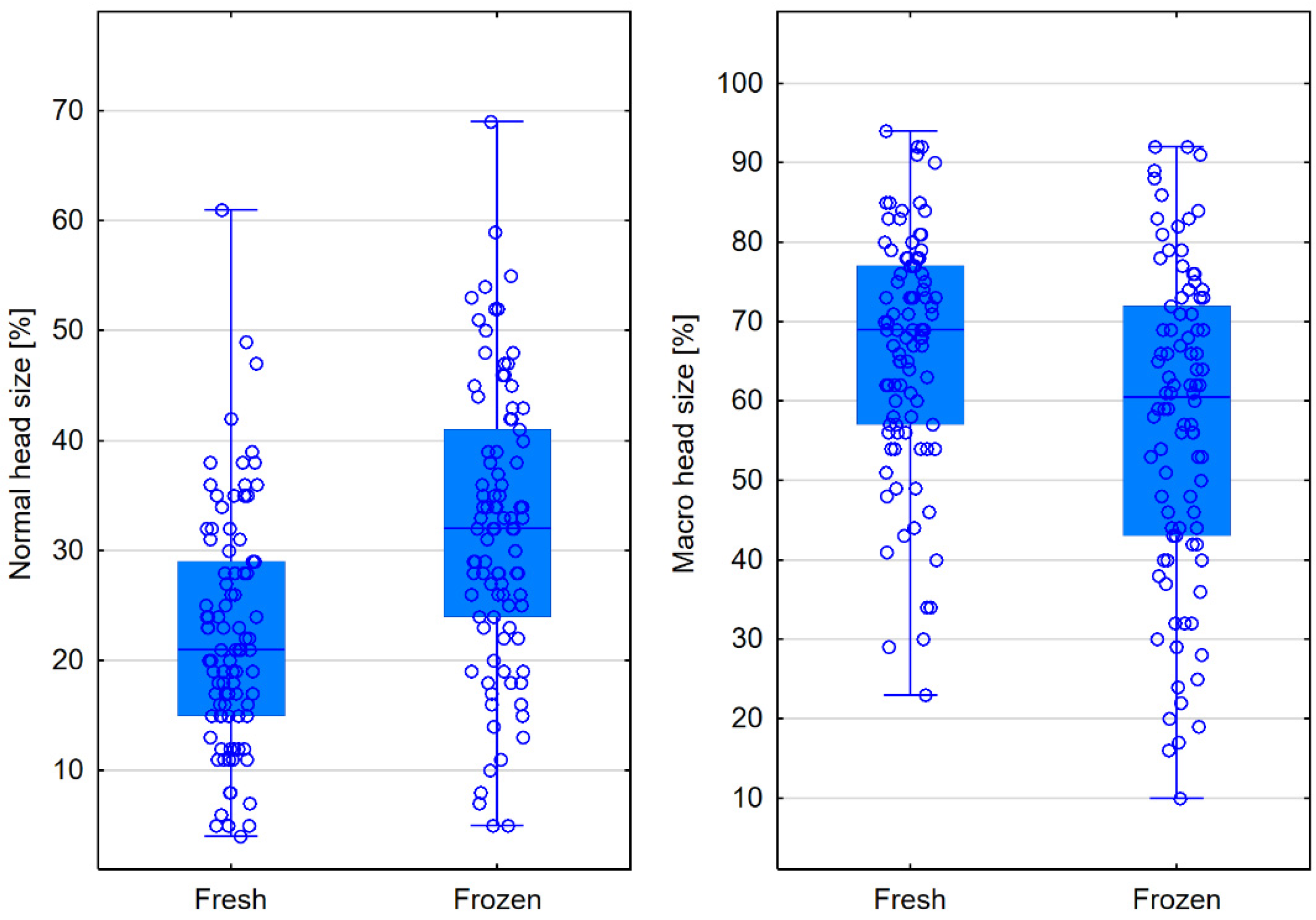
- Head size: normal, micro, and macro;
- -
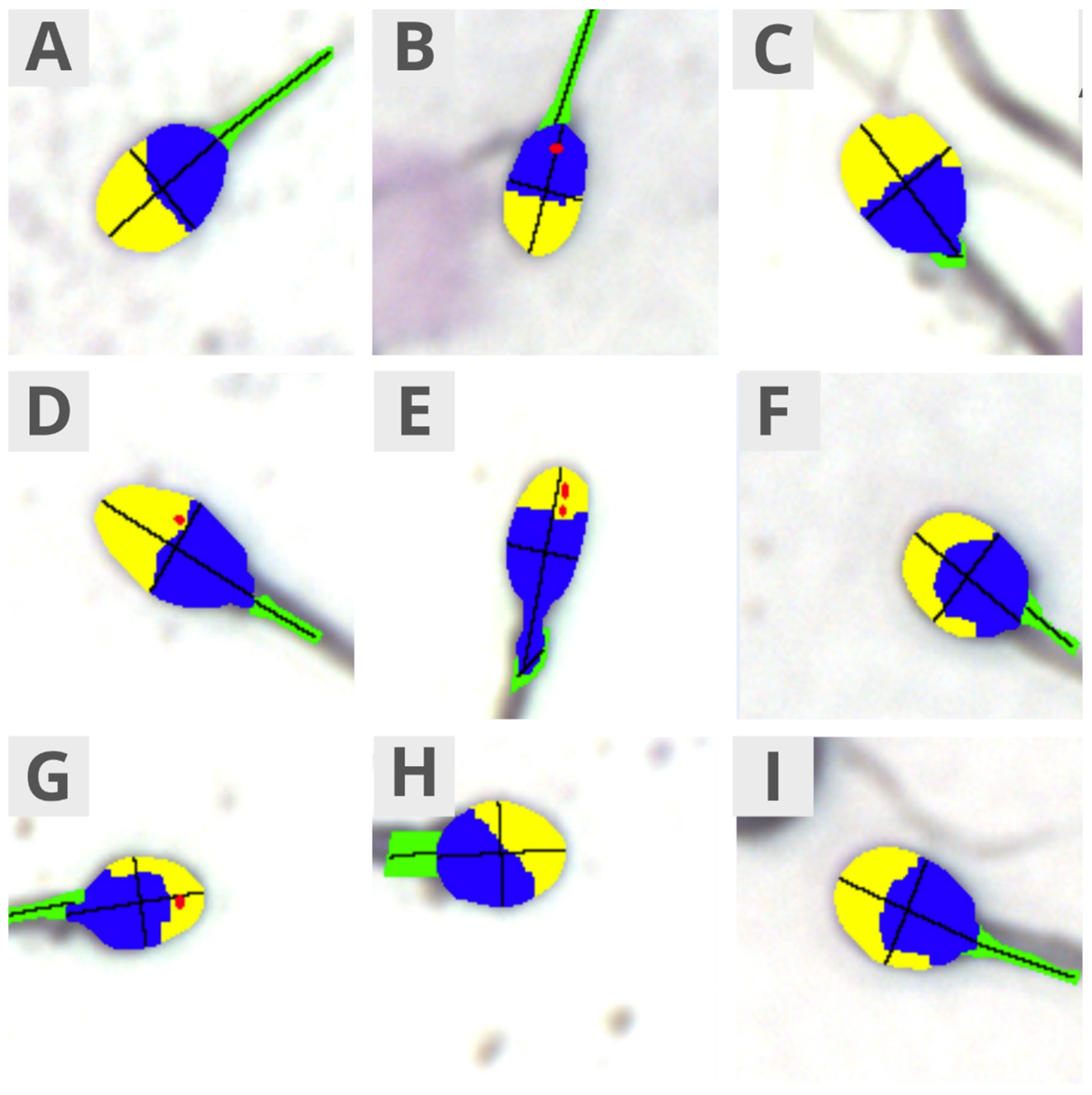
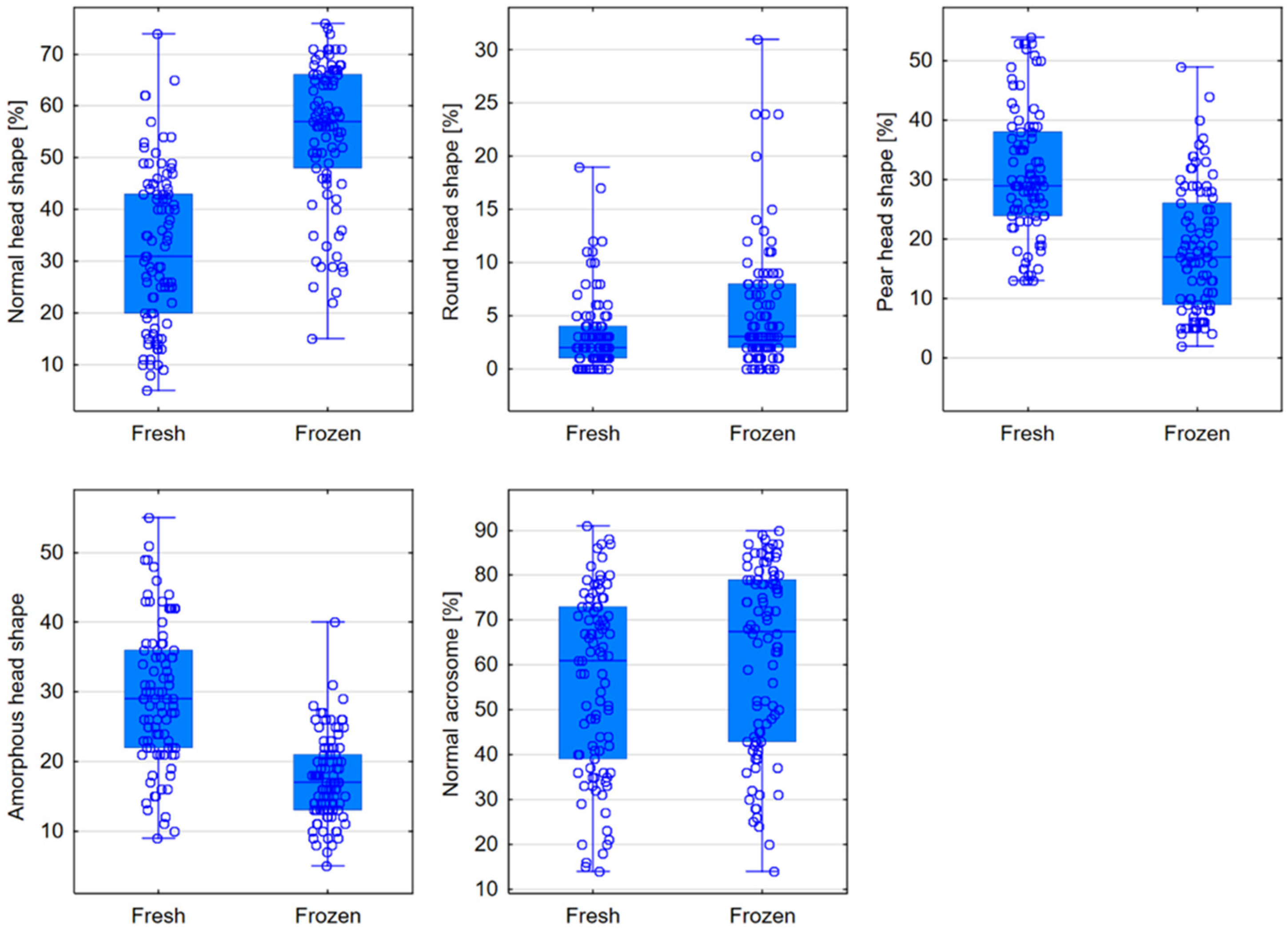
- Head shape: normal, conical, thin, round, pear-shaped, and amorphous;
- -
- Acrosome: normal/abnormal;
- -
- Midpiece: normal, abnormal size, abnormal insertion, and abnormal angle;
- -
- Morphometrics: head length, head width, head area, head circumference, ellipsoidal head, elongated head, smooth head, regular head, midpiece width, midpiece area, midpiece angle, and acrosome-to-head ratio.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the globe. Reprod. Biol. Endocrinol. 2015, 13, 2015. [Google Scholar] [CrossRef] [PubMed]
- Zańko, A.; Martynowicz, I.; Citko, A.; Konopka, P.; Paszko, A.; Pawłowski, M.; Szczerbiński, Ł.; Siewko, K.; Krętowski, A.J.; Kuczyński, W.; et al. The Influence of Lifestyle on Male Fertility in the Context of Insulin Resistance—Identification of Factors That Influence Semen Quality. J. Clin. Med. 2024, 13, 2797. [Google Scholar] [CrossRef] [PubMed]
- Cocuzza, M.; Alvarenga, C.; Pagani, R. The epidemiology and etiology of azoospermia. Clinics 2013, 68 (Suppl. S1), 15–26. [Google Scholar] [CrossRef] [PubMed]
- Barratt, C.L.R. Semen analysis is the cornerstone of investigation for male infertility. Practitioner 2007, 251, 8–10, 12, 15–17. [Google Scholar]
- Goyal, R.; Kotru, M.; Gogia, A.; Sharma, S. Qualitative defects with normal sperm counts in a patient attending infertility clinic. Indian. J. Pathol. Microbiol. 2018, 61, 233–235. [Google Scholar]
- Boitrelle, F.; Shah, R.; Saleh, R.; Henkel, R.; Kandil, H.; Chung, E.; Vogiatzi, P.; Zini, A.; Arfa, M.; Agarwal, A. The Sixth Edition of the WHO Manual for Human Semen Analysis: A Critical Review and SWOT Analysis. Life 2021, 11, 1368. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- López-Botella, A.; Velasco, I.; Acién, M.; Sáez-Espinosa, P.; Todolí-Torró, J.-L.; Sánchez-Romero, R.; Gómez-Torres, M.J. Impact of Heavy Metals on Human Male Fertility—An Overview. Antioxidants 2021, 10, 1473. [Google Scholar] [CrossRef]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th ed.; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Tamburrino, L.; Traini, G.; Marcellini, A.; Vignozzi, L.; Baldi, E.; Marchiani, S. Cryopreservation of Human Spermatozoa: Functional, Molecular and Clinical Aspects. Int. J. Mol. Sci. 2023, 24, 4656. [Google Scholar] [CrossRef]
- Jungwirth, A.; Diemer, T.; Kopa, Z.; Krausz, C.; Minhas, S.; Tournaye, H. EAU Guidelines on Male Fertility; European Association of Urology: Arnhem, The Netherlands, 2019. [Google Scholar]
- Directive 2004/23/EC OF the European Parliament and of the Council of 31 March 2004 on Setting Standards of Quality and Safety for the Donation, Procurement, Testing, Processing, Preservation, Storage and Distribution of Human Tissues and Cells, Vol. L 102, 2004, pp. 48–58. Available online: https://eur-lex.europa.eu/legal-content/EN/NIM/?uri=CELEX:32004L0023 (accessed on 9 December 2024).
- Commission Directive 2006/17/EC of 8 February 2006 Implementing Directive 2004/23/EC of the European Parliament and of the Council as Regards Certain Technical Requirements for the Donation, Procurement and Testing of Human Tissues and Cells Text with EE, Vol. L 330M, 2006, pp. 162–174. Available online: https://eur-lex.europa.eu/eli/dir/2006/17/oj (accessed on 9 December 2024).
- Ohlander, S.; Hotaling, J.; Kirshenbaum, E.; Niederberger, C.; Eisenberg, M.L. Impact of fresh versus cryopreserved testicular sperm upon intracytoplasmic sperm injection pregnancy outcomes in men with azoospermia due to spermatogenic dysfunction: A meta-analysis. Fertil. Steril. 2014, 101, 344–349. [Google Scholar] [CrossRef]
- Yu, Z.; Wei, Z.; Yang, J.; Wang, T.; Jiang, H.; Li, H.; Tang, Z.; Wang, S.; Liu, J. Comparison of intracytoplasmic sperm injection outcome with fresh versus frozen-thawed testicular sperm in men with nonobstructive azoospermia: A systematic review and meta-analysis. J. Assist. Reprod. Genet. 2018, 35, 1247–1257. [Google Scholar]
- Kuczyński, W.; Dhont, M.; Grygoruk, C.; Grochowski, D.; Wołczyński, S.; Szamatowicz, M. The outcome of intracytoplasmic injection of fresh and cryopreserved ejaculated spermatozoa—A prospective randomized study. Hum. Reprod. 2001, 16, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Tournaye, H.; Merdad, T.; Silber, S.; Joris, H.; Verheyen, G.; Devroey, P.; Van Steirteghem, A. No differences in outcome after intracytoplasmic sperm injection with fresh of with frozen-thawed epididymal spermatozoa. Hum. Reprod. 1999, 14, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Hungerford, A.; Bakos, H.W.; Aitken, R.J. Sperm cryopreservation: Current status and future developments. Reprod. Fertil. Dev. 2023, 35, 265–281. [Google Scholar] [CrossRef]
- Borate, G.M.; Meshram, A. Cryopreservation of Sperm: A Review. Cureus 2022, 14, e31402. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Tang, Y.-L.; Hu, J.-L.; Zhou, W.-J.; Huang, Z.-H.; Luo, X.-F.; Li, Z.; Zhu, W.-B. Update on techniques for cryopreservation of human spermatozoa. Asian J. Androl. 2022, 24, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Eastick, J.; Venetis, C.; Cooke, S.; Storr, A.; Susetio, D.; Chapman, M. Is early embryo development as observed by time-lapse microscopy dependent on whether fresh or frozen sperm was used for ICSI? A cohort study. J. Assist. Reprod. Genet. 2017, 34, 733–740. [Google Scholar] [CrossRef]
- O‘Connell, M.; McClure, N.; Lewis, S.E.M. The effects of cryopreservation on sperm morphology, motility and mitochondrial function. Hum. Reprod. 2002, 17, 704–709. [Google Scholar] [CrossRef]
- Hammadeh, M.E.; Askari, A.S.; Georg, T.; Rosenbaum, P.; Schmidt, W. Effect of freeze-thawing procedure on chromatin stability, morphological alteration and membrane integrity of human spermatozoa in fertile and subfertile men. Int. J. Androl. 1999, 22, 155–162. [Google Scholar] [CrossRef]
- Ozimic, S.; Ban-Frangez, H.; Stimpfel, M. Sperm Cryopreservation Today: Approaches, Efficiency, and Pitfalls. Curr. Issues Mol. Biol. 2023, 45, 4716–4734. [Google Scholar] [CrossRef]
- Di Santo, M.; Tarozzi, N.; Nadalini, M.; Borini, A. Human Sperm Cryopreservation: Update on Techniques, Effect on DNA Integrity, and Implications for ART. Adv. Urol. 2012, 13, 854837. [Google Scholar] [CrossRef]
- Hungerford, A.J.; Bakos, H.W.; Aitken, R.J. Analysis of sperm separation protocols for isolating cryopreserved human spermatozoa. Reprod. Fertil. 2023, 4, 220133. [Google Scholar] [CrossRef] [PubMed]
- Coutton, C.; Escoffier, J.; Martinez, G.; Arnoult, C.; Ray, P.F. Teratozoospermia: Spotlight on the main genetic actors in the human. Hum. Reprod. Update 2015, 21, 455–485. [Google Scholar] [CrossRef] [PubMed]
- De Braekeleer, M.; Nguyen, M.H.; Morel, F.; Perrin, A. Genetic aspects of monomorphic teratozoospermia: A review. J. Assist. Reprod. Genet. 2015, 32, 615–623. [Google Scholar] [CrossRef]
- Chemes, H.E. Sperm Ultrastructure in Fertile Men and Male Sterility: Revisiting Teratozoospermia. In The Sperm Cell: Production, Maturation, Fertilization, Regeneration; Cambridge University Press: Cambridge, UK, 2017; pp. 36–58. [Google Scholar]
- Fesahat, F.; Henkel, R.; Agarwal, A. Globozoospermia syndrome: An update. Andrologia 2019, 52, e13459. [Google Scholar] [CrossRef]
- Carmignac, V.; Dupont, J.-M.; Fierro, R.C.; Berberet, J.; Bruno, C.; Lieury, N.; Dulioust, E.; Auger, J.; Fauque, P. Diagnostic genetic screening for assisted reproductive technologies patients with macrozoospermia. Andrology 2017, 5, 37–380. [Google Scholar] [CrossRef]
- Elkhatib, R.A.; Paci, M.; Longepied, G.; Saias-Magnan, J.; Courbiere, B.; Guichaoua, M.-R.; Levy, N.; Metzler-Guillemain, C.; Mitchell, M.J. Homozygous deletion of SUN5 in three men with decapitated spermatozoa. Hum. Mol. Genet. 2017, 26, 3167–3171. [Google Scholar] [CrossRef]
- Fang, J.; Zhang, J.; Zhu, F.; Yang, X.; Cui, Y.; Liu, J. Patients with acephalic spermatozoa syndrome linked to SUN5 mutations have a favorable pregnancy outcome from ICSI. Andrology 2018, 33, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Walczak-Jędrzejowska, R.; Bakalczuk, S.; Berger, A.; Bergier, L.; Filipiak, E.; Frącki, S.; Jędrzejczak, P.; Kula, K.; Marchlewska, K.; Piasecka, M.; et al. Podstawowe badanie nasienia wg standardów Światowej Organizacji Zdrowia z roku 2010—Rekomendacje Polskiego Towarzystwa Andrologicznego i Krajowej Izby Diagnostów Laboratoryjnych. Warsaw, 2016. Available online: https://kidl.org.pl/get-file/85_rekomendacjebadanienasienia80.pdf (accessed on 9 December 2024).
- O‘Neill, H.C.; Nikoloska, M.; Ho, H.; Doshi, A.; Maalouf, W. Improved cryopreservation of spermatozoa using vitrification: Comparison of cryoprotectants and a novel device for long-term storage. J. Assist. Reprod. Genet. 2019, 36, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Ragini, G.; Caccamo, A.M.; Serra, A.D.; Guercilena, S. Computerized slow-staged freezing of semen from men with testicular tumors or Hodgkin’s disease preserves sperm better than standard vapor freezing. Fertil. Steril. 1990, 53, 1072–1075. [Google Scholar] [CrossRef]
- Ashwood-Smith, M.J.; Grant, E. Genetic stability in cellular systems stored in the frozen state. Ciba Found. Symp. 1977, 52, 251–272. [Google Scholar]
- Wierzbowski, S. Potrzeby, Możliwości i Warunki Tworzenia Rezerw Genetycznych Ssaków (Needs, Possibilities, and Conditions for Creating Genetic Reserves of Mammals). Biotechnologia 1990. Available online: http://rcin.org.pl/Content/186953/PDF/POZN271_221459_biotechnologia-1990-no1-wierzbowski.pdf (accessed on 9 December 2024).
- Huang, C.; Lei, L.; Wu, H.-L.; Gan, R.-X.; Yuan, X.-B.; Fan, L.-Q.; Zhu, W.-B. Long-term cryostage of semen in a human sperm bank does not affect clinical outcomes. Fertil. Steril. 2019, 112, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Raad, G.; Lteif, L.; Lahoud, R.; Azoury, J.; Tanios, J.; Hazzouri, M. Cryopreservation media differentially affect sperm motility, morphology and DNA integrity. Andrology 2018, 6, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Androni, D.A.; Dodds, S.; Tomlinson, M.; Maalouf, W.E. Is pre-freeze sperm preparation more advantageous than post-freeze? Reprod Fertil 2021, 2, 17–25. [Google Scholar] [CrossRef]
- Dede, G.; Saylan, A. The effect of astaxanthin on human sperm parameters after cryopreservation. Can. Urol. Assoc. J. 2022, 16, E552–E557. [Google Scholar] [CrossRef]
- Ghantabpour, T.; Nashtaei, M.S.; Nekoonam, S.; Razaei, H.; Amidi, F. The Effect of Astaxanthin on Motility, Viability, Reactive Oxygen Species, Apoptosis, and Lipid Peroxidation of Human Spermatozoa During the Freezing-Thawing Process. Biopreserv Biobank 2022, 22, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Gan, R.-X.; Hu, J.-L.; Liu, F.; Hong, Y.; Zhu, W.-B.; Li, Z. Clinical benefit for cryopreservation of single human spermatozoa for ICSI: A systematic review and meta-analysis. Andrology 2022, 10, 82–91. [Google Scholar] [CrossRef]
- Hammadeh, M.E.; Dehn, C.; Hippach, M.; Zeginiadou, T.; Stieber, M.; Georg, T.; Rosenbaum, P.; Schmidt, W. Comparison between computerized slow-stage and static liquid nitrogen vapour freezing methods with respect to the deleterious effect on chromatin and morphology of spermatozoa from fertile and subfertile men. Int. J. Androl. 2001, 24, 66–72. [Google Scholar] [CrossRef]
- Morris, G.J.; Acton, E.; Murray, B.J.; Fonseca, F. Freezing injury: The special case of the sperm cell. Cryobiology 2012, 64, 71–80. [Google Scholar] [CrossRef]
- Tongdee, P.; Sukprasert, M.; Satirapod, C.; Wongkularb, A.; Choktanasiri, V. Comparison of Cryopreserved Human Sperm between Ultra Rapid Freezing and Slow Programmable Freezing: Effect on Motility, Morphology and DNA Integrity. J. Med. Assoc. Thai 2015, 98 (Suppl. S4), S33–S42. [Google Scholar]
- Verheyen, G.; Pletincx, I.; Van Steirteghem, A. Effect of freezing method, thawing temperature and post-thaw dilution/washing on motility (CASA) and morphology characteristics of high-quality human sperm. Hum. Reprod. 1993, 8, 1678–1684. [Google Scholar] [CrossRef]
- Calamera, J.C.; Buffone, M.G.; Doncel, G.F.; Brugo-Olmeda, S.; de Vincentiis, S.; Calamera, M.M.; Storey, B.T.; Alvarez, J.G. Effect of thawing temperature on the motility recovery of cryopreserved human spermatozoa. Fertil. Steril. 2010, 93, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Menkveld, R.; Wong, W.Y.; Lombard, C.J.; Wetzels, A.M.; Thomas, C.M.; Merkus, H.M. Semen parameters, including WHO and strict criteria morphology, in a fertile population: An effort towards standardization of in-vivo thresholds. Hum. Reprod. 2001, 16, 1165–1171. [Google Scholar] [CrossRef]
- Aziz, N.; Said, T.; Paasch, U.; Agarwal, A. The relationship between human sperm apoptosis, morphology and the sperm deformity index. Hum. Reprod. 2007, 22, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Said, T.M.; Agarwal, A.; Sharma, R.K.; Thomas, A.J., Jr.; Sikka, S.C. Impact of sperm morphology on DNA damage caused by oxidative stress induced by beta-nicotinamide adenine dinucleotide phosphate. Fertil. Steril. 2005, 83, 95–103. [Google Scholar] [CrossRef]
- Said, T.M.; Aziz, N.; Sharma, R.K.; Lewis-Jones, I.; Thomas, A.J., Jr.; Agarwal, A. Novel association between sperm deformity index and oxidative stress-induced DNA damage in infertile male patients. Asian J. Androl. 2005, 7, 121–126. [Google Scholar] [CrossRef]
- Aziz, N.; Sharma, R.K.; Mahfouz, R.; Jha, R.; Agarwal, A. Association of sperm morphology and the sperm deformity index (SDI) with poly (ADP-ribose) polymerase (PARP) cleavage inhibition. Fertil. Steril. 2011, 95, 2481–2484. [Google Scholar] [CrossRef] [PubMed]
- Gil-Salom, M.; Romero, J.; Minguez, Y.; Rubio, C.; De los Santos, M.J.; Remohí, J.; Pellicer, A. Pregnancies after intracytoplasmic sperm injection with cryopreserved testicular spermatozoa. Hum. Reprod. 1996, 11, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Friedler, S.; Raziel, A.; Strassburger, D.; Komarovsky, D.; Ron-El, R. The outcome of intracytoplasmic injection of fresh and cryopreserved epididymal spermatozoa from patients with obstructive azoospermia--a comparative study. Hum. Reprod. 1998, 13, 1872–1877. [Google Scholar] [CrossRef]
- Garrels, K.L.; Zini, A.S.; Casper, R.F.; Meriano, J.S.; Jarvi, K.A. Fresh and frozen epididymal sperm yield comparable pregnancy rates for intracytoplasmic sperm injection. Arch. Androl. 1998, 41, 159–165. [Google Scholar] [CrossRef]
- Ulug, U.; Bener, F.; Karagenc, L.; Ciray, N.; Bahceci, M. Outcomes in couples undergoing ICSI: Comparison between fresh and frozen-thawed surgically retrieved spermatozoa. Int. J. Androl. 2005, 28, 343–349. [Google Scholar] [CrossRef]
- Cherouveim, P.; Vagios, S.; Hammer, K.; Fitz, V.; Jiang, V.S.; Dimitriadis, I.; Sacha, C.R.; James, K.E.; Bormann, C.L.; Souter, I. The impact of cryopreserved sperm on intrauterine insemination outcomes: Is frozen as good as fresh? Front. Reprod. Health 2023, 31, 1181751. [Google Scholar] [CrossRef] [PubMed]
- Hai, E.; Zhang, J.; Zhang, J. Sperm freezing damage: The role of regulated cell death. Cell Death Discov. 2024, 10, 239. [Google Scholar] [CrossRef] [PubMed]
- Gouhier, C.; Pons-Rejraji, H.; Dollet, S.; Chaput, L.; Bourgne, C.; Berger, M.; Pereira, B.; Tchirkov, A.; Brugnon, F. Freezing Does Not Alter Sperm Telomere Length despite Increasing DNA Oxidation and Fragmentation. Genes 2023, 14, 1039. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, E.T.; McClure, N.; Lewis, S.E. Cryopreservation of human semen and prepared sperm: Effects on motility parameters and DNA integrity. Fertil. Steril. 2001, 76, 892–900. [Google Scholar] [CrossRef]
- Spanò, M.; Cordelli, E.; Leter, G.; Lombardo, F.; Lenzi, A.; Gandini, L. Nuclear chromatin variations in human spermatozoa undergoing swim-up and cryopreservation evaluated by the flow cytometric sperm chromatin structure assay. Mol. Hum. Reprod. 1999, 5, 29–37. [Google Scholar] [CrossRef]
- Rios, A.P.; Gascón, A.; Martínez, J.V.; Balasch, S.; Botella, I.M. Sperm preparation after freezing improves motile sperm count, motility, and viability in frozen-thawed sperm compared with sperm preparation before freezing-thawing process. J. Assist. Reprod. Genet. 2018, 35, 237–245. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Morphology | Fresh Semen | Frozen Semen | p Level |
|---|---|---|---|
| Normal [%] | 4 (2–7) | 10 (6–14) | <0.0001 |
| Teratozoospermia Index (TZI) | 1.60 (1.51–1.67) | 1.41 (1.34–1.48) | <0.0001 |
| Sperm Deformation Index (SDI) | 2.56 (2.31–2.82) | 1.86 (1.67–2.17) | <0.0001 |
| Multiple Anomalies Index (MAI) | 2.82 (2.60–3.13) | 2.20 (2.00–2.46) | <0.0001 |
| Head Size | Fresh Semen | Frozen Semen | p Level |
|---|---|---|---|
| Normal [%] | 21 (15–29) | 32 (24–41) | <0.0001 |
| Micro [%] | 8 (5–15) | 6.5 (3–15) | 0.2694 |
| Macro [%] | 69 (57–77) | 60.5 (43–72) | <0.0001 |
| Head Shape | Fresh Semen | Frozen Semen | p Level |
|---|---|---|---|
| Normal [%] | 31 (20–43) | 57 (48–66) | <0.0001 |
| Conical [%] | 0 (0–1) | 1 (0–2) | 0.0665 |
| Thin [%] | 3 (1–5) | 2 (0–5) | 0.0580 |
| Round [%] | 2 (1–4) | 3 (2–8) | <0.0001 |
| Pear-shaped [%] | 29 (24–38) | 17 (9–26) | <0.0001 |
| Amorphous [%] | 29 (22–36) | 17 (13–21) | <0.0001 |
| Acrosome | |||
| Normal [%] | 61 (39–73) | 67.5 (43–79) | 0.0009 |
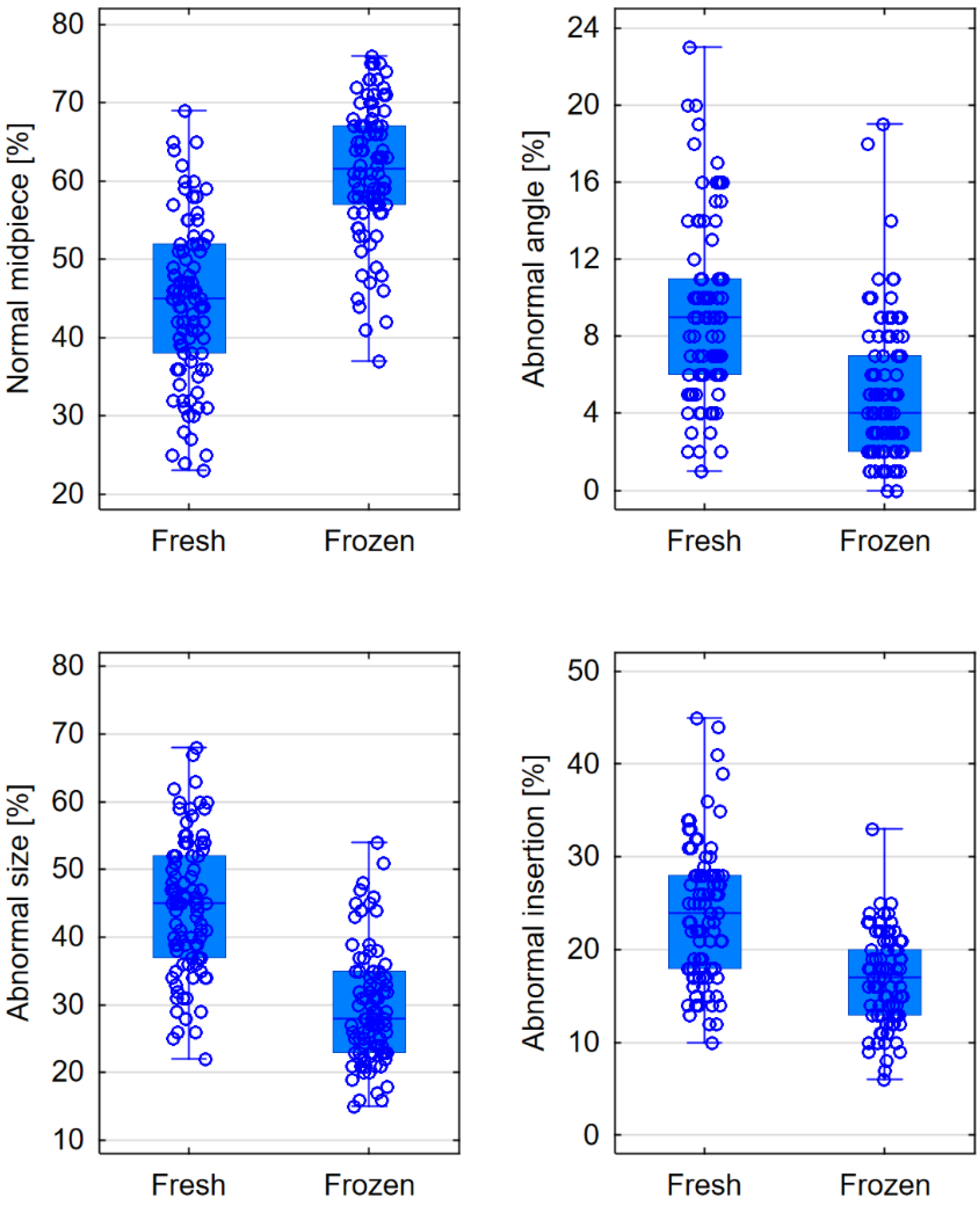
| Midpiece | Fresh Semen | Frozen Semen | p Level |
|---|---|---|---|
| Normal midpiece [%] | 45 (38–52) | 61.5 (57–67) | <0.0001 |
| Abnormal size [%] | 45 (37–52) | 28 (23–35) | <0.0001 |
| Abnormal insertion [%] | 24 (18–28) | 17 (13–20) | <0.0001 |
| Abnormal angle [%] | 9 (6–11) | 4 (2–7) | <0.0001 |
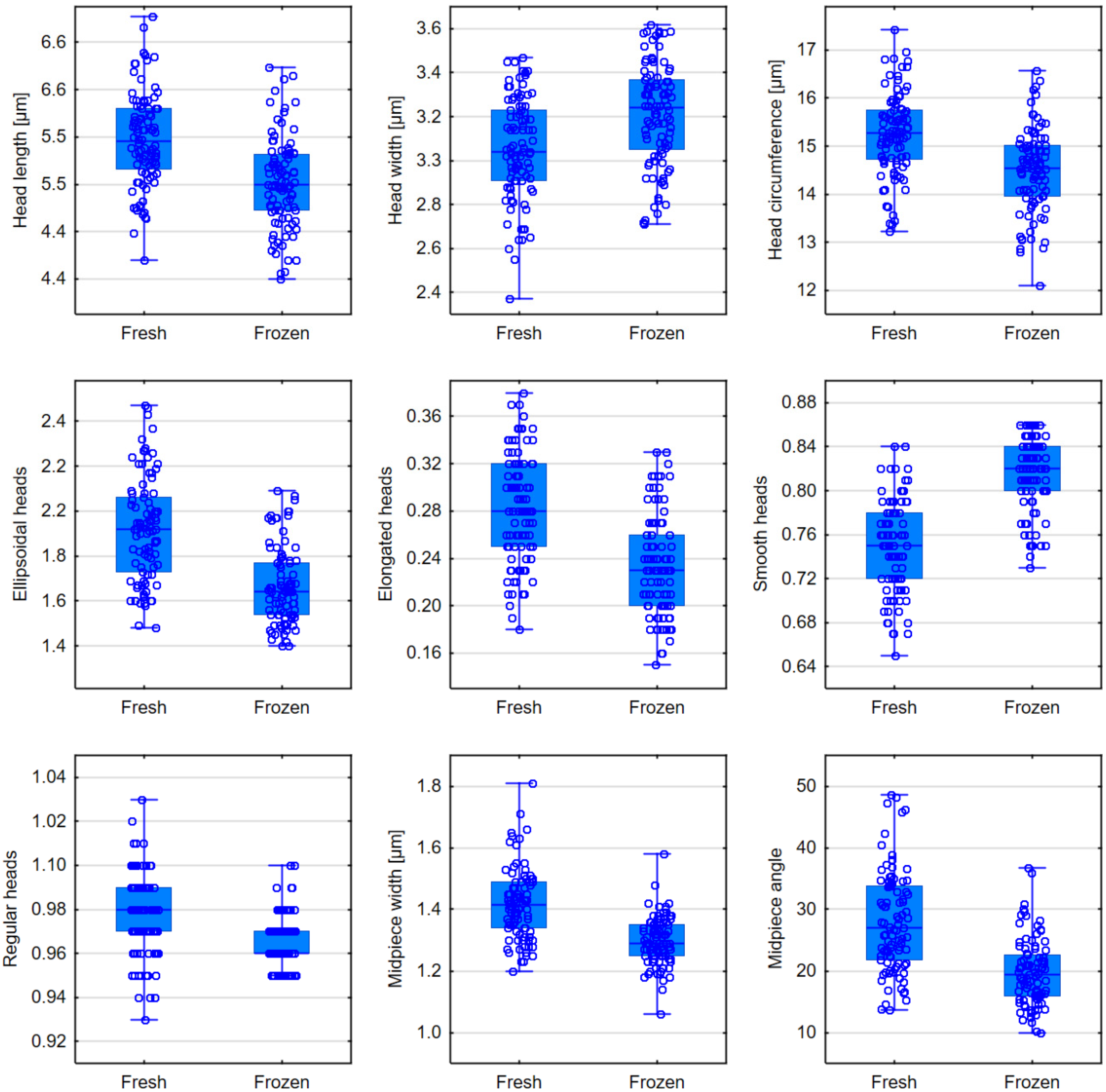
| Morphometrics | Fresh Semen | Frozen Semen | p Level |
|---|---|---|---|
| Head length [μm] | 5.57 (5.33–5.84) | 5.20 (4.98–5.45) | <0.0001 |
| Head width [μm] | 3.04 (2.91–3.23) | 3.24 (3.05–3.37) | <0.0001 |
| Head area [μm2] | 13.78 (12.89–14.48) | 13.72 (12.69–14.54) | 0.7831 |
| Head circumference [μm] | 15.27 (14.73–15.75) | 14.55 (13.96–15.02) | <0.0001 |
| Ellipsoidal heads | 1.92 (1.73–2.06) | 1.64 (1.54–1.77) | <0.0001 |
| Elongated heads | 0.28 (0.25–0.32) | 0.23 (0.20–0.26) | <0.0001 |
| Smooth heads | 0.75 (0.72–0.78) | 0.82 (0.80–0.84) | <0.0001 |
| Regular heads | 0.98 (0.97–0.99) | 0.96 (0.96–0.97) | <0.0001 |
| Midpiece width [μm] | 1.42 (1.34–1.49) | 1.29 (1.25–1.35) | <0.0001 |
| Midpiece area [μm2] | 1.64 (1.52–1.82) | 1.69 (1.57–1.79) | 0.7777 |
| Midpiece angle [°] | 27.05 (21.86–33.85) | 19.36 (15.90–22.57) | <0.0001 |
| Acrosome-to-head ratio [%] | 53.46 (48.05–69.86) | 58.65 (50.41–70.53) | 0.0982 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milewska, A.J.; Kuczyńska, A.; Pawłowski, M.; Martynowicz, I.; Deluga-Białowarczuk, S.; Sieczyński, P.; Kuczyński, W.; Milewski, R. The Influence of Cryopreservation on Sperm Morphology and Its Implications in Terms of Fractions of Higher-Quality Sperm. J. Clin. Med. 2024, 13, 7562. https://doi.org/10.3390/jcm13247562
Milewska AJ, Kuczyńska A, Pawłowski M, Martynowicz I, Deluga-Białowarczuk S, Sieczyński P, Kuczyński W, Milewski R. The Influence of Cryopreservation on Sperm Morphology and Its Implications in Terms of Fractions of Higher-Quality Sperm. Journal of Clinical Medicine. 2024; 13(24):7562. https://doi.org/10.3390/jcm13247562
Chicago/Turabian StyleMilewska, Anna Justyna, Agnieszka Kuczyńska, Michał Pawłowski, Iwo Martynowicz, Sebastian Deluga-Białowarczuk, Piotr Sieczyński, Waldemar Kuczyński, and Robert Milewski. 2024. "The Influence of Cryopreservation on Sperm Morphology and Its Implications in Terms of Fractions of Higher-Quality Sperm" Journal of Clinical Medicine 13, no. 24: 7562. https://doi.org/10.3390/jcm13247562
APA StyleMilewska, A. J., Kuczyńska, A., Pawłowski, M., Martynowicz, I., Deluga-Białowarczuk, S., Sieczyński, P., Kuczyński, W., & Milewski, R. (2024). The Influence of Cryopreservation on Sperm Morphology and Its Implications in Terms of Fractions of Higher-Quality Sperm. Journal of Clinical Medicine, 13(24), 7562. https://doi.org/10.3390/jcm13247562