
Exploring App-Based Physiotherapy for Somatic Tinnitus: Results from a Pilot Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Design
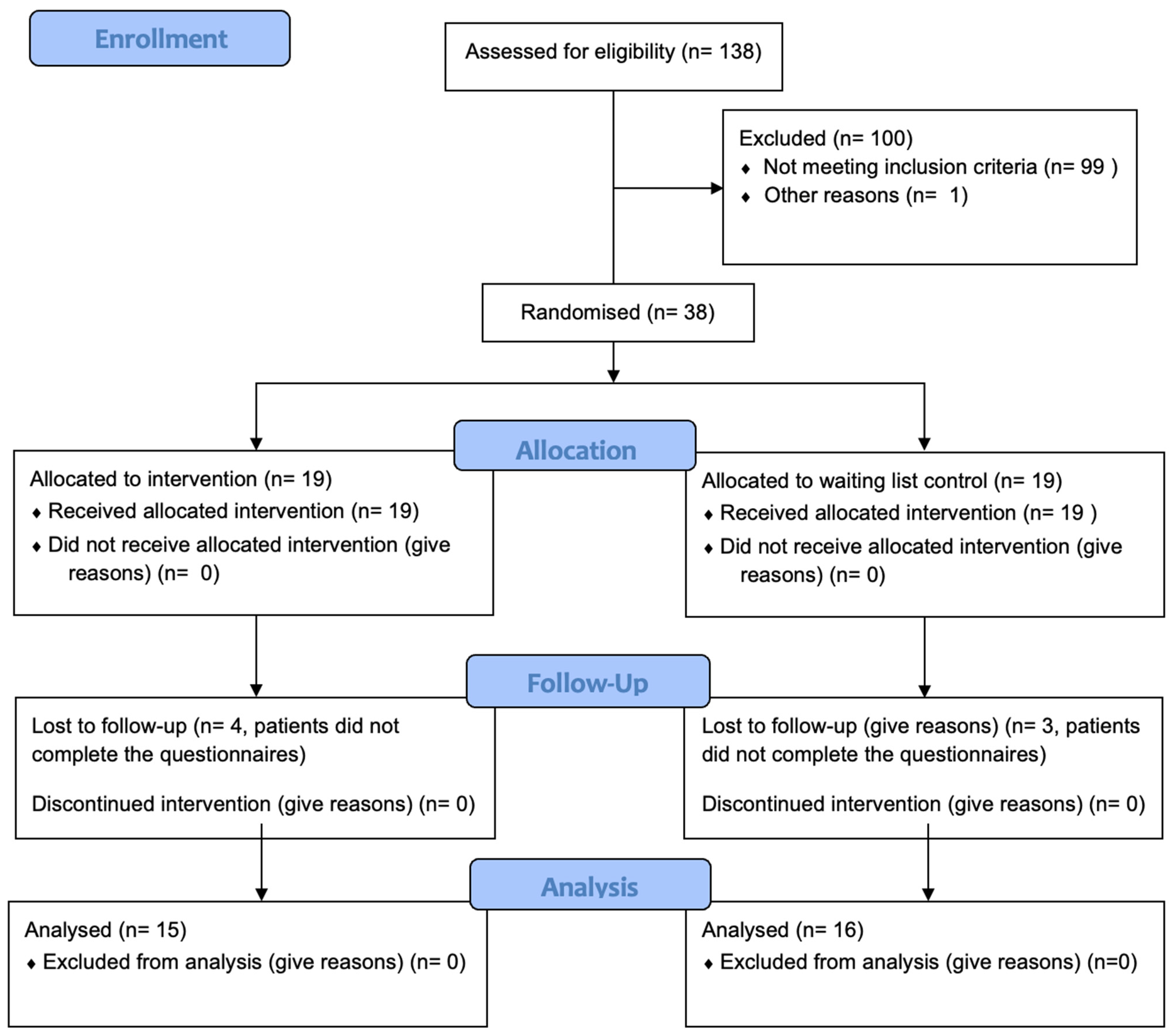
2.2. Participants
2.3. Inclusion and Exclusion Criteria
2.4. Intervention
2.5. Outcome Measures
2.6. Primary Outcome Measure
2.7. Secondary Outcome Measure
2.8. Statistics
3. Results
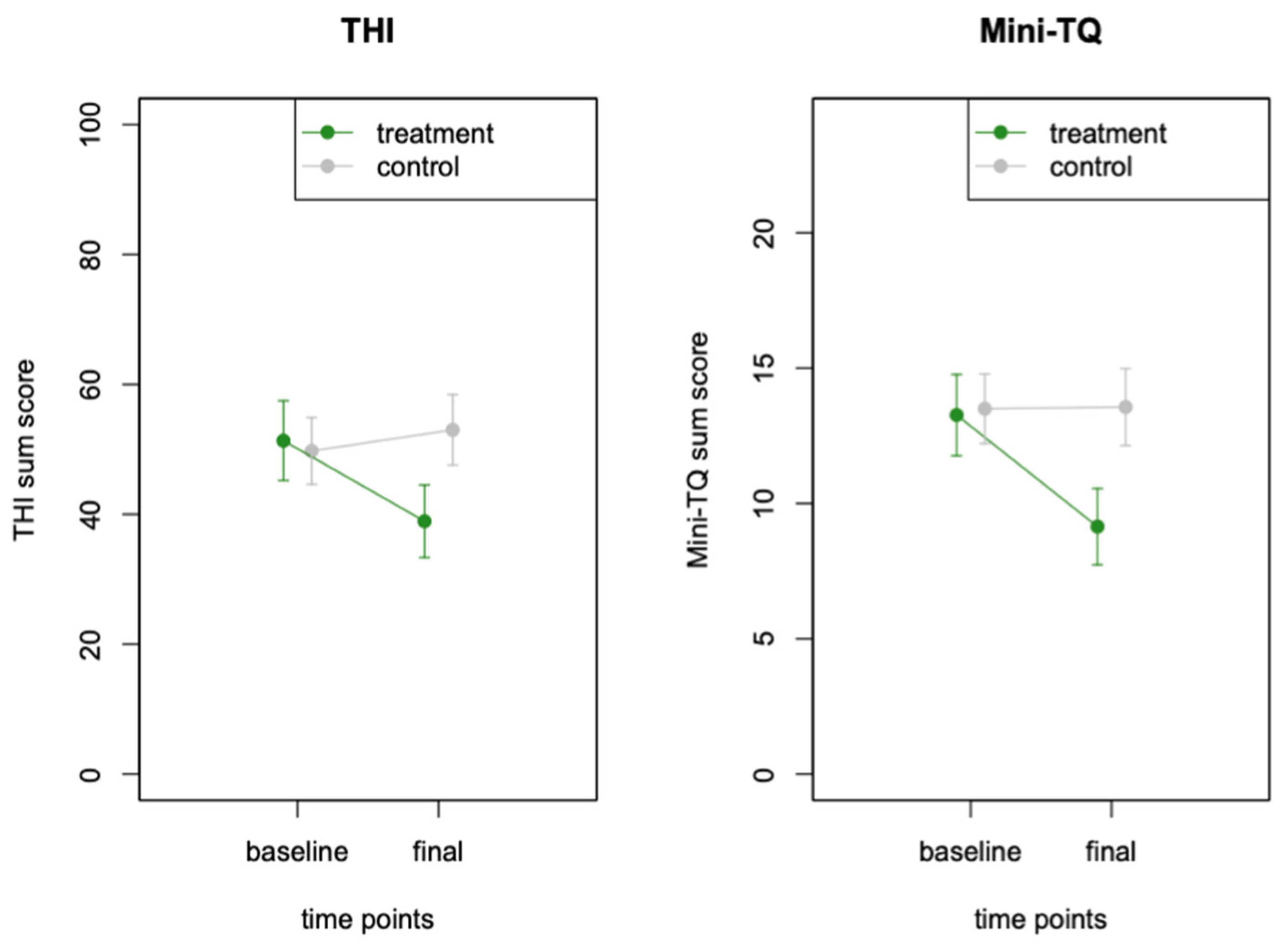
Effect on Tinnitus Distress
4. Discussion
4.1. Limitations and Future Research Questions
4.2. Somatic Tinnitus Treatment via Smartphone Application
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.A.; Dennis, K.C.; Schechter, M.A. General review of tinnitus: Prevalence, mechanisms, effects, and management. J. Speech Lang. Hear. Res. 2005, 48, 1204–1235. [Google Scholar] [CrossRef] [PubMed]
- Hiller, W.; Janca, A.; Burke, K.C. Association between tinnitus and somatoform disorders. J. Psychosom. Res. 1997, 43, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Pinchoff, R.J.; Burkard, R.F.; Salvi, R.J.; Coad, M.L.; Lockwood, A.H. Modulation of tinnitus by voluntary jaw movements. Am. J. Otol. 1998, 19, 785–789. [Google Scholar]
- Zhan, X.; Pongstaporn, T.; Ryugo, D.K. Projections of the second cervical dorsal root ganglion to the cochlear nucleus in rats. J. Comp. Neurol. 2006, 496, 335–348. [Google Scholar] [CrossRef]
- Shore, S.; Zhou, J.; Koehler, S. Neural mechanisms underlying somatic tinnitus. Prog. Brain Res. 2007, 166, 107–123. [Google Scholar]
- Haider, H.F.; Hoare, D.J.; Costa, R.F.P.; Potgieter, I.; Kikidis, D.; Lapira, A.; Nikitas, C.; Caria, H.; Cunha, N.T.; Paço, J.C. Pathophysiology, Diagnosis and Treatment of Somatosensory Tinnitus: A Scoping Review. Front. Neurosci. 2017, 11, 207. [Google Scholar] [CrossRef]
- Ginszt, M.; Szkutnik, J.; Zieliński, G.; Bakalczuk, M.; Stodółkiewicz, M.; Litko-Rola, M.; Ginszt, A.; Rahnama, M.; Majcher, P. Cervical Myofascial Pain Is Associated with an Imbalance of Masticatory Muscle Activity. Int. J. Environ. Res. Public Health 2022, 19, 1577. [Google Scholar] [CrossRef]
- Michiels, S. Somatosensory Tinnitus: Recent Developments in Diagnosis and Treatment. J. Assoc. Res. Otolaryngol. 2023, 24, 465–472. [Google Scholar] [CrossRef]
- Michiels, S.; Van de Heyning, P.; Truijen, S.; Hallemans, A.; De Hertogh, W. Does multi-modal cervical physical therapy improve tinnitus in patients with cervicogenic somatic tinnitus? Man. Ther. 2016, 26, 125–131. [Google Scholar] [CrossRef]
- Michiels, S.; Nieste, E.; Van de Heyning, P.; Braem, M.; Visscher, C.; Topsakal, V.; De Hertogh, W. Does conservative temporomandibular therapy affect tinnitus complaints? A systematic review. J. Oral Facial Pain Headache 2019, 33, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Oostendorp, R.A.B.; Bakker, I.; Elvers, H.; Mikolajewska, E.; Michiels, S.; De Hertogh, W. Cervicogenic somatosensory tinnitus: An indication for manual therapy plus education? Part 2: A pilot study. Man. Ther. 2016, 23, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Michiels, S.; Naessens, S.; Van de Heyning, P.; Braem, M.; Visscher, C.; Gilles, A.; De Hertogh, W. The Effect of Physical Therapy Treatment in Patients with Subjective Tinnitus: A Systematic Review. Front. Neurosci. 2016, 10, 545. [Google Scholar] [CrossRef]
- Van der Wal, A.; Michiels, S.; Van de Heyning, P.; Braem, M.; Visscher, C.; Topsakal, V.; De Hertogh, W. Treatment of somatosensory tinnitus: A randomized controlled trial studying the effect of orofacial treatment as part of a multidisciplinary program. J. Clin. Med. 2020, 9, 888. [Google Scholar] [CrossRef]
- Yu, H.-Z.; Gong, J.-M.; Hong, G.-W.; Zhou, R.-Q.; Fu, X.-P.; Fan, T.; Zheng, Y.-Q.; Peng, Y.-Q.; Li, J.; Wang, Y.-F. The Effect of Physical Therapy on Somatosensory Tinnitus. J. Clin. Med. 2024, 13, 3496. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Nagaraj, M.K.; Prabhu, P. Internet/smartphone-based applications for the treatment of tinnitus: A systematic review. Eur. Arch. Otorhinolaryngol. 2020, 277, 649–657. [Google Scholar] [CrossRef]
- Mehdi, M.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Contemporary Review of Smartphone Apps for Tinnitus Management and Treatment. Brain Sci. 2020, 10, 786. [Google Scholar] [CrossRef]
- Mehdi, M.; Stach, M.; Riha, C.; Neff, P.; Dode, A.; Pryss, R.; Schlee, W.; Reichert, M.; Hauck, F.J. Smartphone and mobile health apps for tinnitus: Systematic identification, analysis, and assessment. JMIR Mhealth Uhealth 2020, 8, e21767. [Google Scholar] [CrossRef]
- Genitsaridi, E.; Partyka, M.; Gallus, S.; Lopez-Escamez, J.A.; Schecklmann, M.; Mielczarek, M.; Trpchevska, N.; Santacruz, J.L.; Schoisswohl, S.; Riha, C. Standardized profiling for tinnitus research: The European School for Interdisciplinary Tinnitus Research Screening Questionnaire (ESIT-SQ). Hear. Res. 2019, 377, 353–359. [Google Scholar] [CrossRef]
- Michiels, S.; Ganz Sanchez, T.; Oron, Y.; Gilles, A.; Haider, H.F.; Erlandsson, S.; Bechter, K.; Vielsmeier, V.; Biesinger, E.; Nam, E.-C. Diagnostic Criteria for Somatosensory Tinnitus: A Delphi Process and Face-to-Face Meeting to Establish Consensus. Trends Hear. 2018, 22, 2331216518796403. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Goebel, G.; Hiller, W. The Tinnitus Questionnaire: A Standard Instrument for Grading the Degree of Tinnitus. Results of a Multicenter Study with the Tinnitus Questionnaire. HNO 1994, 42, 166–172. [Google Scholar] [PubMed]
- Hallam, R.S.; Jakes, S.C.; Hinchcliffe, R. Cognitive variables in tinnitus annoyance. Br. J. Clin. Psychol. 1988, 27, 213–222. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Treatment Group | Control Group | p-Value |
|---|---|---|---|
| Sample Size: N | 15 | 16 | |
| Gender: f/m | 9/6 | 7/9 | 0.586 |
| Age: years (std) | 50.93 (12.78) | 48.00 (13.60) | 0.542 |
| Tinnitus Duration: months (std) | 90.00 (84.71) | 94.85 (94.50) | 0.892 |
| Baseline THI Score: mean (std) | 51.33 (23.77) | 49.75 (20.54) | 0.844 |
| Baseline Mini-TQ Score: mean (std) | 13.27 (5.81) | 13.5 (5.13) | 0.907 |
| Parameter | Treatment Group | Control Group | F | p | Cohen’s d [95% CI] |
|---|---|---|---|---|---|
| THI Score | |||||
| Baseline | 51.33 (23.77) | 49.75 (20.54) | 1.71 | ||
| Final | 38.93 (21.66) | 53.0 (21.74) | F (1, 29) = 22.53 | 0.0001 | [0.85; 2.56] |
| Mini-TQ Score | |||||
| Baseline | 13.27 (5.81) | 13.5 (5.14) | 1.02 | ||
| Final | 9.14 (5.27) | 13.56 (5.68) | F (1, 28) = 9.79 | 0.0041 | [0.24; 1.80] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michiels, S.; Wölflick, S.; Simões, J.; Schlee, W. Exploring App-Based Physiotherapy for Somatic Tinnitus: Results from a Pilot Study. J. Clin. Med. 2024, 13, 7203. https://doi.org/10.3390/jcm13237203
Michiels S, Wölflick S, Simões J, Schlee W. Exploring App-Based Physiotherapy for Somatic Tinnitus: Results from a Pilot Study. Journal of Clinical Medicine. 2024; 13(23):7203. https://doi.org/10.3390/jcm13237203
Chicago/Turabian StyleMichiels, Sarah, Stella Wölflick, Jorge Simões, and Winfried Schlee. 2024. "Exploring App-Based Physiotherapy for Somatic Tinnitus: Results from a Pilot Study" Journal of Clinical Medicine 13, no. 23: 7203. https://doi.org/10.3390/jcm13237203
APA StyleMichiels, S., Wölflick, S., Simões, J., & Schlee, W. (2024). Exploring App-Based Physiotherapy for Somatic Tinnitus: Results from a Pilot Study. Journal of Clinical Medicine, 13(23), 7203. https://doi.org/10.3390/jcm13237203