
The Sensory Landscape and Embodied Experiences in Anorexia Nervosa Treatment: An Inpatient Sensory Ethnography

 , , ,
, , ,
Abstract
1. Introduction
Sensory Perceptions and Embodiment in Anorexia Nervosa
2. Methods
2.1. Setting
2.2. Sensory Ethnography
2.3. Research Team
2.4. Recruitment, Data Generation, and Collection
2.4.1. The Sensory Wellbeing Workshop
2.4.2. Semi-Structured Interviews
2.4.3. Sensory Mapping and Walkthroughs
2.4.4. Guided Sensory Reflection with AI-Assisted Visualization
2.4.5. Participant Observation
3. Results
3.1. Analysis Process
3.2. Synthesis of Findings
3.2.1. Feeling of Entrapment—“A Fat Body Trapped in a Small Space”
“I hate the feel and texture of velvet (expresses a shivering of dislike); it’s dry and is a very unpleasant sensation… My experience in the ward is very unpleasant. Something like being exposed to sensory stimuli you don’t like most. So touching velvet is very unpleasant for me. It’s dry. And I don’t like cushions as well. So, I relate all these unpleasant sensations to the ward”.
3.2.2. “Snow Leopard”—Duality of Experience and Emotional Ambivalence
“If I could put my ward experience into a material object, it would probably have to be a large soft toy, of some description, large soft toy, something like the snow leopard… Because it’s white. It would be soft and cuddly, but the animal itself is also quite a predator, so there’d always be that element of wariness. So, I would see that as my illness”.
“I’ve always been a huggy person, but my upbringing didn’t involve hugs. So, for me, white is pure, white is clean, and it is newness, newness of life. And although there is an element to be nearby to hug, and although deteriorating because it is a predator, and it can pounce at any time”[P5].
“I think any animal looks after its young. And I think that there is an element of nurture here from the staff. That I can relate to animals when they look after their young for a period of time and then they let them go into the blue to look after themselves. And here you get the same sensation, because although I’m not their young, they’re still next to me, caring for me, teaching me the way of life. So now I can go off into the world, and explore new pathway just like, you know, a leopard or snow leopard would do that for their young”[P5].
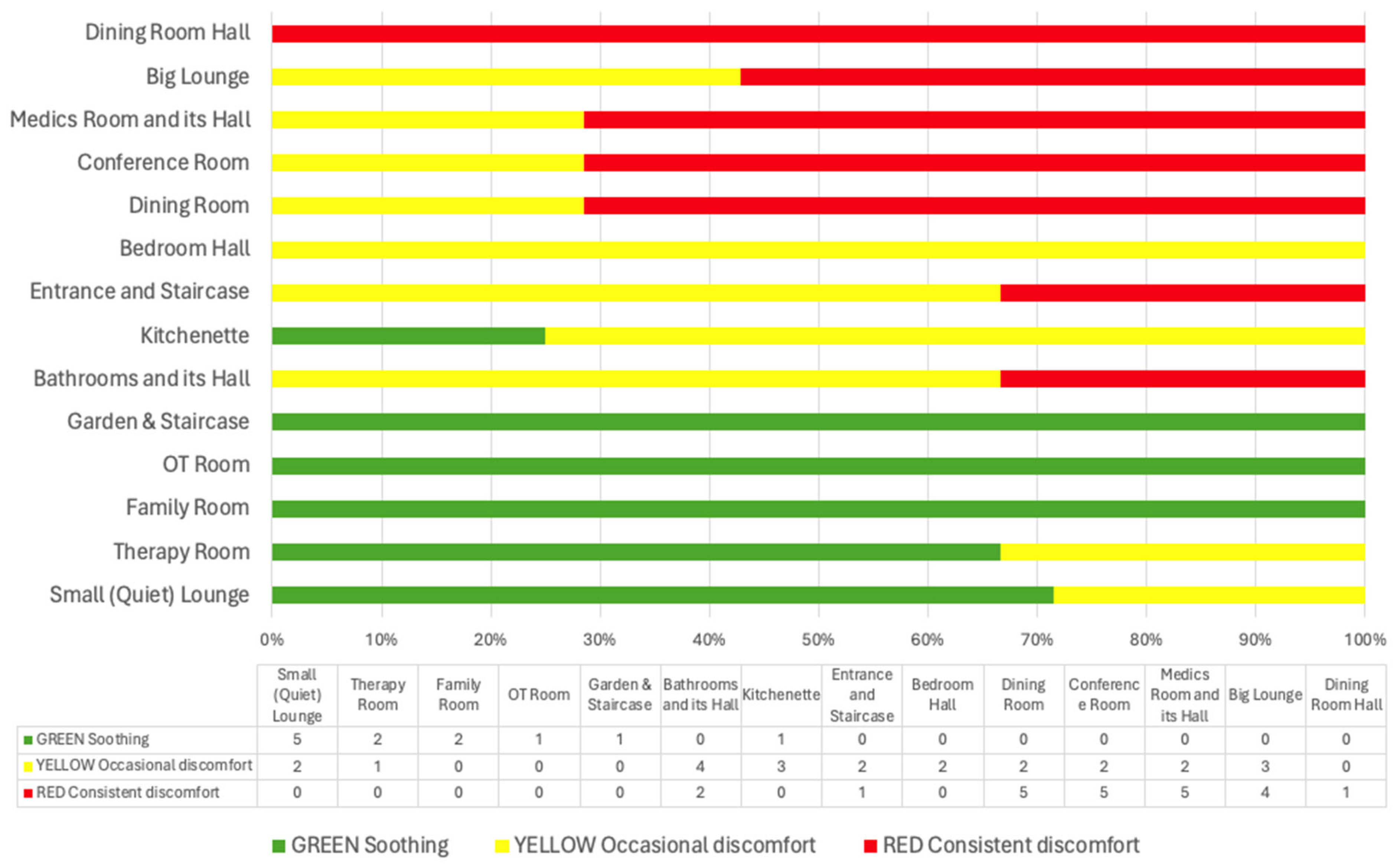
3.2.3. Sensory Mapping
4. Discussion
5. Limitations, Clinical Implications, and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Publishing. Diagnostic and Statistical Manual of Mental Disorders; Text revision; American Psychiatric Publishing: Washington, DC, USA, 2000. [Google Scholar]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders: A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, D.F.; Melen, S.; Mitchison, D.; Vos, T.; Whiteford, H.; Ferrari, A.J. The hidden burden of eating disorders: An extension of estimates from the Global Burden of Disease Study 2019. Lancet Psychiatry 2021, 8, 320–328. [Google Scholar] [CrossRef] [PubMed]
- van Hoeken, D.; Hoek, H.W. Review of the burden of eating disorders: Mortality, disability, costs, quality of life, and family burden. Curr. Opin. Psychiatry 2020, 33, 521–527. [Google Scholar] [CrossRef] [PubMed]
- UK, National Guideline Alliance. Eating Disorders: Recognition and Treatment; UK, National Guideline Alliance: London, UK, 2017. [Google Scholar]
- Hay, P. Current approach to eating disorders: A clinical update. Intern. Med. J. 2020, 50, 24–29. [Google Scholar] [CrossRef]
- Crone, C.; Fochtmann, L.J.; Attia, E.; Boland, R.; Escobar, J.; Fornari, V.; Golden, N.; Guarda, A.; Jackson-Triche, M.; Manzo, L. The American Psychiatric Association practice guideline for the treatment of patients with eating disorders. Am. J. Psychiatry 2023, 180, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Toppino, F.; Martini, M.; Longo, P.; Caldas, I.; Delsedime, N.; Lavalle, R.; Raimondi, F.; Abbate-Daga, G.; Panero, M. Inpatient treatments for adults with anorexia nervosa: A systematic review of literature. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2024, 29, 38. [Google Scholar] [CrossRef] [PubMed]
- de Vos, J.A.; LaMarre, A.; Radstaak, M.; Bijkerk, C.A.; Bohlmeijer, E.T.; Westerhof, G.J. Identifying fundamental criteria for eating disorder recovery: A systematic review and qualitative meta-analysis. J. Eat. Disord. 2017, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Kotilahti, E.; West, M.; Isomaa, R.; Karhunen, L.; Rocks, T.; Ruusunen, A. Treatment interventions for severe and enduring eating disorders: Systematic review. Int. J. Eat. Disord. 2020, 53, 1280–1302. [Google Scholar] [CrossRef]
- Fichter, M.M.; Quadflieg, N.; Crosby, R.D.; Koch, S. Long-term outcome of anorexia nervosa: Results from a large clinical longitudinal study. Int. J. Eat. Disord. 2017, 50, 1018–1030. [Google Scholar] [CrossRef]
- Rankin, R.; Conti, J.; Ramjan, L.; Hay, P. A systematic review of people’s lived experiences of inpatient treatment for anorexia nervosa: Living in a “bubble”. J. Eat. Disord. 2023, 11, 95. [Google Scholar] [CrossRef]
- Himmerich, H.; Keeler, J.L.; Davies, H.L.; Tessema, S.A.; Treasure, J. The evolving profile of eating disorders and their treatment in a changing and globalised world. Lancet 2024, 403, 2671–2675. [Google Scholar] [CrossRef] [PubMed]
- Espíndola, C.R.; Blay, S.L. Anorexia nervosa’s meaning to patients: A qualitative synthesis. Psychopathology 2009, 42, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.; Aouad, P.; Hambleton, A.; Touyz, S.; Maguire, S. ‘In an otherwise limitless world, I was sure of my limit.’Experiencing Anorexia Nervosa: A phenomenological metasynthesis. Front. Psychiatry 2022, 13, 894178. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, E.; Norton, C.; Stewart, C.; Tchanturia, K. Same behaviours, different reasons: What do patients with co-occurring anorexia and autism want from treatment? Int. Rev. Psychiatry 2019, 31, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Kiely, L.; Conti, J.; Hay, P. Conceptualisation of severe and enduring anorexia nervosa: A qualitative meta-synthesis. BMC Psychiatry 2023, 23, 606. [Google Scholar] [CrossRef]
- Conti, J.E.; Joyce, C.; Hay, P.; Meade, T. “Finding my own identity”: A qualitative metasynthesis of adult anorexia nervosa treatment experiences. BMC Psychol. 2020, 8, 110. [Google Scholar] [CrossRef]
- Cobbaert, L.; Hay, P.; Mitchell, P.B.; Roza, S.J.; Perkes, I. Sensory processing across eating disorders: A systematic review and meta-analysis of self-report inventories. Int. J. Eat. Disord. 2024, 57, 1465–1488. [Google Scholar] [CrossRef]
- Riva, G.; Dakanalis, A. Altered processing and integration of multisensory bodily representations and signals in eating disorders: A possible path toward the understanding of their underlying causes. Front. Hum. Neurosci. 2018, 12, 49. [Google Scholar] [CrossRef]
- Sim, L.; Peterson, C.B. The peril and promise of sensitivity in eating disorders. Int. J. Eat. Disord. 2021, 54, 2046–2056. [Google Scholar] [CrossRef]
- Martin, E.; Dourish, C.; Rotshtein, P.; Spetter, M.; Higgs, S. Interoception and disordered eating: A systematic review. Neurosci. Biobehav. Rev. 2019, 107, 166–191. [Google Scholar] [CrossRef]
- Kinnaird, E.; Stewart, C.; Tchanturia, K. The relationship of autistic traits to taste and olfactory processing in anorexia nervosa. Mol. Autism 2020, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, E.; Stewart, C.; Tchanturia, K. Interoception in anorexia nervosa: Exploring associations with alexithymia and autistic traits. Front. Psychiatry 2020, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, E.; Dandil, Y.; Li, Z.; Smith, K.; Pimblett, C.; Agbalaya, R.; Stewart, C.; Tchanturia, K. Pragmatic sensory screening in anorexia nervosa and associations with autistic traits. J. Clin. Med. 2020, 9, 1182. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, E.; Stewart, C.; Tchanturia, K. Taste sensitivity in anorexia nervosa: A systematic review. Int. J. Eat. Disord. 2018, 51, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Tchanturia, K. Supporting Autistic People with Eating Disorders: A Guide to Adapting Treatment and Supporting Recovery; Jessica Kingsley Publishers: London, UK, 2021. [Google Scholar]
- Tchanturia, K.; Baillie, C.; Biggs, C.; Carr, A.; Harrison, A.; Li, Z.; McFie, C.; Oyeleye, O.; Toloza, C. Sensory wellbeing workshops for inpatient and day-care patients with anorexia nervosa. Neuropsychiatrie 2022, 36, 51–59. [Google Scholar] [CrossRef]
- Bell, K.; Coulthard, H.; Wildbur, D. Self-disgust within eating disordered groups: Associations with anxiety, disgust sensitivity and sensory processing. Eur. Eat. Disord. Rev. 2017, 25, 373–380. [Google Scholar] [CrossRef]
- Zucker, N.L.; Merwin, R.M.; Bulik, C.M.; Moskovich, A.; Wildes, J.E.; Groh, J. Subjective experience of sensation in anorexia nervosa. Behav. Res. Ther. 2013, 51, 256–265. [Google Scholar] [CrossRef]
- Brand-Gothelf, A.; Parush, S.; Eitan, Y.; Admoni, S.; Gur, E.; Stein, D. Sensory modulation disorder symptoms in anorexia nervosa and bulimia nervosa: A pilot study. Int. J. Eat. Disord. 2016, 49, 59–68. [Google Scholar] [CrossRef]
- Merwin, R.M.; Moskovich, A.A.; Wagner, H.R.; Ritschel, L.A.; Craighead, L.W.; Zucker, N.L. Emotion regulation difficulties in anorexia nervosa: Relationship to self-perceived sensory sensitivity. Cogn. Emot. 2013, 27, 441–452. [Google Scholar] [CrossRef]
- Westwood, H.; Mandy, W.; Tchanturia, K. Clinical evaluation of autistic symptoms in women with anorexia nervosa. Mol. Autism 2017, 8, 1–9. [Google Scholar] [CrossRef]
- Tchanturia, K. What We Can Do About Autism and Eating Disorder Comorbidity; Wiley Online Library: Hoboken, NJ, USA, 2022; Volume 30, pp. 437–441. [Google Scholar]
- Eli, K.; Lavis, A. Material environments and the shaping of anorexic embodiment: Towards a materialist account of eating disorders. Cult. Med. Psychiatry 2022, 46, 344–363. [Google Scholar] [CrossRef] [PubMed]
- Csordas, T.J. Embodiment as a Paradigm for Anthropology. In Body/Meaning/Healing; Springer: Berlin/Heidelberg, Germany, 2002; pp. 58–87. [Google Scholar]
- Desjarlais, R.; Jason Throop, C. Phenomenological approaches in anthropology. Annu. Rev. Anthropol. 2011, 40, 87–102. [Google Scholar] [CrossRef]
- Eli, K.; Warin, M. Anthropological Perspectives on Eating Disorders: Deciphering Cultural Logics; SAGE Publications Sage UK: London, UK, 2018; Volume 55, pp. 443–453. [Google Scholar]
- Warin, M. Transformations of intimacy and sociality in anorexia: Bedrooms in public institutions. Body Soc. 2005, 11, 97–113. [Google Scholar] [CrossRef]
- Eli, K. Between difference and belonging: Configuring self and others in inpatient treatment for eating disorders. PLoS ONE 2014, 9, e105452. [Google Scholar] [CrossRef] [PubMed]
- Lester, R.J. The (dis) embodied self in anorexia nervosa. Soc. Sci. Med. 1997, 44, 479–489. [Google Scholar] [CrossRef]
- Lavis, A. The Boundaries of a Good Anorexic: Exploring Pro-Anorexia on the Internet and in the Clinic. Ph.D. Thesis, Goldsmiths, University of London, London, UK, 2011. [Google Scholar]
- Pink, S. Situating sensory ethnography: From academia to intervention. In Doing Sensory Ethnography; Sage: London, UK, 2009; pp. 7–23. [Google Scholar]
- Pink, S. Doing Sensory Ethnography; Sage: London, UK, 2015. [Google Scholar]
- Li, Z.; Holetic, V.; Webb, J.; Chubinidze, D.; Byford, S.; Tchanturia, K. In-person and online sensory wellbeing workshop for eating disorders: Updated case series. J. Eat. Disord. 2023, 11, 117. [Google Scholar] [CrossRef]
- Jewitt, C.; Leder Mackley, K. Methodological dialogues across multimodality and sensory ethnography: Digital touch communication. Qual. Res. 2019, 19, 90–110. [Google Scholar] [CrossRef]
- Clarke, V.; Braun, V. Successful Qualitative Research: A Practical Guide for Beginners; Sage: London, UK, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Westwood, H.; Kerr-Gaffney, J.; Stahl, D.; Tchanturia, K. Alexithymia in eating disorders: Systematic review and meta-analyses of studies using the Toronto Alexithymia Scale. J. Psychosom. Res. 2017, 99, 66–81. [Google Scholar] [CrossRef]
- Hay, P.; McIntosh, G.; Bulik, C. Specialist supportive clinical management for severe and enduring anorexia nervosa: A clinician’s manual. In Managing Severe and Enduring Anorexia Nervosa; Routledge: Oxfordshire, UK, 2016; pp. 112–127. [Google Scholar]
- Wilson, G.T.; Grilo, C.M.; Vitousek, K.M. Psychological treatment of eating disorders. Am. Psychol. 2007, 62, 199. [Google Scholar] [CrossRef]
- Serpell, L.; Treasure, J.; Teasdale, J.; Sullivan, V. Anorexia nervosa: Friend or foe? Int. J. Eat. Disord. 1999, 25, 177–186. [Google Scholar] [CrossRef]
- Williams, S.; Reid, M. Understanding the experience of ambivalence in anorexia nervosa: The maintainer’s perspective. Psychol. Health 2010, 25, 551–567. [Google Scholar] [CrossRef] [PubMed]
- Gulliksen, K.S.; Nordbø, R.H.; Espeset, E.M.; Skårderud, F.; Holte, A. The process of help-seeking in anorexia nervosa: Patients’ perspective of first contact with health services. Eat. Disord. 2015, 23, 206–222. [Google Scholar] [CrossRef] [PubMed]
- Geller, J.; Srikameswaran, S. Treatment non-negotiables: Why we need them and how to make them work. Eur. Eat. Disord. Rev. Prof. J. Eat. Disord. Assoc. 2006, 14, 212–217. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Participant Code * | Gender | Age | Ethnicity | Diagnosis | Duration | Comorbidity | Participant Observation | Sensory Wellbeing Workshop | Semi-Structured Interview | Guided Sensory Reflection with AI Assisted Visualization | Sensory Mapping & Walkthroughs |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P1 | Female | 19 | Black/Black British—Other | AN | 3 years | Autism | ✔ | ✔ | ✔ | ✔ | |
| P2 | Female | 19 | White British | AN | 3 years | Autism | ✔ | ✔ | ✔ | ✔ | ✔ |
| P3 | Female | 42 | White British | AN | >3 years | EUPD; agoraphobia; chronic fatigue syndrome; PTSD; anxiety | ✔ | ✔ | ✔ | ✔ | ✔ |
| P4 | Female | 19 | White British | AN | 2 years | ✔ | ✔ | ✔ | ✔ | ✔ | |
| P5 | Female | 61 | White British | AN | >3 years | ✔ | ✔ | ✔ | ✔ | ||
| P6 | Female | 20 | White British | AN | 2 years | ✔ | ✔ | ✔ | ✔ | ✔ | |
| P7 | Female | 18 | Mixed Race British—Other Mixed-Race | AN | <1 years | ✔ | ✔ | ✔ | ✔ | ✔ | |
| P8 | Female | 30 | White Other | AN | <1 years | Suspected EUPD and autism | ✔ | ✔ | ✔ | ||
| P9 | Female | 23 | White British | AN | 9 years | ✔ | ✔ | ✔ | ✔ | ||
| P10 | Female | 34 | White British | AN | 19 years | OCD; recurrent depressive disorder; EUPD | ✔ | ✔ | ✔ |
| Master Theme | Subordinate Theme | Cross-Cutting Themes |
|---|---|---|
| 1. Sensory Triggers of Distress This theme and its relevant sub-themes explore the various sensory stimuli that contribute to feelings of discomfort, anxiety, and distress. It illustrates how these sensory cues can act as constant reminders of the patients’ lack of control over their environment and reinforce the sense of being in a restrictive setting. | 1.1. Echoes of Anxiety | Feeling of Entrapment: “Fat Body Trapped in a Small Space” |
| 1.2. Visual Stressors of Isolation | ||
| 1.3. Olfactory Overwhelm | ||
| 1.4. Taste and Textural Discomfort | ||
| 1.5. Temperature Regulation Challenges | ||
| 2. Ambivalence in Treatment: Navigating Consistency, Sensory Needs, and Personalization This theme and its relevant sub-themes explore patients’ ambivalence toward treatment and their dual experiences of sensory stimuli. It illustrates the need for consistency in preferred sensory experiences, recognizing diverse sensory needs, and creating more opportunities to personalize the sensory landscape. | 2.1. Consistency and Predictability | “Snow Leopard”—Duality of Experience and Emotional Ambivalence |
| 2.2. Recognition of Sensory Needs and Personalization |
| Sensory Object |  Dual Nature of Snow Leopard |  Velvet Cushion of Discomfort |  Sticky Rubber Ball of Struggles |  Cracked Gray Square |  Trapped Body in a Small Space |  Isolated Blue Sphere |  Bittersweet Cracker with Jam |
| Themes | Duality of experience and emotional ambivalence | Feeling of entrapment | Feeling of entrapment Duality of experience and emotional ambivalence | Feeling of entrapment Duality of experience and emotional ambivalence | Feeling of entrapment | Feeling of entrapment | Duality of experience and emotional ambivalence |
| Sensory Characteristics | Visual: white, large. Tactile: soft, cuddly. | Visual: brown. Tactile: dry, unpleasant. Olfactory: smell of deodorant. | Visual: round, hand-sized, red with pointy bits Tactile: rigid, sticky, cold, sweaty, clammy Auditory: loud, hollow sound Gustatory: sour orange taste | Visual: large, gray, with cracks Tactile: rigid, cold, smooth Auditory: soft, dull metallic sound | Visual: a drawing depicting a large body enclosed in a small, confined space | Visual: large, blue Tactile: hard, smooth Temperature: very cold | Visual: cracker with jam Texture: crunchy and slimy Gustatory: bittersweet, with a mix of textures |
| Emotional States/Responses | Feeling cared for and nurtured yet aware of potential threat. Safety vs. vulnerability. Dependence vs. independence. Comfort vs. fear. | Dislike Discomfort Aversion Frustration and distress Sensory overload Resistance | Confusion Frustration Mixed feelings of comfort and discomfort Alienation Attachment Emotional ambivalence | Sense of damage and imperfection Feeling of rigidity Curiosity and fear | Isolation | Isolation | Discomfort with mixed textures |
| Quotes | “It would be soft and cuddly but the animal itself is also quite a predator so there’d always be that element of weariness… “ | “I hate the feel and texture of velvet; it’s dry and is a very unpleasant sensation… My experience in the ward is very unpleasant. Something like being exposed to sensory stimuli you don’t like the most.’’ | “Kinda sticky as in like you just want something to stop but it’s just there and it just sticks… Each day like it’s just there are going to be tough times every day… Because it’s cold, sometimes it can be helpful, but sometimes it’s like the worst thing you know.” | “It is rigid, and it has cracks. It’s got this problem. It should be complete, but it is damaged… Just the sense that there could be something inside that could be useful” | “A fat body trapped in a small space’‘ | “It’s a large circle, it’s blue, it’s cold, and it evokes feelings of being isolated because it’s distant.” | “It’s like bittersweet. But then the texture is also crunchy and slimy… If I hear a crunch in a smooth thing, it’ll really upset me.” |
| Participants | P5 | P2 | P4 | P3 | P6 | P7 | P1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chubinidze, D.; Zesch, E.; Sarpong, A.; Li, Z.; Baillie, C.; Tchanturia, K. The Sensory Landscape and Embodied Experiences in Anorexia Nervosa Treatment: An Inpatient Sensory Ethnography. J. Clin. Med. 2024, 13, 7172. https://doi.org/10.3390/jcm13237172
Chubinidze D, Zesch E, Sarpong A, Li Z, Baillie C, Tchanturia K. The Sensory Landscape and Embodied Experiences in Anorexia Nervosa Treatment: An Inpatient Sensory Ethnography. Journal of Clinical Medicine. 2024; 13(23):7172. https://doi.org/10.3390/jcm13237172
Chicago/Turabian StyleChubinidze, Dimitri, Elisa Zesch, Amanda Sarpong, Zhuo Li, Claire Baillie, and Kate Tchanturia. 2024. "The Sensory Landscape and Embodied Experiences in Anorexia Nervosa Treatment: An Inpatient Sensory Ethnography" Journal of Clinical Medicine 13, no. 23: 7172. https://doi.org/10.3390/jcm13237172
APA StyleChubinidze, D., Zesch, E., Sarpong, A., Li, Z., Baillie, C., & Tchanturia, K. (2024). The Sensory Landscape and Embodied Experiences in Anorexia Nervosa Treatment: An Inpatient Sensory Ethnography. Journal of Clinical Medicine, 13(23), 7172. https://doi.org/10.3390/jcm13237172