


The Effect of the Cheneau Brace on Respiratory Function in Girls with Adolescent Idiopathic Scoliosis Participating in a Schroth Exercise Program

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
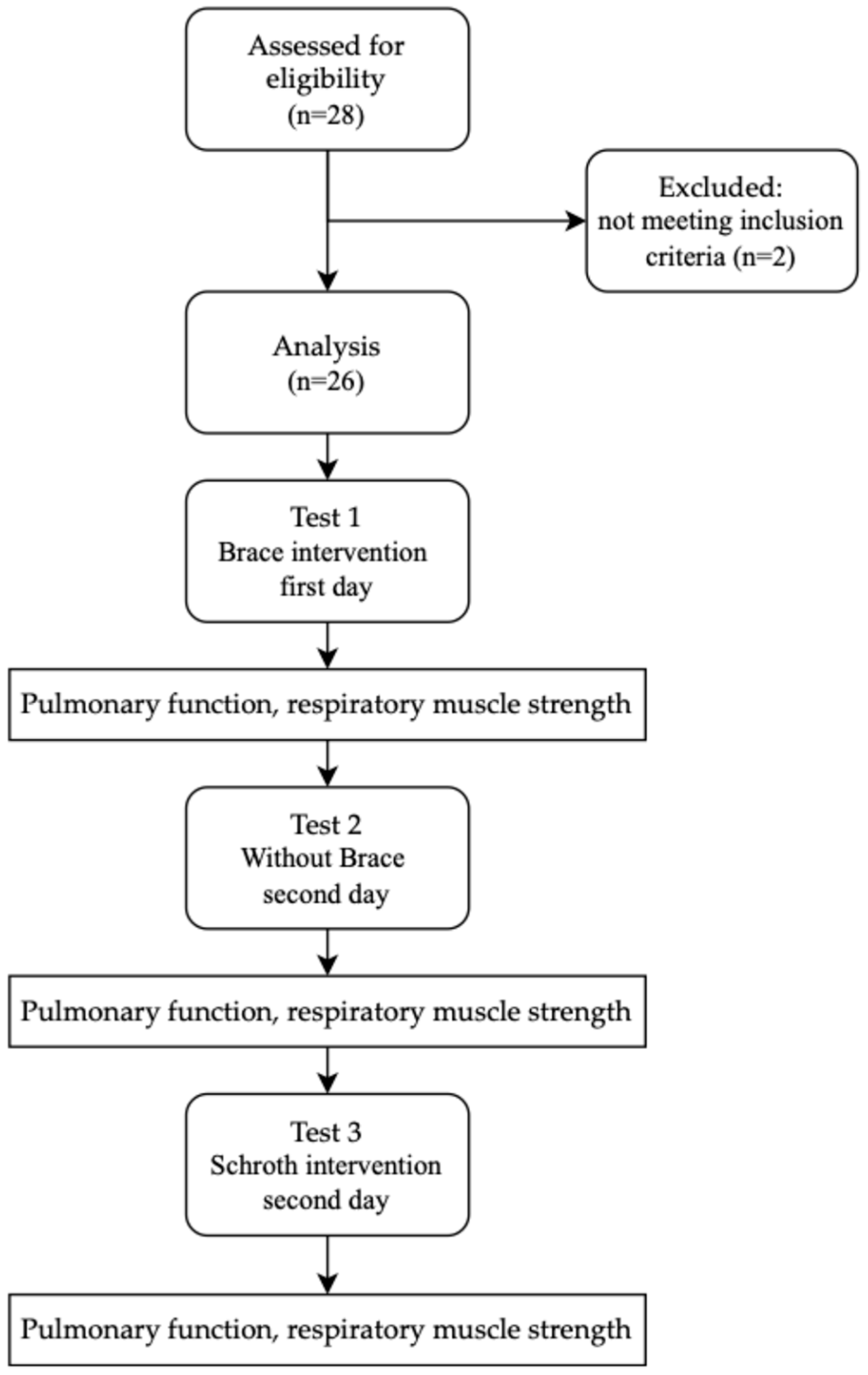
2.2. Experimental Procedure
2.2.1. Test 1—Brace Intervention—First Day of the Present Study
2.2.2. Test 2—Without the Brace—The Day After the First Test
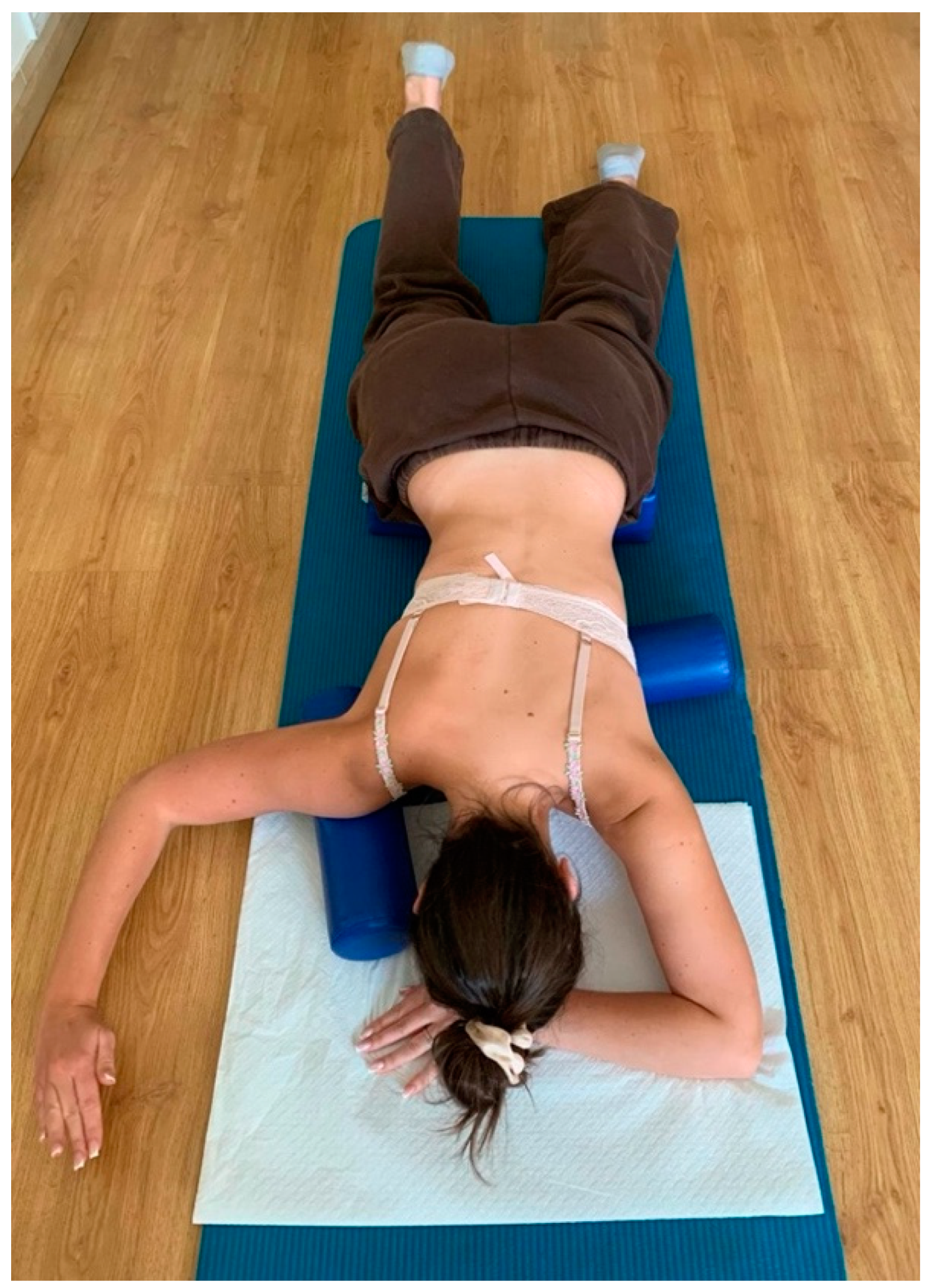
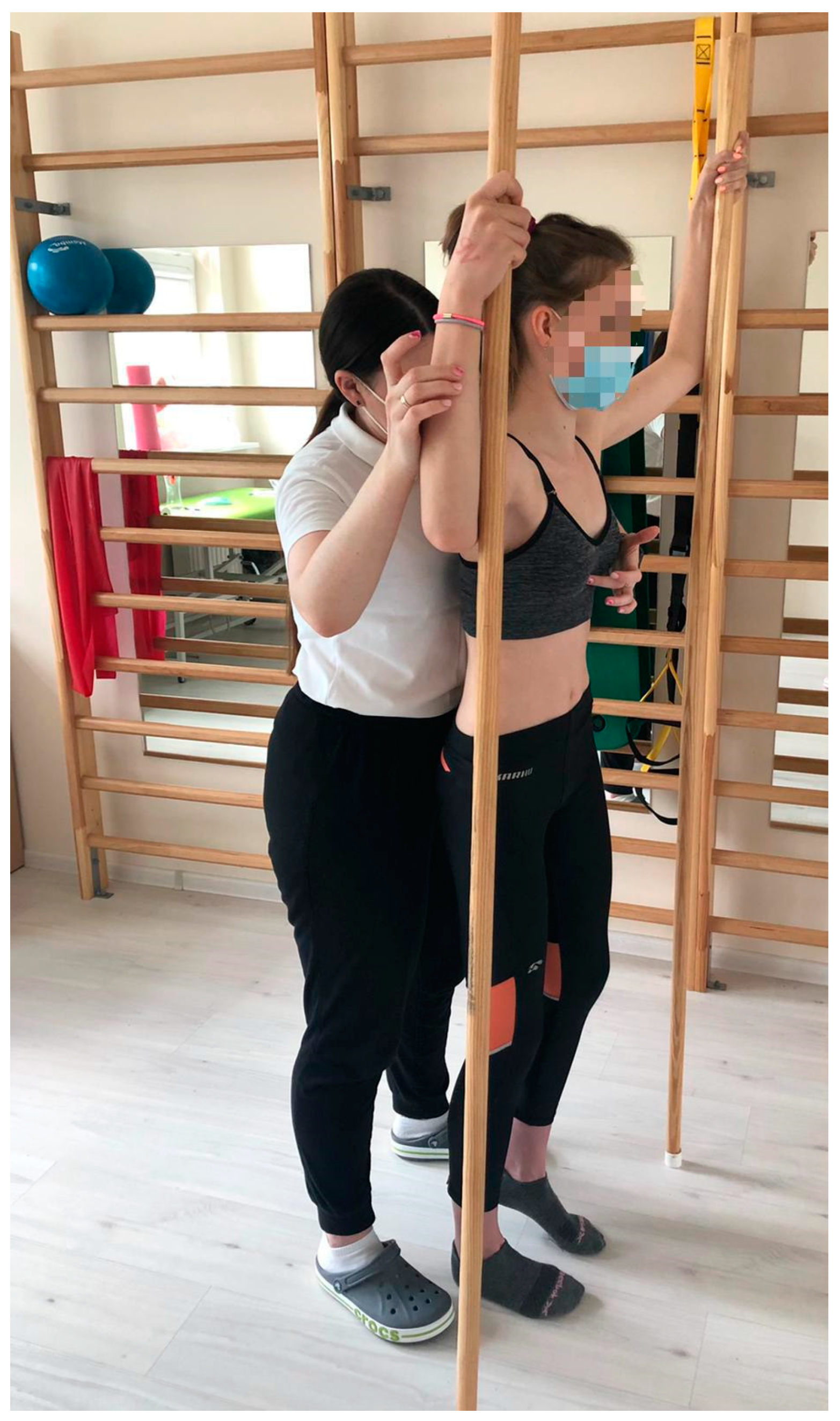
2.2.3. Test 3—Schroth Intervention—The Day After the First Test
2.3. Respiratory Examination
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Charles, Y.P.; Diméglio, A.; Marcoul, M.; Bourgin, J.F.; Marcoul, A.; Bozonnat, M.C. Influence of idiopathic scoliosis on three-dimensional thoracic growth. Spine 2008, 33, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Jandrić, S. Low back pain and scoliosis in adolescents. Pain Pract. 2016, 16, 93. [Google Scholar]
- de Baat, P.; van Biezen, E.C.; de Baat, C. Scoliose: Overzicht van typen, oorzaken, diagnostiek en behandeling 1 [Scoliosis: Review of types, aetiology, diagnostics, and treatment 1]. Ned. Tijdschr. Tandheelkd. 2012, 119, 474–478. [Google Scholar] [CrossRef]
- Thomas, J.J.; Stans, A.A.; Milbrandt, T.A.; Kremers, H.M.; Shaughnessy, W.J.; Larson, A.N. Trends in Incidence of Adolescent Idiopathic Scoliosis: A Modern US Population-based Study. J. Pediatr. Orthop. 2021, 41, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Nie, Q.; Liu, J.; Jiang, Z. Prevalence of scoliosis in children and adolescents: A systematic review and meta-analysis. Front. Pediatr. 2024, 12, 1399049. [Google Scholar] [CrossRef]
- Blachnio, K.; Kopcial, S.; Piecuch, D.; Hanczyk, E. Conservative treatment of adolescent idiopathic scoliosis (AIS): A narrative review of current evidence and implications for clinical practice. Qual. Sport 2024, 22, 54352. [Google Scholar] [CrossRef]
- Kinikli, G.I.; Apaydın, Z.B.; Beydağı, M.G.; Bozgeyik, S.; vGuney, H.; Demirkiran, G. Body image disturbance in patients with adolescent idiopathic scoliosis: Correlation with deformity perception, trunk aesthetic, and quality of life. J. Exerc. Ther. Rehabil. 2022, 9, 125–132. [Google Scholar] [CrossRef]
- Rafferty, A.; Fleming, N.; Kiely, P.; Mockler, D.; Dockrell, S. Does exercise therapy improve pulmonary function in patients with Adolescent Idiopathic Scoliosis? Physiother. Theory Pract. 2022, 39, 1095–1105. [Google Scholar] [CrossRef]
- Yagci, G.; Demirkiran, G.; Yakut, Y. In-brace alterations of pulmonary functions in adolescents wearing a brace for idiopathic scoliosis. Prosthet. Orthot. Int. 2019, 43, 434–439. [Google Scholar] [CrossRef]
- Newton, P.O.; Faro, F.D.; Gollogly, S.; Betz, R.R.; Lenke, L.G.; Lowe, T.G. Results of preoperative pulmonary function testing of adolescents with idiopathic scoliosis. A study of six hundred and thirty-one patients. J. Bone Jt. Surg. Am. 2005, 87, 1937–1946. [Google Scholar] [CrossRef]
- Johnston, C.E.; Richards, B.S.; Sucato, D.J.; Bridwell, K.H.; Lenke, L.G.; Erickson, M.; Spinal Deformity Study Group. Correlation of preoperative deformity magnitude and pulmonary function tests in adolescent idiopathic scoliosis. Spine 2011, 36, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Spratt, K.F.; Peterson, K.K.; Spoonamore, M.J.; Ponseti, I.V. Health and function of patients with untreated idiopathic scoliosis: A 50-year natural history study. JAMA 2003, 289, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Lonstein, J.E. Scoliosis: Surgical versus nonsurgical treatment. Clin. Orthop. Relat. Res. 2006, 443, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Tsiligiannis, T.; Grivas, T. Pulmonary function in children with idiopathic scoliosis. Scoliosis 2012, 7, 7. [Google Scholar] [CrossRef]
- Karol, L.A.; Johnston, C.; Mladenov, K.; Schochet, P.; Walters, P.; Browne, R.H. Pulmonary function following early thoracic fusion in non-neuromuscular scoliosis. J. Bone Jt. Surg. Am. 2008, 90, 1272–1281. [Google Scholar] [CrossRef]
- Visconti, R.D.R.; Cossich, V.R.A.; Aquino, J.D.; Laett, C.T.; de Mantos Santos, L.; Carelli, L.E.; de Barros, A.G.C.; de Souza Portes Meirelles, R.; Gavilao, U.F.; da Silva, S.C. Cardiorespiratory function of patients with adolescent idiopathic scoliosis. Coluna/Columna 2021, 20, 89–95. [Google Scholar] [CrossRef]
- Martínez-Llorens, J.R.M.; Ramírez, M.; Colomina, M.J.; Bagó, J.; Molina, A.; Cáceres, E.; Gea, J. Muscle dysfunction and exercise limitation in adolescent idiopathic scoliosis. Eur. Respir. J. 2010, 36, 393–400. [Google Scholar] [CrossRef]
- Redding, G.; Mayer, O.H.; White, K.; Bompadre, V.; Emerson, J.; Krengel, W.; Campbell, R. Maximal respiratory muscle strength and vital capacity in children with early onset scoliosis. Spine 2017, 42, 1799–1804. [Google Scholar] [CrossRef]
- Flores, F.; Cavaleiro, J.; Lopes, A.A.; Ribeiro, F.; Oliveira, A. Preoperative pulmonary function and respiratory muscle strength in Portuguese adolescents with idiopathic scoliosis. Rev. Port. Pneumol. 2006, 22, 52–53. [Google Scholar] [CrossRef]
- Saraiva, B.M.A. Impact of scoliosis severity on functional capacity in patients with adolescent ıdiopathic scoliosis. Pediatr. Exerc. Sci. 2018, 30, 243–250. [Google Scholar] [CrossRef]
- dos Santos Alves, V.L.; Stiburov, R.; Avanzi, O. Impact of a physical rehabilitation program on the respiratory function of adolescents with idiopathic scoliosis. Chest 2006, 130, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.; Garrido, E. Effect of idiopathic thoracic scoliosis on the tracheobronchial tree. BMJ Open Respir. Res. 2018, 5, e000264. [Google Scholar] [CrossRef] [PubMed]
- Redding, G.J. Early Onset Scoliosis: A Pulmonary Perspective. Spine Deform. 2014, 2, 425–429. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, D.; Zhang, G.; Ma, B.; Ma, Y.; Yang, Y.; Xing, S.; Kang, X.; Gao, B. Effects of spinal deformities on lung development in children: A review. J. Orthop. Surg. Res. 2023, 18, 246. [Google Scholar] [CrossRef]
- Sancho-Chust, J.N.; Chiner, E.; Camarasa, A.; Senent, C. Differences in pulmonary function based on height prediction obtained by using alternative measures. Respiration 2010, 79, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Sousa, C.M.S.; Pessoa, A.L.C.; Carelli, L.E.; Ribeiro, C.O.; Lopes, A.J.; Melo, P.L. Respiratory oscillometry and functional analyses in patients with idiopathic scoliosis. Braz. J. Med. Biol. Res. 2023, 56, e12898. [Google Scholar] [CrossRef]
- Karaali, E.; Çiloğlu, O.; Görgülü, F.F.; Ekiz, T. Ultrasonographic measurement of diaphragm thickness in patients with severe thoracic scoliosis. J. Ultrasound. 2021, 24, 75–79. [Google Scholar] [CrossRef]
- Çimen, O.; Öner, A.; Köksal, A.; Dirvar, F.; Mert, M. Evaluation of the Parameters Affecting Respiratory Functions at Adolescent Idiopathic Scoliosis Patients. Clin. Spine Surg. 2022, 35, E236–E241. [Google Scholar] [CrossRef] [PubMed]
- Grivas, T.B.; Negrini, S.; Aubin, C.E.; Aulisa, A.G.; De Mauroy, J.C.; Donzelli, S.; Hresko, M.T.; Kotwicki, T.; Lou, E.; Maruyama, T.; et al. Nonoperative management of adolescent idiopathic scoliosis (AIS) using braces. Prosthet. Orthot. Int. 2022, 46, 383–391. [Google Scholar] [CrossRef]
- Negrini, S.; Aulisa, A.G.; Aulisa, L.; Circo, A.B.; de Mauroy, J.C.; Durmala, J.; Grivas, T.B.; Knott, P.; Kotwicki, T.; Maruyama, T.; et al. 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 2012, 7, 3. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Bettany-Saltikov, J.; Parent, E.; Romano, M.; Villagrasa, M.; Negrini, S. Physiotherapeutic scoliosis-specific exercises for adolescents with idiopathic scoliosis. Eur. J. Phys. Rehabil. Med. 2014, 50, 111–121. [Google Scholar] [PubMed]
- Ceballos Laita, L.; Tejedor Cubillo, C.; Mingo Gómez, T.; Jiménez Del Barrio, S. Effects of corrective, therapeutic exercise techniques on adolescent idiopathic scoliosis. A systematic review. Arch. Argent Pediatr. 2018, 116, e582–e589. [Google Scholar]
- Schreiber, S.; Parent, E.C.; Hill, D.L.; Hedden, D.M.; Moreau, M.J.; Southon, S.C. Patients with adolescent idiopathic scoliosis perceive positive improvements regardless of change in the Cobb angle–Results from a randomized controlled trial comparing a 6-month Schroth intervention added to standard care and standard care alone. SOSORT 2018 Award winner. BMC Musculoskelet. Disord. 2019, 20, 319. [Google Scholar]
- Fusco, C.; Zaina, F.; Atanasio, S.; Romano, M.; Negrini, A.; Negrini, S. Physical exercises in the treatment of adolescent idiopathic scoliosis: An updated systematic review. Physiother. Theory Pract. 2011, 27, 80–114. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xu, T.; Zhou, J.; Han, B.; Wu, Q.; Jin, W.; Zhang, X. The Superiority of Schroth Exercise Combined Brace Treatment for Mild-to-Moderate Adolescent Idiopathic Scoliosis: A Systematic Review and Network Meta-Analysis. World Neurosurg. 2024, 186, 184–196.e9. [Google Scholar] [CrossRef]
- Çetinkaya, İ.; Kuru Çolak, T.; Saka, S.; Korkmaz, M.F. Respiratory function and respiratory muscle strength in adolescent idiopathic scoliosis. Spine Deform. 2024, 12, 635–641. [Google Scholar] [CrossRef]
- Yurt, Y.; Yatar, İ.; Malkoç, M.; Yakut, Y.; Mıhçıoğlu, S.; Koltak, C. The effect of brace treatment on pulmonary functions in adolescent idiopathic scoliosis: An 8-month follow-up study. J. Back Musculoskelet. Rehabil. 2021, 34, 887–893. [Google Scholar] [CrossRef]
- Ran, B.; Fan, Y.; Yuan, F.; Guo, K.; Zhu, X. Pulmonary function changes and its influencing factors after preoperative brace treatment in patients with adolescent idiopathic scoliosis: A retrospective case-control study. Medicine 2016, 95, e5088. [Google Scholar] [CrossRef]
- Piątek, E.; Kuczyński, M.; Ostrowska, B. Postural control in girls with adolescent idiopathic scoliosis while wearing a Chêneau brace or performing active self-correction: A pilot study. PeerJ 2019, 7, e7513. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Caruso, P.; Albuquerque, A.L.; Santana, P.V.; Cardenas, L.Z.; Ferreira, J.G.; Prina, E.; Trevizan, P.F.; Pereira, M.C.; Iamonti, V.; Pletsch, R.; et al. Diagnostic methods to assess inspiratory and expiratory muscle strength. J. Bras. Pneumol. 2015, 41, 110–123. [Google Scholar] [CrossRef]
- Laveneziana, P.; Albuquerque, A.; Aliverti, A.; Babb, T.; Barreiro, E.; Dres, M.; Dubé, B.P.; Fauroux, B.; Gea, J.; Guenette, J.A.; et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur. Respir. J. 2019, 53, 1801214. [Google Scholar] [CrossRef] [PubMed]
- Hariri, L.P.; Smith, M.L.; Mino-Kenudson, M.; Allen, T.C.; Attanoos, R.; Borczuk, A.; Burke, L.; Cagle, P.T.; Capelozzi, V.; Dacic, S.; et al. Pulmonary Pathology Society Perspective on the 2018 American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society Idiopathic Pulmonary Fibrosis Clinical Practice Guidelines. Ann. Am. Thorac. Soc. 2020, 17, 550–554. [Google Scholar] [CrossRef]
- Cooper, B.G. An update on contraindications for lung function testing. Thorax 2011, 66, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Kennedy, J.D.; Robertson, C.F.; Hudson, I.; Phelan, P.D. Effect of bracing on respiratory mechanics in mild idiopathic scoliosis. Thorax 1989, 44, 548–553. [Google Scholar] [CrossRef]
- Abdelaal, A.A.M.; Abd El Kafy, E.M.A.E.S.; Elayat, M.S.E.M.; Sabbahi, M.; Badghish, M.S.S. Changes in pulmonary function and functional capacity in adolescents with mild idiopathic scoliosis: Observational cohort study. J. Int. Med. Res. 2018, 46, 381–391. [Google Scholar] [CrossRef]
- Gao, C.; Zheng, Y.; Fan, C.; Yang, Y.; He, C.; Wong, M. Could the clinical effectiveness be improved under the integration of orthotic intervention and scoliosis-specific exercise in managing adolescent idiopathic scoliosis: A randomized controlled trial study. Am. J. Phys. Med. Rehabil. 2019, 98, 642–648. [Google Scholar] [CrossRef]
- Otman, S.; Kose, N.; Yakut, Y. The efficacy of Schroth s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey. Saudi Med. J. 2005, 26, 1429–1435. [Google Scholar]
- Kim, M.J.; Park, D.S. The effect of Schroth’s three-dimensional exercises in combination with respiratory muscle exercise on Cobb’s angle and pulmonary function in patients with idiopathic scoliosis. Phys. Ther. Rehabil. Sci. 2017, 6, 113–119. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Mikelatou, K.; Boutis, A.; Tsafantakis, E.; Mermiri, D.-Z. Assessment of respiratory function in adolescents with idiopathic scoliosis treated with brace. Eur. Respir. J. 2018, 52, PA4580. [Google Scholar]
- Lehnert-Schroth, C. The “four-curved” scoliosis. The effect on the additional lumbosacral spinal curve by the three dimensional Schroth’s scoliosis treatment. ZFA Z. Fur Allg. 1981, 57, 2227–2231. [Google Scholar]
- Barrios, C.; Pérez-Encinas, C.; Maruenda, J.I.; Laguía, M. Significant ventilatory functional restriction in adolescents with mild or moderate scoliosis during maximal exercise tolerance test. Spine 2005, 30, 1610–1615. [Google Scholar] [CrossRef]
- Campbell, R.M., Jr.; Smith, M.D.; Mayes, T.C.; Mangos, J.A.; Willey-Courand, D.B.; Kose, N.; Pinero, R.F.; Alder, M.E.; Duong, H.L.; Surber, J.L. The effect of opening wedge thoracostomy on thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis. J. Bone Jt. Surg. Am. 2004, 86-A, 1659–1674. [Google Scholar] [CrossRef]
- Liu, W.; Ma, C.Z.; Luo, C.L.; Li, Y.Y.; Wu, H.D. Effect of Schroth Exercise on Pulmonary Function and Exercise Capacity in Patients with Severe Adolescent Idiopathic Scoliosis. In Proceedings of the 12th Asian-Pacific Conference on Medical and Biological Engineering, APCMBE 2023. IFMBE Proceedings, Suzhou, China, 18–21 May 2023; Wang, G., Yao, D., Gu, Z., Peng, Y., Tong, S., Liu, C., Eds.; Springer: Cham, Switzerland, 2024; Volume 104. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with AIS (n = 26) | ||
|---|---|---|
| Age [years] | 15.7 ± 1.5 | |
| Height [cm] | 166.8 ± 6.1 | |
| Body mass [kg] | 53.6 ± 6.6 | |
| BMI [kg/m2] | 19.3 ± 2 | |
| AIS curve pattern | 84.6% R thoracic/L lumbar | 15.4% L thoracic/R lumbar |
| Primary Cobb angle [degrees] | 31.5 ± 7.9 | |
| Risser sign | 2.7 ± 1.8 | |
| Schroth therapy [months] | 26.2 ± 19.4 | |
| Brace treatment [months] | 25.9 ± 19.3 | |
| Variable | Test 1with Brace | Test 2Without the Brace | Test 3After Exercise | p * | p # | p ~ |
|---|---|---|---|---|---|---|
| X (SD) (95% CI) | X (SD) (95% CI) | X (SD) (95% CI) | ||||
| VC [l] | 2.6 ± 0.4 (2.4–2.7) | 2.8 ± 0.5 (2.6–3.0) | 2.8 ± 0.4 (2.6–0.3) | <0.001 * a | 0.780 | <0.001 * b |
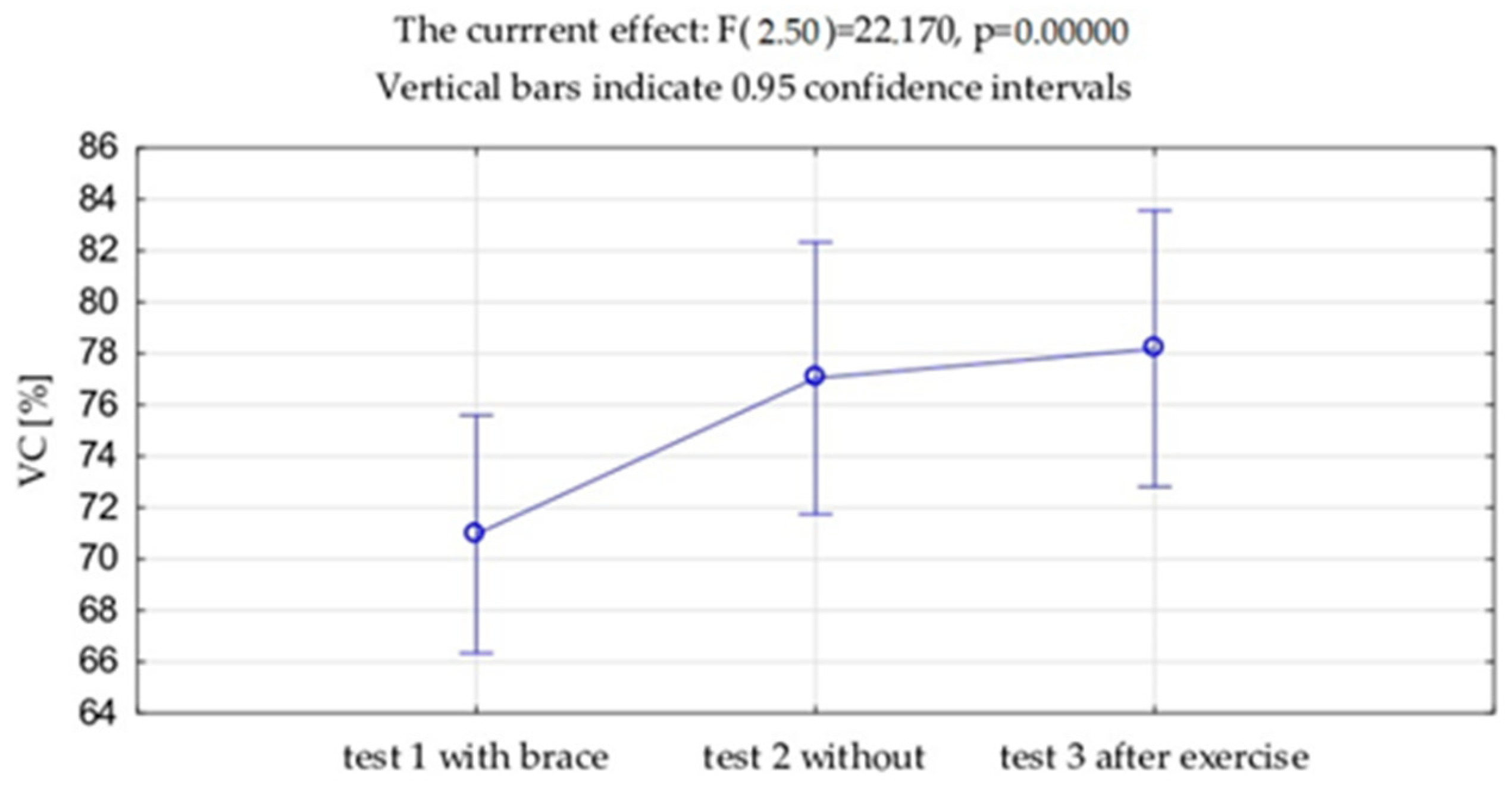
| VC [%] | 71.0 ± 11.4 (66.3–75.6) | 77.0 ± 13.1 (71.7–82.3) | 78.2 ± 13.3 (72.8–83.5) | <0.001 * b | 0.269 | <0.001 * b |
| FVC [l] | 2.7 ±0.5 (2.5–2.9) | 2.9 ± 0.5 (2.7–2.1) | 3.0 ± 0.5 (2.8–3.2) | 0.002 * a | 0.414 | <0.001 * b |
| FVC [%] | 74.4 ± 13.1 (69.1–79.7) | 80.9 ± 13.4 (75.4–86.3) | 82.3 ± 14.6 (76.4–88.2) | 0.002 * a | 0.331 | <0.001 * b |
| FEV1 [l] | 2.5 ± 0.5 (2.3–2.7) | 2.6 ± 0.5 (2.4–2.8) | 2.7 ± 0.5 (2.4–2.9) | 0.05 * a | 0.492 | 0.016 * a |
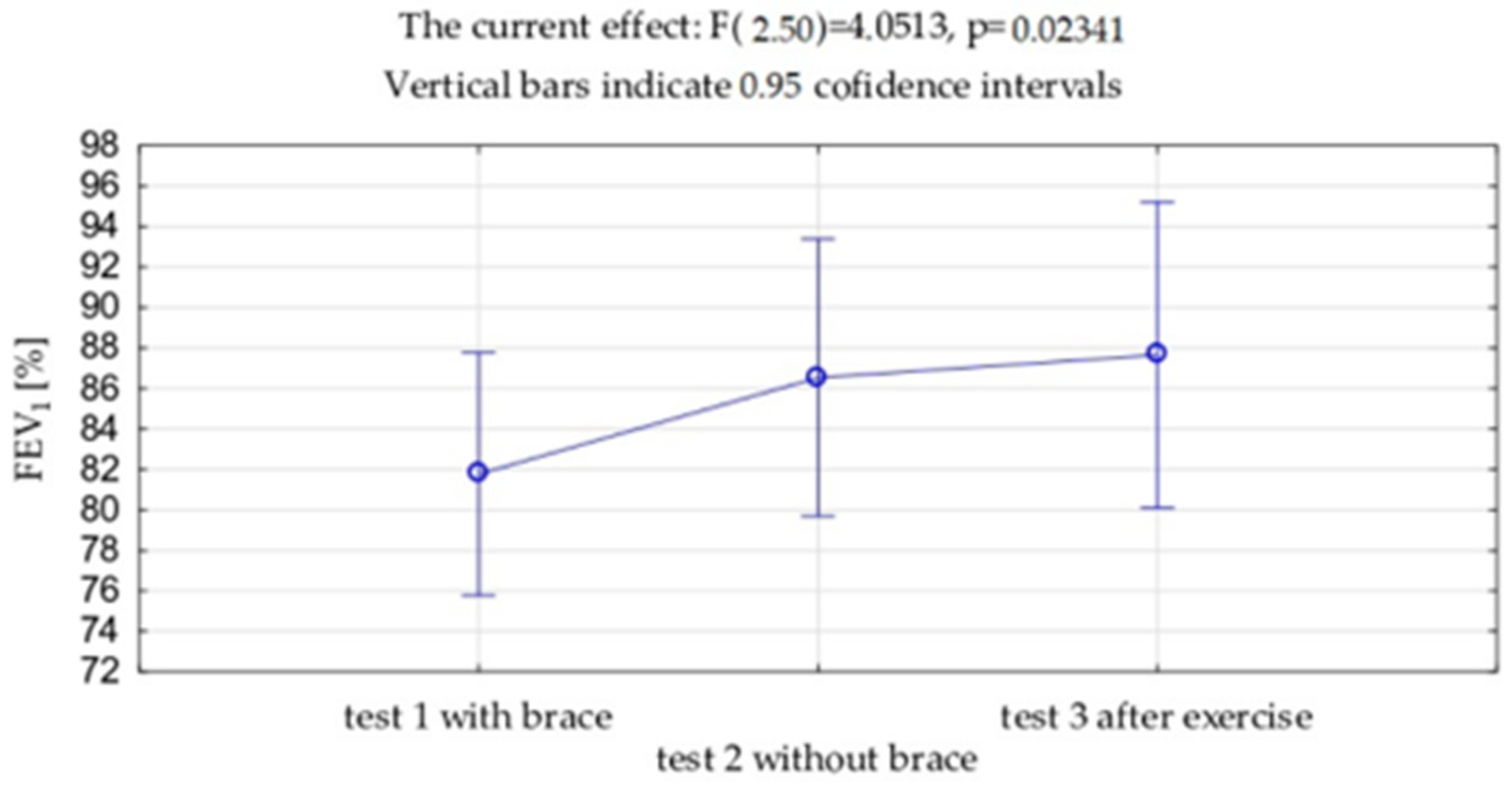
| FEV1 [%] | 81.8 ± 14.8 (75.7–87.7) | 86.5 ± 16.9 (79.6–93.3) | 87.6 ± 18.7 (80.1–95.2) | 0.05 * a | 0.526 | 0.020 * a |
| FEV1%VC | 91.3 ± 8.5 (87.8–94.7) | 89.2 ± 9.3 (85.4–93.0) | 90.4 ± 10.2 (86.3–94.6) | 0.203 | 0.350 | 0.633 |
| PEF [L/s] | 4.6 ± 1.1 (4.1–5.0) | 4.6 ± 1.1 (4.1–5.0) | 4.8 ± 1.4 (4.2–5.3) | 0.937 | 0.283 | 0.318 |
| PEF [%] | 67.1 ± 15.6 (60.8–73.4) | 67.1 ± 16.0 (60.6–73.6) | 69.4 ± 19.4 (61.6–77.3) | 0.989 | 0.351 | 0.400 |
| MEF50 | 3.5 ± 1.0 (3.1–3.9) | 3.4 ± 1.2 (2.9–3.9) | 3.5 ± 1.2 (3.0–4.0) | 0.837 | 0.439 | 0.596 |
| MEF50 [%] | 82.9 ± 23.5 (73.4–92.3) | 82.2 ± 27.9 (70.9–93.5) | 83.0 ± 27.2 (72.0–94.0) | 0.838 | 0.821 | 0.965 |
| MEF25 | 2.1 ± 0.7 (1.8–2.4) | 2.1 ± 0.8 (1.7–2.4) | 2.1 ± 0.7 (1.8–2.3) | 0.725 | 0.829 | 0.923 |
| MEF25 [%] | 98.3 ± 35.2 (84.1–112.5) | 93.4 ± 40.6 (77.0–109.8) | 93.6 ± 31.8 (80.7–106.4) | 0.725 | 0.985 | 0.288 |
| Test 1 with Brace | Test 2 Without the Brace | Test 3 After Exercise | p * | p # | p ~ | |
|---|---|---|---|---|---|---|
| X (SD) (95% CI) | X (SD) (95% CI) | X (SD) (95% CI) | ||||
| PImax [kPa] | 4.4 ± 1.7 (3.7–5.1) | 4.0 ± 1.6 (3.4–4.7) | 4.5 ± 1.7 (3.9–5.2) | 0.028 * a | 0.009 * a | 0.706 |
| PImax [%] | 73.4 ± 29.4 (61.6–85.3) | 67.3 ± 27.2 (56.3–78.2) | 73.8 ± 26.9 (62.9–84.2) | 0.055 * | 0.002 * | 0.911 |
| PEmax [kPa] | 6.2 ± 1.8 (5.4–6.9) | 5.9 ± 1.7 (5.1–6.6) | 6.1 ± 1.7 (5.4–6.8) | 0.210 | 0.368 | 0.825 |
| PImax (Test 1) | PImax (Test 2) | PImax (Test 3) | PEmax (Test 1) | PEmax (Test 2) | PEmax (Test 3) | |
|---|---|---|---|---|---|---|
| Schroth therapy [months] | 0.415 | 0.370 | 0.322 | 0.155 | 0.453 | 0.453 |
| Brace treatment [months] | 0.434 | 0.381 | 0.255 | 0.177 | 0.406 | 0.486 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badowska, A.; Okrzymowska, P.; Piatek-Krzywicka, E.; Ostrowska, B.; Rozek-Piechura, K. The Effect of the Cheneau Brace on Respiratory Function in Girls with Adolescent Idiopathic Scoliosis Participating in a Schroth Exercise Program. J. Clin. Med. 2024, 13, 7143. https://doi.org/10.3390/jcm13237143
Badowska A, Okrzymowska P, Piatek-Krzywicka E, Ostrowska B, Rozek-Piechura K. The Effect of the Cheneau Brace on Respiratory Function in Girls with Adolescent Idiopathic Scoliosis Participating in a Schroth Exercise Program. Journal of Clinical Medicine. 2024; 13(23):7143. https://doi.org/10.3390/jcm13237143
Chicago/Turabian StyleBadowska, Anna, Paulina Okrzymowska, Elzbieta Piatek-Krzywicka, Bozena Ostrowska, and Krystyna Rozek-Piechura. 2024. "The Effect of the Cheneau Brace on Respiratory Function in Girls with Adolescent Idiopathic Scoliosis Participating in a Schroth Exercise Program" Journal of Clinical Medicine 13, no. 23: 7143. https://doi.org/10.3390/jcm13237143
APA StyleBadowska, A., Okrzymowska, P., Piatek-Krzywicka, E., Ostrowska, B., & Rozek-Piechura, K. (2024). The Effect of the Cheneau Brace on Respiratory Function in Girls with Adolescent Idiopathic Scoliosis Participating in a Schroth Exercise Program. Journal of Clinical Medicine, 13(23), 7143. https://doi.org/10.3390/jcm13237143