


Predictive Value of Monocyte-To-Lymphocyte Ratio in Differentiating Heart Failure with Reduced Ejection Fraction in Patients with Severe Aortic Stenosis—A Retrospective Analysis

 , , , ,
, , , ,
Abstract

1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
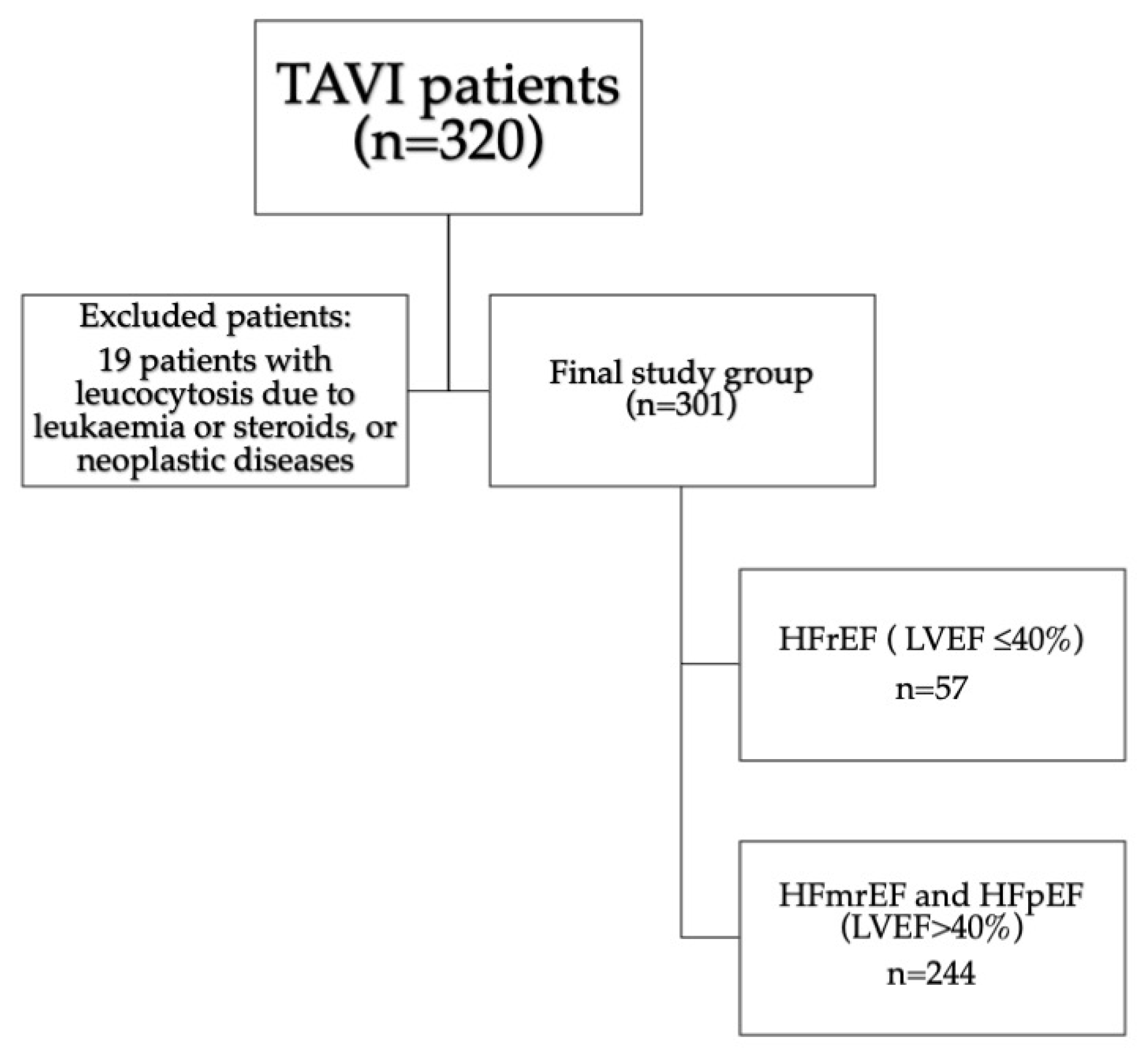
3.1. Patients Characteristics
3.2. Uni and Multivariable Analysis
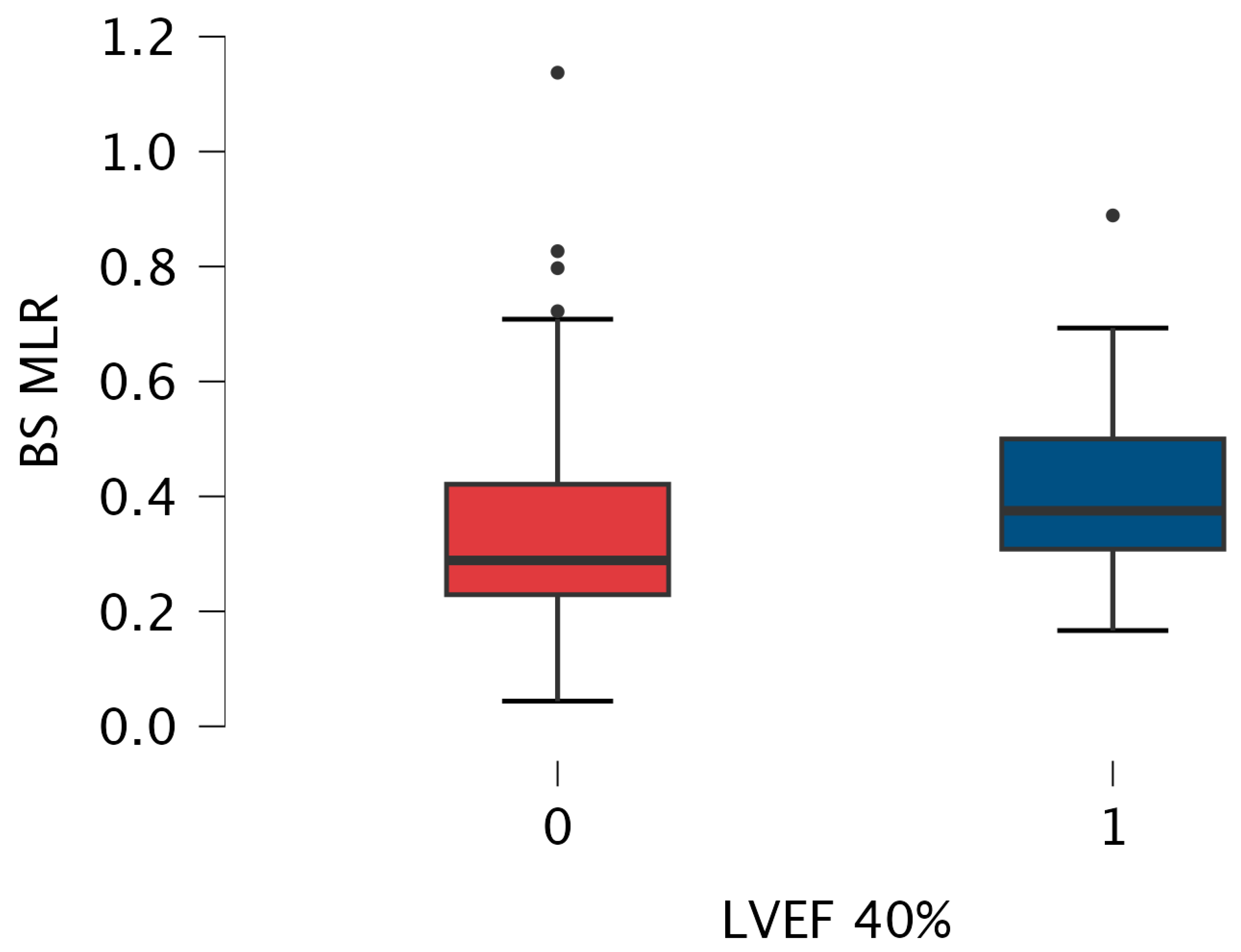
3.3. MLR and NTproBNP Comparisons between Subgroups (Figure 3)
3.4. Sub-Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akahori, H.; Tsujino, T.; Masuyama, T.; Ishihara, M. Mechanisms of aortic stenosis. J. Cardiol. 2018, 71, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Zerebiec, K.; Rożanowska, A.; Czestkowska, E.; Długosz, D.; Chyrchel, B.; Surdacki, A. Is left ventricular hypertrophy a friend or foe of patients with aortic stenosis? Postep. Kardiol Interwencyjne 2018, 14, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Protasiewicz, M. Transcatheter aortic valve replacement beneficial in patients with severely reduced left ventricle ejection fraction: Does the type of valve also matter? ESC Hear. Fail. 2024, 11, 1813–1815. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Orwat, S.; Kaleschke, G.; Kerckhoff, G.; Radke, R.; Baumgartner, H. Low flow, low gradient severe aortic stenosis: Diagnosis, treatment and prognosis. EuroIntervention 2013, 9, S38–S42. [Google Scholar] [CrossRef]
- Camarzana, A.; Annweiler, C.; Pinaud, F.; Abi-Khalil, W.; Rouleau, F.; Duval, G.; Prunier, F.; Furber, A.; Biere, L. Prognostic value of a comprehensive geriatric assessment for predicting one-year mortality in presumably frail patient with symptomatic aortic stenosis. Arch. Med Sci. 2021, 18, 1446–1452. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sanz, A.P.; Gómez, J.L.Z. How to improve patient outcomes following TAVI in 2024? Recent advances. Kardiologia Polska 2024, 82, 696–701. [Google Scholar] [CrossRef]
- Fraccaro, C.; Al-Lamee, R.; Tarantini, G.; Maisano, F.; Napodano, M.; Montorfano, M.; Frigo, A.C.; Iliceto, S.; Gerosa, G.; Isabella, G.; et al. Transcatheter aortic valve implantation in patients with severe left ventricular dysfunction: Immediate and mid-term results, a multicenter study. Circ. Cardiovasc. Interv. 2012, 5, 253–260. [Google Scholar] [CrossRef]
- Reichl, J.J.; Stolte, T.; Tang, S.; Boeddinghaus, J.; Wagener, M.; Leibundgut, G.; Kaiser, C.A.; Nestelberger, T. Prognostic Impact of Left Ventricular Ejection Fraction Improvement after Transcatheter Aortic Valve Replacement. J. Clin. Med. 2024, 13, 3639. [Google Scholar] [CrossRef]
- Spilias, N.; Martyn, T.; Denby, K.J.; Harb, S.C.; Popovic, Z.B.; Kapadia, S.R. Left Ventricular Systolic Dysfunction in Aortic Stenosis: Pathophysiology, Diagnosis, Management, and Future Directions. Struct. Hear. 2022, 6, 100089. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, G.; Apostolos, A.; Drakopoulou, M.; Simopoulou, C.; Karmpalioti, M.; Toskas, P.; Stathogiannis, K.; Xanthopoulou, M.; Ktenopoulos, N.; Latsios, G.; et al. Long-Term Outcomes of Aortic Stenosis Patients with Different Flow/Gradient Patterns Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2024, 13, 1200. [Google Scholar] [CrossRef] [PubMed]
- Decotto, S.; Villar, G.F.; Knorre, M.E.; Bergier, M.; Orellano, A.; Vega, B.S.; Busnelli, G.; Rossi, E.; Del Castillo, S.; Falconi, M.; et al. Surgical aortic valve replacement in patients with reduced ejection fraction. Prevalence and follow-up. Curr. Probl. Cardiol. 2024, 49, 102725. [Google Scholar] [CrossRef] [PubMed]
- Benck, K.N.; Nesbitt, K.; Dranow, E.; Glotzbach, J.P.; Tandar, A.; Pereira, S.J. Transcatheter Aortic Valve Replacement Improves Quality of Life and Ventricular Function With Low-Flow/Low-Gradient Aortic Stenosis. J. Soc. Cardiovasc. Angiogr. Interv. 2024, 3, 101266. [Google Scholar] [CrossRef] [PubMed]
- Bain, E.R.; George, B.; Jafri, S.H.; Rao, R.A.; Sinha, A.K.; Guglin, M.E. Outcomes in patients with aortic stenosis and severely reduced ejection fraction following surgical aortic valve replacement and transcatheter aortic valve replacement. J. Cardiothorac. Surg. 2024, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Elmariah, S.; Palacios, I.F.; McAndrew, T.; Hueter, I.; Inglessis, I.; Baker, J.N.; Kodali, S.; Leon, M.B.; Svensson, L.; Pibarot, P.; et al. Outcomes of Transcatheter and Surgical Aortic Valve Replacement in High-Risk Patients With Aortic Stenosis and Left Ventricular Dysfunction: Results from the Placement of Aortic Transcatheter Valves [PARTNER] trial [cohort A]. Circ. Cardiovasc. Interv. 2013, 6, 604–614. [Google Scholar] [CrossRef]
- Aronow, W.S.; Salahuddin, A.; Spevack, D.M. At what flow rate does aortic valve gradient become severely elevated? Implications for guideline recommendations on aortic valve area cutoffs. Arch. Med Sci. 2024, 20, 713–718. [Google Scholar] [CrossRef]
- Grodecki, K.; Olasińska-Wiśniewska, A.; Cyran, A.; Urbanowicz, T.; Kwieciński, J.; Geers, J.; Tamarappoo, B.K.; Perek, B.; Gocoł, R.; Nawara-Skipirzepa, J.; et al. Quantification of Aortic Valve Fibrotic and Calcific Tissue from CTA: Prospective Comparison with Histology. Radiology 2024, 312, e240229. [Google Scholar] [CrossRef]
- Ambrosino, P.; Marcuccio, G.; Manzo, F.; Mancusi, C.; Merola, C.; Maniscalco, M. The Clinical Application of Established and Emerging Biomarkers for Chronic Respiratory Diseases. J. Clin. Med. 2023, 12, 6125. [Google Scholar] [CrossRef]
- Shahim, B.; Redfors, B.; Lindman, B.R.; Chen, S.; Dahlen, T.; Nazif, T.; Kapadia, S.; Gertz, Z.M.; Crowley, A.C.; Li, D.; et al. Neutrophil-to-Lymphocyte Ratios in Patients Undergoing Aortic Valve Replacement: The PARTNER Trials and Registries. J. Am. Hear. Assoc. 2022, 11, e024091. [Google Scholar] [CrossRef]
- Curran, F.M.; Bhalraam, U.; Mohan, M.; Singh, J.S.; Anker, S.D.; Dickstein, K.; Doney, A.S.; Filippatos, G.; George, J.; Metra, M.; et al. Neutrophil-to-lymphocyte ratio and outcomes in patients with new-onset or worsening heart failure with reduced and preserved ejection fraction. ESC Hear. Fail. 2021, 8, 3168–3179. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Olasińska-Wiśniewska, A.; Michalak, M.; Perek, B.; Al-Imam, A.; Rodzki, M.; Witkowska, A.; Straburzyńska-Migaj, E.; Bociański, M.; Misterski, M.; et al. Pre-operative systemic inflammatory response index influences long-term survival rate in off-pump surgical revascularization. PLoS ONE 2022, 17, e0276138. [Google Scholar] [CrossRef] [PubMed]
- Olasińska-Wiśniewska, A.; Perek, B.; Grygier, M.; Urbanowicz, T.; Misterski, M.; Puślecki, M.; Stefaniak, S.; Stelmark, K.; Lesiak, M.; Jemielity, M. Increased neutrophil-to-lymphocyte ratio is associated with higher incidence of acute kidney injury and worse survival after transcatheter aortic valve implantation. Cardiol. J. 2021, 30, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Firut, A.; Margaritescu, D.N.; Turcu-Stiolica, A.; Bica, M.; Rotaru, I.; Patrascu, A.-M.; Radu, R.I.; Marinescu, D.; Patrascu, S.; Streba, C.T.; et al. Preoperative Immunocyte-Derived Ratios Predict Postoperative Recovery of Gastrointestinal Motility after Colorectal Cancer Surgery. J. Clin. Med. 2023, 12, 6338. [Google Scholar] [CrossRef]
- Cai, C.; Zeng, W.; Wang, H.; Ren, S. Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio [PLR] and Monocyte-to-Lymphocyte Ratio [MLR] as Biomarkers in Diagnosis Evaluation of Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Retrospective, Observational Study. Int. J. Chronic Obstr. Pulm. Dis. 2024, 19, 933–943. [Google Scholar] [CrossRef]
- Hu, Y.; Li, Y.; Xing, Z.; Cao, Y.; Long, H.; Guo, Y. Predictive score for in-hospital mortality in patients with severe acute exacerbations of chronic obstructive pulmonary disease. Arch. Med Sci. 2024. [Google Scholar] [CrossRef]
- Olasińska-Wiśniewska, A.; Urbanowicz, T.; Grodecki, K.; Kübler, P.; Perek, B.; Grygier, M.; Misterski, M.; Walczak, M.; Szot, M.; Jemielity, M. Monocyte-to-lymphocyte ratio correlates with parathyroid hormone concentration in patients with severe symptomatic aortic stenosis. Adv. Med Sci. 2023, 68, 396–401. [Google Scholar] [CrossRef]
- Liu, H.; Chen, S.; Song, S.; Wei, H.; Li, Y.; Wu, Y. Neutrophil-to-lymphocyte ratio and prognostic nutritional index in predicting composite endpoint of early safety following transcatheter aortic valve replacement. Adv. Clin. Exp. Med. 2025, 34. [Google Scholar] [CrossRef]
- Urbanowicz, T.; Michalak, M.; Olasińska-Wiśniewska, A.; Rodzki, M.; Krasińska, A.; Perek, B.; Krasiński, Z.; Jemielity, M. Monocyte/Lymphocyte Ratio and MCHC as Predictors of Collateral Carotid Artery Disease—Preliminary Report. J. Pers. Med. 2021, 11, 1266. [Google Scholar] [CrossRef]
- Hua, Y.; Sun, J.-Y.; Lou, Y.-X.; Sun, W.; Kong, X.-Q. Monocyte-to-lymphocyte ratio predicts mortality and cardiovascular mortality in the general population. Int. J. Cardiol. 2023, 379, 118–126. [Google Scholar] [CrossRef]
- Vakhshoori, M.; Nemati, S.; Sabouhi, S.; Shakarami, M.; Yavari, B.; Emami, S.A.; Bondariyan, N.; Shafie, D. Prognostic impact of monocyte-to-lymphocyte ratio in coronary heart disease: A systematic review and meta-analysis. J. Int. Med Res. 2023, 51, 03000605231204469. [Google Scholar] [CrossRef] [PubMed]
- Vakhshoori, M.; Nemati, S.; Sabouhi, S.; Tavakol, G.; Yavari, B.; Shakarami, M.; Bondariyan, N.; Emami, S.A.; Shafie, D. Selection of Monocyte-to-Lymphocyte Ratio [MLR] or Lymphocyte-to-Monocyte Ratio [LMR] as Best Prognostic Tool in Heart Failure: A Systematic Review. SN Compr. Clin. Med. 2023, 5, 227. [Google Scholar] [CrossRef]
- Shahid, F.; Lip, G.Y.; Shantsila, E. Role of Monocytes in Heart Failure and Atrial Fibrillation. J. Am. Hear. Assoc. 2018, 7, e007849. [Google Scholar] [CrossRef] [PubMed]
- Mueller, K.A.L.; Langnau, C.; Harm, T.; Sigle, M.; Mott, K.; Droppa, M.; Borst, O.; Rohlfing, A.-K.; Gekeler, S.; Günter, M.; et al. Macrophage Migration Inhibitory Factor Promotes Thromboinflammation and Predicts Fast Progression of Aortic Stenosis. Arter. Thromb. Vasc. Biol. 2024, 44, 2118–2135. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, Y.; Xu, L. Pharmacological therapy targeting the immune response in atherosclerosis. Int. Immunopharmacol. 2024, 141, 112974. [Google Scholar] [CrossRef]
- Lassalle, F.; Rosa, M.; Staels, B.; Van Belle, E.; Susen, S.; Dupont, A. Circulating Monocyte Subsets and Transcatheter Aortic Valve Replacement. Int. J. Mol. Sci. 2022, 23, 5303. [Google Scholar] [CrossRef]
- Ley, K.; Miller, Y.I.; Hedrick, C.C. Monocyte and macrophage dynamics during atherogenesis. Arter. Thromb. Vasc. Biol. 2011, 31, 1506–1516. [Google Scholar] [CrossRef]
- Radzyukevich, Y.V.; Kosyakova, N.I.; Prokhorenko, I.R. Participation of Monocyte Subpopulations in Progression of Experimental Endotoxemia [EE] and Systemic Inflammation. J. Immunol. Res. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Williams, H.; Mack, C.D.; Li, S.C.H.; Fletcher, J.P.; Medbury, H.J. Nature versus Number: Monocytes in Cardiovascular Disease. Int. J. Mol. Sci. 2021, 22, 9119. [Google Scholar] [CrossRef]
- Suthahar, S.S.A.; Nettersheim, F.S.; Alimadadi, A.; Wang, E.; Billitti, M.; Resto-Trujillo, N.; Roy, P.; Hedrick, C.C.; Ley, K.; Orecchioni, M.; et al. Olfr2-positive macrophages originate from monocytes proliferate in situ and present a pro-inflammatory foamy-like phenotype. Cardiovasc. Res. 2024, cvae153. [Google Scholar] [CrossRef]
- Patel, V.K.; Williams, H.; Li, S.C.H.; Fletcher, J.P.; Medbury, H.J. Monocyte Subset Recruitment Marker Profile Is Inversely Associated With Blood ApoA1 Levels. Front. Immunol. 2021, 12, 616305. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Xia, Y.; Shi, D.; Yang, L.; Xie, M.; Wang, Z.; Gao, F.; Shao, Q.; Ma, X.; Zhou, Y. Relation of Monocyte Number to Progression of Aortic Stenosis. Am. J. Cardiol. 2022, 171, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Navani, R.V.; Dayawansa, N.H.; Nanayakkara, S.; Palmer, S.; Noaman, S.; Htun, N.M.; Walton, A.S.; Peter, K.; Stub, D. Post-Procedure Monocyte Count Levels Predict Major Adverse Cardiovascular Events [MACE] Following Transcatheter Aortic Valve Implantation (TAVI) for Aortic Stenosis. Hear. Lung Circ. 2024, 33, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, G.G.; Stortecky, S.; Meier, B.; Windecker, S.; Wenaweser, P. Severe aortic stenosis and coronary artery disease. EuroIntervention 2013, 9, S63–S68. [Google Scholar] [CrossRef]
- Lunardi, M.; Bianchini, F.; Aurigemma, C.; Romagnoli, E.; Paraggio, L.; Bianchini, E.; Zito, A.; Trani, C.; Burzotta, F. When to perform percutaneous coronary interventions in TAVI patients? Recent advances. Kardiologia Polska 2024, 82, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Castrichini, M.; Vitrella, G.; De Luca, A.; Altinier, A.; Korcova, R.; Pagura, L.; Radesich, C.; Sinagra, G. Clinical impact of myocardial fibrosis in severe aortic stenosis. Eur. Hear. J. Suppl. 2021, 23, E147–E150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 LVEF ≤ 40% n = 57 | Group 2 LVEF > 40% n = 244 | p Value | |
|---|---|---|---|
| Age [years] [median, Q1–Q3] | 78 [71–82] | 80 [76–83] | 0.013 |
| Female sex [n, %] BMI [median, Q1–Q3] | 19 [33] 26.8 [22.8–28.7] | 149 [61.1] 27.2 [24.3–30.5] | <0.001 0.097 |
| EuroScore II [median, Q1–Q3] | 8.34 [5.77–16.11] | 4.57 [2.87–7.75] | 0.001 |
| DM [n, %] | 29 [50.9] | 95 [38.9] | 0.103 |
| HA [n, %] | 38 [66.7] | 189 [77.5] | 0.123 |
| COPD [n, %] | 11 [19.3] | 40 [16.4] | 0.563 |
| AF [n, %] | 20 [35.1] | 98 [40.2] | 0.548 |
| Coronary artery disease [n, %] | 36 [63.2] | 111 [45.5] | 0.019 |
| Previous myocardial infarction [n, %] | 31 [54.4] | 71 [29.1] | <0.001 |
| Previous PCI [n, %] | 13 [50] | 53 [42.7] | 0.522 |
| Previous CABG [n, %] | 19 [33.3] | 41 [16.8] | 0.009 |
| Previous stroke or TIA [n, %] | 8 [14] | 46 [18.9] | 0.449 |
| NYHA III–IV [n, %] | 54 [94.7] | 215 [88.1] | 0.230 |
| Mean transvalvular gradient [mmHg] [median, Q1–Q3] | 41 [35–52] | 58 [49–68] | <0.001 |
| Peak transvalvular gradient [mmHg] [median, Q1–Q3] | 70 [58–86] | 92 [81.5–109.1] | <0.001 |
| LVEF [%] [median, Q1–Q3] | 35 [25–40] | 60 [50–60] | <0.001 |
| PASP [mmHg] [median, Q1–Q3] | 46 [40–60] | 42 [35–50] | 0.003 |
| AVA [cm2] [median, Q1–Q3] | 0.7 [0.6–0.78] | 0.6 [0.5–0.7] | 0.193 |
| Group 1 LVEF ≤ 40% n = 57 | Group 2 LVEF > 40% n = 244 | p Value | |
|---|---|---|---|
| NTproBNP pg/mL | 6425 [3434–10,200] | 2080 [1015–4357.8] | <0.001 |
| GFR [ml/min/1.73 m2] [median, Q1–Q3] | 55 [38–66] | 55 [45–67] | 0.299 |
| Neu [10 × 9/L] [median, Q1–Q3] | 4.94 [4.31–6.15] | 4.7 [3.67–5.93] | 0.157 |
| Lymp [10 × 9/L] [median, Q1–Q3] | 1.48 [1.05–1.76] | 1.39 [1.08–1.82] | 0.736 |
| Mono [10 × 9/L] [median, Q1–Q3] | 0.52 [0.36–0.65] | 0.41 [0.33–0.53] | 0.003 |
| MLR [median, Q1–Q3] | 0.37 [0.29–0.47] | 0.30 [0.23–0.41] | 0.004 |
| NLR [median, Q1–Q3] | 3.68 [2.77–4.93] | 3.39 [2.39–4.54] | 0.132 |
| PLR [median, Q1–Q3] | 109 [99–123.9] | 128.6 [98.2–194.6] | 0.521 |
| Hemoglobin [mmol/L] [median, Q1–Q3] | 8.1 [7.6–8.9] | 7.9 [7.2–8.5] | 0.053 |
| Univariable Analysis | p | Multivariable Analysis | p | |
|---|---|---|---|---|
| Age | OR 0.95 [95%CI 0.91–0.99] | 0.014 | ||
| Female sex | OR 0.32 [95%CI 0.17–0.59] | <0.001 | OR 0.308, 95%CI 0.160–0.593 | <0.001 |
| BMI | OR 0.94 [95%CI 0.88–1.01] | 0.079 | ||
| AF | OR 0.81 [95%CI 0.44–1.47] | 0.48 | ||
| Coronary artery disease | OR 2.05 [95%CI 1.13–3.72] | 0.018 | ||
| Previous myocardial infarction | OR 2.9 [95%CI 1.61–5.24] | <0.001 | ||
| Previous CABG | OR 2.48 [95%CI 1.30–4.72] | 0.006 | ||
| HA | OR 0.32 [95%CI 0.31–1.09] | 0.091 | ||
| DM | OR 1.62 [95%CI 0.91–2.90] | 0.101 | ||
| COPD | OR 1.22 [95%CI 0.58–2.56] | 0.60 | ||
| NTproBNP | OR 1.00 [95%CI 1.00–1.00] | <0.001 | OR 1.000, 95%CI 1.000–1.000 | <0.001 |
| GFR | OR 0.99 [95%CI 0.98–1.01] | 0.26 | ||
| NLR | OR 1.08 [95%CI 0.95–1.22] | 0.25 | ||
| MLR | OR 14.35 [95%CI 2.88–71.45] | 0.001 | OR 7.393, 95%CI 1.363–40.091 | 0.020 |
| PLR | OR 1.00 [0.99–1.01] | 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olasińska-Wiśniewska, A.; Urbanowicz, T.; Perek, B.; Misterski, M.; Grodecki, K.; Grygier, M.; Straburzyńska-Migaj, E.; Jemielity, M. Predictive Value of Monocyte-To-Lymphocyte Ratio in Differentiating Heart Failure with Reduced Ejection Fraction in Patients with Severe Aortic Stenosis—A Retrospective Analysis. J. Clin. Med. 2024, 13, 6249. https://doi.org/10.3390/jcm13206249
Olasińska-Wiśniewska A, Urbanowicz T, Perek B, Misterski M, Grodecki K, Grygier M, Straburzyńska-Migaj E, Jemielity M. Predictive Value of Monocyte-To-Lymphocyte Ratio in Differentiating Heart Failure with Reduced Ejection Fraction in Patients with Severe Aortic Stenosis—A Retrospective Analysis. Journal of Clinical Medicine. 2024; 13(20):6249. https://doi.org/10.3390/jcm13206249
Chicago/Turabian StyleOlasińska-Wiśniewska, Anna, Tomasz Urbanowicz, Bartłomiej Perek, Marcin Misterski, Kajetan Grodecki, Marek Grygier, Ewa Straburzyńska-Migaj, and Marek Jemielity. 2024. "Predictive Value of Monocyte-To-Lymphocyte Ratio in Differentiating Heart Failure with Reduced Ejection Fraction in Patients with Severe Aortic Stenosis—A Retrospective Analysis" Journal of Clinical Medicine 13, no. 20: 6249. https://doi.org/10.3390/jcm13206249
APA StyleOlasińska-Wiśniewska, A., Urbanowicz, T., Perek, B., Misterski, M., Grodecki, K., Grygier, M., Straburzyńska-Migaj, E., & Jemielity, M. (2024). Predictive Value of Monocyte-To-Lymphocyte Ratio in Differentiating Heart Failure with Reduced Ejection Fraction in Patients with Severe Aortic Stenosis—A Retrospective Analysis. Journal of Clinical Medicine, 13(20), 6249. https://doi.org/10.3390/jcm13206249