
Semaglutide Treatment Effects on Liver Fat Content in Obese Subjects with Metabolic-Associated Steatotic Liver Disease (MASLD)

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Design of the Study
2.2. MR Spectroscopy and MR Imaging Examination
2.3. Body Composition
2.4. Characterization of Fatty Acid Profile of Very-Low-Density Lipoprotein (VLDL) Triglycerides
2.5. Biochemical Analyses
2.6. Statistics
3. Results
3.1. Subjects and Their Baseline Characteristics
3.2. Semaglutide Treatment Affects Body Weight and Liver Fat
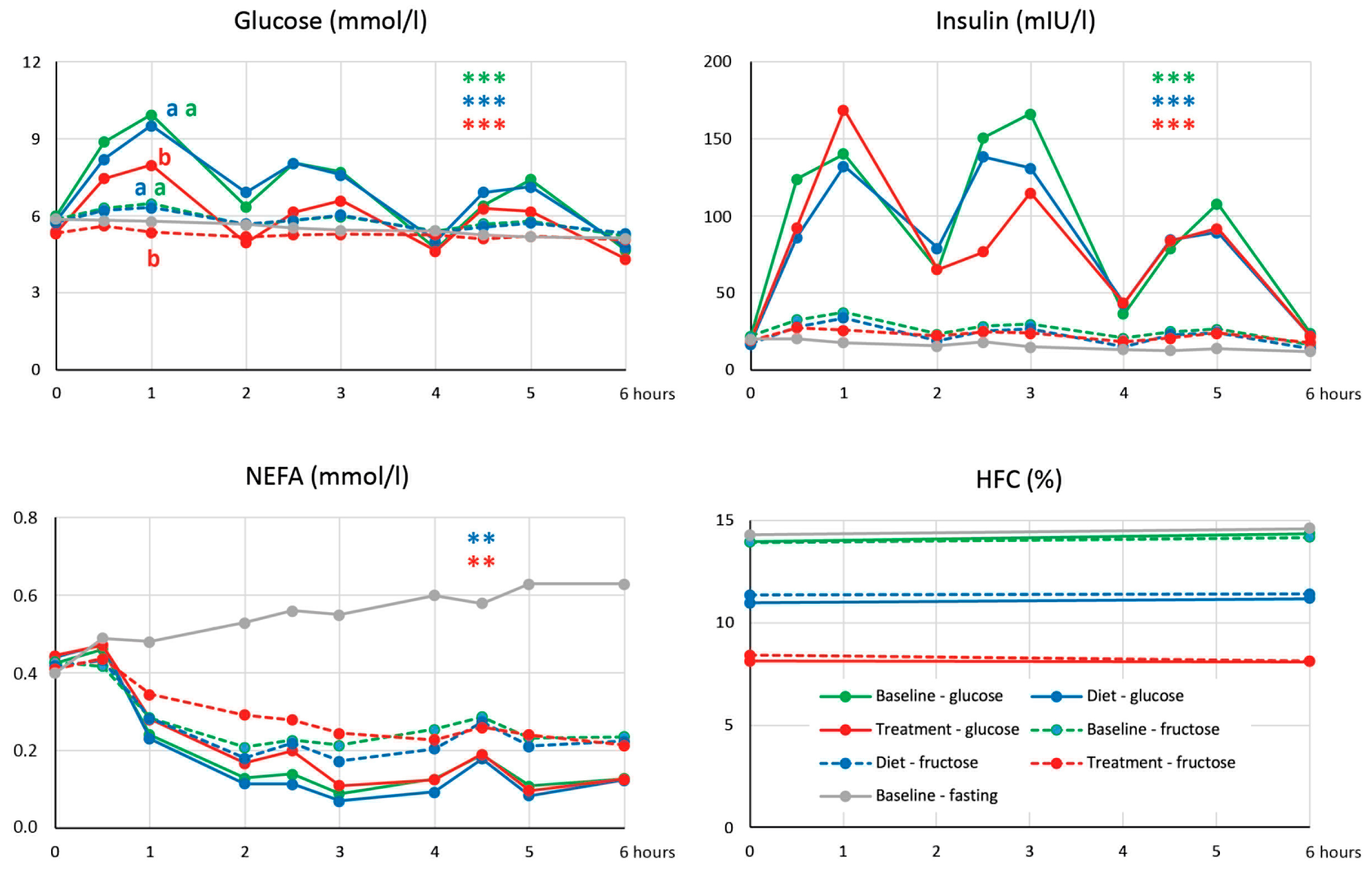
3.3. Semaglutide Treatment Does Not Affect Acute Changes of Liver Fat after Repeated Loads of Glucose and/or Fructose
3.4. Semaglutide Treatment Affects Glucoregulation
3.5. Semaglutide Treatment Affects Fatty Acid Profile of Plasma VLDL-TG
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): A systematic review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Amini-Salehi, E.; Letafatkar, N.; Norouzi, N.; Joukar, F.; Habibi, A.; Javid, M.; Sattari, N.; Khorasani, M.; Farahmand, A.; Tavakoli, S.; et al. Global prevalence of nonalcoholic fatty liver disease: An updated meta-analysis on 78 million population over 38 countries. Arch. Med. Res. 2024, 55, 103043. [Google Scholar] [CrossRef] [PubMed]
- Quek, J.; Chan, K.E.; Wong, Z.Y.; Tan, C.; Tan, B.; Lim, W.H.; Tan, D.J.H.; Tang, A.S.P.; Tay, P.; Xiao, J.; et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2023, 8, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Paklar, N.; Mijic, M.; Filipec-Kanizaj, T. The Outcomes of Liver Transplantation in Severe Metabolic Dysfunction-Associated Steatotic Liver Disease Patients. Biomedicines 2023, 11, 3096. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Das, S.; Samajdar, S.S.; Joshi, S.R. Role of semaglutide in the treatment of nonalcoholic fatty liver disease or non-alcoholic steatohepatitis: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2023, 17, 102849. [Google Scholar] [CrossRef]
- Zhu, K.; Kakkar, R.; Chahal, D.; Yoshida, E.M.; Hussaini, T. Efficacy and safety of semaglutide in non-alcoholic fatty liver disease. World J. Gastroenterol. 2023, 29, 5327–5338. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Targher, G. Glucagon-Like Peptide-1 Receptor Agonists for Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: An Updated Meta-Analysis of Randomized Controlled Trials. Metabolites 2021, 11, 73. [Google Scholar] [CrossRef]
- Nevola, R.; Epifani, R.; Imbriani, S.; Tortorella, G.; Aprea, C.; Galiero, R.; Rinaldi, L.; Marfella, R.; Sasso, F.C. GLP-1 Receptor Agonists in Non-Alcoholic Fatty Liver Disease: Current Evidence and Future Perspectives. Int. J. Mol. Sci. 2023, 24, 1703. [Google Scholar] [CrossRef]
- Dusilova, T.; Kovar, J.; Drobny, M.; Sedivy, P.; Dezortova, M.; Poledne, R.; Zemankova, K.; Hajek, M. Different acute effects of fructose and glucose administration on hepatic fat content. Am. J. Clin. Nutr. 2019, 109, 1519–1526. [Google Scholar] [CrossRef]
- Kovar, J.; Dusilova, T.; Sedivy, P.; Bruha, R.; Gottfriedova, H.; Pavlikova, P.; Pitha, J.; Smid, V.; Drobny, M.; Dezortova, M.; et al. Acute responses of hepatic fat content to consuming fat, glucose and fructose alone and in combination in non-obese non-diabetic individuals with non-alcoholic fatty liver disease. J. Physiol. Pharmacol. 2021, 72, 45–53. [Google Scholar] [CrossRef]
- Lambert, J.E.; Ramos-Roman, M.A.; Browning, J.D.; Parks, E.J. Increased de novo lipogenesis is a distinct characteristic of individuals with nonalcoholic fatty liver disease. Gastroenterology 2014, 146, 726–735. [Google Scholar] [CrossRef] [PubMed]
- Sedivy, P.; Dezortova, M.; Burian, M.; Dusilova, T.; Kovar, J.; Hajek, M. Comparison of accuracy of magnetic resonance spectroscopic and imaging techniques for the liver steatosis assessment. Chem. Listy 2021, 115, 46–53. [Google Scholar]
- Longo, R.; Pollesello, P.; Ricci, C.; Masutti, F.; Kvam, B.J.; Bercich, L.; Croce, L.S.; Grigolato, P.; Paoletti, S.; de Bernard, B.; et al. Proton MR spectroscopy in quantitative in vivo determination of fat content in human liver steatosis. J. Magn. Reson. Imaging 1995, 5, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Havel, R.J.; Eder, H.A.; Bragdon, J.H. The distribution and chemical composition of ultracentrifugally separated lipoproteins in human serum. J. Clin. Investig. 1955, 34, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef]
- Eder, K. Gas chromatographic analysis of fatty acid methyl esters. J. Chromatogr. B Biomed. Appl. 1995, 671, 113–131. [Google Scholar] [CrossRef]
- Hudgins, L.C.; Hellerstein, M.; Seidman, C.; Neese, R.; Diakun, J.; Hirsch, J. Human fatty acid synthesis is stimulated by a eucaloric low fat, high carbohydrate diet. J. Clin. Investig. 1996, 97, 2081–2091. [Google Scholar] [CrossRef]
- Loomba, R.; Abdelmalek, M.F.; Armstrong, M.J.; Jara, M.; Kjaer, M.S.; Krarup, N.; Lawitz, E.; Ratziu, V.; Sanyal, A.J.; Schattenberg, J.M.; et al. Semaglutide 2.4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: A randomised, placebo-controlled phase 2 trial. Lancet Gastroenterol. Hepatol. 2023, 8, 511–522. [Google Scholar] [CrossRef]
- Donnelly, K.L.; Smith, C.I.; Schwarzenberg, S.J.; Jessurun, J.; Boldt, M.D.; Parks, E.J. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J. Clin. Investig. 2005, 115, 1343–1351. [Google Scholar] [CrossRef]
- Lee, J.J.; Lambert, J.E.; Hovhannisyan, Y.; Ramos-Roman, M.A.; Trombold, J.R.; Wagner, D.A.; Parks, E.J. Palmitoleic acid is elevated in fatty liver disease and reflects hepatic lipogenesis. Am. J. Clin. Nutr. 2015, 101, 34–43. [Google Scholar] [CrossRef]
- Taher, J.; Baker, C.L.; Cuizon, C.; Masoudpour, H.; Zhang, R.; Farr, S.; Naples, M.; Bourdon, C.; Pausova, Z.; Adeli, K. GLP-1 receptor agonism ameliorates hepatic VLDL overproduction and de novo lipogenesis in insulin resistance. Mol. Metab. 2014, 3, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Soto-Catalan, M.; Opazo-Rios, L.; Quiceno, H.; Lazaro, I.; Moreno, J.A.; Gomez-Guerrero, C.; Egido, J.; Mas-Fontao, S. Semaglutide Improves Liver Steatosis and De Novo Lipogenesis Markers in Obese and Type-2-Diabetic Mice with Metabolic-Dysfunction-Associated Steatotic Liver Disease. Int. J. Mol. Sci. 2024, 25, 2961. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.N.; Jin, T. Hepatic function of glucagon-like peptide-1 and its based diabetes drugs. Med. Rev. (2021) 2024, 4, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Xu, A.; Wang, Y.; Keshaw, H.; Xu, L.Y.; Lam, K.S.; Cooper, G.J. The fat-derived hormone adiponectin alleviates alcoholic and nonalcoholic fatty liver diseases in mice. J. Clin. Investig. 2003, 112, 91–100. [Google Scholar] [CrossRef]
- van Bloemendaal, L.; RG, I.J.; Ten Kulve, J.S.; Barkhof, F.; Konrad, R.J.; Drent, M.L.; Veltman, D.J.; Diamant, M. GLP-1 receptor activation modulates appetite- and reward-related brain areas in humans. Diabetes 2014, 63, 4186–4196. [Google Scholar] [CrossRef]
- Blundell, J.; Finlayson, G.; Axelsen, M.; Flint, A.; Gibbons, C.; Kvist, T.; Hjerpsted, J.B. Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. Diabetes Obes. Metab. 2017, 19, 1242–1251. [Google Scholar] [CrossRef]
- Adiels, M.; Taskinen, M.R.; Packard, C.; Caslake, M.J.; Soro-Paavonen, A.; Westerbacka, J.; Vehkavaara, S.; Hakkinen, A.; Olofsson, S.O.; Yki-Jarvinen, H.; et al. Overproduction of large VLDL particles is driven by increased liver fat content in man. Diabetologia 2006, 49, 755–765. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| n | 16 |
|---|---|
| Age (years) | 47.0 ± 12.4 |
| Weight (kg) | 120.3 ± 12.0 |
| BMI (kg/m2) | 36.2 ± 3.8 |
| Waist circumference (cm) | 120 ± 10 |
| Total body fat (kg) | 39.4 ± 7.9 |
| Total body fat (%) | 32.4 ± 3.7 |
| Glucose (mmol/L) | 5.92 ± 0.47 |
| Insulin (mIU/L) | 21.1 ± 6.9 |
| HOMA-IR | 5.24 ± 1.64 |
| Triglyceride (mmol/L) | 1.36 ± 0.29 |
| Cholesterol (mmol/L) | 4.51 ± 0.68 |
| ALT (µkat/L) | 0.60 ± 0.15 |
| AST (µkat/L) | 0.48 ± 0.12 |
| GGT (µkat/L) | 0.75 ± 0.83 |
| Hepatic fat content (%) | 13.3 ± 8.5 |
| Dietary Intervention | Treatment | Diet vs. Treatment | |||
|---|---|---|---|---|---|
| Start | End | Start | End | p | |
| Adiposity | |||||
| Weight (kg) | 116.8 ± 13.0 | 117.0 ± 11.6 | 118.7 ± 12.3 | 112.1 ± 12.4 *** | 0.0008 |
| BMI (kg/m2) | 35.1 ± 4.0 | 35.2 ± 3.5 | 35.7 ± 3.9 | 33.7 ± 3.8 *** | 0.0008 |
| Total body fat (kg) | 36.7 ± 8.4 | 37.0 ± 7.6 | 38.5 ± 8.3 | 34.0 ± 8.1 *** | 0.0001 |
| Total body fat (%) | 31.1 ± 4.1 | 31.4 ± 3.8 | 32.1 ± 4.0 | 30.1 ± 4.0 *** | 0.0002 |
| Subcutan. fat (cm2) | 372 ± 124 | 380 ± 130 | 391 ± 140 | 349 ± 131 *** | 0.0042 |
| Visceral fat (cm2) | 318 ± 72 | 318 ± 70 | 322 ± 70 | 293 ± 63 ** | 0.0052 |
| Liver fat | |||||
| HFC (%) | 12.35 ± 8.77 | 11.02 ± 8.06 | 12.21 ± 7.56 | 8.33 ± 4.98 *** | 0.0250 |
| HFV (mL) | 276 ± 230 | 238 ± 198 | 266 ± 186 | 161 ± 99 *** | 0.0507 |
| Biochemistry | |||||
| HOMA-IR | 5.26 ± 1.73 | 4.43 ± 1.58 * | 5.43 ± 2.19 | 4.55 ± 1.77 | 0.9439 |
| Insulin (mIU/L) | 20.6 ± 6.2 | 17.1 ± 5.5 * | 20.5 ± 7.5 | 18.9 ± 6.6 | 0.4331 |
| Glucagon (pmol/L) | 7.16 ± 3.06 | 7.80 ± 3.50 | 8.35 ± 3.08 | 5.98 ± 2.60 *** | 0.0007 |
| Glucose (mmol/L) | 5.71 ± 0.53 | 5.80 ± 0.46 | 5.91 ± 0.46 | 5.35 ± 0.34 | <0.0001 |
| TG (mmol/L) | 1.25 ± 0.31 | 1.36 ± 0.47 | 1.40 ± 0.44 | 1.14 ± 0.32 ** | 0.0166 |
| VLDL-TG (mmol/L) | 0.83 ± 0.27 | 0.99 ± 0.43 | 0.99 ± 0.39 | 0.76 ± 0.32 ** | 0.0115 |
| NEFA (mM) | 0.45 ± 0.12 | 0.43 ± 0.13 | 0.41 ± 0.14 | 0.43 ± 0.09 | 0.1297 |
| ΒHB (µmol/L) | 45.1 ± 22.3 | 37.8 ± 13.5 | 41.1 ± 21.0 | 46.8 ± 22.0 | 0.3484 |
| Cholesterol (mmol/L) | 4.63 ± 0.74 | 4.38 ± 0.72 | 4.56 ± 0.68 | 4.56 ± 0.90 | 0.2070 |
| Leptin (µg/L) | 58.3 ± 27.6 | 58.6 ± 25.7 | 65.1 ± 31.0 | 49.1 ± 27.0 *** | 0.0125 |
| Adiponectin (µg/L) | 6046 ± 2135 | 6127 ± 1883 | 5876 ± 1940 | 6102 ± 2179 | 0.7236 |
| FGF-19 # (ng/L) | 196 ± 168 | 189 ± 149 | 164 ± 91 | 206 ± 165 | 0.3390 |
| FGF-21 ## (ng/L) | 209 ± 135 | 192 ± 109 | 193 ± 109 | 184 ± 119 | 0.7936 |
| Spexin (ng/L) | 130 ± 77 | 131 ± 70 | 131 ± 87 | 123 ± 78 | 0.3303 |
| ALT (µkat/mmol) | 0.64 ± 0.17 | 0.62 ± 0.27 | 0.62 ± 0.24 | 0.54 ± 0.28 | 0.4164 |
| AST (µkat/mmol) | 0.46 ± 0.13 | 0.45 ± 0.11 | 0.46 ± 0.11 | 0.43 ± 0.12 | 0.6519 |
| GGT (µkat/mmol) | 0.66 ± 0.82 | 0.66 ± 0.65 | 0.70 ± 0.67 | 0.62 ± 0.79 * | 0.1167 |
| Dietary Intervention | Treatment | |||
|---|---|---|---|---|
| Δ HFC (%) | Δ HFV (mL) | Δ HFC (%) | Δ HFV (mL) | |
| Δ HFC (%) | 1.000 *** | 0.974 *** | 1.000 *** | 0.945 *** |
| Δ HFV (mL) | 0.974 *** | 1.000 *** | 0.945 *** | 1.000 *** |
| Δ weight (kg) | 0.888 *** | 0.836 *** | 0.284 | 0.230 |
| Δ BMI (kg/m2) | 0.903 *** | 0.849 *** | 0.338 | 0.274 |
| Δ total body fat (kg) | 0.882 *** | 0.840 *** | 0.021 | −0.078 |
| Δ total body fat (%) | 0.834 *** | 0.804 *** | 0.011 | −0.174 |
| Δ subcutaneous fat (cm2) | 0.551 * | 0.541 * | 0.441 | 0.303 |
| Δ visceral fat (cm2) | 0.781 ** | 0.683 ** | 0.720 ** | 0.672 ** |
| Δ HOMA-IR | 0.226 | 0.209 | −0.319 | −0.182 |
| Δ insulin | 0.201 | 0.179 | −0.401 | −0.257 |
| Δ glucagon | 0.330 | 0.314 | −0.059 | −0.077 |
| Δ glucose | 0.189 | 0.195 | 0.219 | 0.288 |
| Δ TG | 0.329 | 0.351 | −0.346 | −0.264 |
| Δ VLDL-TG | 0.312 | 0.337 | −0.507 * | −0.393 |
| Dietary Intervention | Treatment | Diet vs. Treatment | |||
|---|---|---|---|---|---|
| Fatty Acid | Start | End | Start | End | p |
| 14:0 | 0.52 ± 0.13 | 0.49 ± 0.12 | 0.47 ± 0.12 | 0.50 ± 13 | 0.1548 |
| 16:0 | 23.34 ± 1.99 | 23.05 ± 1.97 | 23.44 ± 1.74 | 22.60 ± 1.59 * | 0.3149 |
| 18:0 | 3.59 ± 0.81 | 3.39 ± 0.83 | 3.44 ± 0.87 | 3.34 ± 0.81 | 0.7889 |
| 16:1n − 7 | 2.82 ± 0.92 | 3.02 ± 0.81 | 2.85 ± 0.80 | 2.50 ± 0.51 * | 0.0229 |
| 18:1n − 9 | 42.64 ± 3.12 | 42.75 ± 2.29 | 43.09 ± 3.00 | 43.10 ± 3.30 | 0.9075 |
| 18:1n − 7 | 3.02 ± 0.58 | 3.37 ± 0.75 | 3.31 ± 0.55 | 3.17 ± 0.62 | 0.0833 |
| 18:2n − 6 | 17.93 ± 2.87 | 17.82 ± 2.57 | 17.43 ± 2.06 | 18.35 ± 2.96 * | 0.2510 |
| 18:3n − 6 | 0.32 ± 0.14 | 0.33 ± 0.11 | 0.33 ± 0.13 | 0.32 ± 0.10 | 0.5981 |
| 20:2n − 6 | 0.39 ± 0.06 | 0.41 ± 0.07 | 0.40 ± 0.07 | 0.40 ± 0.09 | 0.4159 |
| 20:3n − 6 | 0.40 ± 0.09 | 0.42 ± 0.09 | 0.40 ± 0.09 | 0.41 ± 0.10 | 0.7185 |
| 20:4n − 6 | 1.39 ± 0.35 | 1.37 ± 0.32 | 1.47 ± 0.39 | 1.42 ± 0.34 | 0.7248 |
| 22:4n − 6 | 0.23 ± 0.05 | 0.24 ± 0.06 | 0.25 ± 0.08 | 0.23 ± 0.05 | 0.1386 |
| 18:3n − 3 | 1.42 ± 0.77 | 1.41 ± 0.73 | 1.32 ± 0.69 | 1.48 ± 0.67 | 0.0833 |
| 18:4n − 3 | 0.31 ± 0.11 | 0.33 ± 0.08 | 0.33 ± 0.08 | 0.31 ± 0.09 | 0.3261 |
| 20:4n − 3 | 0.05 ± 0.01 | 0.05 ± 0.02 | 0.05 ± 0.02 | 0.05 ± 0.02 | 0.6206 |
| 20:5n − 3 | 0.27 ± 0.17 | 0.27 ± 0.13 | 0.26 ± 0.15 | 0.28 ± 0.19 | 0.8443 |
| 22:5n − 3 | 0.15 ± 0.05 | 0.16 ± 0.05 | 0.16 ± 0.05 | 0.16 ± 0.05 | 0.7511 |
| 22:6n − 3 | 0.51 ± 0.16 | 0.52 ± 0.14 | 0.48 ± 0.15 | 0.54 ± 0.19 | 0.3750 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dusilová, T.; Kovář, J.; Laňková, I.; Thieme, L.; Hubáčková, M.; Šedivý, P.; Pajuelo, D.; Burian, M.; Dezortová, M.; Miklánková, D.; et al. Semaglutide Treatment Effects on Liver Fat Content in Obese Subjects with Metabolic-Associated Steatotic Liver Disease (MASLD). J. Clin. Med. 2024, 13, 6100. https://doi.org/10.3390/jcm13206100
Dusilová T, Kovář J, Laňková I, Thieme L, Hubáčková M, Šedivý P, Pajuelo D, Burian M, Dezortová M, Miklánková D, et al. Semaglutide Treatment Effects on Liver Fat Content in Obese Subjects with Metabolic-Associated Steatotic Liver Disease (MASLD). Journal of Clinical Medicine. 2024; 13(20):6100. https://doi.org/10.3390/jcm13206100
Chicago/Turabian StyleDusilová, Tereza, Jan Kovář, Ivana Laňková, Lenka Thieme, Monika Hubáčková, Petr Šedivý, Dita Pajuelo, Martin Burian, Monika Dezortová, Denisa Miklánková, and et al. 2024. "Semaglutide Treatment Effects on Liver Fat Content in Obese Subjects with Metabolic-Associated Steatotic Liver Disease (MASLD)" Journal of Clinical Medicine 13, no. 20: 6100. https://doi.org/10.3390/jcm13206100
APA StyleDusilová, T., Kovář, J., Laňková, I., Thieme, L., Hubáčková, M., Šedivý, P., Pajuelo, D., Burian, M., Dezortová, M., Miklánková, D., Malínská, H., Svobodová Šťastná, P., Poledne, R., Hájek, M., & Haluzík, M. (2024). Semaglutide Treatment Effects on Liver Fat Content in Obese Subjects with Metabolic-Associated Steatotic Liver Disease (MASLD). Journal of Clinical Medicine, 13(20), 6100. https://doi.org/10.3390/jcm13206100