
Particularities of a Cardiac Amorphous Left Ventricular Tumor in a Patient with Coronary Artery Disease—Diagnostic and Therapeutic Challenges: A Case Report and Literature Review

 , ,
, ,  ,
,
Abstract

1. Introduction
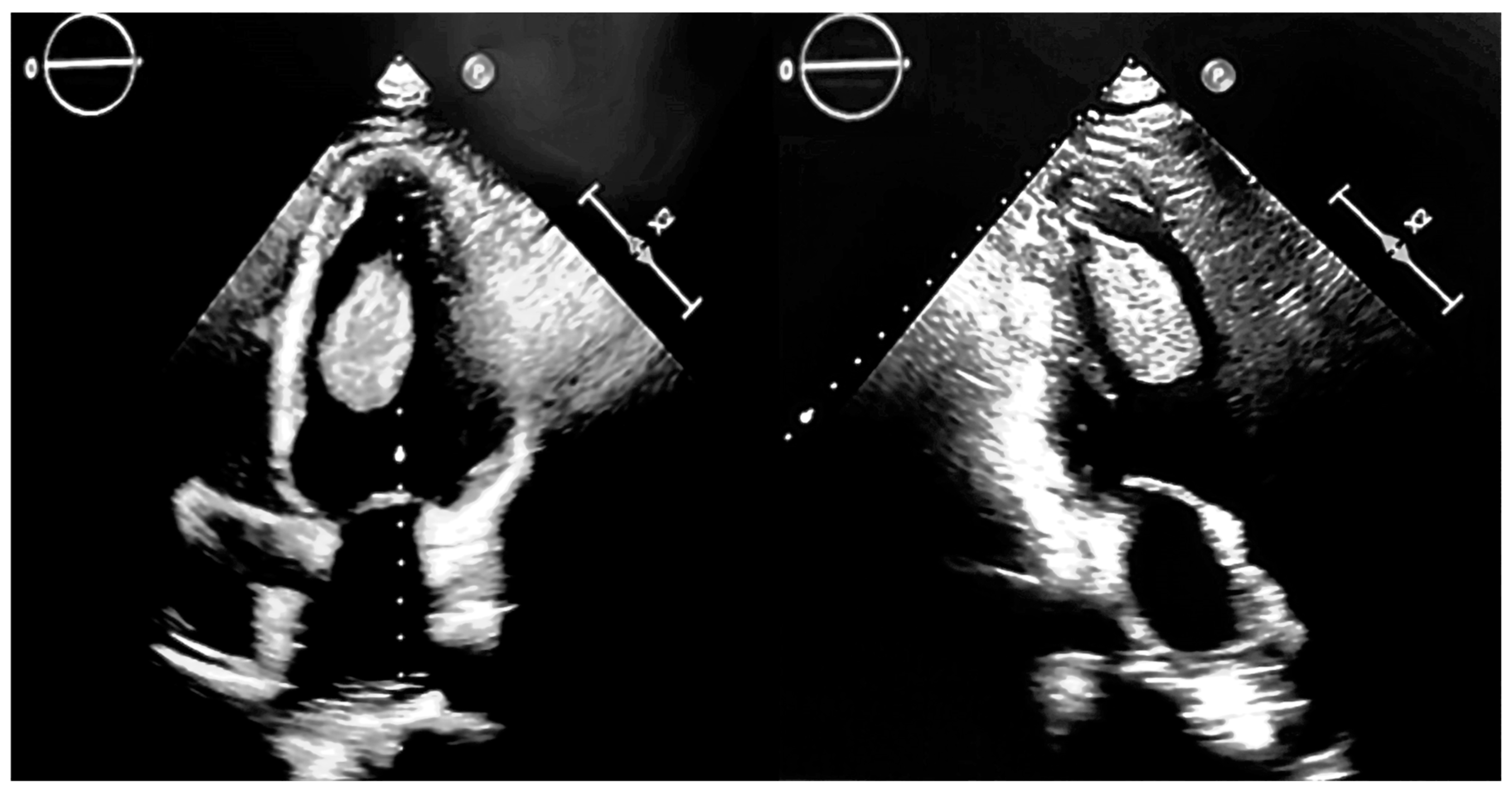
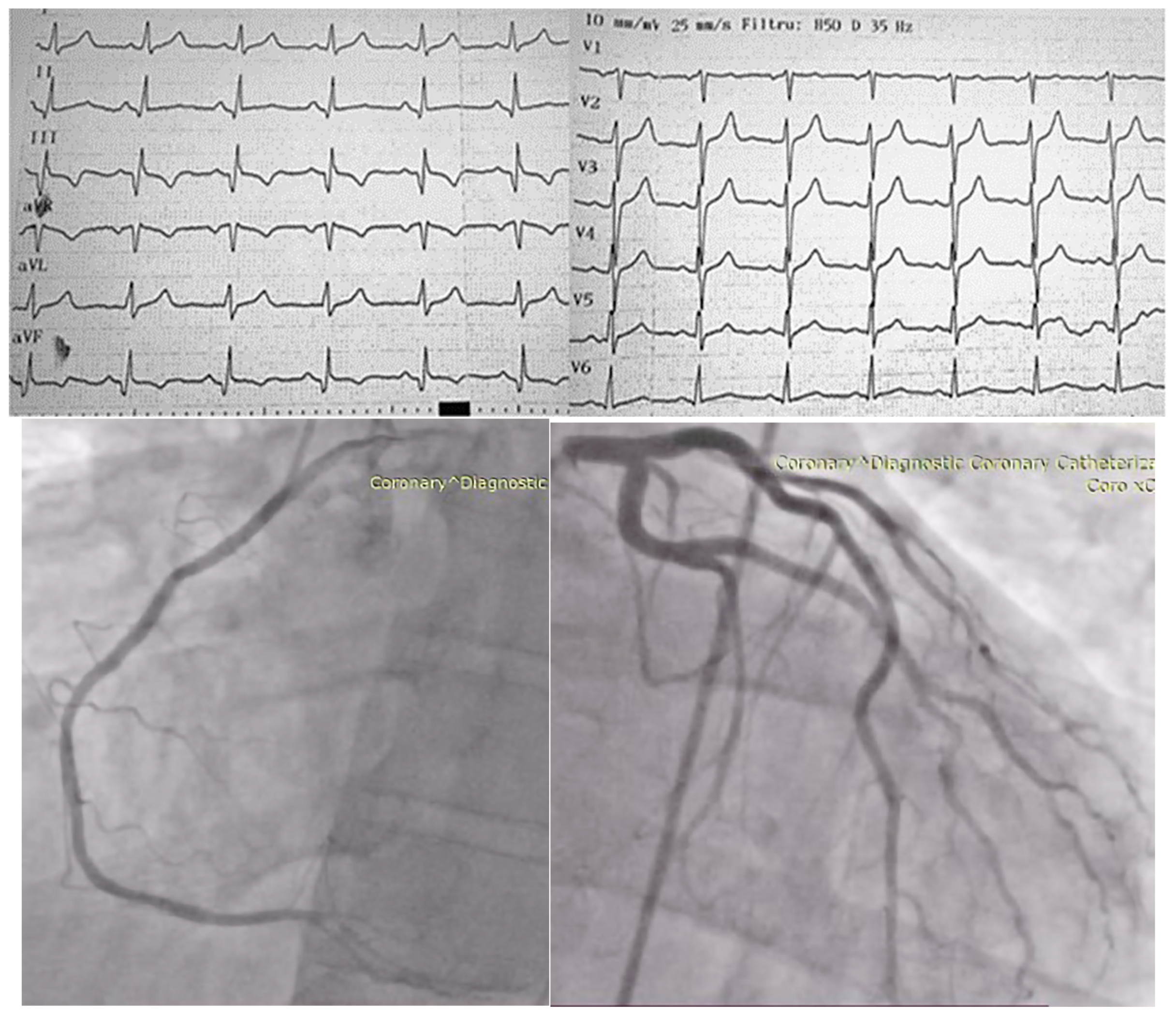
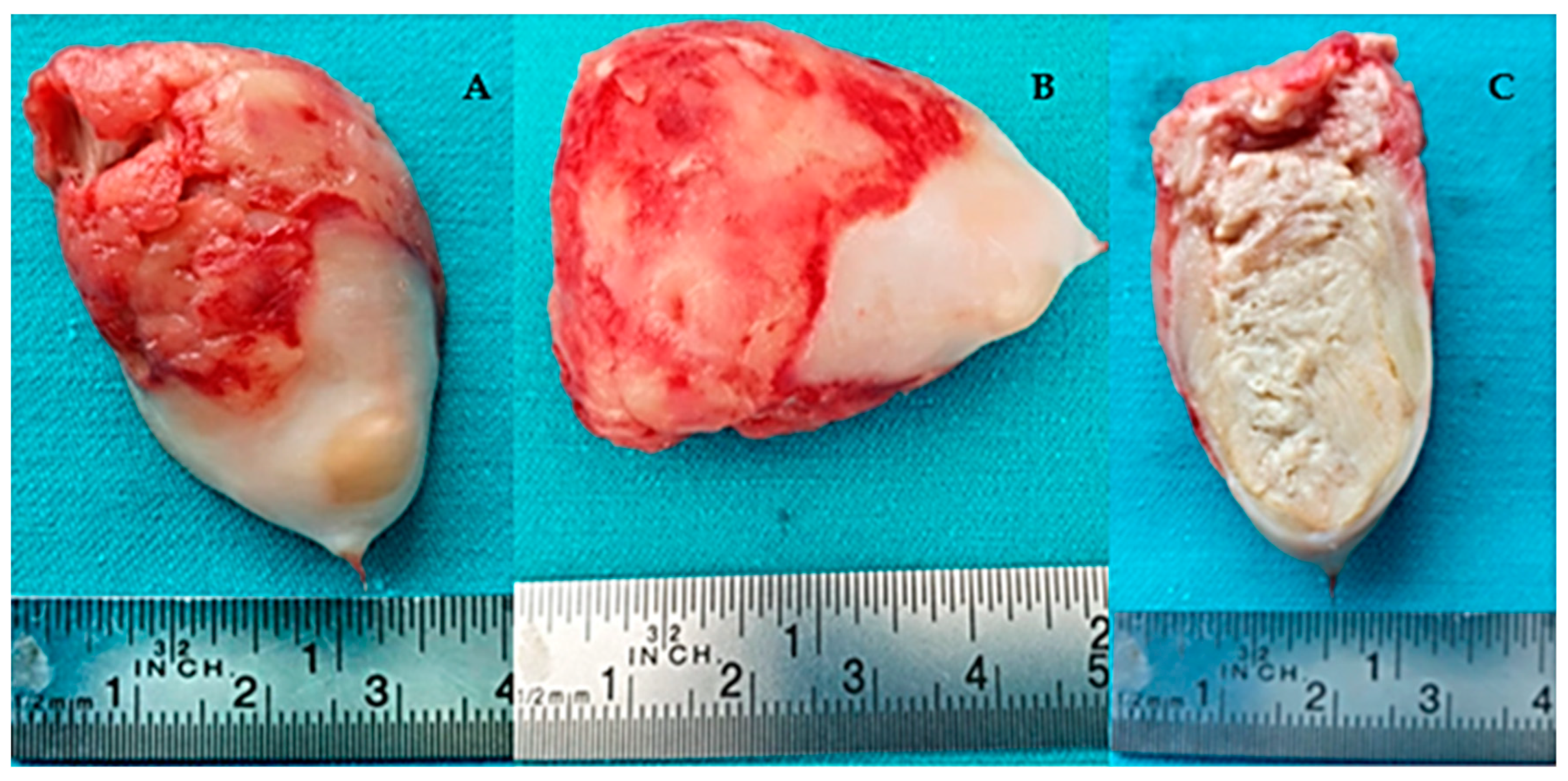
2. Case Presentation
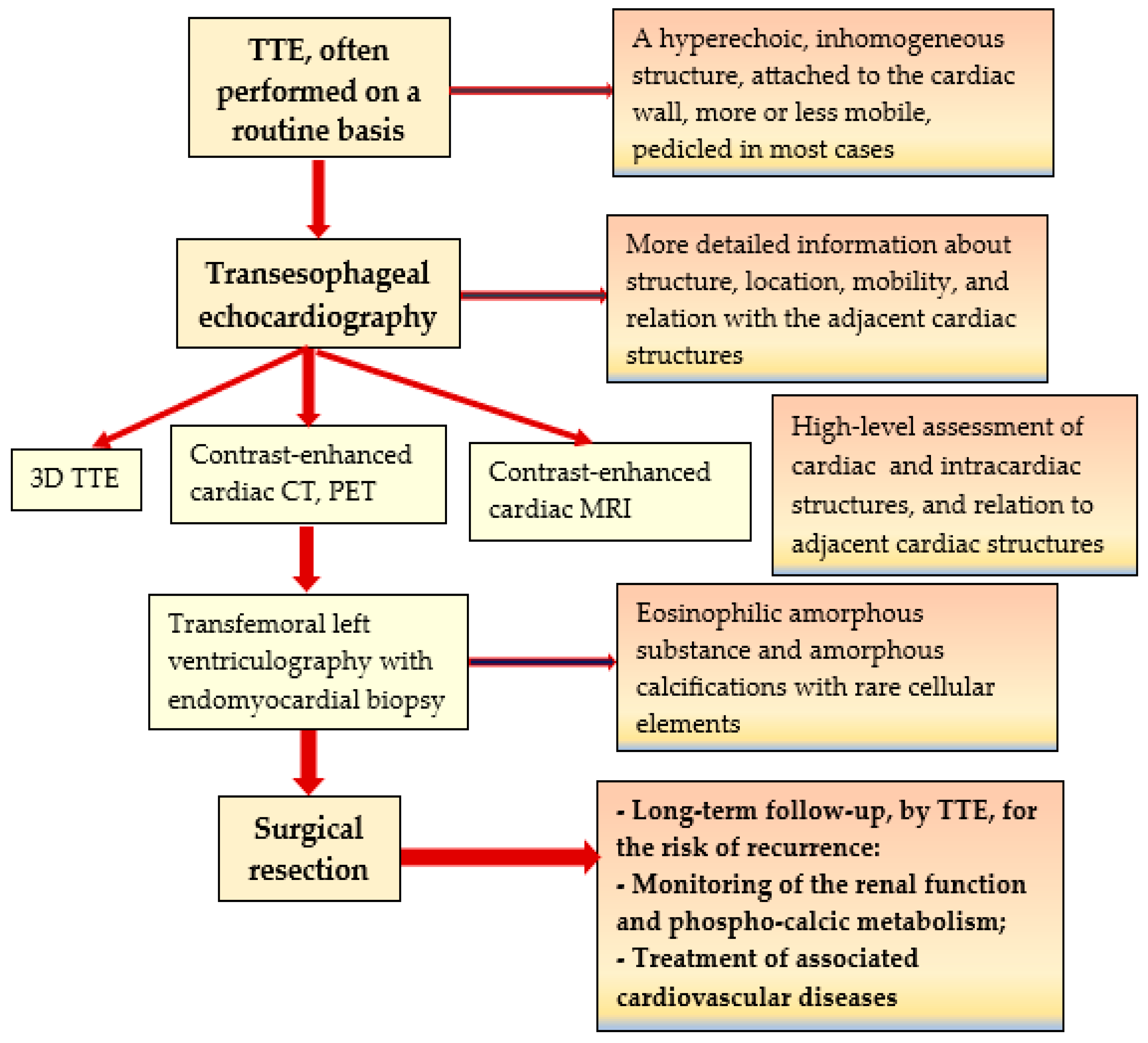
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reynolds, C.; Tazelaar, H.D.; Edwards, W.D. Calcified Amorphous Tumor of the Heart (Cardiac CAT). Hum. Pathol. 1997, 28, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Halder, V.; Ghosh, S.; Kumar, B.; Guha Neogi, S.; Thirunavukkarasu, B.; Bal, A. Calcified Amorphous Tumor of Left Ventricle: A Rare Cardiac Tumor. Cureus 2021, 13, e17908. [Google Scholar] [CrossRef] [PubMed]
- Ufuk, F.; Kilic, I.D. Case 315: Cardiac Calcified Amorphous Tumor. Radiology 2023, 308, e220881. [Google Scholar] [CrossRef] [PubMed]
- Kerndt, C.; Cameron, E.; Nowak, C.; Lesoski, C.; Lesoski, C.; Vishwanath, R. Echocardiography Findings in Cardiac Calcified Amorphous Tumor: A Systematic Review. J. Am. Coll. Cardiol. 2021, 77, 1339. [Google Scholar] [CrossRef]
- de Hemptinne, Q.; de Cannière, D.; Vandenbossche, J.-L.; Unger, P. Cardiac Calcified Amorphous Tumor: A Systematic Review of the Literature. Int. J. Cardiol. Heart Vasc. 2015, 7, 1–5. [Google Scholar] [CrossRef]
- Shah, A.C.; Marcoff, L.; Talati, S.; Donahue, J.; Uretsky, S.; Magovern, C.; Gillam, L.D. A Rare Beast: Cardiac Calcified Amorphous Tumor. CASE 2018, 2, 139–141. [Google Scholar] [CrossRef]
- Tsushima, S.; Maeda, T.; Nakashima, S.; Muraki, S.; Sakurada, T.; Sasaki, J.; Araki, E. Calcified Amorphous Tumor Diagnosed After Stroke:Report of a Case. Kyobu Geka 2024, 77, 316–318. [Google Scholar]
- Eizawa, S.; Morimoto, Y.; Yamada, A.; Sato, M. Multiple Calcified Amorphous Tumours of the Heart. BMJ Case Rep. 2023, 16, e254823. [Google Scholar] [CrossRef]
- Ushioda, R.; Shirasaka, T.; Kikuchi, S.; Kamiya, H.; Kanamori, T. Calcified Amorphous Tumor Located on a Severely Calcified Mitral Annulus in a Patient with Normal Renal Function. J. Surg. Case Rep. 2022, 2022, rjab608. [Google Scholar] [CrossRef]
- Endo, T.; Lei, K.; Ahsan, C. Cardiac Tumor in the Left Ventricular Outflow Tract: Atypical Presentation of Calcified Amorphous Tumor. J. Surg. Case Rep. 2022, 2022, rjac179. [Google Scholar] [CrossRef]
- Suzue, T.; Sawayama, Y.; Suzuki, T.; Nakagawa, Y. A Rapidly Growing Cardiac Calcified Amorphous Tumour Diagnosed after Coronary Artery Bypass Graft Surgery: A Case Report. Eur. Heart J. Case Rep. 2021, 5, ytab243. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, Y.; Matsuyama, H.; Shindo, A.; Matsuura, K.; Niwa, A.; Hirota, Y.; Fukuma, T.; Ito, H.; Kozuka, Y.; Tomimoto, H. Cerebral Embolism Associated with Calcified Amorphous Tumor: A Review of Cerebral Infarction Cases. Intern. Med. 2021, 60, 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Hatori, K.; Mohara, J.; Shibata, S.; Murata, M.; Fukuda, N.; Hiroi, S.; Koyano, T. Cardiac Calcified Amorphous Tumor in a Patient with Lung Cancer. Gen. Thorac. Cardiovasc. Surg. Cases 2024, 3, 35. [Google Scholar] [CrossRef]
- Ghabally, M.; Shebli, B.; Alafandi, B.Z.; Allouzi, S.; Markaby, J.; Malhis, M.; Babi, A. An Ambiguous Presentation of Cardiac Calcified Amorphous Tumor in a 37-Year-Old Male. J. Surg. Case Rep. 2023, 2023, rjad397. [Google Scholar] [CrossRef]
- Odujoko, O.; Asad, M.; Bal, S.; Dodge, J.; Janjua, J. A Rare Case of Cardiac Calcified Amorphous Tumor in a 34-Year-Old Woman Diagnosed at Autopsy. Am. J. Clin. Pathol. 2023, 160, S3–S4. [Google Scholar] [CrossRef]
- Kimura, M.; Niwa, J.-I.; Ito, H.; Matsuyama, K.; Doyu, M. Multiple Cerebral Infarctions Due to Calcified Amorphous Tumor Growing Rapidly from an Antecedent Infection and Decreasing Rapidly by Detachment of Fibrin and Antithrombotic Drugs: A Case Report. BMC Neurol. 2022, 22, 391. [Google Scholar] [CrossRef] [PubMed]
- Koyama, Y.; Tsujimoto, S.; Yamamoto, M. Calcified Amorphous Tumor in the Aortic Valve Identified by Computed Tomography. J. Thorac. Cardiovasc. Surg. 2020, 159, e161–e163. [Google Scholar] [CrossRef]
- Yamanaka, T.; Fukatsu, T.; Uchimuro, T.; Takanashi, S. Cardiac calcified amorphous tumour associated with multiple myeloma. BMJ Case Rep. CP 2020, 13, e233679. [Google Scholar] [CrossRef]
- Okazaki, A.; Oyama, Y.; Hosokawa, N.; Ban, H.; Miyaji, Y.; Moody, S. The first report of calcified amorphous tumor associated with infective endocarditis: A case report and review of literature. Am. J. Case Rep. 2020, 21, e922960-1. [Google Scholar] [CrossRef]
- Formelli, B.; Farina, A.; Pescini, F.; Palumbo, V.; Grazia D’Alfonso, M.; Oddo, A.; Mori, F.; Poggesi, A. Cardiac Calcified Amorphous Tumor as a Rare Cause of Ischemic Stroke: Clinical Case. Circ. Cardiovasc. Imaging 2020, 13, e009623. [Google Scholar] [CrossRef]
- Tudoran, M.; Tudoran, C.; Ciocarlie, T.; Pop, G.N.; Berceanu-Vaduva, M.M.; Velimirovici, D.E.; Ahmed, A.A.; Berceanu-Vaduva, D.M. Aspects of Heart Failure in Patients with Ischemic Heart Disease after Percutaneous Coronary Revascularization with Polymer-Coated Drug-Eluting Stents versus Bare-Metal Stents. Mater. Plast. 2019, 56, 37–40. [Google Scholar] [CrossRef]
- Takahashi, Y.; Inaba, Y.; Tsuchiya, H.; Minegishi, S.; Niino, T.; Endo, H.; Kubota, H. Clinical Features of Cardiac Calcified Amorphous Tumor: A Narrative Review. Cardiol. Rev. 2024. [Google Scholar] [CrossRef] [PubMed]
- Perone, F.; Bernardi, M.; Redheuil, A.; Mafrica, D.; Conte, E.; Spadafora, L.; Ecarnot, F.; Tokgozoglu, L.; Santos-Gallego, C.G.; Kaiser, S.E.; et al. Role of Cardiovascular Imaging in Risk Assessment: Recent Advances, Gaps in Evidence, and Future Directions. J. Clin. Med. 2023, 12, 5563. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Authors/Year | No. of Patients/Gender/Age | Associated Conditions | Location in LV | Symptoms | Renal Status | CAT Evolution |
|---|---|---|---|---|---|---|---|
| 1. | Tsushima et al./2024 [7] | 1/M/58 | Hemodialysis | A mass attached to the posterior mitral leaflet and dense mitral annular calcification | Acute stroke | Heamodyalisis for 2 years | Unknown |
| 2. | Hatori et al./2024 [13] | 1/F/77 | Systemic hypertension, lung cancer, coronary artery disease | A mobile mass in the LV outflow tract attached to the non-coronary and the right coronary aortic cusp | Dyspnea, chest pain | Creatinine = 0.85 mg/dL | Unknown |
| 3. | Eizawa et al./2023 [8] | 1/F/80 | Calcified mitral annulus | Mobile mass originating from the mitral annulus of the posterior leaflet | Left eye vision loss due to an embolus at the bifurcation of the retinal artery | NR | Unknown |
| 4. | Ufuc et al./2023 [3] | 1/M/58 | Not significant | Calcified, irregular tubular, and infiltrative mass in the inferior-basal segment of LV, extending in the mid-inferior wall, mid-inferior septum, and inferior papillary muscle | Chest pain, palpitations | NR | 3 years |
| 5. | Ghaballi et al./2023 [14] | 1/M/37 | Not significant | An irregular mass with a wide base attached to the atrial wall | Chest pain | NR | 5 years |
| 6. | Odujoko et al./2023 [15] | 1/F/34 | Type 1 diabetes mellitus, hypertension, Hashimoto thyroiditis, mesenteric ischemia, recent myocardial infarction of the posterolateral LV, moderate/severe coronary atherosclerosis, end-stage renal disease under hemodialysis | Masses on the mitral valve, the endocardium, and subendocardial portions of the left and right ventricles | Abdominal pain, gluteal pain, and diarrhea | Creatinine = 3.52 mg/dL, CKD | Autopsy finding |
| 7. | Ushioda et al./2022 [9] | 1/F/86 | 90% stenosis of the right coronary artery requiring coronary artery bypass, preserved ejection fraction, severe mitral annular calcifications | A mobile mass within the anterior annulus of the mitral valve | Episodes of syncope | NR | Unknown |
| 8. | Endo et al./2022 [10] | 1/F/71 | Diabetes mellitus, multiple myeloma | A mobile, nonobstructive mass attached to the anterior leaflet of the mitral valve | Asymptomatic | NR | Unknown |
| 9. | Kimura et al./2022 [16] | 1/F/82 | Mitral annular calcification, repeated strokes, dental infection | A calcified mass on the posterior leaflet | Acute stroke | NR | 7 months |
| 10. | Nishiguchi et al./2021 [12] | 1/F/67 | Stroke, systolic hypertension, hyperlipidemia | A pedunculated mass attached to the posterior leaflet of the mitral valve | Visual impairment | Creatinine = 1.45 mg/dL | 5 months |
| 11. | Kumar et al./2021 [2] | 1/F/46 | Chronic kidney disease stage 4, right thromboembolic frontoparietal infarct (2 months ago), coronary artery disease requiring coronary artery by-pass, heart failure with reduced ejection fraction | A pedunculated mobile mass attached to the intraventricular septum | Signs and symptoms of decompensated heart failure and decreased urine output | NR | Unknown |
| 12. | Suzue et al./2021 [11] | 1/F/83 | Coronary artery bypass graft surgery, mitral annular calcification | Mobile, pediculated mass adherend to the posterior commissure of the mitral valve | Asymptomatic | Creatinine—0.43 mg/dL | 4 months |
| 13. | Koyama et al./2021 [17] | 1/F/83 | Aortic valve stenosis | Encapsulated mass between the noncoronary and the left coronary aortic cusp | Symptoms attributed to aortic valve stenosis | NR | Unknown |
| 14. | Yamanaka et al./2020 [18] | 1/F/82 | Systemic hypertension, diabetes mellitus type 2, multiple myeloma, chemotherapy, MAC | An immobile, calcified mass on the mitral annulus | Asymptomatic | Creatinine = 0.61 mg/dL | 18 months |
| 15. | Okazaki et al./2020 [19] | 1/M/67 | Chronic hemodialysis, heart failure, systemic hypertension, gastric cancer, infectious endocarditis with Enterococcus faecalis | A mobile, cystic lesion with a mass inside the cyst attached to the apex of the LV wall | Fatigue, stomatitis, and diarrhea | ESRD | 5 months |
| 16 | Formelli et al./2020 [20] | 1/F/79 | Systemic hypertension, polyglobulia | An echodense, not mobile left atrial mass | Ischemic stroke | NR | 3 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Streian, C.G.; Tudoran, C.; Staicu, R.E.; Negru, A.G.; Mederle, A.L.; Borza, C.; Lascu, A. Particularities of a Cardiac Amorphous Left Ventricular Tumor in a Patient with Coronary Artery Disease—Diagnostic and Therapeutic Challenges: A Case Report and Literature Review. J. Clin. Med. 2024, 13, 6092. https://doi.org/10.3390/jcm13206092
Streian CG, Tudoran C, Staicu RE, Negru AG, Mederle AL, Borza C, Lascu A. Particularities of a Cardiac Amorphous Left Ventricular Tumor in a Patient with Coronary Artery Disease—Diagnostic and Therapeutic Challenges: A Case Report and Literature Review. Journal of Clinical Medicine. 2024; 13(20):6092. https://doi.org/10.3390/jcm13206092
Chicago/Turabian StyleStreian, Caius Glad, Cristina Tudoran, Raluca Elisabeta Staicu, Alina Gabriela Negru, Alexandra Laura Mederle, Claudia Borza, and Ana Lascu. 2024. "Particularities of a Cardiac Amorphous Left Ventricular Tumor in a Patient with Coronary Artery Disease—Diagnostic and Therapeutic Challenges: A Case Report and Literature Review" Journal of Clinical Medicine 13, no. 20: 6092. https://doi.org/10.3390/jcm13206092
APA StyleStreian, C. G., Tudoran, C., Staicu, R. E., Negru, A. G., Mederle, A. L., Borza, C., & Lascu, A. (2024). Particularities of a Cardiac Amorphous Left Ventricular Tumor in a Patient with Coronary Artery Disease—Diagnostic and Therapeutic Challenges: A Case Report and Literature Review. Journal of Clinical Medicine, 13(20), 6092. https://doi.org/10.3390/jcm13206092